






 Author Affiliations
Author Affiliations
Abstract
Background: The non-urgent population uses several critical resources in emergency services, which challenge their efficiency. A better understanding of the non-urgent patient will inform policies and programs that can reduce the burden on emergency services while providing alternative care options for this patient population. This scoping review aims to examine and identify gaps in the existing literature across multiple countries that represent diverse healthcare systems with varying levels of development and healthcare access. The goal is to understand what motivates this population to seek emergency-level care and how this affects emergency services.
Methodology: We systematically searched 5 electronic databases (CINAHL, MEDLINE, PubMed, PsycINFO, and Scopus) following the steps outlined by the Joanna Briggs Institute Manual of Evidence Synthesis and reporting guidelines from the preferred reporting items for systematic reviews and meta-analyses extension for scoping reviews (PRISMA-ScR) checklist.
Results: We selected 47 studies for review whose publication dates ranged from 2000 to 2024. The selection included 23 countries with high, upper-middle, and lower-middle incomes. The study designs primarily consisted of surveys and questionnaires, interviews, chart reviews, and database analyses. Thematic analysis revealed 12 motivation themes, 10 proposed solution themes, various methods of triage, and implications for non-urgent use in emergency services.
Conclusion: The study revealed a research gap in low-income countries and emphasized the need for context-specific solutions, improved primary care access, and enhanced health literacy. These findings have important implications for policy, practice, and future research addressing global non-urgent emergency rooms (ER) use.
Keywords
Non-urgent patients, Emergency department, Motivation, Electronic databases, Thematic analysis.
Introduction
Emergency departments (EDs) are important access points across international health care systems. Misuse of emergency services is a significant health care challenge faced by hospitals and emergency services worldwide. There is an established but growing concern about how patients utilize ER and emergency medical services (EMS). The data trend reported by the Healthcare Cost and Utilization Project between 2006 and 2019 shows that the total volume of ER patients rose by approximately 19% across the United States. During that timeframe.[1] In 2019, 123 million of the 143.4 million patients seen in the ER were considered “treat and street,” leaving approximately 15% of patients considered emergent or urgent.[1] The primary function of the ER and EMS is to treat life-threatening emergent or urgent cases that require a rapid diagnosis and urgent or emergent treatment. The U.S. Department of Health and Human Services published a report highlighting the trends in ER utilization between 2009 and 2018. The results show that the use of the ER is trending upward and reveal concern for ED reliance by mental health patients, as well as a subset of patients known as “superusers.” It also highlights research showing that efforts to reduce the non-urgent patient population through various means have, thus far, been largely ineffective.[2]
The changing culture of the non-urgent ED patient represents a complex shift influenced by patient-related factors and healthcare access. The high volume of non-urgent patients seeking emergency-level care can negatively impact emergency services in several ways, including overcrowding, delays in care, increased wait times, adverse events, resource strains, and rising care costs in EDs.[3,4] Several studies indicate a global problem with ED use by non-urgent patients. McIntyre et al.[5] published a study in 2023 referencing studies from multiple countries examining non-urgent use of the ED. Examining cross-cultural differences in health care as it relates to non-urgent patients seeking emergency care is important because differing health care systems may influence what motivates this patient population.
Currently, there are 195 independent sovereign nations in the world, and as such, there is a wide spectrum of health care delivery systems.[6] Despite the varying degrees of health care delivery, four universally recognized health care systems make up most systems used worldwide. These are known as the Beveridge, Bismarck, National Healthcare Insurance, and Out-of-Pocket models.[7] It is also well-documented that developed and industrialized countries have more well-established health care systems. While there is no definitive list of countries considered “wealthy,” some common ways economists and analysts define the wealth of a nation include those with high-income as defined by The World Bank with a gross national income per capita of $13,846 or more in 2024, those with advanced economies as defined by the International Monetary Fund’s World Economic Outlook report which focuses on the macroeconomic and financial stability of a nation, or those who are part of the Organization for Economic Cooperation and Development which provides evidence-based policy analysis and economic data through its bi-annual economic surveys.[8-10]
Wealthier nations and urban centers within middle-income countries tend to have more advanced and standardized health care systems with a formal health care structure and EDs.[11] In contrast, impoverished nations struggle with instability and structured health care provisions. Many of these underdeveloped countries face significant challenges in providing adequate health care (including emergency medical care) for their populations. These challenges include a lack of infrastructure, political instability, corruption, and vulnerability to natural disasters and climate change. Formal EDs, prehospital care, and emergency transport are relatively rare in poorer countries. If they do exist, they are highly under-resourced, especially in rural areas with limited health care access.[12-14] Few published studies have analyzed ED use in hospitals of developing nations, and none have addressed non-urgent patients specifically. More studies linking non-urgent patients to EDs are available from well-developed nations, including but not limited to Canada, the United Kingdom (UK), Australia, the U.S., Saudi Arabia, France, Spain, Switzerland, and Germany.[15-18] This review aims to uncover cross-cultural differences in the motivation of non-urgent patients seeking emergency care from various countries, regardless of income status.
