






 Author Affiliations
Author Affiliations
Abstract
Background: Antenatal care (ANC) is essential for safeguarding maternal and neonatal health by enabling early detection of pregnancy complications and encouraging healthy practices. However, despite free services in government hospitals, limited awareness and persistent knowledge gaps among women in low-resource settings, such as District Swat, hinder timely access and optimal utilization.
Aim: This study aimed to assess the level of knowledge regarding antenatal care among pregnant women attending selected government hospitals in District Swat.
Methodology: This descriptive cross-sectional study was conducted at a government hospital in District Swat. A total of 377 pregnant women aged 15–49 years were recruited using convenience sampling. Data were collected through a structured, modified questionnaire including demographic details and 33 ANC knowledge items. The tool demonstrated good reliability, with a Cronbach’s alpha of 0.87.
Results: Most pregnant women were moderately knowledgeable of antenatal care, with a smaller number being knowledgeable. The knowledge gaps were detected in areas that are closely connected with danger signs during pregnancy, nutrition, and the necessity of regular visits to ANC. Important relationships were presented among the knowledge levels and the demographic factors chosen.
Conclusion: The research findings were that, though most pregnant women had moderate knowledge of antenatal care, there are areas of significant knowledge gaps. It is needed to enhance maternal knowledge and increase the safe results of pregnancy by strengthening health education during ANC visits and creating more specific actions aimed at generating awareness.
Keywords
Antenatal care, Knowledge, Pregnant women, Maternal health, Neonatal health.
Introduction
This research is primarily dedicated to antenatal care (ANC), the knowledge of pregnant women, the health of a mother, the monitoring of pregnancy, and the government healthcare services. Antenatal care can be described as the daily medical and nursing care given to pregnant women with the view of maintaining the health of both the mother and the child such as routine check-ups, nutritional counseling, detection of complications, and health education[1] ANC awareness among the pregnant women is paramount in ensuring that the pregnant women use the services promptly, follow medical prescriptions, and minimize maternal and neonatal complications. Proper knowledge of the red flags, vaccinations, diets, and hygiene in pregnancy allows women to make the correct choice and take an active part in their health care.[2] Poor knowledge may result in delayed consultation, inadequate adherence to supplementation, susceptibility to obstetric complications, and an increase in the morbidity in the mother and the baby.[3] The government hospitals are the main providers of maternal care in Swat as they provide free or subsidized services, but there are problems with patient education, awareness, and access to services. In this study, the researcher will determine the extent of knowledge among pregnant women on ANC to establish gaps and evidence-based interventions to address maternal health.[4]
Maternal and neonatal morbidity and mortality are big issues in the entire world, with the greatest population in the low- and middle-income countries having minimal access to good antenatal care. Research in the developing states reveals that most pregnant women lack the knowledge in terms of timing, frequency, and content of ANC visits, nutritional requirements, signs of danger in pregnancy, and prenatal preparation. This ignorance is usually further boosted by illiteracy levels, cultural beliefs, inadequate health education, and counseling by health care providers. In Pakistan, particularly in the district of Swat, the evidence concerning the knowledge of pregnant women about ANC services is scarce, and it is difficult to come up with tailored interventions.[2,3]
Antenatal services play a crucial role in minimizing maternal and fetal complications like preeclampsia, gestational diabetes, anemia, infections, and pre-term delivery. Educated mothers will be more willing to visit ANC regularly, adhere to the dietary and lifestyle recommendations, and seek medical help on warning signs in a timely manner.[3] The World Health Organization stresses the fact that pregnant women need at least four dedicated ANC visits that would help track the process and enhance the results. Nonetheless, in resource-constrained environments, most of the women receive fewer visits often because they lack awareness, resources, or because of sociocultural constraints.[4]
Pregnancy education enhances maternal confidence, lessens anxiety, and ensures healthier behavior. To illustrate, the ANC knowledge about the significance of iron and folic acid supplementation, the student should be familiar with the manifestation of bleeding or edema, and the student must know when to report the reduced fetal activity.[5] Health education may occur in clinics, community health, or home visits on the part of trained healthcare professionals. Nevertheless, in most hospitals in Swat, the human resources, overcrowding, and lack of counseling minimize the chance of successful maternal education.[6]
Knowledge related to pregnancy not only influences health behaviors but also maternal and neonatal outcomes. Females who have poor ANC knowledge have higher chances of developing preventable complications, delay in care seeking, and adverse birth experiences.[7] On the other hand, individuals who have sufficient knowledge are more compliant with ANC schedules, nutrition, higher rates of institutional delivery, and better practices for their newborns. Knowledge gaps in pregnant women are thus critical to the formulation of effective interventions, the minimization of maternal and infant morbidity, and the general health status of the area.[8]
It is postulated that paternal education, socioeconomic status, parity, and exposure to health messages have significant effects on ANC knowledge. The more educated women are, the better they understand and adhere to some recommended antenatal practices.[9] The family and cultural norms may either promote or impede the use of ANC services. In some cases, the myths surrounding pregnancy and delivery practices could render women unable to access timely care. Knowledge assessment enables healthcare professionals to detect these obstacles and adopt administrative educational interventions.[10]
Swat has government hospitals serving a wide population of both urban and rural communities, which creates a special challenge to the delivery of maternal health care. The quality of ANC counseling may be impacted by high patient turnover, insufficient staffing, and limited resources.[11] Maternal knowledge assessment in these environments becomes highly essential to inform the interventions and the efficient use of resources. Proper education plans can empower female individuals to make the right decisions, identify danger signs in earlier stages, and get medical care in time.
