






 Author Affiliations
Author Affiliations
Abstract
Background: Human immunodeficiency virus (HIV) self-testing (HIVST) is a promising tool for expanding HIV testing access and increasing early detection, particularly in settings with high HIV burden. This study aims to evaluate the utilization of HIVST among partners of people living with HIV (PLHIV) in Nifas Silk Lafto sub-city, Addis Ababa, Ethiopia, and to explore factors that influence its uptake.
Objective: This study aimed to assess the utilization of HIVST among partners of PLHIV attending ART clinics in Nifas Silk Lafto sub-city, Addis Ababa, and to identify the factors associated with its use.
Methods: A cross-sectional study was conducted with 362 participants who were partners of PLHIV attending ART clinics. Data was collected through face-to-face interviews using structured questionnaires to assess demographic factors, HIV status awareness, utilization of HIVST, and associated barriers. Descriptive and multivariate logistic regression analyses were performed to identify significant factors influencing HIVST uptake. The significance of odds ratios was determined with a 95% confidence interval (CI) and p < 0.05.
Results: HIVST utilization for partner testing was 25.4%, with 92 out of 362 participants using HIVST. Key factors significantly associated with lower utilization included being 40 years or older (Adjusted odds ratio (AOR): 0.14, 95% CI: 0.05, 0.37), having only elementary education (AOR: 0.33, 95% CI: 0.14, 0.76), and secondary education (AOR: 0.33, 95% CI: 0.15, 0.71), and being unaware of the partner’s HIV status (AOR: 0.26, 95% CI: 0.11, 0.59). Additionally, individuals on ART for less than a year were less likely to utilize HIVST (AOR: 0.09, 95% CI: 0.01, 0.67).
Conclusion: Utilization of HIVST among partners of PLHIV remains low. Factors such as age, education level, HIV status disclosure, and ART duration influence testing uptake. Addressing stigma, enhancing awareness, and improving access to HIVST kits are crucial to increasing utilization. These findings can inform targeted HIV prevention strategies in Ethiopia and similar resource-limited settings.
Keywords
Human immunodeficiency virus, Antiretroviral therapy, Human immunodeficiency virus self-testing, Index partner testing, People living with human immunodeficiency virus.
Introduction
Human immunodeficiency virus remains a global health crisis, with an estimated 38.4 million (33.9 million–43.8 million) people living with HIV worldwide. In 2021, approximately 1.5 million new infections and 650,000 AIDS-related deaths were recorded. Alarmingly, 25% of PLHIV are not receiving treatment, and 4.1 million are unaware of their status.[1] In Africa, an estimated 25.7 million individuals live with HIV, with 862,000 new infections reported annually.[2] Eastern and southern Africa exhibit the highest prevalence rates, where many PLHIV remain unaware of their status, driving both transmission and new cases.[2]
Ethiopia, despite significant progress in HIV treatment and prevention, still bears a heavy disease burden, with an estimated 850,000 PLHIV. Antiretroviral therapy (ART) has notably enhanced survival and quality of life for PLHIV, yet HIV testing remains pivotal for reducing transmission and initiating timely treatment.[3] HIVST represents a transformative approach, enabling individuals to perform rapid diagnostic tests (RDTs) using saliva specimens and interpreting their results independently. This strategy addresses barriers such as fear of testing, confidentiality concerns, and costs associated with visiting healthcare facilities. By facilitating early detection, HIVST aligns with the first 95 of the joint united nations programme on HIV/AIDS (UNAIDS) 95-95-95 targets, aiming for 95% of PLHIV to know their status by 2030.[4]
Ethiopia has adopted a phased approach to HIVST implementation, starting with directly assisted testing and semi-restricted unassisted testing, before transitioning to an open-access model via social marketing. This strategy seeks to maximize uptake among eligible populations while maintaining cost-effectiveness.[5] However, despite its potential, HIVST uptake remains suboptimal in many regions, including Ethiopia. While studies from Malawi, Kenya, and South Africa demonstrate the effectiveness of HIVST in increasing testing rates, the Ethiopian context is less well-documented.[6-9]
Statement of the problem: HIVST has been introduced as a crucial entry point for HIV care and treatment. Target populations include partners of index cases enrolled in ART clinics, as well as other high-risk groups.[5] Despite this, studies in urban Ethiopia and across sub-Saharan Africa indicate that HIV testing rates remain below expectations. By 2020, the country had not met the UNAIDS 95-95-95 target, leaving a gap of approximately 46,000 undiagnosed PLHIV.[3,10,11] Addressing this gap is essential, as HIVST has promised to expand testing coverage, particularly among vulnerable populations who face barriers such as stigma and discrimination.[5]
In 2020, Ethiopia implemented guidelines for unassisted oral HIVST targeting specific populations to enhance testing rates, case detection, and early treatment.[5] However, there is limited local data on the uptake, effectiveness, and factors influencing HIVST utilization, underscoring the need for this study.
