







 Author Affiliations
Author Affiliations
Abstract
Background: Bell’s Palsy is an idiopathic, non-progressive neuropathy of the facial nerve occurring in a lower motor neuron pattern. The treatment conventionally consists of steroids, but the effectiveness of the addition of antivirals such as acyclovir, valacyclovir, and famciclovir is not established. Our study aims to assess the effectiveness of antiviral drugs for the treatment of Bell’s Palsy patients.
Methods: A systematic search was performed on PubMed, Cochrane Library, and ClinicalTrials.gov, from January 1992 to December 2022, to collect randomized controlled trials (RCTs) considering the addition of antivirals in treating Bell’s palsy. The bibliographies of the identified trials and Google Scholar were reviewed to identify additional data. A meta-analysis was launched to assess the overall facial recovery, measured in terms of the odds ratios (ORs) and a corresponding 95% confidence interval (CI). Secondary outcomes are adverse effects attributable to the use of antivirals.
Results: A total of 18 studies were included in the qualitative synthesis of this systematic review. Among the included studies, 15 studies representing 2,563 patients contributed to the meta-analysis. There were statistically significant differences in complete facial recovery between the antiviral group and the comparison group, with a pooled odds ratio of 1.79 (95% CI: 1.24-2.60, P= 0.002), indicating higher recovery outcomes in the antiviral group.
Conclusion: Overall, adding antivirals to the therapy provided a significant additional benefit in facial recovery from Bell’s Palsy. Adding antiviral drugs such as acyclovir, valacyclovir, and famciclovir to the conventional therapy consisting of steroids achieves a better treatment for Bell’s palsy patients.
Keywords
Bell’s Palsy, Acyclovir, Valacyclovir, Famciclovir, Antivirals
Introduction
Bell’s palsy, also known as idiopathic facial palsy, is a non-progressive neurological disorder of the facial nerve (7th cranial nerve), considered the most common cranial neuropathy. It is characterized by a spontaneous acute paralysis of the face that occurs temporarily in a lower motor neuron pattern and may be preceded by weakness on one side of the face [1]. Additional symptoms commonly include numbness and mild pain, especially around the ear on the weak side, associated with an unusually high sensitivity to sound stimuli and a disturbed sense of taste [1]. Epidemiological studies have reported an annual incidence of 15 to 30 per 100,000 people, regardless of age and gender, and a peak incidence between the ages of 15 and 45, with about 1 in 60 lifetime risks [2]. Decreased blood supply (ischemia) and compression of the facial nerve are the direct contributors to facial paralysis, but the exact etiology of Bell’s palsy is still debated. The inherited tendency, viral infections (e.g., herpes simplex virus, herpes zoster virus), and immune disorders are frequently proposed as a causes for this disorder, and many possible pathological mechanisms have been recently suggested [3]. Although the precise cause of Bell’s palsy is unclear, viral infection remains the widely accepted etiology, based on serological evidence reporting seropositive for Herpes Simplex virus (HSV) in Bell’s Palsy patients, mainly HSV-1 and HSV-2 [3, 4, 5]. As the HSV can be transformed into its latent form, “virion”, it can survive many treatments and conditions. This is why they are commonly not completely eradicated and remain present in the trigeminal ganglia of the human body, causing many neurodegenerative illnesses after their reactivation. Based on this evidence, some physicians prescribe antiviral treatments (such as acyclovir, valacyclovir, and famciclovir) for the treatment of this type of facial nerve paralysis, being capable of eradicating Herpes Simplex Virus and other viral infections [6].
Acyclovir and its prodrugs valacyclovir and famciclovir are the gold standards in treating the herpes virus infections. Their mechanism of action is focused on targeting viral replication through the inhibition of DNA polymerase [7]. Valacyclovir has a higher bioavailability, and although it is claimed to lead to steadier plasma concentration, its way of action is identical to acyclovir’s [8].
The outcome of Bell’s palsy is frequently favorable even without treatment, but convenient and effective treatment can significantly increase the likelihood of improvement in terms of a shorter time to a complete recovery. Most clinicians treat patients with corticosteroids, as they are proven from many randomized controlled trials to have a significant efficacy [9]. Furthermore, the addition of antiviral drugs into the therapy has gained popularity and was widely suggested in recently published guidelines, such as the American Academy of Neurology, but has not yet been established [10]. Many clinical trials were performed to validate the effectiveness of antiviral drugs for the treatment of idiopathic facial paralysis; some trials advocated for steroid monotherapy [11, 12], and others found a benefit in the combination of steroids and antivirals [13, 14]. Therefore, no clear consensus exists, and the best treatment remains variable and unclear. Given the conflicting data, we performed this systematic review and meta-analysis to gather additional powered randomized controlled trials, to robustly determine whether the use of acyclovir/valacyclovir/famciclovir provides a significant effectiveness in the treatment of Bell’s Palsy patients, alone or in combination with other proven effective drugs such as steroids, in comparison with control therapies without antivirals. Our aim of interest is to resolve this uncertainty, to achieve the best therapy for idiopathic facial palsy that can reduce facial nerve damage and optimize the patient’s chance for a complete recovery by improving facial nerve function.
Methodology
This systematic review was conducted to the suggested “Preferred Reporting Items for Systematic Review and Meta-analysis” (PRISMA) 2020 guidelines [15], and its protocol was registered in PROSPERO (https://www.crd.york.ac.uk/prospero/), with the registration number 42022365585.
Search strategy
We performed a systematic electronic database and registry search for studies published on PubMed, Cochrane Library, and ClinicalTrials.gov, from January 1992 to December 2022, to identify randomized controlled trials over the last 30 years dealing with antiviral treatment for patients with Bell’s palsy, without any restrictions on language. The bibliographies of the identified trials and Google Scholar were reviewed to identify additional published or unpublished studies not included in the initial search.
The following Medical Subject Headings (MeSH) terms and keywords were used in the search: “bell’s palsy”, “bell palsy”, “herpetic facial paralysis”, “idiopathic facial palsy”, “idiopathic facial paralysis”, “antiviral drugs”, “antiviral agents”, “antivirals”, “antiviral treatments”, “acyclovir”, “aciclovir”, “valacyclovir”, “valaciclovir”, “famciclovir”, “famcyclovir”, “facial recovery”, “Hemifacial spasms”, “complete recovery”, “partial recovery”.
Study selection and eligibility criteria
Studies that met the following eligibility criteria were included: 1) RCTs of antiviral therapy (acyclovir, valacyclovir, famciclovir, or other analogs), alone or in combination with any other drug, in comparison with control therapies (without antivirals), irrespective of the route of administration (oral or parenteral) and length of the treatment, 2) study population of at least 40 Bell’s palsy patients, and 3) a follow-up period of at least 2 weeks and sufficient outcome data. Participants of any age with clinically diagnosed Bell’s palsy were included, irrespective of the time of evolution of symptoms or any associated conditions.