Despite the importance of ANC knowledge identified, there are very limited studies that have been conducted within the government hospitals of Swat. Local research evidence is essential to the development of specific health education and training of healthcare personnel, as well as informing policy.[12] This study will address this gap by determining the level of knowledge of pregnant women on antenatal care, such as the knowledge of ANC visits, danger signs, nutrition, supplementation, and institutional delivery practices.
Antenatal care can largely prevent pregnancy complications and adverse outcomes. Inadequate maternal knowledge is a contributing factor to late healthcare-seeking behavior, lack of adherence to medical recommendations, and greater weakness to maternal and neonatal morbidity and mortality. Assessing the knowledge of pregnant women is important to enable health professionals to develop context-based strategies, focus more on education, and enhance quality maternal health care services.[13] Knowledge gaps can also be understood to help in the promotion of patient-centered care, maternal empowerment, and an overall improvement of the healthcare delivery system in the tertiary care setting.
In Swat, tertiary care hospitals have a critical role to play in offering specialized maternal and child care. The large number of patients and the complexity of cases demand that nurses and other caregivers train and mentor pregnant women. The evaluation of maternal knowledge about antenatal care will guarantee the areas of highest priority, decrease risks that can be prevented, enhance patient satisfaction, and secure safe maternal and neonatal outcomes.[14]
In general, maternal knowledge assessment is an important step towards enhancing the services of antenatal care. By pinpointing the areas of vulnerability and deploying specific educational interventions, medical professionals will be able to improve the safety of mothers and fetus, their access to ANC services in a timely manner, and help to optimize health outcomes in the area.[15] The study will be of great use to the healthcare administrators, policymakers, and nurse educators in Swat to enhance the practice of antenatal care and maternal health services.
Methodology
The research design was a quantitative descriptive cross-sectional study to determine the level of knowledge on ANC among the pregnant women who are visiting the selected government hospitals within the District Swat. These are hospitals where maternal and child healthcare services are offered in a full package, including the routine antenatal checkups, counselling, and health education. The sample size was 377 pregnant women between the ages of 15 and 49 years who were attending the antenatal clinics at the time of data collection. Women in a critical condition, in the emergency, or not willing to take part were excluded.
RAOSOFT sample size calculator was used to calculate the sample size with a 95% confidence level and with 5% margin of error. Due to the size of the estimated population, the required sample size was obtained to be 377 respondents to have sufficient statistical power and representativeness. Another sampling method that was used was non-probability convenience sampling, where eligibility depended on the fact that the participants had to be eligible and available at a given time of the study.
Data collection procedure: Ethical approval was then given by the Graduate Study Committee (GSC) of the National College of Nursing, Swat, before the data collection. The administrations of the chosen government hospitals also gave written permission. Participants were informed about the reason and the aim of the study orally and in writing, and informed consent was obtained.
A structured, modified questionnaire with a high degree of reliability (Cronbach’s alpha = 0.87) was used to collect the data. The instrument was made up of two parts. The demographic variables that were contained in the first section were age, education, and religion. The second part entailed 33 questions that tested the knowledge about antenatal care. The scores of knowledge were divided into good (76100%), moderate (5175%), and poor (050%). Responses in the form of completed questionnaires were put in a secure location that guaranteed confidentiality and integrity of data.
Data analysis procedure: The data were coded and typed into SPSS version 27 to analyze them. The demographic characteristics and knowledge levels were summed up with the help of descriptive statistics, such as frequencies, percentages, means, and standard deviations. Chi-square tests were used to calculate the inferential analysis between demographic variables and categories of knowledge. The p-value below 0.05 was taken as statistically significant.