This scoping review aims to cross-culturally map the available peer-reviewed literature to describe why adults use the ER for non-urgent problems. Increasing our understanding of these motivators will inform stakeholders and propose solutions and alternative care pathways to reduce the burden on emergency services.
Scoping review question
- The main research question is: What existing literature is available to examine what motivates non-urgent patients from different countries to seek an emergency level of care?
- The research sub-question is: How does the non-urgent population affect emergency medical systems?
Methodology
Our search strategy followed the steps outlined in the Joanna Briggs Institute (JBI) Manual of Evidence Synthesis and reporting guidelines from the PRISMA-ScR checklist.[19,20] This standardized methodology helped to determine the extent, range, and nature of research conducted in this area and provides transparency and replicability of the review process.
Inclusion criteria: The review included full-text, peer-reviewed articles examining adults aged 18 and older identified as non-urgent by varying triage methods and seeking emergency-level care. We particularly emphasized understanding patients’ motivations for non-urgent ED visits. We limited our review to studies in English or translated into English, acknowledging this as a potential limitation that may have excluded valuable insights from non-English-speaking countries.
In addition to patient-focused studies, we included research examining the operational, financial, or other effects of non-urgent patients on emergency services. We also considered relevant prehospital medicine studies if they aligned with our stated objectives. To generate comprehensive insights into the variables most strongly associated with inappropriate ED use, we included qualitative, quantitative, and mixed-methods studies in our review.
Exclusion criteria: We designed our exclusion criteria to maintain focus and avoid potential confounding factors. We excluded studies concentrating on specific complaints (such as chest pain or abdominal pain) or imaging techniques (like Computed Tomography scan (CT) scans or magnetic resonance imaging (MRI)), as these might skew our understanding of medical specialties or conditions, potentially obscuring broader motivational factors. Notably, we also excluded studies examining ED use during the coronavirus disease 2019 (COVID-19) pandemic. We based this decision on several factors: the unprecedented nature of the pandemic dramatically altered healthcare-seeking behaviors and ED operations; many countries implemented temporary measures that changed usual care pathways; and the pandemic created a general atmosphere of health anxiety, potentially inflating perceptions of symptom urgency. Additionally, at the time of our review, the full impact of COVID-19 on long-term ED utilization patterns was not yet clear. By excluding these studies, we aimed to focus on more stable, long-term patterns of non-urgent ED use, providing a baseline understanding for future research comparing how crises might alter these established patterns.
We also chose to exclude pediatric studies, recognizing that ED use for children often follows different patterns and motivations, typically driven by parental decision-making rather than the patient’s own choices. Including these studies would have introduced variables beyond the scope of our research questions.
Search strategy and information sources: We used keywords, index terms, and medical subject headings (MeSH) terms for searching in 5 academic databases: CINAHL, MEDLINE, PubMed, PsycINFO, and Scopus. We did not search gray literature due to time limits, and we acknowledge that this selection might not capture all studies published in non-indexed journals. However, this selection provided a robust and comprehensive foundation for our scoping review.
Source of evidence selection: We utilized Zotero software version 6.0.30 (provided by ATSU, AZ, U.S.) for reference management. We uploaded all selected studies into the management system and removed all duplicates. We have summarized the study selection process in a PRISMA flow diagram in Figure 1.
Critical appraisal of individual sources of evidence: We evaluated the quality of each study based on several criteria using the JBI Critical Appraisal checklist for qualitative research, analytical cross-sectional studies, and mixed methods research. We also used the PRISMA-ScR critical appraisal and reporting guidelines.[21,22]
Data extraction: We used Covidence systematic review software (VERITAS Health Innovation, Melbourne, Australia) for data extraction. Using Covidence was a strategic choice to enhance efficiency and reduce the potential for human error. Our data extraction process was designed to be iterative, as recommended by the JBI methodology.[23]
Data items: For each source, we extracted data variables, including standard details (title, date of publication, authors, study design, sample size, and methods), country of study, type of health care system, study aims and objectives, definition, or criteria used to define “non-urgent”; sample size, and main themes, motivations, or factors examined or identified for care-seeking behaviors; knowledge gaps identified; and implications and recommendations for practice, policy, or research based on the study findings.
