






 Author Affiliations
Author Affiliations
Abstract
Rathke’s cleft cysts (RCCs) are typically benign lesions arising in the sellar region; however, they may occasionally result in clinically significant complications, including hormonal dysfunction and compression of the optic apparatus. We describe two adult patients with differing postoperative outcomes following surgical management.
This case report aims to highlight the variable clinical presentation, diagnostic challenges, and unpredictable postoperative outcomes of Rathke’s cleft cysts, emphasizing the importance of long-term follow-up.
The first patient was a 45-year-old man who presented with the complaint of headaches and blurred vision. During his workup, he was found to have panhypopituitarism. He underwent endoscopic transsphenoidal surgery, and he recovered. His symptoms settled, and repeated imaging didn’t show any obvious residual lesion.
The second patient was a 53-year-old woman who was initially diagnosed with a pituitary macroadenoma based on imaging. However, intraoperatively it turned out to be a RCC. The immediate postoperative scans were reassuring, with complete cyst removal and good decompression of the optic chiasm. A few months later, on follow-up imaging, a small cyst was seen to be developing again, with mild pressure over the pituitary stalk.
These two cases just didn’t play out the same. RCCs might have the “benign” label, but reality doesn’t always go by the book. Our first patient got better and stayed that way. However, the second one stayed fine at first, but then her cyst reappeared. This explains that RCCs sometimes may follow an unpredictable course. This highlights the importance of ongoing follow-up and multidisciplinary management after successful surgery.
Keywords
Rathke’s cleft cyst, Sellar lesions, Endoscopic transsphenoidal surgery, Panhypopituitarism, Optic chiasm compression.
Introduction
Rathke’s cleft cysts (RCC) sit in the sellar or suprasellar regions, emerging from leftover bits of Rathke’s pouch, the embryonic piece that becomes the anterior pituitary. RCCs are typically discovered incidentally during computed tomography scans or magnetic resonance imaging (MRI).[1] Most don’t cause symptoms, but they are found in 13%–33% of patients on autopsy studies.[2,3] RCCs can happen at any age but are more common in the fourth to sixth decades of life, with a female predominance of a 2:1 ratio.[1,3,4] Clinical presentation depends on the size and location of the cyst. Symptoms may include headaches and blurred vision if the cyst compresses the optic chiasm, or hormonal disturbances like decreased pituitary function or diabetes insipidus.[5]
MRI is usually the go-to test.[6] On imaging, RCCs often show up as neat, round, non-enhancing cysts. The signal can change depending on what’s inside the cyst: T1 bright spots usually mean protein-rich or hemorrhagic fluid, while T2 bright spots suggest simple fluid.[3] Even so, telling RCCs apart from other pituitary tumors, like non-functioning adenomas, isn’t always easy. One of our patients was a good example, in whom the imaging initially suggested something else, and we only knew for sure once we looked under the microscope. Recurrence can happen, sometimes months or even years after surgery, so keeping an eye on these patients long-term is important.[3,7]
Case presentation
Patient A: A 45-year-old man visited us with the complaint of headaches for three months and some blurring of vision, and he was feeling unusually tired. Visual testing showed mild bitemporal hemianopia. A blood workup was done, which revealed panhypopituitarism. An MRI was done, which revealed a 2.5 × 2.1 × 2.0 cm cyst in the sellar region, pressing on the optic chiasm. He underwent endoscopic transsphenoidal resection.