Results
Demographic characteristics of participants: The demographic profile shows that nearly half of the participants were aged 25-34 years (47.2%), followed by those aged 15-24 years (29.7%), indicating a predominantly young reproductive-age population. Most women were married between 18 and 24 years (57.6%), while more than one-fifth (22.6%) entered marriage before the age of 18, reflecting the persistence of early marriage. Educational attainment varied, with the largest proportion having secondary education (32.6%), followed by no formal education (24.4%) and primary education (23.3%), whereas only 19.6% had higher education. Regarding husbands’ education, the majority had secondary (38.5%) or higher education (37.1%), suggesting a relatively better educational status among spouses. In terms of parity, most participants were multigravida (61.5%), indicating previous pregnancy experience. Occupationally, more than half of the women were housewives (57.6%), while 26.0% were employed and 16.4% worked as laborers. Overall, the findings reflect a population with varied educational and socioeconomic backgrounds.
| Variable | Category | Frequency (n) | Percentage (%) |
| Age (years) | 15-24 | 112 | 29.7 |
| 25-34 | 178 | 47.2 | |
| 35-44 | 70 | 18.6 | |
| 45-49 | 17 | 4.5 | |
| Age at marriage | <18 | 85 | 22.6 |
| 18-24 | 217 | 57.6 | |
| >24 | 75 | 19.9 | |
| Education | Primary | 88 | 23.3 |
| Secondary | 123 | 32.6 | |
| Higher | 74 | 19.6 | |
| No formal education | 92 | 24.4 | |
| Husband’s education | Primary | 92 | 24.4 |
| Secondary | 145 | 38.5 | |
| Higher | 140 | 37.1 | |
| Parity | Primigravida | 145 | 38.5 |
| Multigravida | 232 | 61.5 | |
| Occupation | Housewife | 217 | 57.6 |
| Employed | 98 | 26.0 | |
| Laborer | 62 | 16.4 |
Table 1: Demographic characteristics of participants
The findings showed that more than half of the pregnant women (61.5%) were not attending their first ANC visit, while 59.4% reported making regular antenatal visits. Slightly over half of the respondents (56.2%) followed the ANC schedule provided by healthcare workers, and a large majority (73.7%) adhered to the advice given during ANC visits. Most participants (87.8%) perceived antenatal care as useful, reflecting a positive attitude toward ANC services. Support from husbands was reported by 79.1% of women, whereas support from mothers-in-law was comparatively lower at 59.9%. Less than half of the respondents received the government honorarium (38.2%) or felt motivated by government measures (46.9%). About one-third of the women (34.0%) reported facing financial problems related to ANC visits.
| Question | Yes n (%) | No n (%) |
| First ANC visit | 145 (38.5) | 232 (61.5) |
| Regular ANC visits | 224 (59.4) | 153 (40.6) |
| Follow scheduled visits | 212 (56.2) | 165 (43.8) |
| Follow the advice given | 278 (73.7) | 99 (26.3) |
| Think ANC useful | 331 (87.8) | 46 (12.2) |
| Husband supportive | 298 (79.1) | 79 (20.9) |
| Mother-in-law supportive | 226 (59.9) | 151 (40.1) |
| Government honorarium received | 144 (38.2) | 233 (61.8) |
| Government measures motivating | 177 (46.9) | 200 (53.1) |
| Financial problems for ANC | 128 (34.0) | 249 (66.0) |
Table 2: Knowledge regarding ANC visits
Figure 1 illustrates the overall knowledge level of participants regarding antenatal care (ANC). Nearly half of the respondents (48.3%) demonstrated a moderate level of knowledge, indicating partial awareness of recommended ANC practices. About one-quarter of participants (24.9%) achieved a good knowledge score, reflecting adequate understanding of ANC components and importance. However, a considerable proportion (26.8%) had poor knowledge, suggesting substantial gaps in essential ANC information. These findings highlight that although awareness of ANC exists among many participants, comprehensive knowledge remains insufficient for a significant segment, underscoring the need for targeted educational interventions to improve ANC-related understanding.