Significance of the study: This study addresses a critical knowledge gap regarding HIVST uptake in Ethiopia, particularly among partners of PLHIV. By identifying barriers and facilitators, it aims to inform policy and programmatic interventions, contributing to more effective HIV testing strategies.
Key Contributions:
- Early HIV detection and treatment: Early diagnosis enables timely ART initiation, reducing transmission and improving health outcomes.
- Partner involvement in HIV care: Encouraging partners to test for HIV fosters shared responsibility, strengthens support systems, and mitigates stigma.
- Advancing global HIV goals: Insights from this study can support progress toward the UNAIDS 95-95-95 targets by promoting testing and early treatment.
Broader implications: The findings will inform public health strategies to improve access to HIVST, reduce stigma, and enhance education on HIV testing. This evidence can be leveraged to advocate for expanded HIVST availability, integrate self-testing into national programs, and tailor interventions to the needs of underserved populations, particularly in low-resource settings.
Methodology
Study area: The study was conducted in Addis Ababa, the capital city of Ethiopia. Nifas Silk Lafto sub-city, located in the southwestern part of the city, has a total population of 376,880 at an elevation of 2224 meters above sea level. The sub-city is home to 8 health centers, including ART centers, serving a total of 5068 ART clients and PLHIV. For this study, 4 health centers with the highest number of ART clients were included.
Study period: The study was conducted from January 1 to February 28, 2023, among clients in the ART clinics of Nifas Silk Lafto sub-city health centers.
Study design: This institutional-based cross-sectional study assessed HIVST utilization and factors associated with its utilization among partners of PLHIV at Nifas Silk Lafto sub-city health centers from January 1 to February 28, 2023.
Population
- Source Population: All ART users at Nifas Silk Lafto sub-city ART clinics.
- Study Population: Randomly selected eligible clients using multistage sampling during the study period.
Eligibility criteria:
- Inclusion criteria
- Adults aged 18 years and above.
- ART clients attending follow-up during the study period.
- ART clients who volunteered to participate in the study.
- Exclusion criteria
- Clients who were severely ill during the study period.
Sample size determination: The sample size for this study was calculated using the single population proportion formula, which is expressed as:
n = (Zα/2) ² × P × (1-P) / d²
Where:
- n = required sample size
- P = prevalence rate, assumed to be 50% (0.5) to ensure the maximum variability and provide a conservative estimate
- Zα/2 = standard normal value at the 95% confidence level (Z = 1.96)
- d = margin of error (5% or 0.05)
- q = 1-P
Substituting the values:
n = (1.96)² × 0.5 × (1-0.5) / (0.05)²
n = 384
Since the target population is less than 10,000 (N = 5068), the sample size was adjusted using the finite population correction formula:
n_adj = n / (1 + (n / N))
Substituting values:
n_adj = 384 / (1 + (384 / 5068))
n_adj = 357
To account for a potential non-response rate of 10%, an additional 10% was added to the adjusted sample size:
n_final = n_adj + (0.1 × n_adj) = 357 + 36 = 393
Thus, the final sample size was determined to be approximately 393 participants.
Sampling technique: A multi-stage sampling technique was employed for this study. From the eight health centers in the Nifas Silk Lafto sub-city, four were selected using a lottery method. Participants were then proportionally allocated to each health center based on the number of patients attending their ART clinics. To recruit participants, systematic random sampling was applied. A list of monthly patient flow to the ART clinics was used as the sampling frame. With an average of 2534 patients visiting the clinics monthly, and about 31 patients attending daily, every sixth patient on the list was selected after randomly identifying the first participant.
This approach ensured that the sample was representative of the target population while maintaining randomization and proportional allocation across the selected health centers.
Results
Socio-demographic characteristics: A total of 362 participants were included in the study, yielding a response rate of 92.1%, as 31 participants were unable to complete the questionnaire. Among the participants, 162 (44.8%) were aged between 30 and 39 years, and 218 (60.2%) were female. Regarding marital status, 179 (49.5%) were married, while 134 (37%) completed high school. In terms of employment, a significant proportion of the participants, 101 (27.9%), were unemployed, whereas 112 (30.9%) reported having private jobs (Table 1).
