






 Author Affiliations
Author Affiliations
Abstract
Background: Access to diagnostic tests in resource-constrained settings is a major hurdle that patients face in their endeavours to receive appropriate healthcare services. A 2016 study found that only 38.5 % of visited health facilities reported the availability of all types of basic laboratory investigations for focused antenatal care in Addis Ababa. The impact of the unavailability of diagnostic tests has dire consequences on the health outcomes of patients in Africa. Additionally, even when it is available, access to diagnostic tests is not guaranteed. Hence, the main objective of this study was to have a comprehensive assessment of the accessibility of diagnostic tests and associated factors, from a patient’s perspective.
Methodology: A cross-sectional study was conducted in Hawassa, Ethiopia, from April 15 to May 15, 2023. Stratified random sampling was used to collect data.
Results: 52% of patients encountered outsourcing of diagnostic tests to another facility due to the unavailability of the tests within the facility. The unavailability of diagnostic tests has various root causes, including stockouts of reagents, malfunctioning machines, and a lack of skilled personnel. Among these, 89.1% encountered this problem two or more times.
Conclusion: Accessing diagnostic tests remains a major hurdle for patients in resource-constrained settings. Access to diagnostic tests has serious implications for health outcomes, and this study focused on assessing access to diagnostic tests from a patient’s perspective.
Keywords
Access to diagnostic tests, Laboratory services, Diagnostic test, Sub-Saharan Africa, Diagnostic tests availability.
Introduction
Access to diagnostic tests in resource-constrained settings is a major hurdle that patients face in their endeavor to receive appropriate healthcare services. The unavailability of diagnostic tests creates a barrier for underserved communities to access optimal and affordable healthcare services. This problem is widespread in developing countries, and it is mainly linked to resource constraints due to a lack of trained professionals, equipment, reagents, and maintenance issues.
A study conducted in the Afar region, Ethiopia, in 2018 revealed that only 52.8% of the facilities have all the essential diagnostic tests required for Focused Antenatal Care (FANC).[1] This serves as a testament to the severity of the problem, as these are basic tests needed for FANC care. In addition, a 2016 study found that only 38.5 % of visited health facilities reported the availability of all types of basic FANC laboratory investigations in Addis Ababa.[2] Being the capital city, Addis Ababa’s case reveals that the scarcity of access to diagnostic tests is not limited to remote areas but also affects major cities. The problem affected priority healthcare areas such as FANC, and the problem was even severe in the non-priority healthcare sector.
Exploring further studies on the availability of essential diagnostic tests, we find more alarming signs of this deep-rooted problem. A study done in 2019 in Jimma Zone, Ethiopia, revealed that out of the total health facilities with laboratories visited, only 23.3% had clinical chemistry service, of which 77.2% of the results were reported outside of the allowable error limit.[3] The study also found that all of the facilities that had clinical chemistry tests are located in the city. This underscores the gravity of the problem, further highlighting the inequitable distribution of access to diagnostic tests to underserved communities and remote locations. It also supports the argument that diagnostic tests in non-focused areas of health policy are rarely available in health facilities.
Furthermore, another study conducted in 2021 in ten developing countries, such as Bangladesh, Haiti, Malawi, Namibia, Nepal, Kenya, Rwanda, Senegal, Tanzania, and Uganda, showed that only 19.2% have access to essential diagnostic tests in primary care, whereas only 68.4% are available in hospitals.[4] This example further solidifies the severity and widespread prevalence of the problem in resource-constrained settings.
In addition, the consequence of the inaccessibility of diagnostic tests has dire consequences on the health outcomes of the patients. It can delay diagnosis and treatment, increase misdiagnosis, and prolong the turnaround time for test results and the time patients spend inside the health facilities. This further exacerbates patients’ dissatisfaction and distrust in the healthcare system, leading to a reduction in healthcare utilization.
A 2017 study at Tikur Anbessa Specialized Hospital in Ethiopia found that only 59.7% of patients were satisfied with clinical laboratory services.[5] This highlights the level of dissatisfaction of patients with laboratory services even in big facilities. Large facilities tend to face high dissatisfaction levels due to a high flow of patients and comprehensiveness of the services provided, making management and resource allocation difficult. Unless these dissatisfactions are addressed adequately and on time, they could grow into distrust in the healthcare system, which sets a vicious cycle.