Analysis and presentation of results: We synthesized data using a descriptive qualitative approach and thematic analysis, chosen for its alignment with our exploratory research questions and flexibility in handling diverse study designs and contexts. Thematic analysis proved particularly valuable given the heterogeneity of included studies, encompassing quantitative, qualitative, and mixed-methods research from 23 countries with varying health care systems.
Results
The initial search yielded 1,204 results. We excluded 728 records that were duplicates or were irrelevant to the inclusion or exclusion criteria. We reviewed 214 studies for eligibility. After reading abstracts and full texts, we excluded 167 articles. Reasons for exclusion included studies that were not relevant (did not discuss non-urgent patients, wrong study design, did not discuss motivation, discussed a specific complaint (the study was complaint-driven only), were not translatable to English, had the wrong comparators, or were unavailable. We recorded the selection process in a PRISMA flow diagram illustrated in Figure 1.
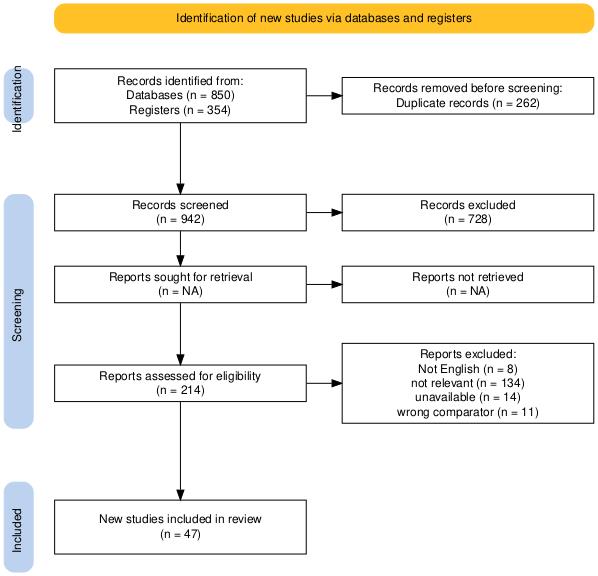
Figure 1: PRISMA flow diagram
Distribution by publication dates: Dates of publication ranged from 2000 to 2024. The distribution of studies was low for the first 10 years but then showed a general trend of increasing publications over time, with more frequent publications in more recent years. Results are presented in Figure 2.
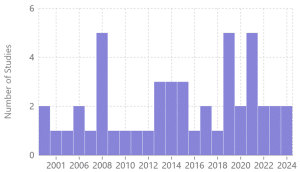
Figure 2: Distribution of studies by year
Distribution by country and continent: The study selection included 23 countries containing a mix of high, upper-middle, and lower-middle incomes. Of the studies selected, 74% were from high-income countries. We found no studies from low-income countries. Four high-income countries contributed the most to the study, while the other countries had a selection of one or two. A summary of this data is presented in Table 1.
| Country | Wealth status | Number of studies |
| Australia | High income | 5 |
| Canada | High income | 4 |
| England | High income | 2 |
| France | High income | 1 |
| Germany | High income | 1 |
| Hong Kong | High income | 1 |
| Israel | High income | 1 |
| Italy | High income | 2 |
| Japan | High income | 1 |
| Netherlands | High income | 1 |
| New Zealand | High income | 1 |
| Poland | High income | 1 |
| Qatar | High income | 1 |
| Saudi Arabia | High income | 4 |
| Scotland | High income | 1 |
| Switzerland | High income | 2 |
| United States | High income | 9 |
| Brazil | Upper middle income | 2 |
| China | Upper middle income | 1 |
| Iran | Upper middle income | 1 |
| St. Vincent & Grenadines | Upper middle income | 1 |
| Turkey | Upper middle income | 3 |
| Kenya | Lower middle income | 1 |
Table 1: Countries, income status, and number of studies
Another interesting perspective is to note the distribution of studies by continent. Europe has the highest number of studies, followed by North America and Australia. Asia contributed to 10 studies, but it contains developed and developing countries, making this analysis more complex. The other developing regions of Africa, the Caribbean, and South America are consistently underrepresented, creating substantial knowledge gaps. This imbalance raises concerns about the global applicability of research findings and the potential overlooking of unique challenges and perspectives from less-represented or under-reported areas. These data are represented in Figure 3.
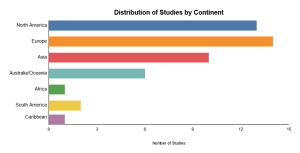
Figure 3: Distribution of studies by continent
Study designs: Study designs were primarily cross-sectional and qualitative. The research methodologies relied on four primary approaches: surveys/questionnaires, interviews, chart reviews, and database analyses. Surveys and questionnaires provide a standardized way to collect information from many participants and are useful for collecting quantitative data on attitudes, experiences, and behavior. This type of data collection process offers consistency and reliability. Interviews, whether semi-structured or structured, allow for more in-depth conversations on the topics and offer candid experiences from the patient’s perspective. This feedback allows researchers to explore qualitative data that might otherwise be missed in a fixed-format survey. This type of study is valuable for complex psychosocial phenomena or when gathering personal accounts.