We excluded trials in which a drug considered effective for treating Bell’s palsy was given to the control group (e.g., corticosteroid drugs such as prednisone) unless it was given in a similar way to the experimental group. We also excluded trials comparing different types of antivirals or different dosage schemes, unless they included a placebo group. Titles and abstracts were screened to identify potentially eligible studies. Then, full-text papers were assessed for eligibility by one author (SD) and checked independently by another author (CH). The number of identified, included, and excluded records is mapped out by a flow diagram that depicts the flow of information through the different phases, presented in the PRISMA statement [15].
Data extraction
Data on trial details, treatments, and outcomes were extracted and recorded into a standardized data extraction sheet. If multiple follow-up periods existed in a study, only data at the longest follow-up point were collected. The outcome of interest was the complete facial recovery of Bell’s palsy patients after receiving the treatment. Secondary outcomes were adverse effects attributable to the given therapy. The following information was extracted from all the studies by the author (SD): first author; year of publication; study design; study setting; sample size (with the number of patients in each treatment group); basic patient characteristics (i.e., mean age, gender); type of intervention and comparator with administered doses; primary and secondary outcomes; and length of follow-up.
Statistical analysis
The data included trial details and adverse effects were summarized and presented in a tabulated form for the qualitative comparison across studies to determine the effect of adding antivirals to the therapy of Bell’s palsy. For the meta-analysis, the OR and corresponding 95% CI of each study were pooled and evaluated for outcomes. An OR of greater than “one” favors the antiviral treatment, and it was considered statistically significant at the P <0.05 level if the 95% CI excludes the value “one”. The heterogeneity among the trials was assessed by the I2 statistic [16], which describes the percentage of total variation attributable to heterogeneity rather than chance alone, “homogeneity”, using the thresholds in the Cochrane Handbook for Systematic Reviews of Interventions as guidance. If heterogeneity was present, odds ratios were calculated using the random effects model. The results of the meta-analysis were presented in a forest plot displaying the results from each study and the corresponding 95% CI. We assessed the likelihood of publication and small-study bias by visual inspection of the funnel plot [17]. The meta-analysis was performed using Review Manager (RevMan) (Computer program). Version 5.4. The Cochrane Collaboration, 2020.
Results
Search results
A total of 67 records were identified from PubMed, Cochrane Library, Clinicaltrials.gov, and Google Scholar. After duplicate removal, 46 studies were available for screening based on their titles and abstracts. We excluded 21 articles due to irrelevance and non-conformity to the inclusion criteria. After assessing the full texts for eligibility, we excluded seven studies for the following reasons: inadequate study population, inadequate study design (not randomized controlled trials), very short follow-up period (two weeks or less), and insufficient outcome data. Ultimately, 18 studies were included in the qualitative synthesis of this systematic review, and we adopted 15 studies for the quantitative synthesis (meta-analysis). The detailed steps of study selection are shown in the flow diagram. (Figure 1)
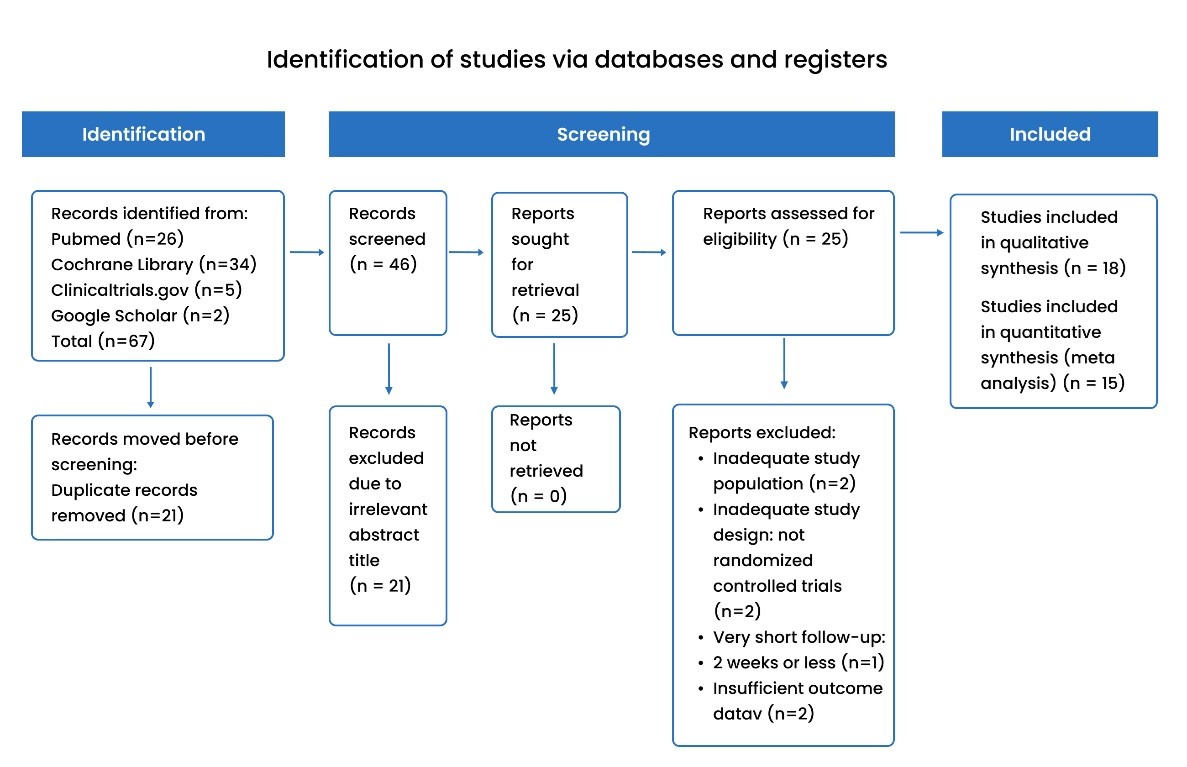
Figure 1: PRISMA flow diagram of the different phases of the study selection process [15].
Characteristics of included studies
Of the 18 eligible articles, 15 studies were direct RCTs and were included in the qualitative synthesis and the meta-analysis: 10 were double-blinded [11,12,13,14,18,19,20,21,22,23], one was single-blinded [24], three were not blinded [25,26,27], and one was not clear about the blinding process [28]. The three remaining studies were included in the qualitative synthesis: two studies reported separately secondary outcomes of antiviral drugs from the previously done RCT “Engstrom et al., 2008” [29, 30], and one study assessed the cost-effectiveness of antivirals using secondary data from previous RCTs [31].