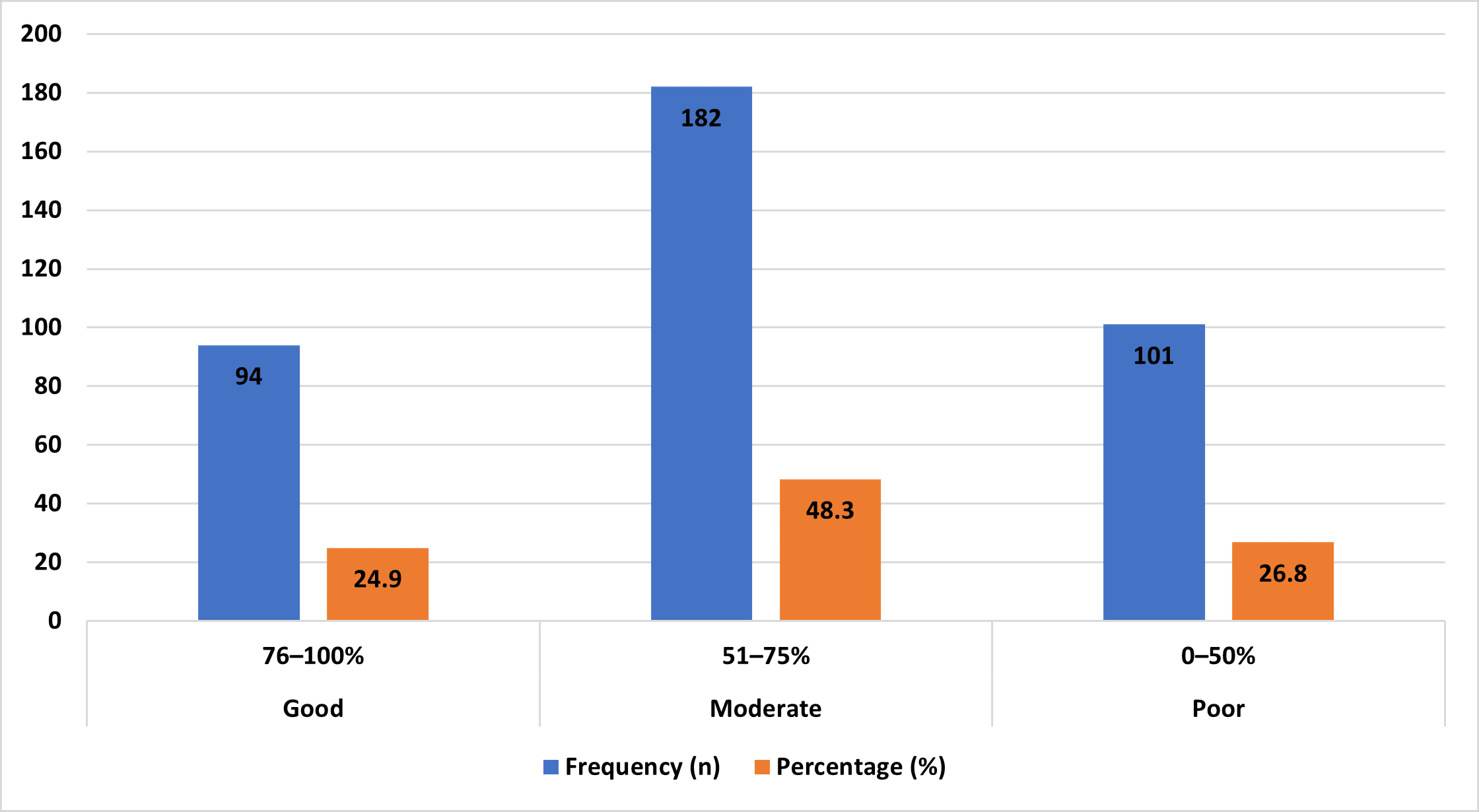
Figure 1: Overall, knowledge level regarding ANC
Table 3 presents the association between education level and knowledge regarding ANC. A clear and statistically significant relationship was observed between educational status and ANC knowledge (χ² = 42.5, p < 0.001). Participants with no formal education showed the highest proportion of poor knowledge (48.9%) and the lowest proportion of good knowledge (9.8%). As the level of education increased, the proportion of participants with good knowledge also increased, reaching 43.2% among those with higher education. Conversely, poor knowledge markedly declined with increasing education, from 48.9% in the uneducated group to only 6.8% among those with higher education. These findings indicate that education plays a crucial role in improving knowledge of ANC, emphasizing the importance of female education in enhancing maternal health awareness and utilization of antenatal services.
| Education | Poor knowledge n (%) | Moderate knowledge n (%) | Good knowledge n (%) | Total | χ² | p-value |
| No formal education | 45 (48.9) | 38 (41.3) | 9 (9.8) | 92 | 42.5 | <0.001 |
| Primary | 28 (31.8) | 44 (50.0) | 16 (18.2) | 88 | – | – |
| Secondary | 23 (18.7) | 63 (51.2) | 37 (30.1) | 123 | – | – |
| Higher | 5 (6.8) | 37 (50.0) | 32 (43.2) | 74 | – | – |
Table 3: Association between education level and ANC knowledge
Table 4 shows a statistically significant association between age and knowledge regarding antenatal care (ANC) (χ² = 14.7, p = 0.023). Younger participants aged 15-24 years had the highest proportion of poor knowledge (31.3%) and the lowest proportion of good knowledge (15.1%). In contrast, good knowledge increased progressively with age, reaching 32.9% among those aged 35-44 years and peaking at 64.7% in the 45-49 years age group. Moderate knowledge was most common among participants aged 15-24 years (53.6%) and 25-34 years (50.6%). These findings suggest that increasing age, reflecting greater life experience and repeated exposure to maternal health services, is associated with better knowledge of ANC.