Chart reviews from the selected studies involved a systematic search through previously established medical records. This technique is helpful in augmenting data in a mixed-method study to provide quantitative clinical data and insights into treatment patterns, outcomes, and health care processes. Database analyses offer large-scale data sets that can help to identify patterns or trends. As stated in each study, interviews, surveys, and questionnaires were developed through known and accepted methods. This adherence to methodological rigor enhances the credibility and reliability of the findings derived from these studies (Figure 4).
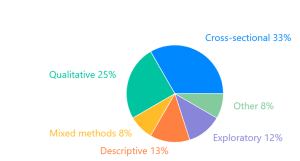
Figure 4: Study designs and methods
Thematic analysis: Studies revealed various methods of triage, 12 motivation themes, and 10 proposed solution themes. Some studies discussed the implications for non-urgent use in emergency services.
Triage methods: Triage methods define the urgency of a patient’s condition so that emergent patients can be treated promptly. Triage methods vary internationally, and the selected studies reflected this diversity by employing a range of different triage systems. Recognized triage methods found in this review include the Canadian triage and acuity scale (CTAS; 9 studies), emergency severity index (ESI, 4 studies), the Manchester triage system (MTS, three studies), the Australasian triage scale (ATS, three studies), the Swiss emergency triage scale (SETS, two studies), the emergency nurses classification in hospital (CIMU, 1 study), and the hospital urgency appropriateness protocol (HUAP, 1 study). Additionally, there were 13 studies that did not mention a triage method and 11 studies that used the hospital’s method (which was not named or was a modified version of a triage protocol). One of these studies mentioned an unnamed three-color-coded system (green, yellow, red), and one mentioned an unnamed five-color system (black, red, blue, green, yellow). This distribution is presented in figure 5.
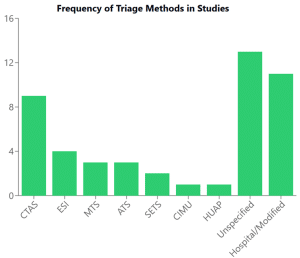
Figure 5: Frequency of triage methods
When examining the distribution of triage methods across different continents, as depicted in figure 6, we observed intriguing patterns that reveal the complex landscape of global emergency medical practices. Countries with more centralized health care systems, such as Canada, tend to have more consistent triage methods nationally, while countries with decentralized or mixed systems, such as the United States, show more variation. Resource availability also plays a crucial role, with high-income countries more likely to implement and maintain complex, standardized triage systems, while lower-middle income countries may rely on simpler or locally developed methods due to resource constraints. Additionally, cultural perceptions of urgency and specific health care priorities of different countries may affect how triage systems are developed and implemented. This analysis highlights two critical issues: the lack of an internationally accepted triage protocol and the absence of a universally accepted definition of “non-urgent” cases.
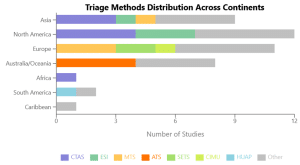
Figure 6: Triage methods across continents
Motivation for non-urgent ER visit: Analyzing motivations for non-urgent ER visits reveals a complex landscape of patient decision-making across different health care systems and cultural contexts. We identified 12 themes representing patients’ reasons or motivations for seeking an emergency level of care for a non-urgent problem, with some notable contradictions and inconsistencies emerging. Themes include perceived urgency and severity (20 countries), access and availability issues (13 countries), quality and trust perceptions (12 countries), convenience and efficiency (11 countries), specific service needs (10 countries), referrals and recommendations (8 countries), health system navigation issues (8 countries), financial considerations (7 countries), dissatisfaction with primary care (7 countries), personal preferences and expectations (6 countries), transportation and location (5 countries), and cultural and social factors (3 countries). Figure 7 represents these themes.
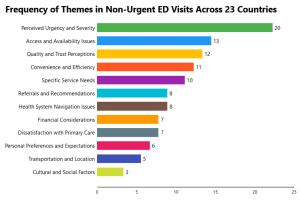
Figure 7: Frequency of themes in non-urgent visits across 23 countries
While “perceived urgency and severity” is the most common theme, mentioned in 20 out of 23 countries, its prominence varied significantly across different contexts. It was particularly important in Poland, Switzerland, Turkey, and Israel, suggesting that how patients assess their condition is a significant factor in non-urgent ED visits. Cultural differences variability highlights the need for more nuanced, culturally sensitive approaches to understanding perceived urgency. Financial considerations sometimes overshadowed urgency perceptions in the United States system. Cultural contexts across societies also influenced this theme, with varying thresholds for an “urgent” condition.