| Variable | Frequency | Percentage |
| Age category (years)
<30 30-39 40-49 >50 |
121 162 53 26 |
33.3 44.8 14.7 7.2 |
| Sex
Male Female |
144 218
|
39.8 60.2 |
| Ethnicity
Amhara Oromia Tigray Others (Gurage, Wolayita) |
90 145 65 62 |
24.9 40.0 18.0 17.1 |
| Marital status
Single Married Divorced Widowed
|
116 179 37 30
|
32.0 49.5 10.2 8.3
|
| Religion
Orthdox Catholic Protestant Muslim Others |
179 17 59 91 16 |
49.5 4.7 16. 3 25.1 4.4 |
| Level of education
Cannot read and write Elementary (1-8) Secondary (9-12) Diploma and above |
45 104 134 79 |
12.4 28.8 37.0 21.8 |
| Occupation
Government employee Merchant Private job No job Others |
85 58 112 101 6 |
23.5 16.0 30.9 27.9 1.7 |
Table 1: Socio-demographic characteristics of index cases who had follow-up at ART clinics
Utilization of HIVST: Of all the index cases (n=362), 92 (25.4%) participants had HIV self-test as shown in the figure below (Figure 1).
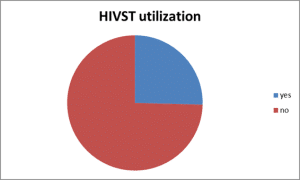
Figure 1: Utilization of HIVST among index cases who had follow-up at ART clinics at Nifas Silk Lafto health centers, Addis (n = 362)
Factors associated with the utilization of HIVST in index partner testing
Educational status of index cases: Analysis by educational status revealed that the practice of self-testing increased with higher levels of education. Among the 92 participants who utilized self-testing, the majority (33, 35.9%) had attained a diploma or higher educational status (Figure 2).
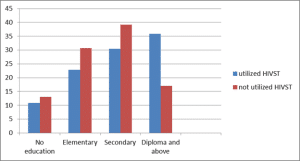
Figure 2: Utilization of HIVST by educational status among index cases who had follow-up at ART clinics at Nifas Silk Lafto health centers, Addis Ababa, Ethiopia, 2023 (n = 362), Jan-Feb 2023
HIV status of partners of index cases: Among the study participants, 222 (61.3%) have HIV positive partners, 39 (10.8%) have negative partners, while 101 (27.9%) of them do not know the sero-status of their partner (Figure 3).
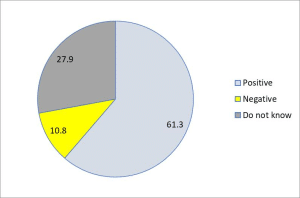
Figure 3: HIV status of partners as disclosed by index cases who had follow-up at ART clinics at Nifas Silk Lafto health centers, Addis Ababa, Ethiopia, 2023 (n = 362)
HIV status disclosure and duration of ART: Majority of the participants knew their status for greater than one year, 249 (68.8%), and 148 (40.9%) had disclosed to their partner, while a quarter of them did not disclose 93 (25.7%). Regarding their ART status, 177 (48.9%) were on ART for 1- 5 years of duration while 20 (5.5%) were on ART for more than 10 years (Table 2).
| Variable | Frequency | Percentage |
| Time of HIV diagnosis?
< 1 year >1 year |
113 249 |
31.2 68.8
|
| To whom have you disclosed your status?
Partner Children Sibling Parents Partner and children Children and parents Partner and parents I have not disclosed yet Other |
148 22 11 61 8 4 4 93 11 |
40.9 6.1 3 16.9 2.2 1.1 1.1 25.7 3
|
| Duration of stay at ART
Less than 1 year 1-5 years 5-10years Greater than 10 years |
113 177 48 20
|
31.2 48.9 13. 3 5.5 |
Table 2: HIV status disclosure and duration of ART of index cases who had follow-up at ART clinics at Nifas Silk Lafto health centers, Addis Ababa, Ethiopia, 2023 (n = 362)
Knowledge and practice of HIVST by index: Most participants (310, 85.6%) reported being advised about index partner testing. Of the participants, 229 (63.3%) had heard about HIVST, with the primary source of knowledge being ART clinics for 213 (58.8%). Among those who had not utilized HIVST for their partners (270, 74.6%), the most cited barrier was the lack of proper pre- and post-test counseling (137, 50.7%). The preferred place for testing was health facilities (276, 76.2%), and most participants (240, 66.3%) preferred to get tested during regular working hours.
For those who utilized HIVST, 70 (76.1%) referred their partners to health facilities after testing. However, the majority (71, 77.2%) reported taking more than one week to return to a health facility with the test result. Regarding knowledge about HIVST, a significant portion of participants (133, 36.7%) had no information about it, and only 144 (39.8%) were aware of the sample collection site. More than half of the participants demonstrated knowledge of the time it takes to obtain results (Table 3).
| Variable | Frequency | Percentage |
| Have you been advised about index partner testing?
Yes No |
310 52 |
85.6 14.4 |
| Have you heard about HIVST?
Yes No |
229 133 |
63. 3 36.7 |
| Where did you hear about HIVST?