The impact of the unavailability of diagnostic tests has dire consequences on the health outcomes of patients in Africa. A study conducted in Tanzania in 2011 showed that out of 494 patients clinically diagnosed and admitted to the hospital,l only 57.7% had a smear positive.[6] This underscores the importance of confirmatory testing to tackle misdiagnosis and enhance health outcomes. Numerous studies have conclusively agreed that clinical diagnosis without diagnostic test confirmation is more likely to be misdiagnosed and overdiagnosed.
However, some early initiatives showed promising results in addressing this issue. A 2007 review conducted by the Centers for Disease Control and Prevention (CDC), the Ethiopian Public Health Institute, and other partners on the effectiveness of private-public partnerships to improve the quality of laboratory services showed encouraging results.[7] The review found the reduction of average turnaround time from 7 days to 2 days in Addis Ababa and from 10 days to 5 days in the Amhara region. This was the first initiative to establish a public-private partnership addressing issues related to the quality of laboratory services and specimen referral using the Ethiopian Postal Services.[8]
A 2023 WHO regional strategy on diagnostics and laboratory services and system for the African region reports that 47% of global population has little to no access to diagnostics, and only 30% of health facilities in Africa have the necessary equipment and reagents to perform basic diagnostic tests due to lack of national prioritization, underfunding and inadequate resources.[9] This report summarizes the diagnostic challenges in global health, particularly affecting Africa significantly. Similarly, an overview of randomized clinical trials revealed an attempt to assess the impact of diagnostic tools, clinical algorithms, and training and communication packages on antibiotic prescription and clinical outcomes for acute febrile illness in three sub-Saharan African countries.[10] It is the rest attempt that objectively assesses the impact of diagnostic tests on serious issues such as clinical outcome and antimicrobial resistance.
Nevertheless, studies conducted so far have focused on the availability of diagnostic tests in the facilities. Most of these studies relied on the presence and quantity of diagnostic tools within healthcare facilities. However, the availability of diagnostic tests didn’t necessarily guarantee patient’s access to diagnostic tests. Patient’s experience and effort to access diagnostic tests have not been adequately examined. There is a lack of studies that have investigated the problem from the patient’s perspective. The main objective of this study was to assess the accessibility of diagnostic tests to patients and associated factors, with emphasis on the interaction between patients and laboratory services. Additionally, challenges associated with diagnostic care and laboratory services are also examined.
Methodology
Study setting: This study was conducted in Hawassa city, Ethiopia. Hawassa City is the capital of the Sidama region.
Study design and period: A facility-based cross-sectional study was conducted from April 15 to May 15, 2023 (GC).
Study population: The study population consisted of patients from HCSURH, Adare General Hospital, and Motite Fura Primary Hospital. Patients were included in the study while they were accessing healthcare services at the facility.
Sample size determination: For sample size determination, a single population formula was used. A 2023 study found that the availability of diagnostic tests was 86.6%.[11] This finding was used to determine the sample size. As a result, the sample was calculated as follows:
Where:
Z = 1.96 (for 95% confidence level), p = 0.866 (population proportion), and E = 0.05 A 10% non-responder rate was added to account for any non-responders. Therefore, the final sample size became 196.
Sampling method: A stratified random sampling technique was used to collect data from three public hospitals, each representing a different health facility tier. These included one tertiary referral hospital, one secondary general hospital, and one primary hospital in Hawassa.
Data collection: Participants´ data were collected through interviews. Interview questionnaires were prepared prior to the interview. Upon consent, the interview was recorded and later transcribed. The collected data were checked for errors, entered into a digital tool, and cleaned.
Method of data analysis: The collected data were entered into SPSS and rechecked for errors. The analysis was done using SPSS and Python. Descriptive analysis was done using frequency and percentage. The findings were presented using tables and charts.
Inclusion and exclusion criteria
Inclusion criteria: Patients in HCSURH, AGH, and MFPH who were accessing healthcare services were included in the study. Patients above the age of 15 who were conscious and who gave consent were included in the study.
Exclusion criteria: Patients under the age of 15 were not included in this study. In addition, unconscious and non-consenting patients were also not included in this study.
Dependent variable: Outsourcing of diagnostic tests.
Independent variables: Age group, sex, marital status, facility, chronic diseases comorbidity, turnaround time, and digital health use.
Limitation of the study: In the study, lists of confounding variables such as income level and literacy were not examined exhaustively. This might skew some of the findings in the study. In addition, the study relied on patients’ reports without official document confirmation. As a result, it is exposed to recall bias.