All 15 studies compared recovery rates of antiviral drugs with steroids versus steroids alone. Among these 15 studies, 2 studies also compared recovery rates of antiviral treatment alone versus placebo [11, 12]. Antiviral drugs included: acyclovir for eight studies, valacyclovir for four studies, and famciclovir for three studies. The steroids used were prednisone, prednisolone, or methylprednisolone.
A total of 2,563 Bell’s palsy patients were involved in the analysis: 1,283 patients were in the intervention group and received antiviral drugs in their treatment, and 1,280 patients were in the control group. The follow-up periods ranged from 4 weeks to 12 months. The mean age of patients ranged from 9 to 51 years old, and the percentage of male participants ranged from 39% to 70%. The study demographics and clinical characteristics of each included RCT are shown in Table 1
| First author
(Year) |
Study setting | Study design | Sample size | Mean age | % Males | Type of antiviral | Treatment | Length of follow-up | |
| Intervention group (dose) | Control group (dose) | ||||||||
| Adour
(1996) |
United States | RCT (double-blind) | 99 | 43 | 49 | Acyclovir | – Acyclovir (400 mg 5 times daily for 10 days)
– Prednisone (1 mg/kg for 5 days tapered to 10 mg/day for the remaining 5 days) |
Prednisone (the same regimen) | 4 months |
| Chen
(2005) |
China | RCT (-) | 46 | – | – | Acyclovir | – Acyclovir (400 mg 3 times daily for 5 days)
– Prednisone (50 mg/d for 5 days then reduced by 20 mg per 2 days for the next 10 days) |
Prednisone (the same regimen) | 4 weeks |
| Engstrom
(2008) |
Sweden and Finland | RCT (double-blind) | 829 | 40 | 59 | Valacyclovir | – Valaciclovir (1000 mg three times daily for 7 days)
– Prednisolone 60 mg/d for 5 days then reduced by 10 mg per day (for a total treatment time of 10 days) |
Prednisolone (the same regimen) | 12 months |
| – Valaciclovir (1000 mg 3 times daily for 7 days) | Placebo | ||||||||
| Hato (2007) | Japan | RCT (single-blind) | 221 | 50 | 53 | Valacyclovir | – Valacyclovir (1,000 mg/d for 5 days)
– Prednisolone (60 mg/d for 5 days, 30 mg/d for 3 days, and 10 mg/d per day for 2 days) |
Prednisolone (the same regimen) | 6 months |
| Kawaguchi
(2007) |
Japan | RCT (double-blind) | 150 | 51 | 60 | Valacyclovir | – Valaciclovir (500 mg 2 times daily for 5 days)
– Prednisolone (20 mg 3 times daily for 5 days, 10 mg 3 times daily for 2 days, and 10 mg daily for 2 days) |
Prednisolone (the same regimen) | 6 months |
| Khajeh
(2015) |
Zahedan, Iran | RCT (not blinded) | 43 | 9 | 53 | Acyclovir | – Acyclovir (10 mg/kg every 8 hours for 7 days)
– Prednisolone (2 mg/kg daily for 7 days) |
Prednisolone (the same regimen) | 3 months |
| Khedr
(2016) |
Egypt | RCT (double-blind) | 50 | 37 | – | Acyclovir | – Acyclovir (400 mg 3 times daily for 5 days)
– Prednisolone (60 mg daily for 7 days) |
Prednisolone (the same regimen) | 3 months |
| Lee
(2013) |
Seoul, Korea | RCT (double-blind) | 206 | 48 | 51 | Famciclovir | – Famciclovir (750 mg/d for 7 days)
-Methylprednisolone (For 10 days, 64 mg/d for the first 4 days tapered to 48 mg/d for 2 days, 32 mg/d for 2 days, and 16 mg/d for 2 days) |
Methylprednisolone (the same regimen) | 6 months |
| Li (1997) | Shaanxi, China | RCT (double-blind) | 46 | 40 | 48 | Acyclovir | – Acyclovir (800 mg 5 times daily for 7 days)
– Prednisone (60 mg for 5 days tapered in steps of 10 mg for a further 5 days) |
Prednisone (the same regimen) | 6 months |
| Minnerop (2008) | Germany | RCT (not blinded) | 117 | 42 | 51 | Famciclovir | – Famciclovir (250 mg 3 times daily for 7 days)
– Prednisolone (1 mg/kg for 4 days tapered over the following 8 days) |
Prednisolone (the same regimen) | 3 months |
| Shahidullah
(2011) |
Bangladesh | RCT (not blinded) | 68 | 33 | 70 | Famciclovir | – Famciclovir (250 mg 3 times daily for 5 days)
– Prednisolone (60 mg daily for 7 days) |
Prednisolone (the same regimen) | 3 months |
| Sullivan
(2007) |
Scotland, United Kingdom | RCT (double-blind) | 496 | 44 | 51 | Acyclovir | – Acyclovir (400 mg 5 times daily for 10 days)
– Prednisolone (25 mg twice daily for 10 days) |
Prednisolone (at the same regimen) | 9 months |
| – Acyclovir (400 mg 5 times daily for 10 days) | Placebo (lactose) | ||||||||
| Talib
(2021) |
Pakistan | RCT (double-blind) | 60 | 36 | 58 | Acyclovir | – Acyclovir (400 mg 4 times daily for 10 days)
– Prednisolone (1 mg/kg for 10 days) |
Prednisolone (at the same regimen) | 8 weeks |
| Vázquez
(2008) |
Uruguay | RCT (double-blind) | 41 | 41 | 39 | Valacyclovir | – Valaciclovir (2 g for 7 days)
– Prednisone (1 mg/kg for 7 days then reduced for 14 days) |
Prednisone (the same regimen) | 6 months |
| Yeo
(2008) |
South Korea | RCT (double-blind) | 91 | 41 | 45 | Acyclovir | – Acyclovir (2400 mg/d for 5 days)
– Prednisone (1 mg/kg/d (maximum: 80 mg/d) for 4 days, reduced to 60 mg/d on days 5 and 6, 40 mg on days 7 and 8, and 20 mg on days 9 and 10) |
Prednisone (the same regimen) | 6 months |
Table 1: Study demographics and clinical characteristics of included RCT studies.
Outcomes of meta-analysis and heterogeneity assessment
The proportion of patients with complete recovery found in both the intervention (antivirals) and the control (no antivirals) group is shown in Table 2. The pooled proportion of Bell’s palsy patients who achieved complete facial recovery is 83.4% (1,070/1,283) among those who received antiviral drugs in their therapy, compared with 77.7% (995/1280) in those who did not receive antivirals.