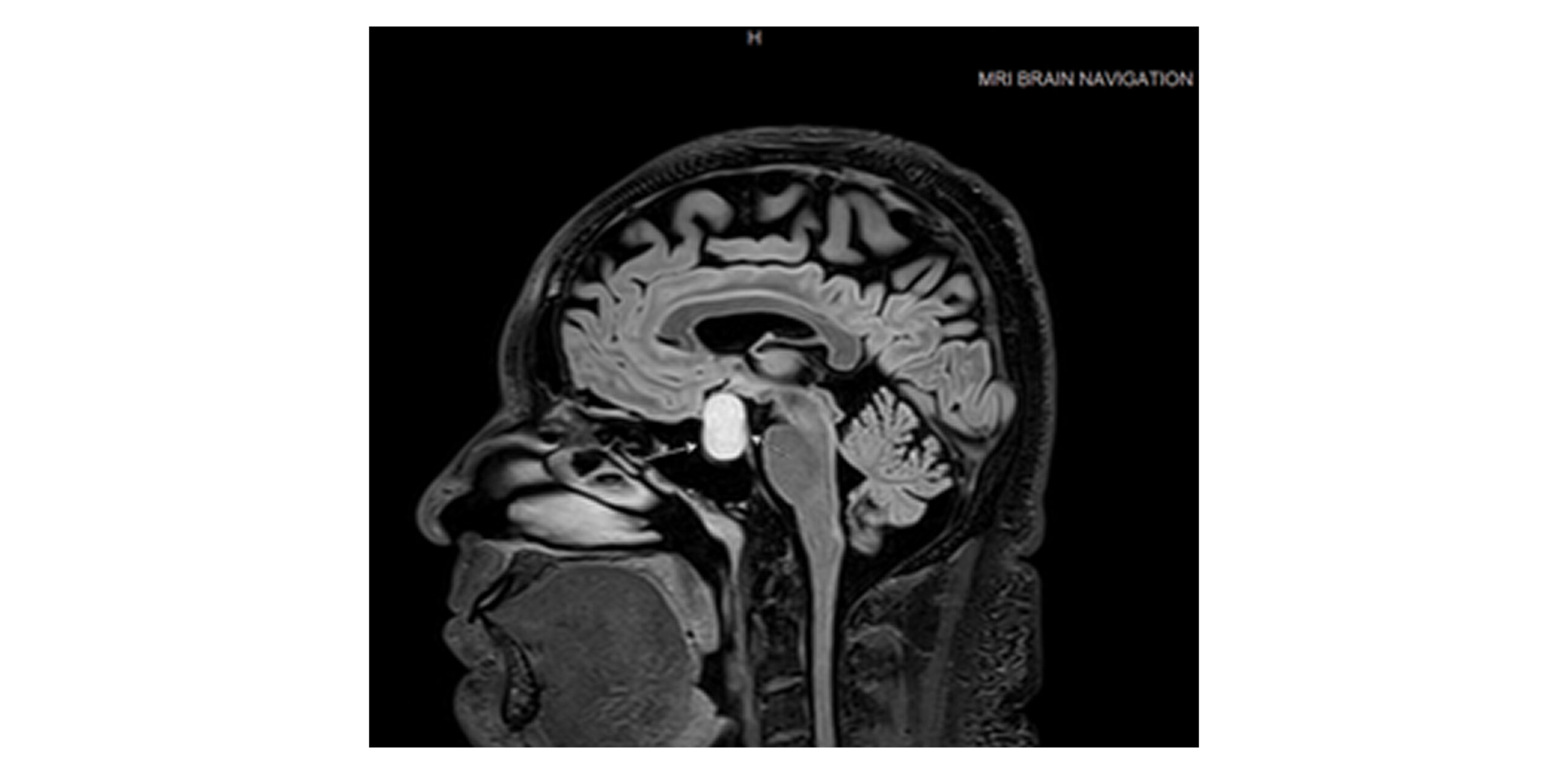
Figure 1: Preoperative MRI of patient A (male) showed a sellar and suprasellar RCC measuring about 2.5 cm, pressing on the optic chiasm
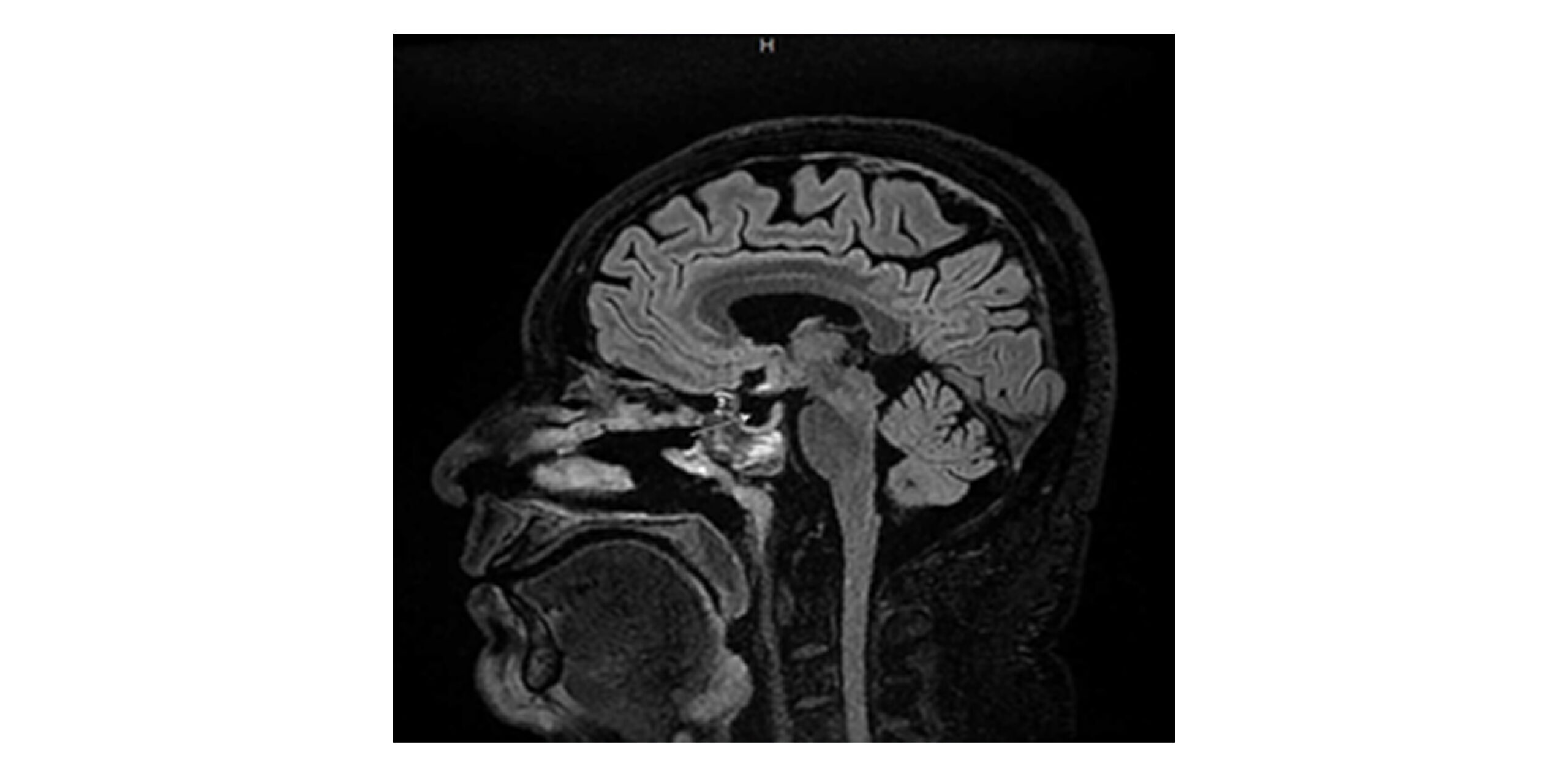
Figure 2: Postoperative MRI brain of patient A (male) demonstrating a clear operative bed and decompression of the optic apparatus with resolution of mass effect
During surgery, it was observed that the cyst contained jelly-like material, no blood, and it got easily separated from the surrounding tissue. After surgery, his headaches subsided, vision returned to normal, and he was started on hormone replacement therapy for the pituitary deficiencies. Follow-up MRI at six months and one year showed no signs of recurrence.
Patient B: A 53-year-old woman presented with dizziness and vertigo. She was previously diagnosed with a pituitary macroadenoma. An MRI was done, which showed a 2 × 1.5 cm cyst in the sellar region extending slightly above the sella, indenting the optic chiasm. She didn’t have any vision problems. The pituitary and stalk were pushed back, but the cavernous sinuses were untouched.