| Age (years) | Poor knowledge n (%) | Moderate knowledge n (%) | Good knowledge n (%) | Total | χ² | p-value |
| 15-24 | 35 (31.3) | 60 (53.6) | 17 (15.1) | 112 | 14.7 | 0.023 |
| 25-34 | 45 (25.3) | 90 (50.6) | 43 (24.1) | 178 | – | – |
| 35-44 | 18 (25.7) | 29 (41.4) | 23 (32.9) | 70 | – | – |
| 45-49 | 3 (17.6) | 3 (17.6) | 11 (64.7) | 17 | – | – |
Table 4: Association between age and ANC knowledge
Discussion
The results of this paper indicated that a big percentage of pregnant women who received their ANC services in the sampled government hospitals within the District Swat had moderate knowledge about ANC, and only 24.9% had good knowledge. This is in line with a study by the Pakistani people, who determined that the maternal knowledge on ANC was sub-optimal, with the need to conduct awareness campaigns to enhance the knowledge levels of the expectant women.[16] In the same line of thought, research conducted in Nigeria and India indicated a similar kind of result, which indicated that even with the availability of the ANC services, there still exist gaps in knowledge among pregnant women.[17] These findings indicate that knowledge by itself cannot work without good health education interventions that are sensitive to the needs of the mother.
The report revealed that 47.2% of the participants were in the (25-34) age bracket, indicating that the majority of ANC attendants were in their prime reproductive age group. Similar results were noted in another study that involved rural Bangladesh where most of the pregnant women using ANC were of the same age group.[18] Younger participants (15-24 years) scored lower in their knowledge than older ones, which is understood by the fact that maternal experience is associated with positive effects on the understanding of the health practice.[19] However, other studies in city areas had indicated more awareness of the younger women as they had better access to their media and health information indicating a contrast that was based on geographical and socio-economic conditions.[20]
The level of education among the participants was closely correlated with knowledge of ANC, since 32.6% of respondents attained secondary education, with higher education being more related to better knowledge scores. This result is in line with one study that was carried out in Ethiopia, where maternal education was a strong factor in ANC knowledge and use.[21] In the same manner, a study in Nepal also emphasized the fact that literate women tended to attend ANC visits scheduled and to follow recommended practices.[22] Nonetheless, research in certain low-resource areas has shown that even educated women could have a poor level of knowledge because of a lack of counseling in health care institutions.[23]
The research established that most of the participants (61.5) were multigravida, and parity seemed to affect the level of knowledge, as primigravida women demonstrated a little less awareness. This is corroborated by evidence found in India, where the knowledge of the practicing mothers concerning ANC was higher, because they had been exposed to it before.[24] Contrastingly, other researchers in sub-Saharan Africa did not find any significant difference in the levels of knowledge across primigravida and multigravida women and showed that repeated exposure does not necessarily result in improved knowledge in the case of poor education.[25]
A higher number of 79.1 percent of the participants reported support for their husbands, whereas mother-in-law support was lower at 59.9%. Favorable family conditions were found to relate to increased rates of compliance with ANC visits. It can be compared to research in Pakistan and Afghanistan, where maternal attendance of ANC was enhanced significantly by the encouragement of spouses.[26] On the other hand, in patriarchal societies, family support has been cited as one of the obstacles, and women may not access services despite their level of knowledge.[27] This highlights the importance of family-based education programs.
A substantial proportion of the participants indicated financial and motivational barriers, as 34% of them said that they were financially constrained, and 53.1% were not motivated by government efforts. Indirect costs and the absence of incentives were found to be similar issues in rural India and Nepal, where ANC utilization was impacted.[28] Conversely, research in an urban area of Pakistan found that women had higher chances of attending ANC in the event that they were given support through finances and transportation, indicating that the socioeconomic environment had a great influence on the decisions women make regarding maternal health.[29]
The analysis revealed that 79.8 of the women were aware that ANC can reduce maternal anemia, and only 49.9 of them were aware that ANC can prevent neonatal jaundice. This observation can be explained by the fact that maternal knowledge is partial, which is confirmed by other African and South Asian studies that report that maternal knowledge is usually complete in relation to general problems, but not when it comes to neonatal complications that are less evident.[30] This means that there is a gap in the area of health education that should focus on the overall benefits of ANC.
In terms of nutrition, 80.9% were able to correctly identify higher iron requirement and 79.1% were able to identify higher caloric requirements during pregnancy. The results are in line with the research carried out in Ethiopia and Bangladesh that revealed that lack of knowledge on nutrition in pregnancy was related to the level of education and also exposure to health education.[31] Nevertheless, opposing results in rural Pakistan indicated a reduced level of awareness caused by cultural dietary limitations, such that the knowledge is not necessarily transferred into practice.[32]
The authors of the current research discovered that 64.2% of the female population was aware of the necessity to check blood pressure, and 71.1% of the population was aware of the necessity to see a specialist about hypertension. These levels of awareness were also similar in India, where the women who were visited by ANC regularly had a higher chance of recognizing signs of danger.[33] On the other hand, research in rural Africa reported exceedingly low awareness of high blood pressure conditions, which was that way because of the quality of counseling and the access to trained medical professionals.[34]
Lastly, the research highlights the significance of specific educational interventions, systematic counseling, and involvement of the community in enhancing the maternal knowledge of ANC. In comparison to other research works, moderate knowledge levels in District Swat show a level of progress and gaps at the same time.[35] An individual intervention based on educational background, parity, family support, and socioeconomic barriers is essential in improving the health outcomes of mothers and the effectiveness of ANC programs.