Owing to the suggested heterogeneity assessed by the I2 statistic (Chi2= 36.32, P= 0.003, I2= 56%), the random-effect meta-analysis model was applied to assess antiviral effects. An OR of greater than “one” indicates that the intervention group had a higher recovery than the control group, whereas an OR of less than “one” indicates that the intervention group had a lower recovery than the comparison group. ORs were considered statistically significant at the P<0.05 level if the 95% CI excluded the value “one”. The OR significantly favored antiviral therapy in five studies [13,14,18,20,27]. The remaining trials had 95% confidence intervals crossing the value “1” indicating no statistical significance. After performing a meta-analysis that includes all 15 studies (with 2 studies containing 2 trials each [11, 12], there were statistically significant differences in complete facial recovery between the antiviral group and the comparison group (OR= 1.79, 95% CI: 1.24-2.60, P= 0.002). These results are presented in a forest plot displaying the results from each study, ORs, and the corresponding 95% CI (Figure 2).
| Antivirals | No Antivirals | |
| Complete recovery (%) | 1,070 (83.4%) | 995 (77.7%) |
| No complete recovery (%) | 213 (16.6%) | 285 (22.3%) |
| Total | 1,283 (100%) | 1,280 (100%) |
Table 2: Proportions of recovery among treatment groups (antivirals and no-antivirals groups) 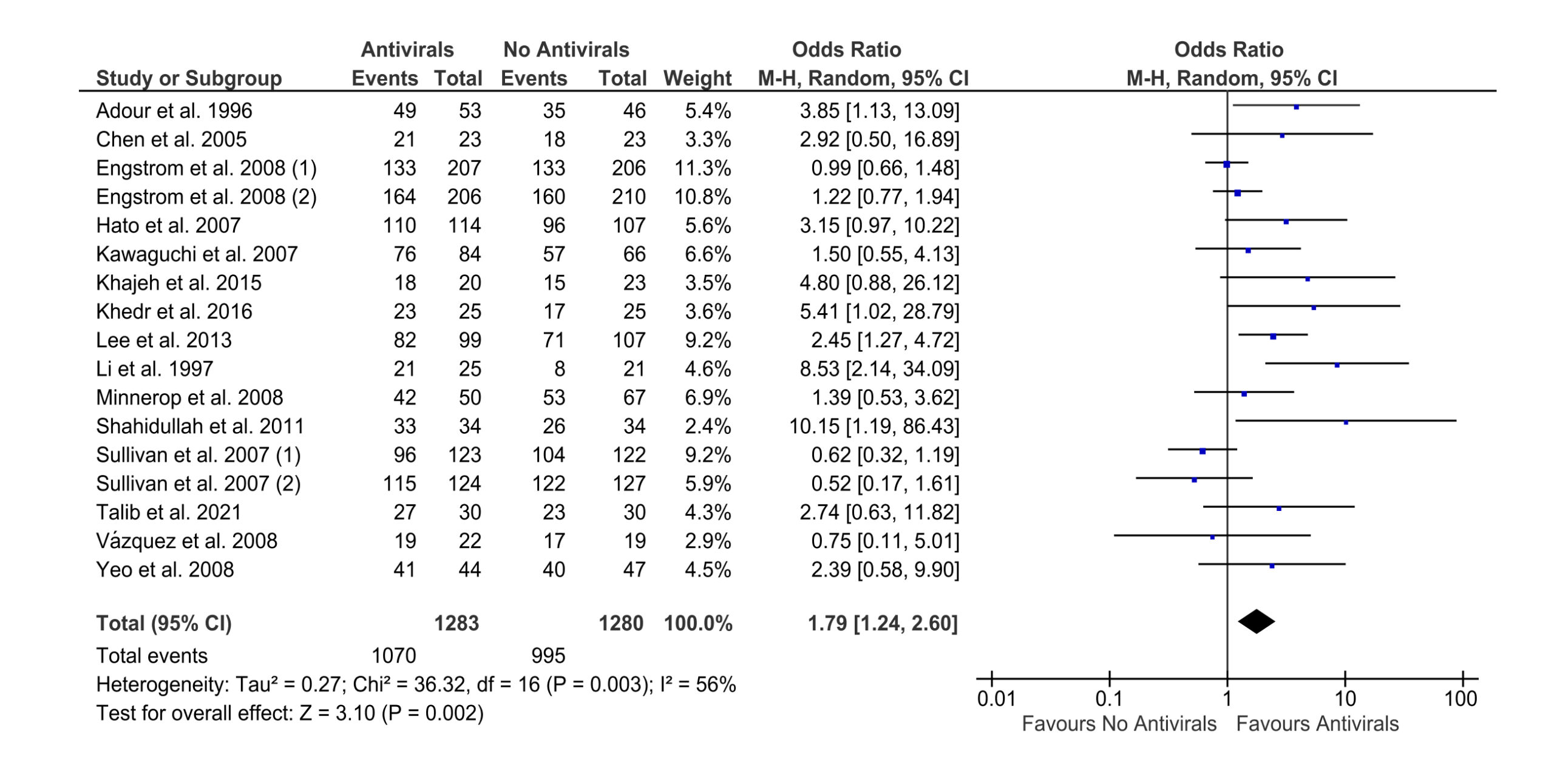
Figure 2: Forest plot of the included RCT studies in the meta-analysis showing the odds ratio estimates and their 95% confidence intervals, based on a random-effect model
Subgroup analysis
Given the detected heterogeneity between the trials (P< 0.05), we performed subgroup analyses to detect the possible sources of heterogeneity. The studies were stratified according to the type of administered antiviral: acyclovir, valacyclovir, or famciclovir. Eight studies used the “acyclovir” antiviral drug [12,14,18,20,21,23,25,28], four studies with “valacyclovir” [11,19,22,24], and three studies with “famciclovir” [13,26,27].
The related forest plots are presented in Figures 3, 4, and 5. Subgroup analyses showed statistically significant differences in complete facial recovery between the intervention and the comparison group when the administered antiviral was “acyclovir” (OR= 2.32, 95% CI: 1.09-4.92, P=0.03) or “famciclovir” (OR= 2.36, 95% CI: 1.41-3.95, P= 0.001). There was no significant difference when “valacyclovir” was used in the therapy (OR= 1.18, 95% CI: 0.89-1.55, P= 0.25). The fixed-effect model was applied instead of the random-effect model to assess the effect of valacyclovir and famciclovir, owing to their non/low heterogeneity assessed by the I2 statistic: valacyclovir (Chi2= 3.89, P= 0.42, I2= 0%), famciclovir (Chi2= 2.97, P= 0.23, I2= 33%).