Results
Socio-demographic information: We interviewed 196 patients from three public hospitals in Hawassa, Ethiopia. The largest proportion of the respondents (36.74%) was within the age group of 26-35. Furthermore, the average age was 36.01, and the median age was 33. Males accounted for 57.66% and females accounted for 42.34% of the respondents. 77.04% were married, and 71.42% of respondents lived in the city. 18.87% of respondents had a chronic disease. Although smartphone access was 50% and internet access was 56.15%, only 19.89% of respondents used digital health services.
|
No. |
Lists |
Outsources diagnostic tests | |||
| Yes | No | ||||
| Frequency | Percentage | Frequency | Percentage | ||
| 1. | Age groups (in years) | ||||
| 14 – 25 | 17 | 8.67% | 33 | 16.84% | |
| 25 – 35 | 40 | 20.41% | 32 | 16.33% | |
| 35 – 45 | 17 | 8.67% | 17 | 8.67% | |
| 45 – 55 | 14 | 7.14% | 7 | 3.57% | |
| > 55 | 14 | 7.14% | 5 | 2.55% | |
| 2. | Sex | ||||
| Female | 45 | 22.96% | 38 | 19.39% | |
| Male | 57 | 29.09% | 56 | 28.57% | |
| 3. | Marital status | ||||
| Married | 87 | 44.39% | 64 | 32.65% | |
| Single | 15 | 7.65% | 30 | 15.30% | |
| 4. | Occupation | ||||
| Farmer | 3 | 1.54% | 7 | 3.59% | |
| Housewife | 5 | 2.56% | 5 | 1.54% | |
| Labourer | 0 | 0% | 3 | 2.56% | |
| Military | 37 | 18.97% | 25 | 12.82% | |
| Private worker | 26 | 13.33% | 23 | 11.79% | |
| Public worker | 5 | 2.56% | 2 | 1.03% | |
| Retired | 11 | 5.64% | 14 | 7.20% | |
| Student | 10 | 5.13% | 11 | 5.64% | |
| Unemployed | 4 | 2.05% | 4 | 2.05% | |
| 5. | Location | ||||
| City | 69 | 35.20% | 71 | 36.22% | |
| Rural | 18 | 9.18% | 16 | 8.16% | |
| Town | 15 | 7.65% | 7 | 3.57% | |
| 6. | Chronic disease Comorbidity | ||||
| Yes | 26 | 13.26% | 11 | 5.61% | |
| No | 76 | 38.77% | 83 | 42.36% | |
| 7. | Digital health solution use | ||||
| Yes | 27 | 13.77% | 12 | 6.12% | |
| No | 75 | 38.26% | 82 | 41.84% | |
| 8. | Smartphone use | ||||
| Yes | 55 | 28.06% | 43 | 21.94% | |
| No | 47 | 23.98% | 51 | 26.02% | |
| 9. | Internet access | ||||
| Yes | 51 | 27.27% | 54 | 28.88% | |
| No | 46 | 24.60% | 36 | 19.35% | |
Table 1: Socio-demographic distribution of patients in health facilities in Hawassa, 2023
Prevalence of facing diagnostic test outsourcing: 52% of patients encountered outsourcing of diagnostic tests to another facility due to the unavailability of the tests within the facility. The unavailability of diagnostic tests has various root causes, including stockouts of reagents, malfunctioning machines, and a lack of skilled personnel. Among these, 89.1% of them encountered this problem two or more times, while 10.9% reported experiencing outsourcing only once.
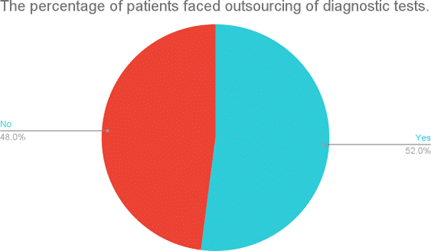
Figure 1: The percentage of patients outsourced for diagnostic tests to other facilities
In addition, the average turnaround time for diagnostic tests was seven hours. When comparing patients who experienced outsourcing with those who did not, patients who experienced outsourcing for diagnostic tests tended to have turnaround times between eight and twelve hours.
Digital health users were more likely to experience outsourcing, even though they made up only 19.89% of the respondents. Most of them used digital tools to get information and chat with or contact health professionals. 44.74% of them used web search to find information, 28.95% used calls and texts to contact health professionals, 15.79% used social media to obtain information, and the remaining 10.53% used various mobile apps for different health-related purposes.