ART clinic Media ART clinic and media I have no information Others |
198 11 15 133 5 |
54.7 3.0 4.1 36.7 1.4 |
| Have you ever used HIVST for your partner?
Yes No |
92 270 |
25.4 74.6 |
| Reason for not utilizing HIVST?
Pre and post-test counseling Misinterpreting result Unreliability of result Availability of test |
137 62 19 52 |
50.7 23.0 7.0 19. 3 |
| Place of preference for HIV test?
Health facility Home Community Which time does your partner prefer to get tested at a health facility? Regular working hours Evening Holiday/weekends Did your partner refer to health facility? Yes No Duration after the test Less than a week Greater than a week Is HIVST useful in prevention of HIV transmission? Yes No Perceived benefit of HIVST 1.To know HIV status 2. Interrupt HIV transmission 3.To bring care and support 4.To protect from getting HIV I do not know 2&3 1-4 1&2 3&4 Sample site Saliva Oral mucosa Blood/serum I don’t know 1&2 Time it gets to get result 10 minutes 30 minutes 40 minutes I don’t know |
276 51 35 240 96 26 70 22 21 71 243 119 93 31 20 25 113 29 26 23 2 144 120 56 34 8 64 235 30 33 |
76.2 14.1 9.7 66. 3 26.5 7.2 76.1 23.9 22.8 77.2 67.1 32.9 25.7 8.6 5.5 6.9 31.2 8.0 7.2 6.4 6 39.8 33.1 15.5 9.4 2.2 17.7 64.9 8. 3 9.1 |
Table 3: Knowledge and practice of HIVST by index cases who had follow-up at ART clinics at Nifas Silk Lafto health centers, Addis Ababa, Ethiopia, 2023 (n = 362)
Factors associated with utilization of HIVST in index partner testing: In the bivariate analysis, sex, age, marital status, educational status, partner’s HIV status, duration of diagnosis, whether participants were advised on partner testing, perceived usefulness of HIVST for HIV prevention, duration of ART treatment, and status disclosure were all found to be significantly associated with HIVST utilization at the 20% level of significance.
However, in the multiple logistic regression models, only age, educational status, partner’s HIV status, being advised on partner testing, duration of ART stay, and status disclosure were found to be significantly associated with the utilization of HIVST at the 5% significance level.
Specifically, participants aged 40 years or older were 86% less likely to use HIVST for partner testing (AOR = 0.14, 95% CI: 0.05, 0.37). Participants with an elementary education background were 67% less likely to use HIVST (AOR = 0.33, 95% CI: 0.14, 0.76), while those with secondary education were also 67% less likely (AOR = 0.33, 95% CI: 0.15, 0.71). Additionally, participants whose partners’ HIV status was unknown were 74% less likely to use HIVST (AOR = 0.26, 95% CI: 0.11, 0.59). Partners of participants who had been on ART for less than one year were 91% less likely to use HIVST for testing (AOR = 0.09, 95% CI: 0.01, 0.67) (Table 4).
| Variables | Utilization of HIVST | AOR (95% CI) | p- value | AOR (95% CI) | p-value | |
| Yes n (%) | No n (%) | |||||
| Sex | ||||||
| Male | 30 (32.6) | 114 (42.2) | 0.66(0.40, 1.09) | 0.105 | 0.61(0.32, 1.15) | 0.129 |
| Female | 62 (67.4) | 156 (57.8) | 1 | 1 | ||
| Age (Years) | ||||||
| 30 | 38 (41.3) | 83 (30.7) | 1 | 1 | ||
| 30-39 | 42 (45.7) | 120 (44.4) | 0.76(0.45, 1.29) | 0.312 | 0.39(0.17, 0.91) | 0.028* |
| ³40 | 11 (13.0) | 67 (24.8) | 0.39(0.19, 0.81) | 0.011 | 0.14(0.05, 0.37) | 0.0001* |
| Marital status | ||||||
| Married | 48 (52.2) | 131 (48.5) | 1 | 1 | ||
| Single | 33 (35.9) | 83 (30.7) | 1.09(0.64, 1.82) | 0.759 | 0.62(0.26, 1.45) | 0.267 |
| Others@ | 11 (11.9) | 56 (20.8) | 0.54(0.26, 1.11) | 0.092 | 0.51(0.20, 1.27) | 0.150 |
| Educational status | ||||||
| No education | 10(10.9) | 35(13.0) | 0.40(0.17, 0.92) | 0.030 | 0.43(0.15, 1.20) | 0.106 |
| Elementary | 21(22.8) | 83(30.7) | 0.35(0.18, 0.68) | 0.002 | 0.33(0.14, 0.76) | 0.009* |
| Secondary | 28(30.4) | 106(39.3) | 0.37(0.20, 0.68) | 0.001 | 0.33(0.15, 0.71) | 0.005* |
| Diploma and above | 33(35.9) | 46(17.0) | 1 | 1 | ||
| Partner HIV status | ||||||
| Positive | 74(80.4) | 148(54.8) | 1 | 1 | ||
| Negative | 8(8.7) | 31(11.5) | 0.52(0.23, 1.18) | 0.116 | 0.46(0.17, 1.31) | 0.146 |
| Do not know | 10(10.9) | 91(33.7) | 0.22(0.11, 0.45) | 0.0001 | 0.26(0.11, 0.59) | 0.001* |
| Duration of Diagnosis | ||||||
| =1 year | 8(8.7) | 105(38.9) | 0.15(0.07, 0.32) | 0.0001 | 1.01(0.15, 6.59) | 0.991 |
| 1 year | 84(91. 3) | 165(61.1) | 1 | 1 | ||
| Advised on partner test | ||||||
| Yes | 87(94.6) | 223(82.6) | 1 | 1 | ||
| No | 5(5.4) | 47(17.4) | 0.27(0.10, 0.71) | 0.008 | 0.19(0.06, 0.57) | 0.003* |
| Usefulness of HIVST | ||||||