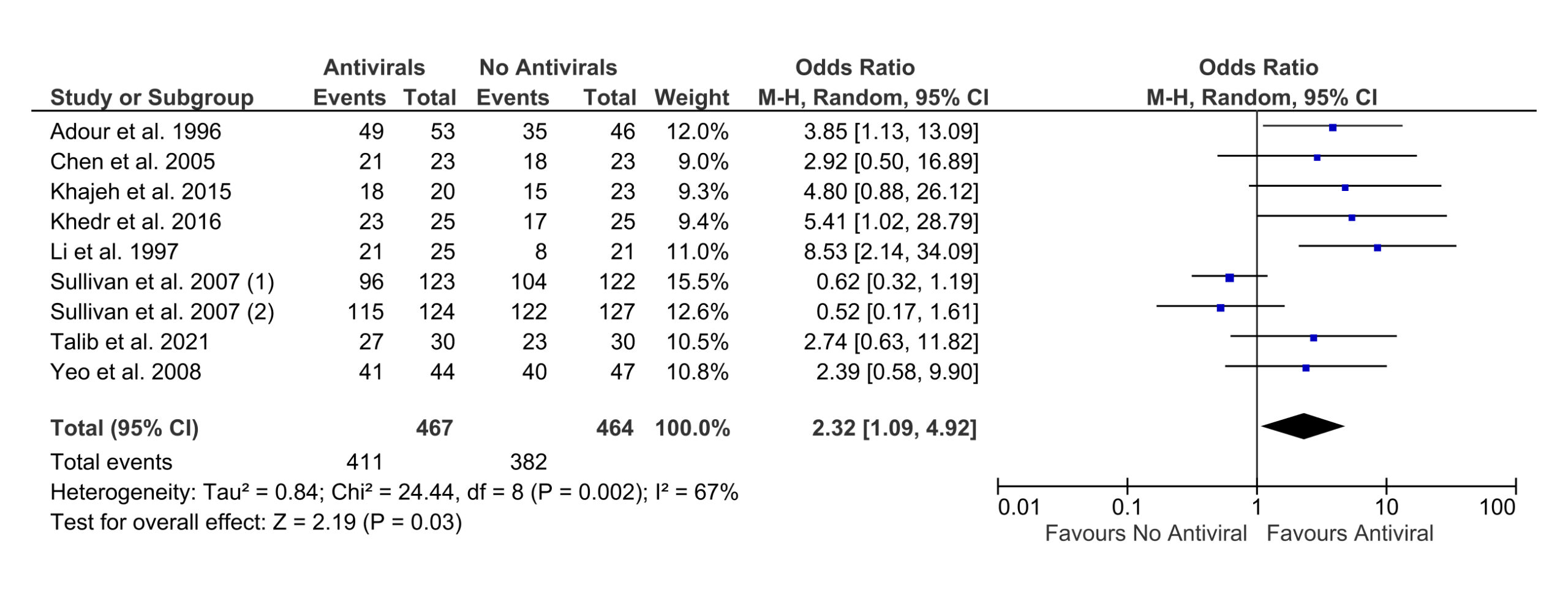
Figure 3: Forest plot of included studies with “acyclovir” antiviral drug
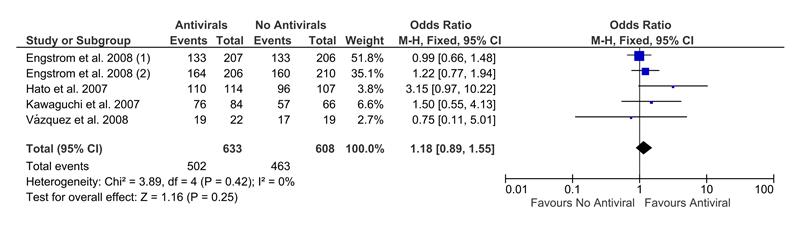
Figure 4: Forest plot of the included studies with “valacyclovir” antiviral drug
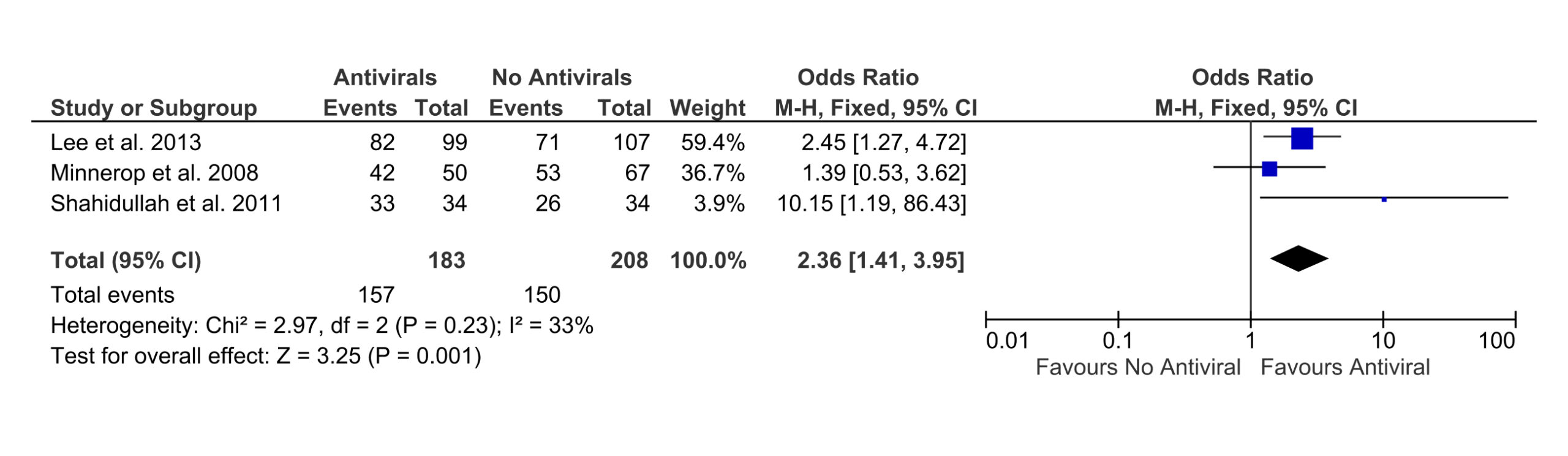
Figure 5: Forest plot of the included studies with “famciclovir” antiviral drug.
Adverse effects
The presence or absence of adverse effects of the administered treatments was reported by 12 studies [11,12,13,14,18,20,22,24,26,28,29,30]. Among all the studies, no serious complications were encountered in patients, with no significant effect of antiviral drugs on the presence of synkinesis or the incidence (or the intensity) of pain. Some RCTs reported mild gastrointestinal complaints, fever, dizziness, nausea, and headache. The adverse effects are presented qualitatively in the summary of findings table (Table 3), with the reported effects of antiviral drugs in each study.
| Study | Reported effect of antiviral drug | Adverse events |
| Adour et al.
(1996) |
– Acyclovir-prednisone is superior to prednisone alone in treating Bell’s palsy patients.
– Suggestion that herpes simplex is the probable cause of Bell’s palsy. |
Gastrointestinal complaints were the most frequently encountered problems; all such complaints were mild to moderate and did not require treatment. |
| Axelsson et al.