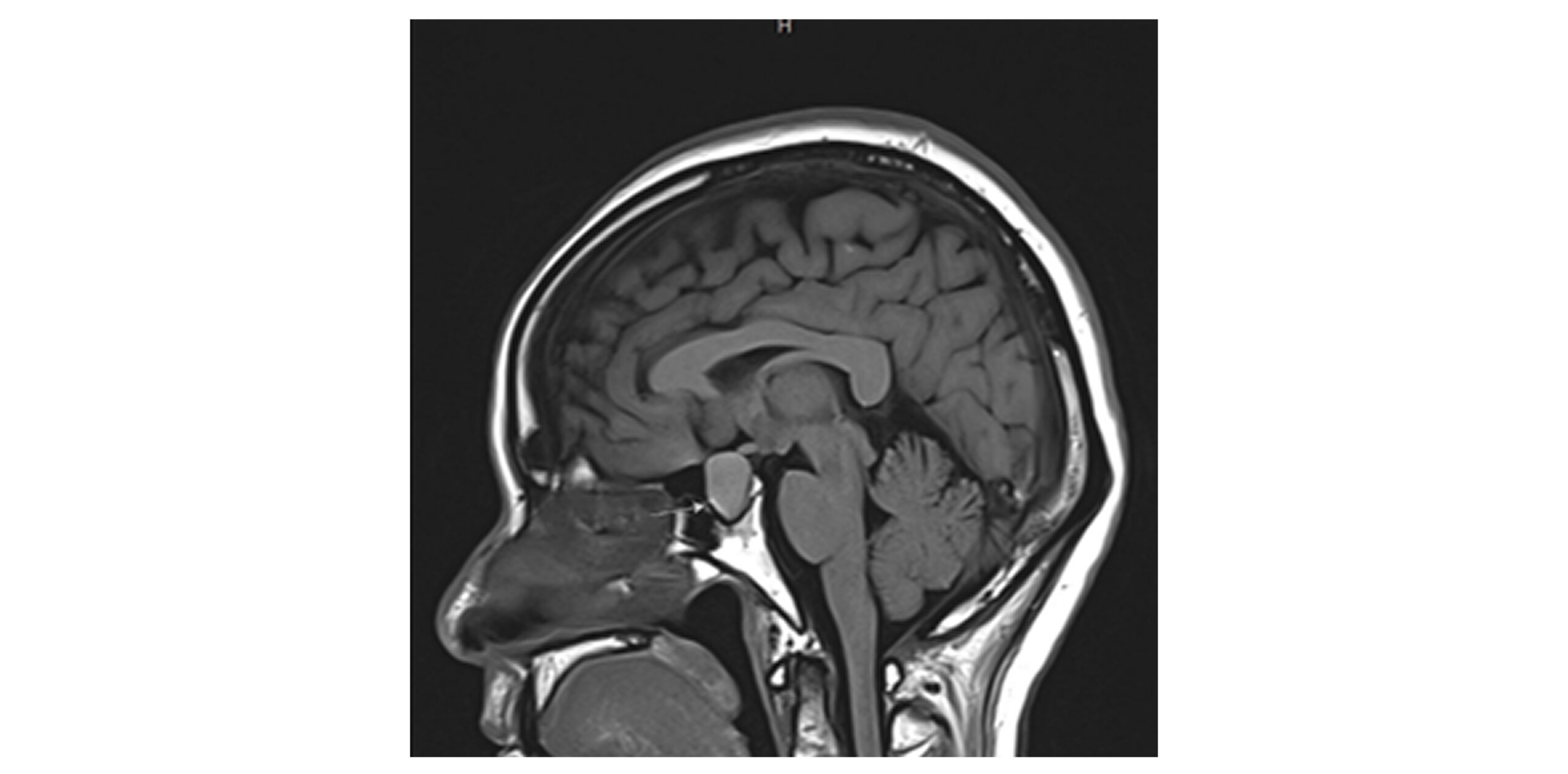
Figure 3: Preoperative MRI brain of patient B (female) demonstrating 2 x 1.5 cm sellar extending into the suprasellar area abducting the optic chiasm with no optic chiasm compression

Figure 4: Preoperative MRI brain navigation of patient B (female) demonstrating a sizable space-occupying lesion in the anterior aspect of the pituitary fossa displacing the pituitary gland and infundibulum posteriorly
Surgery was a bit trickier because of her sinus anatomy. Intraoperatively, the cyst was found to have both blood and protein-rich material and was stuck to the optic chiasm and pituitary stalk. Careful dissection preserved both. Postoperatively, the patient underwent an MRI, and it came out to be normal, confirming full removal and decompression. Histology was done, which confirmed the diagnosis of RCC.
A few months later, an MRI was repeated, which caught a small new cyst (1.5 × 1.2 × 1.6 cm) in the pituitary fossa, lightly pressing on the pituitary stalk. However, she had no symptoms, so we decided to keep monitoring her with regular imaging.