| Yes | 70(76.1) | 173 (64.1) | 1 | 1 | ||
| No | 22(23.9) | 97(35.9) | 0.56(0.33, 0.96) | 0.036 | 0.71(0.35, 1.43) | 0.338 |
| Duration on ART | ||||||
| 1year | 8(8.7) | 109(40.4) | 0.19(0.08, 0.46) | 0.0001 | 0.09(0.01, 0.67) | 0.018* |
| 1-5year | 65(70.7) | 112(41.5) | 1.50(0.81, 2.76) | 0.196 | 0.99(0.45, 2.20) | 0.981 |
| 5year | 19(20.6) | 49(18.1) | 1 | 1 | ||
Table 4: Factors associated with utilization of HIVST in index partner testing in ART clinics of Nifas Silk Lafto health centers of Addis Ababa, Ethiopia, 2023 (n= 362), Jan-Feb 2023
Discussion
The study assessed the utilization of HIVST and associated factors among partners of PLHIV who have ART follow-ups at Nifas Silk Lafto sub-city in Addis Ababa, Ethiopia. The findings revealed that the magnitude of HIVST utilization by index cases and their partners was 92 (25.4%). This utilization rate was lower compared to a study conducted in Malawi (77%), but it was somewhat comparable to findings from Kule refugee camp in Gambella, Western Ethiopia (49.3%) and a study in Senegal among first-time testers from high-risk populations, which reported a rate of 36.8%.[10-13]
The lower uptake of HIVST for index partner testing compared to the UNAIDS 95-95-95 target may be attributed to the introduction of HIVST as a new testing modality.[4] Utilization is dependent on healthcare providers’ willingness to offer the test, as kits are currently available only within health institutions.
Factors Associated with HIVST Utilization
Age: Multivariate logistic regression analysis revealed that age was significantly associated with HIVST utilization. Participants aged 30–39 years and those aged ≥40 years were 61% and 86% less likely, respectively, to use HIVST for partner testing compared to participants aged <30 years. These findings align with a study conducted in Nepal, where younger participants demonstrated greater utilization of HIV testing services.[14] However, this contrasts with a study in western Ethiopia, where older age groups showed higher rates of index partner testing.[15] The disparity may be due to younger individuals being more receptive to healthcare workers’ guidance at ART clinics.
Educational status: Participants with secondary education were 67% less likely to use HIVST for partner testing compared to those with a diploma or higher education. This finding aligns with studies conducted in Kenya and western Ethiopia, which reported similar trends.[15,16] Higher educational levels may enhance understanding of HIV transmission, reduce stigma, and highlight the benefits of partner testing. Education is recognized as a significant social determinant of health.[17]
Partner testing counseling: Participants who were not advised about partner testing during ART visits were 81% less likely to utilize HIVST. This may be due to a lack of consistent exposure to information on the value of partner testing for HIV prevention and early treatment. This finding underscores the importance of providing strong counseling, particularly for individuals who have not disclosed their status to their partners. Strengthening counseling in high-risk areas could help reduce transmission and late diagnosis, contributing to the UNAIDS 95-95-95 goal.[4]
Partner HIV status and ART duration: The study found that participants who were unaware of their partner’s HIV status were 74% less likely to use HIVST kits. Additionally, partners of participants who had been on ART for less than one year were 91% less likely to undergo HIVST. These findings are consistent with studies conducted in western Ethiopia and Jimma.[15,18]
Status disclosure: Among participants who utilized HIVST for partner testing, 90 out of 92 had disclosed their HIV status to their partner. Although status disclosure was not included in the multivariate analysis model, it was identified as a significant factor influencing HIVST utilization. A study from Indonesia also highlighted the importance of status disclosure in facilitating index partner testing.[19] Disclosure fosters ART adherence through psychosocial support, creates a favorable environment for partner testing, and encourages early medical care and treatment.[20,21]
Global perspective on HIVST utilization: Globally, the utilization rate of HIVST varies widely. For instance, in Malawi, HIVST uptake has reached 77% due to integrated national HIVST programs, while Senegal reports a more modest 36.8.[10,22] The variation in uptake underscores the influence of local context, including accessibility, stigma, and public health campaigns.