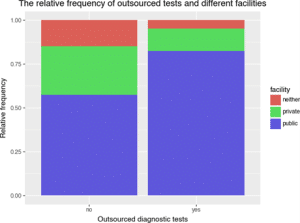
Figure 2: The relative frequency of experiencing outsourcing of diagnostic tests in different health facilities
Outsourcing of diagnostic tests was commonly encountered in public health facilities. 42.85% of patients reported experiencing outsourcing in public health facilities, whereas only 6.63% of patients experienced it in private facilities. Furthermore, patients reported multiple challenges in laboratory services. While 53.8% of the patients reported having no problems, 12.6% cited delayed test results, 11.5% reported receiving incorrect test results, and 8.8% mentioned unprofessional conduct among other issues.
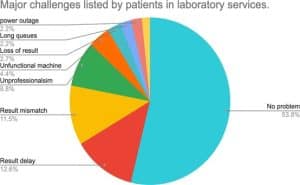
Figure 3: Additional challenges reported by patients in the laboratory services
Almost all of the patients reported solving outsourced diagnostic tests by searching for a facility where the tests are available and getting tested there.
Factors associated with encountering diagnostic test outsourcing: Age group, marital status, facility, chronic disease, turnaround time, and digital health tool use were significant when conducting crude odds ratios. However, in the adjusted odds ratio analysis, only marital status, facility, turnaround time, and digital health tool use remained significant.
Married patients: p = 0.025 (AOR: 2.996, 95% CI 1.147, 7.82) are more likely to encounter outsourcing of diagnostic tests than singles. Patients in public health facilities: p = 0.003 (AOR: 6.153, 95% CI 1.847, 20.499) are more likely to face outsourcing of diagnostic tests. Patients who reported the turnaround time of test results is between four and eight hours: p = 0.023, (AOR: 2.931, 95% CI 1.163, 7.389) are more likely to have encountered outsourcing of diagnostic tests compared to other turnaround times. In addition, patients who use digital health tools: p = 0.003, (AOR: 4.001, 95% CI 1.614, 9.915) are more likely to face outsourcing of diagnostic tests than non-users.
| No. | Lists | Outsourced diagnostic tests | |||||||
| Frequency | Odds ratio | Confidence interval | |||||||
| Yes | No | COR P-value | COR | AOR P-value | AOR | Lower | Upper | ||
| 1. | Age groups (In years) | ||||||||
| 14 – 25 | 17 | 33 | 1 | 1 | 1 | 1 | |||
| 25 – 35 | 40 | 32 | 0.02 | 2.426 | 0.278 | 1.674 | |||
| 35 – 45 | 17 | 17 | 0.145 | 1.941 | 0.635 | 0.748 | |||
| 45 – 55 | 14 | 7 | 0.014 | 3.882 | 0.272 | 2.72 | |||
| > 55 | 14 | 5 | 0.005 | 5.435 | 0.417 | 1.176 | |||
| 2. | Sex | ||||||||
| Female | 45 | 38 | 0.601 | 1.163 | |||||
| Male | 57 | 56 | 1 | 1 | |||||
| 3. | Marital status | ||||||||
| Married | 87 | 64 | 0.003 | 2.854 | 0.025 | 2.996 | 1.147 | 7.82 | |
| Single | 15 | 30 | 1 | 1 | 1 | 1 | |||
| 4. | Occupation | ||||||||
| Farmer | 3 | 7 | 0.357 | 0.471 | |||||
| Housewife | 5 | 5 | 0.476 | 1.833 | |||||
| Labourer | 0 | 3 | 0.909 | 1.1 | |||||
| Military | 37 | 25 | 0.999 | 0 | |||||
| Private worker | 26 | 23 | 0.337 | 1.628 | |||||
| Public worker | 5 | 2 | 0.624 | 1.291 | |||||
| Retired | 11 | 14 | 0.284 | 2.75 | |||||
| Student | 10 | 11 | 0.806 | 0.864 | |||||
| Unemployed | 4 | 4 | 1 | 1 | |||||
| 5. | Location | ||||||||
| City | 69 | 71 | 0.105 | 0.454 | |||||
| Rural | 18 | 16 | 0.26 | 0.525 | |||||
| Town | 15 | 7 | 1 | 1 | |||||
| 6. | Facility | ||||||||
| Public Facilities |
84 |
54 |
0.007 |
4.407 |
0.003 |
6.153 |
1.847 |
20.499 |
|
| Private Facilities | 13 | 26 | 0.683 | 1.292 | 0.748 | 1.256 | |||
| Neither | 5 | 14 | 1 | 1 | 1 | 1 | |||
| 7. | Chronic disease Comorbidity | ||||||||
| Yes | 26 | 11 | 0.016 | 2.581 | 0.061 | 2.523 | |||
| No | 76 | 83 | 1 | 1 | 1 | 1 | |||
| 8. | Turnaround Time | ||||||||
| In less than 2 hours | 38 | 47 | 1 | 1 | 1 | 1 | |||
| in Between 2 and 4 hours | 23 | 15 | 0.082 | 0.916 | 0.071 | 2.313 | |||
| in Between 4 and 8 hours | 25 | 15 | 0.049 | 1.004 | 0.023 | 2.931 | 1.163 | 7.389 | |
| in Between 8 and 12 hours | 4 | 1 | 0.147 | 0.559 | 0.391 | 2.72 | |||