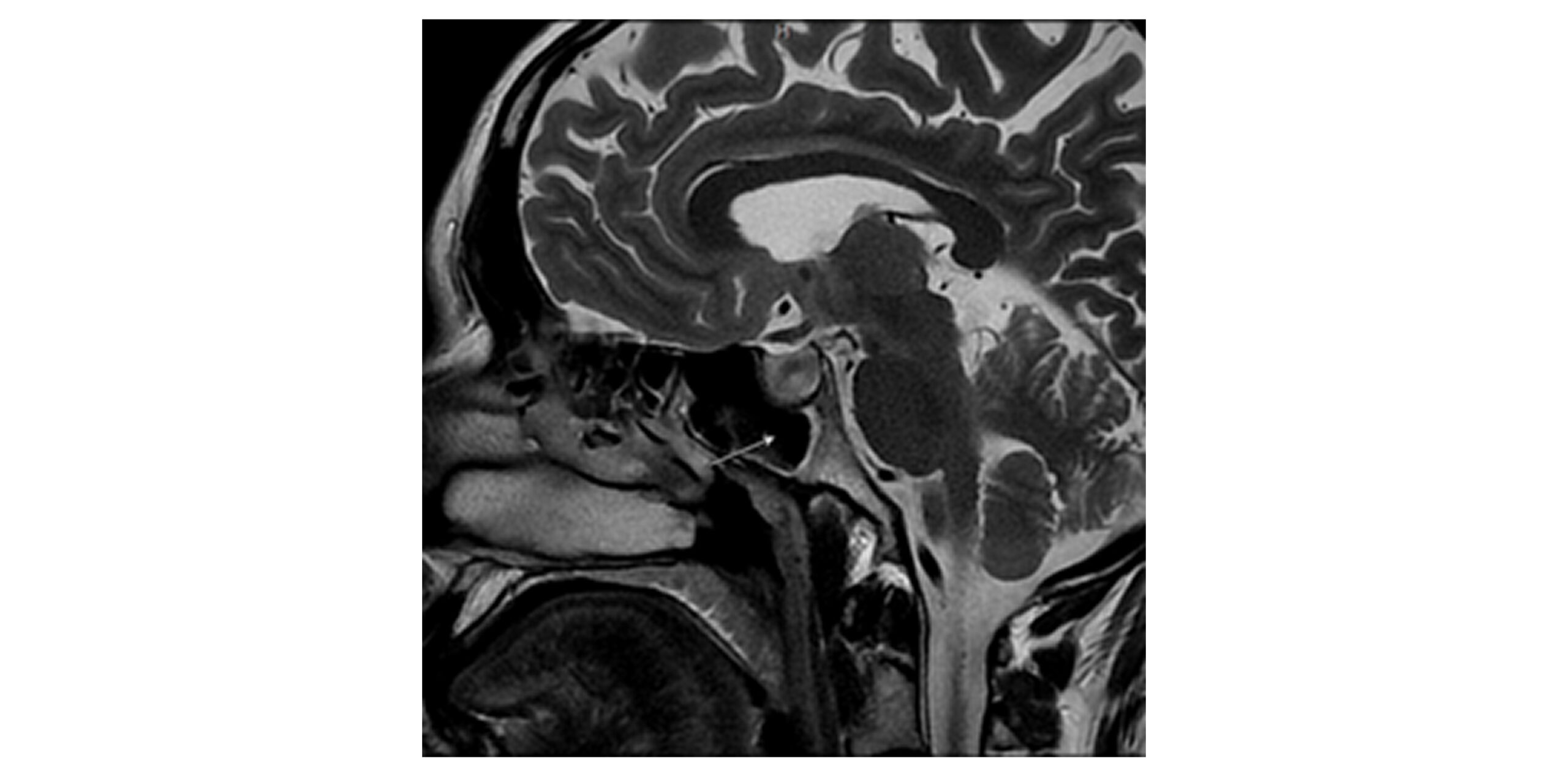

Figure 5 and 6: Postoperative MRI brain of patient B (female) a few months after the follow-up demonstrating a sizable postoperative cyst (1.5 x 1.2 x 1.6 cm) within the pituitary fossa, extending into the suprasellar cistern, causing posterior displacement of the pituitary gland and compressive phenomena on the pituitary stalk
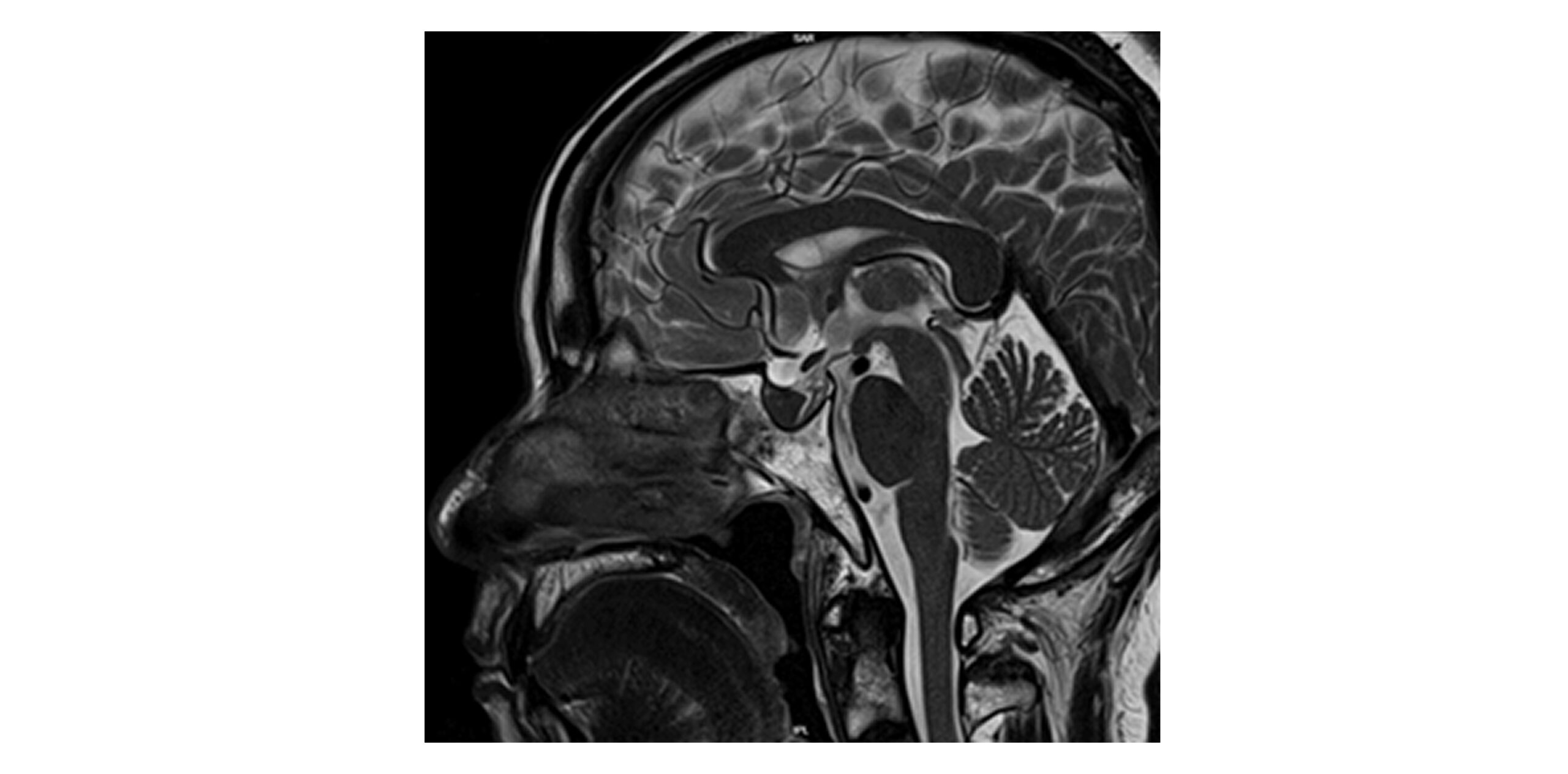
Figure 7: Postoperative MRI brain of patient B (female) few months after the follow-up demonstrating a postoperative cyst in the pituitary fossa measuring 1.0 x 1.3 x 1.4 cm, containing hemorrhagic or proteinaceous material. Cyst demonstrates adhesion to the optic chasm with mild downward traction. Mild compressive phenomena on the pituitary stalk and posterior displacement of the pituitary gland.
Differential diagnosis: In both cases, we considered non-functioning pituitary macroadenoma, craniopharyngioma, and RCC.