In South Africa, HIVST has been promoted in urban areas, but uptake remains uneven, reflecting differences in access and socioeconomic status.[22] Studies from Kenya, Uganda, and Senegal suggest that stigma remains a significant barrier to HIVST uptake, particularly in conservative communities where testing for HIV is stigmatized.[16,20,13]
Key factors influencing HIVST utilization globally: Several common factors have emerged in global research that influence HIVST utilization. These include:
- Age: Younger individuals are more likely to engage with HIVST. This finding is consistent with research from Nepal and Brazil, where younger populations show higher uptake of HIVST.[6,14]
- Education: Higher levels of education correlate with greater HIVST utilization. Studies from Kenya and Uganda have found similar trends, with more educated individuals showing greater awareness and use of HIV testing technologies.[16,20]
- Partner HIV Status Awareness: Individuals who know their partner’s HIV status are more likely to use HIVST. This finding has been observed in Zimbabwe, Kenya, and South Africa, where couples’ knowledge of each other’s HIV status promotes shared responsibility for HIV testing.[8,16,22]
- Duration on ART: People who are newly diagnosed and on ART for less than one year are less likely to use HIVST. This is consistent with findings from Botswana and South Africa, where individuals in the early stages of ART treatment tend to delay engagement with HIV testing.[22]
- Disclosure of HIV Status: HIV status disclosure to partners is strongly associated with HIVST use. This has been reported in Brazil, India, and Kenya, where individuals who openly discuss their HIV status with their partners are more likely to test for HIV.[6,16]
Implications for global HIV prevention strategies: The findings from this study have important implications for global HIV prevention strategies
- Stigma reduction: HIV-related stigma remains a significant barrier in many parts of the world, including Ethiopia. Public health campaigns must work to reduce stigma and normalize HIV testing, particularly for high-risk groups.
- Access to HIVST kits: Making HIVST kits more widely available is crucial. This can be done through healthcare facilities, mobile health units, and pharmacies.
- Educational campaigns: Tailoring HIV education to different populations, including those with lower educational attainment, can improve awareness and increase HIVST use.
- Targeting high-risk groups: Priority should be given to high-risk groups, such as individuals with lower educational levels and newly diagnosed patients, to encourage their engagement with HIVST.
- Couple-based HIV testing: Promoting HIV testing within couples can foster open communication and mutual support. Programs should encourage couple-based HIV testing and provide counseling services to facilitate status disclosure.
Strengths: This is the first study of its kind in the study area, providing valuable insights into the utilization of HIVST among partners of PLHIV in urban Ethiopia. The study was conducted in multiple ART clinics, providing a diverse sample of participants and ensuring the findings are relevant to a broad population of ART clients.
Limitations: Since the study relied on self-reported data, there may be recall bias, especially regarding past utilization of HIVST. The cross-sectional nature of the study prevents the establishment of causal relationships between the factors and HIVST utilization. HIVST kits were not provided during the study period, meaning the study assessed perceived rather than actual utilization, which could affect the accuracy of the findings.
Recommendations:
- Ministry of Health: Develop health education programs that specifically target individuals with lower educational backgrounds, addressing the importance of partner testing and promoting HIVST as a feasible alternative for HIV testing. Ensure that HIVST kits are made widely available at health facilities, particularly for clients who have not tested their partners.
- Health Facilities: Health facilities should develop strategies to distribute HIVST kits to ART clients who have not disclosed their status to their partners, ensuring that information is tailored to the client’s level of education and understanding. Encourage regular counseling sessions on the importance of partner testing and status disclosure, creating an environment where ART clients feel supported in discussing HIV-related matters with their partners.
By addressing these factors, it is possible to increase HIVST utilization and contribute to achieving the 95-95-95 goal of the UNAIDS strategy, which aims to increase testing, treatment, and viral suppression among PLHIV.
Conclusion
The findings of this study highlight several critical insights into HIVST utilization among partners of PLHIV in Addis Ababa, Ethiopia. While the utilization rate of 25.4% remains lower than expected, it provides a valuable snapshot of the current state of HIVST uptake in Ethiopia and offers important lessons for global HIV prevention efforts. The utilization of HIVST for partner testing was found to be low among partners of PLHIV at Nifas Silk Lafto sub-city in Addis Ababa, Ethiopia. Key factors negatively associated with utilization include older age, lower educational status, lack of awareness of the partner’s HIV status, being on ART for less than one year, and failure to disclose HIV status to partners.