Recommendations:
- Government hospitals need to enhance health education programs to enhance the knowledge levels of pregnant women concerning the issue of antenatal care, which includes nutrition, danger signs, vaccinations, and neonatal care.
- Individualized guidance and misconception clarification should be included in every ANC visit through structured counseling sessions to promote individualized counseling.
- Awareness creation and awareness workshops should be carried out through community outreach strategies to access the women in rural and underserved communities.
- The family members (husbands and in-laws) should be advised to support ANC attendance and compliance with medical advice.
- Effective communication and patient education strategies should be trained by the medical personnel to increase knowledge transfer.
- They should be provided with educational resources, including pamphlets, posters, and audio-visual aids in local languages, to enhance comprehension and memorization.
- Maternal knowledge should be evaluated regularly to determine the gaps and design interventions based on the gaps.
- Accessibility, affordability, and adequacy of ANC services should be maintained by policymakers to assist maternal health education.
Conclusion
The study concluded that the general awareness of antenatal care in women in the District Swat who visit the selected government hospitals about antenatal care was moderate with only a quarter of them showing good knowledge. The age of the mother, level of education, number of children, and family support were also important determinants of the level of knowledge, and they underscored how the demographic and social factors could determine awareness. Although we were receiving ANC services, there were loopholes in the knowledge of critical areas of neonatal complications, nutrition, and red flags during pregnancy. These results highlight the importance of organized health education, special counseling, and community participation to enhance maternal education and safe pregnancy behaviors. The improvement of knowledge with the help of well-organized interventions may result in increased compliance with ANC schedules, better maternal and neonatal outcomes, and the quality of the maternal healthcare services, overall.
References
- Younas M, Parpio Y, Ali TS, Awan S. Male partners’ knowledge and practices of antenatal care in District Swat, Khyber Pakhtunkhwa, Pakistan: a cross-sectional study. J Midwifery Reprod Health. 2020;8(1):2005-2015. doi:10.22038/jmrh.2019.33935.1369
Crossref | Google Scholar - Ali SA, Dero AA, Aziz S, Ali G. Factors affecting the utilization of antenatal care among pregnant women: a literature review. J Pregnancy Neonatal Med. 2018;2(2):41-45. doi:10.35841/neonatal-medicine.2.2.41-45
Crossref | Google Scholar - Alqahtani F, Almudarra S, Kamel S, et al. Outbreak investigation of extensively drug-resistant Acinetobacter baumannii cases in the ICU of Al-Qatif Central Hospital in August 2019. Int J Infect Dis. 2020;101:316-317. doi:10.1016/j.ijid.2020.09.825
Crossref | Google Scholar - Rehman L, Shiekh M, Afzal A, Rizvi R. Risk factors, presentation and outcome of meningomyelocele repair. Pak J Med Sci. 2020;36(3):422-425. doi:10.12669/pjms.36.3.1237
PubMed | Crossref | Google Scholar - Mehmood S, Raza H, Abid F, et al. National prevalence rate of hepatitis B and C in Pakistan and its risk factors. J Public Health (Berl). 2020;28:751-764. doi:10.1007/s10389-019-01081-5
Crossref | Google Scholar - Selvarajoo S, Liew JWK, Tan W, et al. Knowledge, attitude and practice on dengue prevention and dengue seroprevalence in a dengue hotspot in Malaysia: A cross-sectional study. Sci Rep. 2020;10(1):9534. doi:10.1038/s41598-020-66212-5
PubMed | Crossref | Google Scholar - Asif M, Khan M, Tariq S. Modeling and exploring stillbirth risks in Northern Pakistan. Healthcare (Basel). 2025;13(12):1436. doi:10.3390/healthcare13121436
Crossref | Google Scholar - Ahmed M, Siddiqui A, Mirani A, Khan A, Siddiqui F, Nadeemuddin. Assessment of husbands’ knowledge on antenatal care in a tertiary care hospital, Karachi. Pak J Health Sci. 2024;5(12):134-138. doi:10.54393/pjhs.v5i12.2197
Crossref | Google Scholar - Zeb A, Ali S, Muhammed D, et al. Effectiveness of nurse led counselling sessions on psychological well-being of mothers with preterm infants at tertiary care hospitals in Swat. Pak J Med Cardiolog Rev. 2025;4(4):1342-1356. doi:10.64105/v5d4fm82 Crossref | Google Scholar
- Muhabaw T, Hailemeskel S, Lambebo A. Male involvement in antenatal care and associated factors among married men with wives who recently gave birth in Debre Tabor town, Northwest Ethiopia. BMC Pregnancy Childbirth. 2024;24(1):642. doi:10.1186/s12884-024-06809-0
PubMed | Crossref | Google Scholar - Lankan S, Rathnayaka P, Rathnayake N. Knowledge, attitudes, and support of partners in preparation for motherhood and maternal satisfaction with partner support: a hospital-based cross-sectional study in the Galle District. Sri Lankan J Nurs. 2025;3(2):18-37. doi:10.4038/sljn.v3i2.59
Crossref | Google Scholar - Shah H, Atta U, Arif U. Nurses’ experiences with ethical dilemmas in critical care settings: A mixed-method study at Saidu Teaching Hospital. medtigo J Med. 2025;3(1):e30623135. doi:10.63096/medtigo30623135
Crossref | Google Scholar - Mahar B, Shah T, Shaikh K, et al. Uncovering the hidden health burden: a systematic review and meta-analysis of iron deficiency anemia among adolescents, and pregnant women in Pakistan. J Health Popul Nutr. 2024;43(1):149. doi:10.1186/s41043-024-00643-y
PubMed | Crossref | Google Scholar - Nazir Q, Ahmad S, Anjum K, et al. Prevalence and risk factors of hepatitis B virus and hepatitis C virus among pregnant women of Faisalabad, Punjab, Pakistan. J Med Health Sci Rev. 2025;2(2):4588-4599.