Case Management
Both patients had endoscopic transsphenoidal surgery without complications. Afterward, they got steroid coverage and hormone replacement as needed, with regular endocrine and imaging follow-up. Patient A was much better at three months. His headaches were gone, and vision became normal. Patient B showed a small new cyst months later, but she had no vision problems and stayed clinically stable. Endocrine follow-up continues for her hormone management.
Discussion
Most RCCs never cause trouble and are diagnosed accidentally on imaging.[3] But sometimes they grow large enough to press on the optic chiasm or affect hormones, which is when surgery comes into play. Our two patients show how differently these cysts can behave. Even with the same treatment, one patient stayed well, while the other developed a small recurrent cyst a month later. Hence, this case sets a good example that RCCs are unpredictable, and surgical success doesn’t always tell the full story. Long-term follow-up and careful monitoring are key.
A notable challenge in RCC diagnosis is their radiological overlap with non-functioning pituitary macroadenomas, particularly when the cyst contents exhibit proteinaceous or hemorrhagic components, which can alter T1 and T2 signal intensities on MRI, mimicking solid tumors.[8] This was evident in our second patient, whose lesion was initially presumed to be a pituitary macroadenoma until intraoperative and pathological assessment confirmed an RCC.
In our second patient, what we found out during the surgery was quite different from what the MRI had suggested initially.[8-10] This explains the limitations of radiological imaging in such cases. A few months later, the cyst recurred, which was unusual. Other reports show that recurrence can happen in anywhere from none to about one-third of cases, depending on the extension of the cyst wall that is removed. In her situation, the recurrent cyst was again pressing on the optic chiasm, as it was shown in the MRI. That’s why this case emphasizes why careful, long-term follow-up with imaging is so important, even when the initial surgery looks completely successful.[11] Surgical management, typically via a transsphenoidal approach, remains the gold standard for symptomatic RCCs, with gross total resection offering the lowest recurrence risk but potentially higher complication rates if the cyst wall is densely adherent to surrounding structures.[12]
These cases illustrate that RCCs, despite being benign, can present with diagnostic ambiguity, necessitate complex surgical decision-making, and require vigilant long-term surveillance. Looking at both of these cases, it wouldn’t be wrong to say that RCCs can behave unpredictably. Even when patients undergo the same type of surgery, outcomes can be very different. This shows why doctors need to stay alert and continue follow-up over the long term, even when the lesion initially seems low-risk.
Conclusion
RCC is benign in nature, but it may present with significant clinical manifestations, including visual impairment and endocrine dysfunction. These cases highlight the unpredictable postoperative outcomes of RCCs, even when managed with standard surgical approaches. Radiological findings may not be able to rule out RCCs from other sellar lesions thus intraoperative assessment remains crucial for definitive diagnosis. Furthermore, the recurrence rate, even after complete resection, emphasizes the importance of long-term follow-up with serial imaging and endocrine evaluation. A multidisciplinary approach is crucial to monitor outcomes and ensure timely identification of recurrence or persistent dysfunction.
References
- Swain SK. Rathke’s cleft cyst: A case report. J Indira Gandhi Inst Med Sci. 2025;11(2):186-188. doi:10.4103/jigims.jigims_44_24
Crossref | Google Scholar - Farrash FA, Hassounah M, Helmi HA, Othman E, Alotaibi NH. Rathke’s cleft cyst presentation mimicking craniopharyngioma: Case report. Int J Surg Case Rep. 2020;68:104-106. doi:10.1016/j.ijscr.2020.01.035
PubMed | Crossref | Google Scholar - Trifanescu R, Ansorge O, Wass JA, Grossman AB, Karavitaki N. Rathke’s cleft cysts. Clin Endocrinol (Oxf). 2012;76(2):151-160. doi:10.1111/j.1365-2265.2011.04235.x
PubMed | Crossref | Google Scholar - Voelker JL, Campbell RL, Muller J. Clinical, radiographic, and pathological features of symptomatic Rathke’s cleft cysts. J Neurosurg. 1991;74(4):535-544. doi:10.3171/jns.1991.74.4.0535
PubMed | Crossref | Google Scholar - Yoon JW, Jo SK, Cha DR, Cho WY, Kim HK. A case of Rathke’s cleft cyst inflammation presenting with diabetes insipidus. Korean J Intern Med. 2001;16(2):132–135. doi:10.3904/kjim.2001.16.2.132
Crossref | Google Scholar - Osborn AG, Preece MT. Intracranial cysts: radiologic-pathologic correlation and imaging approach. Radiology. 2006;239(3):650-664. doi:10.1148/radiol.2393050823
PubMed | Crossref | Google Scholar - Kim JE, Kim JH, Kim OL, et al. Surgical treatment of symptomatic Rathke cleft cysts: clinical features and results with special attention to recurrence. J Neurosurg. 2004;100(1):33-40. doi:10.3171/jns.2004.100.1.0033
PubMed | Crossref | Google Scholar - Goyal R, Khaing I, Madhusuthanan AK, Dimple, Garg G, Anwar S. Radiological Differentiation of Pituitary Adenomas From Other Sellar Masses: A Systematic Review. Cureus. 2025;17(11):e96793. doi:10.7759/cureus.96793
PubMed | Crossref | Google Scholar - Yang C, Bao X, Liu X, et al. Rathke cleft cyst masquerading as pituitary abscess: A case report. Medicine (Baltimore). 2017;96(10):e6303. doi:10.1097/MD.0000000000006303
PubMed | Crossref | Google Scholar - Cosgrove ME. Rathke cleft cyst presenting as recurrent pituitary apoplexy: An unusual case presentation and clinical course. Neuro Neurosurg. 2020.