(2012) |
Valaciclovir did not add any significant effect to prednisolone regarding recovery rate. | No significant effect of valaciclovir on the presence of synkinesis. |
| Berg et al.
(2009) |
– | Valacyclovir did not affect the incidence or intensity of ipsilateral pain in Bell’s palsy. |
| Chen et al.
(2005) |
Acyclovir-prednisone had a significantly better outcome in the treatment of Bell’s palsy as compared with prednisone treatment. | No serious complications. |
| Engstrom et al.
(2008) |
Valaciclovir did not affect facial recovery. | – Non-serious adverse events.
– The number of patients with adverse events did not differ between the groups: abdominal/thoracic pain, fever, tongue swelling, and weight gain. |
| Hato et al.
(2007) |
The valacyclovir and prednisolone therapy was more effective in treating Bell’s palsy than the conventional prednisolone therapy. | No severe adverse effects, although mild gastrointestinal complications were reported. |
| Hernandez et al.
(2009) |
– The treatment without acyclovir has on average lower costs and a higher proportion of individuals recovered.
– Acyclovir is highly unlikely to be considered cost-effective. |
– |
| Kawaguchi et al.
(2007) |
Valacyclovir did not add any significant difference in recovery rates.
|
– |
| Khajeh et al.
(2015) |
The combined prednisolone and acyclovir therapy is far more effective than treatment with prednisolone alone. | – |
| Khedr et al.
(2016) |
The combination of steroid and antiviral treatment increases the possibility of recovery in moderately severe to
complete acute Bell’s palsy. |
No side effects. |
| Lee et al.
(2013) |
Combined treatment with a steroid and an antiviral agent is more effective in treating severe to complete Bell’s palsy than steroid treatment alone. | Side effects of antiviral agents occur in 10% to 20% of all cases, and the most common symptoms are nausea, vomiting, and headache. |
| Li et al.
(1997) |
Combined acyclovir and prednisone therapy can shorten the time to recovery, and improve outcome. | Acyclovir was well tolerated, and there were no untoward side effects or symptoms. |
| Minnerop et al.
(2008) |
A combined treatment
of famciclovir and prednisolone had significantly better chances of recovery and should be considered (at least) in patients with severe BP. |
Skin rash, hair loss. |
| Shahidullah et al.
(2011) |
A considerable number of patients benefited from additional antiviral therapy of famciclovir. | – |
| Sullivan et al.
(2007) |
There is no evidence of a benefit of acyclovir given alone or an additional benefit of acyclovir in combination with prednisolone. | – Adverse events included the expected range of minor symptoms associated with the drugs used (dizziness, dyspepsia, nausea).
– No serious adverse events in any group. |
| Talib et al.
(2021) |
The combination treatment of antiviral-steroids has shown improvement in both recovery and quality of life. | – |
| Vazquez et al.
(2008) |
Antiviral treatment had no additional benefit for Bell’s palsy. | – The only adverse effect recorded was epigastric discomfort and it did not require any treatment.
– The comparison of resting symmetry, voluntary, and total movement scores between the groups showed no significant differences.
|
| Yeo et al.
(2008) |
The benefit of acyclovir in Bell’s palsy has not been definitively established. | – |
Table 3: Summary of findings table and adverse effects reported in each included study
Sensitivity analysis
To investigate the robustness of the obtained results, we performed a sensitivity analysis by comparing the results from both the random-effect model and the fixed-effect model in meta-analysis. There were statistically significant differences in complete facial recovery between the antiviral group and the comparison group using the fixed effect model (OR= 1.45, 95% CI: 1.18-1.78, P= 0.0003), consistently with the random-effect model (Figure 6).
Figure 6: Forest plot of the included RCT studies in the meta-analysis showing the odds ratio estimates and their 95% confidence intervals, based on a fixed effect model
Publication and small-study bias
The likelihood of publication and small-study bias was assessed by visual inspection of the funnel plot [17], where each included study is represented by a dot (Figure 7). The funnel plot shows some asymmetry in the distribution of the included RCTs, suggesting the possibility of publication bias.

Figure 7: Funnel plot of the included RCT studies to detect the presence of publication and small-study bias in the meta-analysis. Each included study is represented by a dot.
Discussion
Idiopathic facial palsy, named “Bell’s palsy”, is a dysfunction of the peripheral facial nerve that appears as an acute weakness of the face, and can be unilateral or bilateral [1]. The precise cause is unknown, but there is some evidence that it may be engendered by viral infections such as the herpes simplex virus (HSV) [1]. Many researchers have been interested in finding the best treatment for Bell’s palsy to increase the likelihood of complete facial recovery. In this study, we launched a systematic review to collect randomized controlled trials that consider antivirals for treating Bell’s palsy patients, and we performed a meta-analysis to assess the effectiveness of antiviral drugs in this field, to reach the best treatment.
Our meta-analysis included data from 15 RCTs containing over 2,500 patients and demonstrated that the presence of antivirals in the therapy provided significantly better outcomes in terms of a complete facial recovery, and the pooled odds ratio for complete recovery among patients was OR= 1.79 with a 95% CI: 1.24-2.60, P= 0.002. Most of these RCTs assessed the effect of the addition of antiviral drugs to steroids in comparison to steroids alone without antivirals.
Subgroup analyses indicated a significant effectiveness in the addition of acyclovir and famciclovir to the treatment, with pooled odds ratios respectively: OR= 2.32, 95% CI: 1.09-4.92, P=0.03 and OR= 2.36, 95% CI: 1.41-3.95, P= 0.001. Our results are consistent with other previous meta-analyses that were performed in this field: Numthavaj et al. [32] suggested that antiviral treatments could be added to prednisone and may provide slightly better recovery, and Fu et al. [33] showed that antiviral addition to steroid therapy is superior to steroid therapy alone.
To provide a solid conclusion on the effect of antivirals on idiopathic facial palsy, our meta-analysis was performed to gather powerful RCTs that compare antivirals and non-antiviral therapies, to achieve the best treatment capable of reducing facial nerve weakness and optimizing complete recovery after paralysis. The study settings and countries of the included RCTs were widely diverse, leading to more likely generalizable results for many Bell’s palsy patients.
However, some features existed among the studies and need to be defined: First, there were different scales assessing the degree of facial recovery in patients: The House-Brackmann scale, facial paralysis recovery index, Yanagihara rating scale which is the conversion scale to the House-Brackmann scale, Sunnybrook scale and these various scales might lead to heterogeneity between trials. Second, the degree of severity of acute Bell’s palsy varies among patients from mild to severe, or in different ascending levels, leading to different times of recovery no matter of the administered treatment. More trials grouping Bell’s palsy patients by severity of the pathology need to be performed. Moreover, many Bell’s palsy patients have positive serological evidence of viruses such as herpes simplex virus (HSV), as the HSV antibodies (IgG and IgM) were present in the blood samples in 70% of patients [34]. The remaining patients had IgG and IgM negative, meaning the absence of viral infection.