Prevalence and risk factors of hepatitis B virus and hepatitis C virus among pregnant women of Fais… - Haq IU, Khan MI, Muhammad A, et al. Challenges Faced by Healthcare Professionals in Screening Newborns for Congenital Heart Defects in Pakistan. Int J Neonatal Screen. 2025;11(4):95. doi:10.3390/ijns11040095
PubMed | Crossref | Google Scholar - Siddique M, Manj YN, Waheed A. Cultural determinants that influence the utilization of maternal and childcare services in Punjab, Pakistan. J Dev Soc Sci. 2024;5(2):660-669. doi:10.47205/jdss.2024(5-II)61
Crossref | Google Scholar - Davis-Floyd R, Daviss BA, Ali I. Introduction. In: Traditional Midwives: Cross-Cultural Perspectives. Routledge; 2025.
Traditional Midwives: Cross-Cultural Perspectives - Ghur A, Randhawa S, Shahid N, et al. A Bottleneck Analysis of Iron and Folic Acid Supplementation Program in Pakistan. Matern Child Nutr. 2025;21(3):e13797. doi:10.1111/mcn.13797
PubMed | Crossref | Google Scholar - Amin M, Aziz MA, Manduzai AK, et al. Standard medical ethnobotany of Kohistan, North Pakistan. J Ethnobiol Ethnomed. 2024;20(1):64. doi:10.1186/s13002-024-00704-w
PubMed | Crossref | Google Scholar - Akram SJ, Akhtar AM, Zakar R. Frequency and determinants of hypoferritinemia without anemia among reproductive age women in Lahore: A cross-sectional study. Pak J Med Sci. 2025;41(12):3462-3471. doi:10.12669/pjms.41.12.12789
PubMed | Crossref | Google Scholar - Ullah S, Amin A, Islam U, et al. Prevalence of malaria in the different hospitals of Takht Bhai and District Mardan, Khyber Pakhtunkhwa. Sciences. 2024;13:1-14
Prevalence of Malaria in the Different Hospitals of Takht Bhai and District Mardan Khyber Pakhtunkh… - Seema A, Aftab N, Batool K, et al. Frequency of preterm birth among patients with preeclampsia at a tertiary care hospital. Indus J Biosci Res. 2025;3(6):1093-1099. doi:10.70749/ijbr.v3i6.2275
Crossref | Google Scholar - Comfort H, McHugh TA, Schumacher AE, et al. Global, regional, and national stillbirths at 20 weeks’ gestation or longer in 204 countries and territories, 1990–2021: findings from the Global Burden of Disease Study 2021. Lancet. 2024;404(10466):1955-1988. doi:10.1016/S0140-6736(24)01925-1
Crossref | Google Scholar - Maryam S, Saleem Z, Haseeb A, et al. Progress on the Global Research Agenda for Antimicrobial Resistance in Human Health in Pakistan: Findings and Implications. Infect Drug Resist. 2025;18:3795-3828. doi:10.2147/IDR.S531874
PubMed | Crossref | Google Scholar - Graham S, Davis-Floyd R. Traditional birth attendants and the biomedical system among the Karamojong of Uganda. In: Davis-Floyd R, Daviss BA, Ali I, eds. Traditional Midwives: Cross-Cultural Perspectives. Routledge; 2026.