This review identified access and availability issues as the second most common theme in 13 countries, especially in Australia, Poland, Turkey, the United States, Brazil, and Saudi Arabia, but with notable inconsistencies in how “access” was defined. Some studies focused on geographic proximity, others on appointment availability or waiting times, and still others on financial accessibility. A striking contradiction emerged in a study from Germany, which suggested that improved primary care access did not significantly reduce non-urgent ED visits, conflicting with findings from other countries. Quality and trust perceptions emerged as influential factors in non-urgent ED use across 12 countries. Turkey, Italy, Hong Kong, Israel, and Germany emphasized these issues more, but the review found inconsistencies in how the studies operationalized these concepts. Some studies focused on the perceived technical quality of care, while others emphasized interpersonal aspects or overall satisfaction. Contradictory findings emerged regarding the relationship between quality perceptions and non-urgent ED use. For instance, a study from Hong Kong found that a higher perceived quality of ED care was associated with increased non-urgent use. In contrast, a United States study suggested that perceived low quality of primary care was a stronger driver. The evidence supporting this theme is moderately strong, drawing from quantitative surveys and qualitative interviews across diverse countries. However, the subjective nature of quality and trust concepts and the lack of standardized measures limit the direct comparability of findings across studies.
Referrals and recommendations, mentioned in Australia, Poland, England, Scotland, and Qatar, and health system navigation issues prevalent in Switzerland, the United States, China, and Saudi Arabia, point to systemic factors contributing to non-urgent ED use. Financial considerations and dissatisfaction with primary care appeared in about a third of the countries. The United States, Hong Kong, and France demonstrated this trend most prominently. However, their importance may vary based on the health care system used, reflecting the influence of different health care financing models. In the United States, it reflects its largely privatized health care system. At the same time, its relevance in Hong Kong and France suggests that the cost can influence ED use even in systems with universal coverage. Studies from the United States, Brazil, and St. Vincent and the Grenadines highlighted personal preferences and transportation issues.
Interestingly, 10 or more countries mentioned the top 5 themes, suggesting these issues are widespread. Surprisingly, cultural and social factors ranked among the least common themes. However, the review identified specific influences of these factors in countries such as St. Vincent and the Grenadines and Saudi Arabia, highlighting the potential impact of local customs and social norms on healthcare-seeking behaviors.
Proposed solutions: We identified 10 key themes for proposed solutions to address non-urgent ED visits and summarized them in table 2. These solutions vary widely, reflecting the complex nature of the problem and the diverse health care contexts in which they are proposed.
| Solution | Key components |
| 1. Improving access to primary care
|
· Extended hours . Same-day appointments · More urgent care centers · Better transportation · Increased workforce |
| 2. Patient education and health literacy
|
· ED vs. primary care use · Chronic condition management · Understanding medical urgency · Available care options |
| 3. Triage and redirection systems
|
· Nurse triage at the ED entrance · Non-urgent referral protocols · ED “fast-track” systems · Telephone triage |
| 4. Enhancing primary care capabilities
|
· Expanded diagnostics/treatment · Better continuity of care · Comprehensive services |
| 5. Utilizing technology and information systems | · Telemedicine options · Care-finding apps · Electronic health records · Data analytics for ED use |
| 6. Addressing social determinants of health
|
· Transportation/housing help · Social services connection · Childcare issue solutions |
| 7. Care coordination and case management
|
· ED-primary care communication · Coordinators for frequent users · Post-ED visit follow-up |
| 8. Financial incentives and policy changes
|
· Non-urgent ED co-pays · Primary care use incentives · Reimbursement model changes · Expanded insurance coverage |
| 9. Alternative care models
|
· ED-primary care co-location · Community paramedicine · Nurse-led clinics |
| 10. Targeted interventions for high utilizers
|
· Frequent user management · Addressing underlying needs · Population-specific programs |
Table 2: Proposed solutions and key components
Discussion
This scoping review analyzed studies from 23 countries of varying income status and health care systems. It revealed several themes that indicate complex motivations for non-urgent ED use and found various proposed solutions. The findings have significant implications for policy, practice, and future research.