Rathke cleft cyst presenting as recurrent pituitary apoplexy: An unusual case presentation and clin… - Dolovac RB, King J, Ovenden C, et al. Impact of sella floor reconstruction on Rathke Cleft Cyst recurrence: a systematic review and meta-analysis. Pituitary. 2025;28(3). doi:10.1007/s11102-025-01521-4
PubMed | Crossref | Google Scholar - Dusick JR, Esposito F, Kelly DF, et al. The extended direct endonasal transsphenoidal approach for nonadenomatous suprasellar tumors. J Neurosurg. 2005;102(5):832-841. doi:10.3171/jns.2005.102.5.0832
PubMed | Crossref | Google Scholar
Acknowledgments
The authors would like to thank the operating room staff, nursing team, radiology department, and endocrinology team for their support in the management of these patients. Their assistance in patient care and coordination is sincerely appreciated.
Funding
This research received no external funding.
Author Information
Corresponding Author:
Safeena Imran
Department of Neurosurgery
King’s College Hospital London, Dubai
Email: [email protected]
Co-Authors:
Umer Shabbir
Department of Emergency Medicine
Midciti Hospital, Karachi, Pakistan
Iqra Kanwal, Muhammad Ibrahim Zahid, Sumaiya Sultana, Muhammad Maaz Hassan
Department of Internal Medicine
Bahria University of Health Sciences Campus, Karachi, Pakistan
Roberto Puxeddu
Department of Surgical Services and Consultant – Otolaryngology
King’s College Hospital London, Dubai
Aneela Darbar
Department of Neurosurgery
King’s College Hospital London, Dubai
Authors Contributions
Safeena Imran conceptualized the case report, coordinated the overall work, and served as the corresponding author. She was responsible for data collection, literature review, manuscript drafting, and submission. Umer Shabbir contributed to the data verification, literature review, manuscript drafting, and critical revision of the content. Iqra Kanwal assisted in the organization of clinical information and manuscript preparation. Muhammad Ibrahim Zahid contributed to data interpretation, literature review, and editing of the manuscript. Sumaiya Sultana assisted in manuscript drafting, formatting, and final review of the content. Muhammad Maaz Hassan contributed to data interpretation, literature review, and manuscript editing. Aneela Darbar supervised the overall clinical work and provided guidance throughout the preparation of the case report. She was the main lead in the surgical management of the patient as a neurosurgeon. Roberto Puxeddu was involved
Ethical Approval
Ethical approval was not required for this case report in accordance with institutional policies, as it describes a retrospective report of clinical cases without experimental intervention.
Conflict of Interest Statement
The authors declare no conflicts of interest.
Guarantor
Safeena Imran is the guarantor of this study and takes full responsibility for the integrity of the data and the accuracy of the data analysis.
DOI
Cite this Article
Imran S, Shabbir U, Kanwal I, et al. When Benign Isn’t Harmless: Divergent Outcomes of Rathke’s Cleft Cysts Presenting with Panhypopituitarism and Optic Apparatus Involvement. medtigo J Neurol Psychiatr. 2026;3(2):e3084325. doi:10.63096/medtigo3084325 Crossref