Traditional birth attendants and the biomedical system among the Karamojong of Uganda - Kare AP, Gujo AB, Yote NY. Quality of antenatal care and associated factors among pregnant women attending government hospitals in Sidama Region, Southern Ethiopia. SAGE Open Med. 2021;9:20503121211058055. doi:10.1177/20503121211058055
PubMed | Crossref | Google Scholar - Bashir S, Ansari AH, Sultana A. Knowledge, Attitude, and Practice on Antenatal Care Among Pregnant Women and its Association With Sociodemographic Factors: A Hospital-Based Study. J Patient Exp. 2023;10:23743735231183578.. doi:10.1177/23743735231183578
PubMed | Crossref | Google Scholar - Gebremariam H, Tesfai B, Tewelde S, Kiflemariam Y, Kibreab F. Level of Knowledge, Attitude, and Practice of Pregnant Women on Antenatal Care in Amatere Health Center, Massawa, Eritrea: A Cross-Sectional Study, 2019. Infect Dis Obstet Gynecol. 2023;2023:1912187. doi:10.1155/2023/1912187
PubMed | Crossref | Google Scholar - Fegita P, Hikmah M, Malik R. Relationship between education level, age, and knowledge of pregnant women with antenatal care status. Sciena Sci J. 2022;1(2):154-164. doi:10.56260/sciena.v1i2.41
Crossref | Google Scholar - Hu W, Hu H, Zhao W, Huang A, Yang Q, Di J. Current status of antenatal care of pregnant women-8 provinces in China, 2018. BMC Public Health. 2021;21(1):1135. doi:10.1186/s12889-021-11154-4
PubMed | Crossref | Google Scholar - Obeagu E. An update on utilization of antenatal care among pregnant women in Nigeria. Int J Curr Res Clin Med Sci. 2022;9(9):21-26. doi:10.22192/ijcrcps.2022.09.09.003
Crossref | Google Scholar - Degu A, Nibret G, Gebrehana H, Getie A, Getnet B. Knowledge and Attitude Towards the Current Pandemic Corona Virus Disease and Associated Factors Among Pregnant Women Attending Antenatal Care in Debre Tabor General Hospital Northwest Ethiopia: An Institutional-Based Cross-Sectional Study. Int J Womens Health. 2021;13:61-71. doi:10.2147/IJWH.S285552
PubMed | Crossref | Google Scholar - Janakiraman B, Gebreyesus T, Yihunie M, Genet MG. Knowledge, attitude, and practice of antenatal exercises among pregnant women in Ethiopia: A cross-sectional study. PLoS One. 2021;16(2):e0247533. doi:10.1371/journal.pone.0247533
PubMed | Crossref | Google Scholar - Besho M, Tsegaye R, Yilma MT, et al. Knowledge, Attitude and Practice Toward Corona virus Infection Among Pregnant Women Attending Antenatal Care at Public Hospitals in Three Wollega Zones, Ethiopia. Int J Gen Med. 2021;14:3563-3573. doi:10.2147/IJGM.S295490
PubMed | Crossref | Google Scholar - Endalew M, Endalew N, Agegnehu A, Mekonnen Z, Teshome D. Knowledge and attitude towards anesthesia for cesarean section and its associated factors among pregnant women attending antenatal care: A cross sectional study. Ann Med Surg (Lond). 2022;75:103299. doi:10.1016/j.amsu.2022.103299
PubMed | Crossref | Google Scholar
Acknowledgments
The authors would like to express their sincere gratitude to Dr. Shah Hussain, Principal/Associate Professor, Janbar, College of Nursing, Swat, for his invaluable supervision, guidance, and support throughout the course of this study.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author Information
Corresponding Author:
Nasar Mian
Department of Nursing
National College of Nursing, Swat, Pakistan
Email: nasarmian819@gmail.com
Co-Authors:
Junaid Ali, Ishfaq Ahmad Mian, Shakir Ullah, Latif Ullah, Nasar Khan, Aiman Rahman, Amna Bibi, Shehnaz Malik
Department of Nursing
National College of Nursing, Swat, Pakistan
Shah Hussain
Department of Nursing
Janbar College of Nursing, Swat, Pakistan
Authors Contributions
Nasar Mian, Junaid Ali, Ishfaq Ahmad Mian, and Shakir Ullah contributed to data collection and data analysis. Latif Ullah, Nasar Khan, and Aiman Rahman were involved in data collection and literature review. Amna Bibi and Shehnaz Malik contributed to data collection and data organization. Shah Hussain was responsible for data analysis and interpretation.
Ethical Approval
Ethical approval for the study was obtained from Saidu Teaching Hospital, Swat (Ref No. SGTH/IRB/2026/12).
Conflict of Interest Statement
The authors declare that there is no conflict of interest.
Guarantor
Nasar Mian is the guarantor of this study and takes full responsibility for the integrity of the data and the accuracy of the data analysis.
DOI
Cite this Article
Nasar M, Ali J, Mian IA, et al. The knowledge of pregnant women regarding antenatal care in selected government hospitals at District Swat. medtigo J Med. 2026;4(1):e3062416. doi:10.63096/medtigo3062416 Crossref