Our review encompassed studies from high-income, upper-middle-income, and lower-middle-income countries with distinct health care system structures. This diversity allows for meaningful comparisons and insights into how different systems influence non-urgent ED use. In high-income countries, there are 4 primary health care systems. Mixed systems, such as Australia’s, combine universal public insurance with private options that, while offering comprehensive care, can lead to access disparities, potentially driving non-urgent ED visits when primary care wait times are long. The National Health Service used in the UK offers free care at the point of service but has long wait times for certain services, which may inadvertently encourage non-urgent ED use.[24] The cost-sharing policy through mandatory private insurance used in Switzerland and the Netherlands might deter some non-urgent ED visits. At the same time, the Netherlands’ strong primary care focus could help redirect patients appropriately. The multi-payer system in the United States lacks universal coverage. High costs can lead to delayed care-seeking and subsequent non-urgent ED use, especially among the uninsured or underinsured.[25]
In upper-middle-income countries such as Turkey and Brazil, transitional systems are trying to keep up with rapid urbanization and changing health care demands. Despite progress towards universal coverage, challenges with access, quality, and wait times can drive patients towards EDs for non-urgent care.[26] China, while working towards universal coverage, faces challenges with its complex system of public insurance schemes and high out-of-pocket costs, which could influence patterns of ED use.[27]
One of the most striking findings is the lack of a universally accepted definition of “non-urgent” cases and the variability in triage methods across different regions. While some standardized systems, such as CTAS in North America and MTS in Europe, are prevalent, unspecified or alternative methods are also significantly used. This lack of standardization complicates how we define non-urgent and how this applies to cross-cultural comparisons, and it may hinder the development of applicable solutions. Future research should focus on adopting standardized triage protocols and a universally accepted definition of non-urgent to facilitate comparison and knowledge across different health care systems.
We identified 12 motivation themes providing valuable insights into why patients choose ERs for non-urgent care. The top three themes are perceived urgency and severity, access and availability, and quality and trust issues. Each of these themes has significant implications. The primary driver of non-urgent ED visits is perceived urgency and severity. Its prominence across 20 out of 23 countries suggests that patients’ subjective assessment of their condition is a crucial factor globally. This finding highlights a critical need for policymakers to enhance public health education to improve individuals’ ability to assess the urgency of their medical conditions and improve health care literacy. Access and availability as a driver of non-urgent ED use is the second most mentioned theme across many countries, highlighting significant barriers to health care access, particularly in countries such as Australia, Poland, and the United States. This indicates that improvements in primary care accessibility and quality could potentially reduce non-urgent ER visits.
Our findings indicate that financial considerations vary in non-urgent ED use across different health care systems and present another contrast. In practice, health care providers should be aware of the financial implications of care for their patients and be prepared to discuss cost-effective care options when appropriate. For research, future studies should examine the impact of various economic models (e.g., co-payments, universal free care) on non-urgent ED use patterns. Cost-effectiveness analyses of interventions to reduce non-urgent ED use would also be valuable. Our review revealed significant variations in non-urgent ED use patterns across different countries and health care systems, suggesting that a solution working in one system might not be readily transferable to another. Cultural norms and social customs play a significant role in ED patterns. The study from St. Vincent and the Grenadines revealed that ED use can be a socially shared custom, often seen in Western countries. It prompts us to consider: How much of what we consider “rational” healthcare-seeking behavior is culturally determined? In other countries, such as Saudi Arabia, there are significant cultural gender norms that influence health care decision-making, and we must consider this for culturally sensitive and equitable policy.[28-30]
These findings suggest that policymakers should consider the importance of context-specific policies for addressing non-urgent ED use and identify the specific cultural and systemic factors that might influence this behavior. For research, this analysis underscores the need for more comparative effectiveness studies, long-term impact assessments, and research on cultural adaptation of interventions. Future efforts should focus on developing flexible, context-sensitive strategies tailored to local health care systems and cultural contexts while ensuring equity across diverse populations.
Strengths, limitations, and future research directions: Strengths of this review include the development of a priori protocol and adherence to JBI and PRISMA-ScR reporting guidelines and checklists.[19,20] The comprehensive literature search, standardized data extraction, and transparent search strategy add rigor, transparency, and credibility to the study.
This review has several limitations. Time constraints, exclusion of non-English studies, and limited access to all available studies reduced the scope’s reach. The predominance of studies from high-income countries limits the generalizability of findings to lower-income settings. Future research should focus on understanding non-urgent ER use in low-income countries and explore how solutions from higher-income countries might be adapted to resource-constrained settings. Additionally, the variability in triage methods and definitions of “non-urgent” across studies makes direct comparisons challenging. Future studies should work towards more standardized definitions and methods to facilitate better cross-cultural analyses.
Lastly, while this review identified numerous proposed solutions, more rigorous evaluations of these interventions’ effectiveness in different contexts are needed.
Future research should focus on implementing and assessing these solutions, particularly in diverse health care systems and cultural settings.