References
- UNAIDS. Global HIV & AIDS statistics-Fact sheet. 2022. Global HIV & AIDS statistics-Fact sheet
- Ethiopian Public Health Institute. HIV Related Estimates and Projections in Ethiopia for the Year 2020 and 2021.
HIV Related Estimates and Projections in Ethiopia for the Year 2020 and 2021 - Central Statistical Agency. The 2016 Ethiopian Demographic and Health Survey (EDHS). 2017. The 2016 Ethiopian Demographic and Health Survey (EDHS)
- World Health Organization. Global update on HIV treatment 2013: results, impact, and opportunities. 2013.
Global update on HIV treatment 2013: results, impact, and opportunities - Ng OT, Chow AL, Lee VJ, et al. Accuracy and user-acceptability of HIV self-testing using an oral fluid-based HIV rapid test. PLoS One. 2012;7(9):e45168. doi:10.1371/journal.pone.0045168 PubMed | Crossref | Google Scholar
- Jordão T, Magno L, Pereira M, et al. Willingness of health care providers to offer HIV self-testing from specialized HIV care services in the northeast of Brazil. BMC Health Serv Res. 2022;22(1):713. doi:10.1186/s12913-022-08091-2
PubMed | Crossref | Google Scholar - MacPherson P, Lalloo DG, Webb EL, et al. Effect of optional home initiation of HIV care following HIV self-testing on antiretroviral therapy initiation among adults in Malawi: a randomized clinical trial. JAMA. 2014;312(4):372-379. doi:10.1001/jama.2014.7182 PubMed | Crossref | Google Scholar
- Thirumurthy H, Masters SH, Mavedzenge SN, Maman S, Omanga E, Agot K. Promoting male partner HIV testing and safer sexual decision making through secondary distribution of self-tests by HIV-negative female sex workers and women receiving antenatal and post-partum care in Kenya: a cohort study. Lancet HIV. 2016;3(6):e266-e274. doi:10.1016/S2352-3018(16)00041-2 PubMed | Crossref | Google Scholar
- Napierala S, Desmond NA, Kumwenda MK, et al. HIV self-testing services for female sex workers, Malawi and Zimbabwe. Bull World Health Organ. 2019;97(11):764-776. doi:10.2471/BLT.18.223560
PubMed | Crossref | Google Scholar - Kahabuka C, Plotkin M, Christensen A, et al. Addressing the First 90: A Highly Effective Partner Notification Approach Reaches Previously Undiagnosed Sexual Partners in Tanzania. AIDS Behav. 2017;21(8):2551-2560. doi:10.1007/s10461-017-1750-5 PubMed | Crossref | Google Scholar
- Izudi J, Okoboi S, Lwevola P, Kadengye D, Bajunirwe F. Effect of disclosure of HIV status on patient representation and adherence to clinic visits in eastern Uganda: A propensity-score matched analysis. PLoS One. 2021;16(10):e0258745. doi:10.1371/journal.pone.0258745 PubMed | Crossref | Google Scholar
- Wegu Y, Sileshi T, Melis T. Assessment of Index Case Family Testing Among Adults Attending Art Clinic at Kule Refugee Camp, Southwest Ethiopia: 2021. HIV AIDS (Auckl). 2022;14:13-21. doi:10.2147/HIV.S344100
PubMed | Crossref | Google Scholar - Lyons CE, Coly K, Bowring AL, et al. Use and Acceptability of HIV Self-Testing Among First-Time Testers at Risk for HIV in Senegal. AIDS Behav. 2019;23(Suppl 2):130-141. doi:10.1007/s10461-019-02552-2 PubMed | Crossref | Google Scholar
- Sharma B, Nam EW. Role of Knowledge, Sociodemographic, and Behavioral Factors on Lifetime HIV Testing among Adult Population in Nepal: Evidence from a Cross-Sectional National Survey. Int J Environ Res Public Health. 2019;16(18):3311. doi:10.3390/ijerph16183311 PubMed | Crossref | Google Scholar
- Edosa M, Merdassa E, Turi E. Acceptance of Index Case HIV Testing and Its Associated Factors Among HIV/AIDS Clients on ART Follow-Up in West Ethiopia: A Multi-Centered Facility-Based Cross-Sectional Study. HIV AIDS (Auckl). 2022;14:451-460. doi:10.2147/HIV.S372795 PubMed | Crossref | Google Scholar
- Mwangi J, Miruka F, Mugambi M, et al. Characteristics of users of HIV self-testing in Kenya, outcomes, and factors associated with use: results from a population-based HIV impact assessment, 2018. BMC Public Health. 2022;22(1):643. doi:10.1186/s12889-022-12928-0 PubMed | Crossref | Google Scholar
- World Health Organization. A conceptual framework for action on the social determinants of health. 2010. A conceptual framework for action on the social determinants of health