From this perspective, future trials should focus on considering antiviral drugs for seropositive Bell’s palsy patients specifically, to detect the effectiveness of antiviral drugs among patients who have a present viral infection. In addition, future studies should be done with a focus on the quality of the included studies to assess the impact of excluding low-quality studies on the results. This systematic review provided a robust conclusion and extensive insight in terms of the best treatment for Bell’s palsy patients for a complete recovery. Antiviral drugs were well tolerated, and there were no serious complications.
Scientific contribution
The effectiveness of antivirals in the treatment of Bell’s palsy has not yet been established in complete facial recovery. This systematic review and meta-analysis needed to be performed to provide a comprehensive assessment of the cumulative evidence on the effect of the addition of antivirals into Bell’s palsy treatment. This offers increased statistical power by pooling data from powered randomized controlled trials that are done in this field and provides more robust insights and precise estimates by analyzing larger datasets of Bell’s palsy patients.
This study robustly showed a statistically significant added therapeutic benefit of adding antivirals to the treatment of Bell’s palsy patients in complete facial recovery, compared with no-antiviral treatment. These findings help to inform decision-making for the treatment of Bell’s palsy patients, they support the current practice of clinicians suggesting using antiviral drugs added to the conventional therapy consisting of steroids.
Conclusion
In conclusion, our evidence suggests that a better treatment therapy for Bell’s palsy could be achieved by the addition of antiviral drugs such as acyclovir, valacyclovir, and famciclovir. There was a statistically significant added therapeutic benefit in achieving complete facial recovery when antivirals were added to the therapy, compared with no-antiviral therapy. Therefore, our robust meta-analysis supports the current practice of clinicians suggesting treating Bell’s palsy patients using antiviral drugs, added to the conventional therapy consisting of steroids. Future studies should be carried out to assess the effectiveness of antivirals in Bell’s palsy patients limited to having positive serological evidence of viral infection, or to identify their effectiveness in Bell’s palsy patients who have a similar degree of severity, to be able to compare the recovery rates more precisely.
References
- Holland NJ, Bernstein JM. Bell’s palsy. BMJ Clin Evid. 2014;2014:1204. Bell’s palsy PubMed | Google Scholar
- Greco A, Gallo A, Fusconi M, Marinelli C, Macri GF, de Vincentiis M. Bell’s palsy and autoimmunity. Autoimmun Rev. 2012;12(2):323-328. doi:10.1016/j.autrev.2012.05.008 PubMed | Crossref | Google Scholar
- Lackner A, Kessler HH, Walch C, Quasthoff S, Raggam RB. Early and reliable detection of herpes simplex virus type 1 and varicella zoster virus DNAs in oral fluid of patients with idiopathic peripheral facial nerve palsy: Decision support regarding antiviral treatment?. J Med Virol. 2010;82(9):1582-1585. doi:10.1002/jmv.21849 PubMed | Crossref | Google Scholar
- Murakami S, Mizobuchi M, Nakashiro Y, Doi T, Hato N, Yanagihara N. Bell palsy and herpes simplex virus: identification of viral DNA in endoneurial fluid and muscle. Ann Intern Med. 1996;124(1 Pt 1):27-30. doi:10.7326/0003-4819-124-1_part_1-199601010-00005 PubMed | Crossref | Google Scholar
- Khine H, Mayers M, Avner JR, Fox A, Herold B, Goldman DL. Association between herpes simplex virus-1 infection and idiopathic unilateral facial paralysis in children and adolescents. Pediatr Infect Dis J. 2008;27(5):468-469. doi:10.1097/INF.0b013e31816507c3 PubMed | Crossref | Google Scholar
- Kłysik K, Pietraszek A, Karewicz A, Nowakowska M. Acyclovir in the Treatment of Herpes Viruses – A Review. Curr Med Chem. 2020;27(24):4118-4137. doi:10.2174/0929867325666180309105519 PubMed | Crossref | Google Scholar
- Kausar S, Said Khan F, Ishaq Mujeeb Ur Rehman M, et al. A review: Mechanism of action of antiviral drugs. Int J Immunopathol Pharmacol. 2021;35:20587384211002621. doi:10.1177/20587384211002621 PubMed | Crossref | Google Scholar
- Schuster AK, Harder BC, Schlichtenbrede FC, Jarczok MN, Tesarz J. Valacyclovir versus acyclovir for the treatment of herpes zoster ophthalmicus in immunocompetent patients. Cochrane Database Syst Rev. 2016;11(11):CD011503. Published 2016 Nov 14. doi:10.1002/14651858.CD011503.pub2 PubMed | Crossref | Google Scholar
- Madhok VB, Gagyor I, Daly F, et al. Corticosteroids for Bell’s palsy (idiopathic facial paralysis). Cochrane Database Syst Rev. 2016;7(7):CD001942. Published 2016 Jul 18. doi:10.1002/14651858.CD001942.pub5 PubMed | Crossref | Google Scholar
- Reich SG. Bell’s Palsy. Continuum (Minneap Minn). 2017;23(2, Selected Topics in Outpatient Neurology):447-466. doi:10.1212/CON.0000000000000447 PubMed | Crossref | Google Scholar
- Engström M, Berg T, Stjernquist-Desatnik A, et al. Prednisolone and valaciclovir in Bell’s palsy: a randomised, double-blind, placebo-controlled, multicentre trial. Lancet Neurol. 2008;7(11):993-1000. doi:10.1016/S1474-4422(08)70221-7 PubMed | Crossref | Google Scholar
- Sullivan FM, Swan IR, Donnan PT, et al. Early treatment with prednisolone or acyclovir in Bell’s palsy. N Engl J Med. 2007;357(16):1598-1607. doi:10.1056/NEJMoa072006 PubMed | Crossref | Google Scholar
- Lee HY, Byun JY, Park MS, Yeo SG. Steroid-antiviral treatment improves the recovery rate in patients with severe Bell’s palsy. Am J Med. 2013;126(4):336-341. doi:10.1016/j.amjmed.2012.08.020 PubMed | Crossref | Google Scholar
- Khedr EM, Badry R, Ali AM, et al. Steroid/Antiviral for the treatment of Bell’s palsy: Double blind randomized clinical trial. Restor Neurol Neurosci. 2016;34(6):897-905. doi:10.3233/RNN-150605 PubMed | Crossref | Google Scholar
- Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. Published 2021 Mar 29. doi:10.1136/bmj.n71 PubMed | Crossref | Google Scholar
- Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557-560. doi:10.1136/bmj.327.7414.557 PubMed | Crossref | Google Scholar
- Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629-634. doi:10.1136/bmj.315.7109.629 PubMed | Crossref | Google Scholar
- Adour KK, Ruboyianes JM, Von Doersten PG, et al. Bell’s palsy treatment with acyclovir and prednisone compared with prednisone alone: a double-blind, randomized, controlled trial. Ann Otol Rhinol Laryngol. 1996;105(5):371-378. doi:10.1177/000348949610500508 PubMed | Crossref | Google Scholar
- Kawaguchi K, Inamura H, Abe Y, et al. Reactivation of herpes simplex virus type 1 and varicella-zoster virus and therapeutic effects of combination therapy with prednisolone and valacyclovir in patients with Bell’s palsy. Laryngoscope. 2007;117(1):147-156. doi:10.1097/01.mlg.0000248737.65607.9e PubMed | Crossref | Google Scholar
- Li Y, Gao P, Mao X, Cao P. Randomized clinical trial of acyclovir plus prednisone versus prednisone alone in Bell’s palsy. Ceylon Journal of Medical Science 1997;40(2):37‐41. Randomized clinical trial of aciclovir plus prednisone versus prednisone alone in Bell’s palsy
- Talib A, Baloch G, Haider Naqvi I, Ubaid M. Steroids with and without antivirals in the treatment of Bell’s Palsy: Does it make any difference in recovery? A study at a tertiary care center, Karachi, Pakistan. Arch Neurosci. 2021;8(3). doi:10.5812/ans.115645 Crossref | Google Scholar
- Vázquez MC, Sánchez N, Calvo J, Perna A. Eficacia de los antivirales en la parálisis de Bell. Revista Médica del Uruguay. 2008;24(3):167-174. Enfermedad con cuerpos de Lewy – SciELO Google Scholar
- Yeo SG, Lee YC, Park DC, Cha CI. Acyclovir plus steroid vs steroid alone in the treatment of Bell’s palsy. Am J Otolaryngol. 2008;29(3):163-166. doi:10.1016/j.amjoto.2007.05.001 PubMed | Crossref | Google Scholar
- Hato N, Yamada H, Kohno H, et al. Valacyclovir and prednisolone treatment for Bell’s palsy: a multicenter, randomized, placebo-controlled study. Otol Neurotol. 2007;28(3):408-413. doi:10.1097/01.mao.0000265190.29969.12 PubMed | Crossref | Google Scholar
- Khajeh A, Fayyazi A, Soleimani G, Miri-Aliabad G, Shaykh Veisi S, Khajeh B. Comparison of the Efficacy of Combination Therapy of Prednisolone – Acyclovir with Prednisolone Alone in Bell’s Palsy. Iran J Child Neurol. 2015;9(2):17-20. Comparison of the Efficacy of Combination Therapy of Prednisolone – Acyclovir with Prednisolone Alone in Bell’s Palsy PubMed | Google Scholar
- Minnerop M, Herbst M, Fimmers R, et al. Bell’s palsy: combined treatment of famciclovir and prednisone is superior to prednisone alone (published correction appears in J Neurol. 2013 Apr;260(4):1200. Kaabar, Pavlina (added)). J Neurol. 2008;255(11):1726-1730. doi:10.1007/s00415-008-0008-6 PubMed | Crossref | Google Scholar
- Shahidullah M, Haque A, Islam MR, et al. Comparative study between combination of famciclovir and prednisolone with prednisolone alone in acute Bell’s palsy. Mymensingh Med J. 2011;20(4):605-613. Comparative study between combination of famciclovir and prednisolone with prednisolone alone in acute Bell’s palsy PubMed | Google Scholar
- Chen WL, Yang ZH, Huang ZQ. Shanghai Kou Qiang Yi Xue. 2005;14(6):590-592. (Outcome of treatment 46 patients with Bell’s palsy with aciclovir and prednisone) PubMed | Google Scholar
- Axelsson S, Berg T, Jonsson L, et al. Bell’s palsy – the effect of prednisolone and/or valaciclovir versus placebo in relation to baseline severity in a randomised controlled trial. Clin Otolaryngol. 2012;37(4):283-290. doi:10.1111/j.1749-4486.2012.02526.x PubMed | Crossref | Google Scholar
- Berg T, Axelsson S, Engström M, et al. The course of pain in Bell’s palsy: treatment with prednisolone and valacyclovir. Otol Neurotol. 2009;30(6):842-846. doi:10.1097/MAO.0b013e3181ab31c8 PubMed | Crossref | Google Scholar
- Hernández RA, Sullivan F, Donnan P, Swan I, Vale L; BELLS Trial Group. Economic evaluation of early administration of prednisolone and/or aciclovir for the treatment of Bell’s palsy. Fam Pract. 2009;26(2):137-144. doi:10.1093/fampra/cmn107 PubMed | Crossref | Google Scholar
- Numthavaj P, Thakkinstian A, Dejthevaporn C, Attia J. Corticosteroid and antiviral therapy for Bell’s palsy: a network meta-analysis. BMC Neurol. 2011;11:1. doi:10.1186/1471-2377-11-1 PubMed | Crossref | Google Scholar
- Fu X, Tang L, Wang C, et al. A Network Meta-Analysis to Compare the Efficacy of Steroid and Antiviral Medications for Facial Paralysis from Bell´s Palsy. Pain Physician. 2018;21(6):559-569. A Network Meta-Analysis to Compare the Efficacy of Steroid and Antiviral Medications for Facial Paralysis from Bell´s Palsy PubMed | Google Scholar
- Musani MA, Farooqui AN, Usman A, et al. Association of herpes simplex virus infection and Bell’s palsy. J Pak Med Assoc. 2009;59(12):823-825. Association of herpes simplex virus infection and Bell’s palsy PubMed | Google Scholar
Acknowledgments
None
Funding
None
Author Information
Corresponding Author:
Sarah Daher
Department of Neurology
Neuroscience Research Center, Lebanese University, Beirut, Lebanon
Email: [email protected]
Co-Authors:
Céline Haddad, Ali Al-Arab
Department of Neurology
Neuroscience Research Center, Lebanese University, Beirut, Lebanon
Authors Contributions
All authors contributed to the conceptualization, investigation, and data curation by acquiring and critically reviewing the selected articles. They were collectively involved in the writing – original draft preparation, and writing – review & editing to refine the manuscript. Additionally, all authors participated in the supervision of the work, ensuring accuracy and completeness. The final manuscript was approved by all named authors for submission to the journal.
Informed Consent
Not applicable
Conflict of Interest Statement
None
Guarantor
Not applicable
DOI
Cite this Article
Daher S, Haddad C, Al-Arab A. The Effect of Antiviral Drugs for the Treatment of Bell’s palsy: A Systematic Review and Meta-analysis. medtigo J Med. 2023;2(3). doi:10.63096/medtigo3062231 Crossref