Conclusion
As emergency medical systems continue to evolve, understanding the non-urgent patient and the effects of ED use can provide valuable insights for policymakers and health care administrators worldwide. This study shows that non-urgent ER use is a complex issue with many variables that have far-reaching implications for addressing the challenge of non-urgent ED use. It highlights the need for context-specific approaches that consider patient perceptions, health care system structures, cultural factors, and the economy. Emergency systems worldwide have similar goals: to provide efficient, effective health care that meets the needs of the population while optimizing the use of emergency services for truly urgent cases. By learning from diverse global patient experiences and adapting solutions to local contexts, health care systems can work towards more efficient resource utilization while ensuring appropriate care for all patients.
References
- Agency for Healthcare Research and Quality. Healthcare Cost and Utilization Project. Updated February, 2025. Accessed January 7, 2024. Healthcare Cost and Utilization Project
- U.S. Department of Health and Human Services. Trends in the Utilization of Emergency Department Services, 2009–2018. Office of the Assistant Secretary for Planning and Evaluation; 2021. Accessed January 7, 2024. Trends in the Utilization of Emergency Department Services, 2009–2018
- American College of Emergency Physicians. Emergency Department Crowding: High Impact Solutions. Emergency Medicine Practice Committee; 2016. Accessed January 7, 2024 Emergency Department Crowding: High Impact Solutions
- Alnasser S, Alharbi M, AAlibrahim A, et al. Analysis of Emergency Department Use by Non-Urgent Patients and Their Visit Characteristics at an Academic Center. Int J Gen Med. 2023;16:221-232. doi:10.2147/IJGM.S391126 PubMed | Crossref | Google Scholar
- McIntyre A, Janzen S, Shepherd L, Kerr M, Booth R. An integrative review of adult patient-reported reasons for non-urgent use of the emergency department. BMC Nurs. 2023;22(1):85. doi:10.1186/s12912-023-01251-7 PubMed | Crossref | Google Scholar
- U.S. Department of State. Independent States in the World. Published March 12, 2025. Accessed January 7, 2024. Independent States in the World
- Harris B. The world has 4 key types of health service – this is how they work. World Economic Forum. Published October 9, 2020. Accessed January 7, 2024. The world has 4 key types of health service – this is how they work
- World Bank. World Bank Country and Lending Groups. Published July 1, 2024. Accessed January 7, 2024. World Bank Country and Lending Groups
- Halton C. World Economic Outlook: What It Is, Examples. Investopedia. Updated April 19, 2022. Accessed January 7, 2024. World Economic Outlook: What It Is, Examples
- European Parliament. The OECD – Promoting ‘better policies for better lives’. Published October, 2014. Accessed February 10, 2024. The OECD – Promoting ‘better policies for better lives’
- Jamison DT, Gelband H, Horton S, et al., eds. Disease Control Priorities: Improving Health and Reducing Poverty. 3rd ed. eBook. The International Bank for Reconstruction and Development / The World Bank; 2017:247-265. doi:10.1596/978-1-4648-0527-1 PubMed | Crossref | Google Scholar
- American Public Health Association. Strengthening Health Systems in Developing Countries. Published October 8, 2009. Accessed February 4, 2024. Strengthening Health Systems in Developing Countries
- Kironji AG, Hodkinson P, de Ramirez SS, et al. Identifying barriers for out of hospital emergency care in low and low-middle income countries: a systematic review. BMC Health Serv Res. 2018;18(1):291. doi:10.1186/s12913-018-3091-0 PubMed | Crossref | Google Scholar
- Oleribe OO, Momoh J, Uzochukwu BS, et al. Identifying Key Challenges Facing Healthcare Systems In Africa And Potential Solutions. Int J Gen Med. 2019;12:395-403. doi:10.2147/IJGM.S223882 PubMed | Crossref | Google Scholar
- Christ M, Grossmann F, Winter D, Bingisser R, Platz E. Modern triage in the emergency department. Dtsch Arztebl Int. 2010;107(50):892-898. doi:10.3238/arztebl.2010.0892 PubMed | Crossref | Google Scholar
- Bahadori M, Mousavi SM, Teymourzadeh E, Ravangard R. Emergency department visits for non-urgent conditions in Iran: a cross-sectional study. BMJ Open. 2019;9(10):e030927. doi:10.1136/bmjopen-2019-030927 PubMed | Crossref | Google Scholar