- Tesfaye T, Darega J, Belachew T, Abera A. HIV positive sero-status disclosure and its determinants among people living with HIV /AIDS following ART clinic in Jimma University Specialized Hospital, Southwest Ethiopia: a facility- based cross-sectional study. Arch Public Health. 2018;76:1. doi:10.1186/s13690-017-0251-3
PubMed | Crossref | Google Scholar - Rahmalia A, Wisaksana R, Laga M, van Crevel R, Peeters Grietens K. Facilitators and barriers to status disclosure and partner testing of women living with HIV in Indonesia: a mixed methods study. Sex Reprod Health Matters. 2022;30(1):2028971. doi:10.1080/26410397.2022.2028971 PubMed | Crossref | Google Scholar
- Izudi J, Okoboi S, Lwevola P, Kadengye D, Bajunirwe F. Effect of disclosure of HIV status on patient representation and adherence to clinic visits in eastern Uganda: A propensity-score matched analysis. PLoS One. 2021;16(10):e0258745. doi:10.1371/journal.pone.0258745 PubMed | Crossref | Google Scholar
- Njau B, Covin C, Lisasi E, et al. A systematic review of qualitative evidence on factors enabling and deterring uptake of HIV self-testing in Africa. BMC Public Health. 2019;19(1):1289. doi:10.1186/s12889-019-7685-1
PubMed | Crossref | Google Scholar - Joseph Davey DL, Wall KM, Naidoo N, et al. HIV testing and linkage to ART following secondary distribution of HIV self-test kits to male partners of women living with HIV: a pilot randomized control trial in Mpumalanga, South Africa. J Int AIDS Soc. 2022;25(6):e25937. doi:10.1002/jia2.25937 PubMed | Crossref | Google Scholar
Acknowledgments
We express our sincere gratitude to everyone who contributed to the development and preparation of this research. Special thanks to Prof. Aster Tsegaye for her invaluable support throughout the process. We also acknowledge Santé Medical College for facilitating this research and the study participants for their cooperation. Our appreciation extends to the Nifas Silk Lafto sub-city Health Office for providing essential information.
Funding
Not reported
Author Information
Corresponding Author:
Henok Bahru Wodajeneh
Department of Internal Medicine
Enchini Hospital, Oromia, Ethiopia
Email: tigidb@gmail.com
Co-Authors:
Tsion Girma Areda
Department of General Practitioner
Addis Ababa Health Bureau, Addis Ababa Ethiopia
Dereje Nigatu Elala
Department of Internal Medicine
Sheik Hassen Yabare Specialized Referral Teaching Hospital, Jigjiga, Ethiopia
Tigist Desta Beyera
Department of Medicine
Armauer Hansen Research Institute, Ethiopia
Ashenafi Tesfaye Bedada
Department of General Surgery
Menelik II Specialized Hospital, Ethiopia
Ashenafi Negash Tekle
Department of Orthopedics and Traumatology
St. Paul’s Hospital Millennium Medical College Addis Ababa, Ethiopia
Kebron Yihenew Getnet
Department of Medicine
Jigjiga Karamara General Hospital, Ethiopia
Surafel Bahru Wodajeneh
Department of Medicine
Bethel Medical College, Addis Ababa, Ethiopia
Authors Contributions
All authors contributed to the conceptualization, investigation, and data curation by acquiring and critically reviewing the selected articles. They were collectively involved in the writing – original draft preparation, and writing – review & editing to refine the manuscript. Additionally, all authors participated in the supervision of the work, ensuring accuracy and completeness. The final manuscript was approved by all named authors for submission to the journal.
Ethical Approval
The study protocol was reviewed, and ethical clearance was obtained from Santé Medical College and Addis Ababa Health Bureau. A support letter was secured from the Addis Ababa Health Bureau for the respective health centers. Informed consent was obtained from each study participant via signature prior to the interview, and the objectives of the study were explained to them. Participants were informed of their right to withdraw from the study at any time or not to answer any question if they did not wish to. Confidentiality was maintained at all levels of the study. Participation in the study was voluntary.
Conflict of Interest Statement
The author declares no conflict of interest.
Guarantor
None
DOI
Cite this Article
Henok BW, Tsion GA, Dereje NE, et al. Utilization of HIV Self-Testing and Associated Factors Among Partners of People Living with HIV in Nifas Silk Lafto Sub-City, Addis Ababa, Ethiopia: A Comparative Global Analysis. medtigo J Med. 2024;2(4):e30622461. doi:10.63096/medtigo30622461 Crossref