- Morgans A, Burgess SJ. What is a health emergency? The difference in definition and understanding between patients and health professionals. Aust Health Rev. 2011;35(3):284-289. doi:10.1071/AH10922 PubMed | Crossref | Google Scholar
- Vecchio N, Davies D, Rohde N. The effect of inadequate access to healthcare services on emergency room visits. A comparison between physical and mental health conditions. PLoS One. 2018;13(8):e0202559. doi:10.1371/journal.pone.0202559 PubMed | Crossref | Google Scholar
- Peters M, Godfrey C, McInerney P, et al. Chapter 11: Scoping Reviews. JBI Manual for Evidence Synthesis. 2020. doi:10.46658/JBIMES-20-12 Crossref
- Tricco AC, Lillie E, Zarin W, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med. 2018;169(7):467-473. doi:10.7326/M18-0850 PubMed | Crossref | Google Scholar
- PRISMA 2020 checklist. PRISMA Statement. Accessed February 4, 2024. PRISMA 2020 checklist
- Kalan L, Chahine RA, Lasfer C. The Effectiveness and Relevance of the Canadian Triage System at Times of Overcrowding in the Emergency Department of a Private Tertiary Hospital: A United Arab Emirates (UAE) Study. Cureus. 2024;16(1):e52921. doi:10.7759/cureus.52921 PubMed | Crossref | Google Scholar
- Miyazawa A, Maeno T, Shaku F, et al. Inappropriate use of the emergency department for nonurgent conditions: Patient characteristics and associated factors at a Japanese hospital. J Gen Fam Med. 2019;20(4):146-153. doi:10.1002/jgf2.249 PubMed | Crossref | Google Scholar
- Funakoshi H, Shiga T, Homma Y, et al. Validation of the modified Japanese Triage and Acuity Scale-based triage system emphasizing the physiologic variables or mechanism of injuries. Int J Emerg Med. 2016;9(1):1. doi:10.1186/s12245-015-0097-9 PubMed | Crossref | Google Scholar
- Sax DR, Warton EM, Mark DG, et al. Evaluation of the Emergency Severity Index in US Emergency Departments for the Rate of Mistriage. JAMA Netw Open. 2023;6(3):e233404. doi:10.1001/jamanetworkopen.2023.3404 PubMed | Crossref | Google Scholar
- Chmielewski N, Moretz J. ESI Triage Distribution in U.S. Emergency Departments. Adv Emerg Nurs J. 2022;44(1):46-53. doi:10.1097/TME.0000000000000390 PubMed | Crossref | Google Scholar
- Elsayed ZM, El-Zeny AB, Moustafa MS, Ellouly HA. Comparison between Australasian Triage Scale and Emergency Severity Index. Egypt J Surg. 2020;39:455. doi:10.4103/ejs.ejs_1_20 Crossref | Google Scholar
- Tikkanen R, Osborn R, Mossialos E, Djordjevic A, Wharton G. International Profiles of Health Care Systems 2020. The Commonwealth Fund. Published December, 2020. Accessed August 2, 2024. International Profiles of Health Care Systems 2020
- Aldosari H. The Effect of Gender Norms on Women’s Health in Saudi Arabia. Arab Gulf States Institute in Washington. Published May 2, 2017. Accessed August 2, 2024. The Effect of Gender Norms on Women’s Health in Saudi Arabia
- Habib S, Khan MA, Hamadneh NN. Gender Sensitivity in Accessing Healthcare Services: Evidence from Saudi Arabia. Sustainability. 2022;14(22):14690. doi:10.3390/su142214690 Crossref | Google Scholar
Acknowledgments
The authors acknowledge the guidance and expertise of Dr. Weber and Hal Bright in the development of this scoping review protocol.
Funding
No external funding was received for this project.
Author Information
Corresponding Author:
Nyala Edwards
Department of Emergency Medicine
Charleston County EMS, South Carolina, United States
Email: [email protected]
Co-Author:
Ken Perry
Department of Emergency Medicine
Charleston County EMS, South Carolina, United States
Authors Contributions
Nyala Edwards and Ken Perry contributed equally to the conceptualization, investigation, and data curation by identifying and critically reviewing the selected literature. Both authors were actively involved in writing – original draft preparation and writing – review & editing, collaboratively refining the manuscript. They also participated in the supervision of the research process, ensuring the accuracy and integrity of the work. The final version of the manuscript was read and approved by both Nyala Edwards and Ken Perry for submission to the journal.
Ethical Approval
Not applicable
Conflict of Interest Statement
The author declares no conflicts of interest.
Guarantor
None
DOI
Cite this Article
Nyala E, Ken P. Understanding What Motivates Non-Urgent Patients to Seek an Emergency Level of Care and How this Impacts Emergency Services on a Global Scale: A Scoping Review. medtigo J Emerg Med. 2025;2(2):e3092222. doi:10.63096/medtigo3092222 Crossref