| Beyond 24 hours | 14 | 16 | 0.756 | 0.494 | 0.745 | 1.176 | |||
| 9. | Digital health solution use | ||||||||
| Yes | 27 | 12 | 0.018 | 2.46 | 0.003 | 4.001 | 1.614 | 9.915 | |
| No | 75 | 82 | 1 | 1 | 1 | 1 | |||
| No | 46 | 36 | 1 | 1 | |||||
Table 2: Factors associated with test outsourcing in health facilities in Hawassa, 2023
Discussion
Healthcare in resource-constrained settings faces multiple challenges, stemming from various causes. Diagnostic tests, particularly, face severe challenges in health facilities in low-resource environments. This posed a barrier for patients in accessing appropriate, timely, and affordable healthcare services. A study conducted in 2021 in ten developing countries revealed 19% availability of diagnostic tests in primary care.[4] This is a stark reality for millions of patients who struggle to access diagnostic tests in Sub-Saharan Africa. It is extremely important to explore patients’ experiences to understand their struggle in accessing diagnostic tests and develop interventions tailored to their needs and challenges.
We found that 50% of respondents have smartphones, while 56.13% have access to the internet. The government of Ethiopia reported 42% smartphone penetration and 19.4% internet access through a recent press release. Our study population seems to surpass in both categories, with a significant edge in internet access. This might be due to 71.42% of our respondents living in the city, and the majority being young. Nevertheless, only 19.89% of the respondents use digital tools for healthcare purposes.
An overwhelming majority of digital health users reported that they use digital tools to look for information or contact health providers. This shows that there is a huge potential for digital tools to be deployed to provide service to customers. However, the enabling factors and the opportunities are not being properly used for healthcare service delivery due to the government’s focus on digitalizing health facilities, and the weakness of the private sector. There is a large gap in leveraging technology and digital tools for healthcare service provision, and consequently, sustaining a low culture of using digital tools for healthcare.
It is a common experience for patients to encounter the unavailability of essential diagnostic tests in health facilities. Usually, this happens when patients are trying to access diagnostic tests ordered by the physicians. Critical diagnostic tests have to be done in the other facility where the test is available, and the result will be returned to the facility where the test was initially ordered, unless the patient reinitiates the entire process in the other facility. 52% of our respondents reported experiencing the outsourcing of diagnostic tests to other facilities. The majority explained that either the tests were unavailable, or the machine was not working, or there were long queues. This highlights the main challenge for accessing diagnostic tests in the health facilities, which is due to a shortage of resources related to reagents, equipment, and trained personnel. Similarly, a study conducted in Uganda in 2017 showed 24.4% availability of spirometry and 6.7% availability of peak flow meters for asthma and COPD diagnosis.[12] It is apparent that resource shortages play a paramount role in the inaccessibility of diagnostic tests to patients in Sub-Saharan Africa. Furthermore, among those who faced the outsourcing of diagnostic tests, 89.1% reported they encountered the problem multiple times. This underscores the magnitude and severity of the problem, posing a significant challenge in accessing appropriate and timely healthcare services.
The World Health Organization (WHO) releases an essential diagnostic list (EDL) informing national and international organizations about critical diagnostic tests. A 2020 EDL report consists of multiple suggestions and recommendations.[13] It structured the recommendations in four categories: General In Vitro Diagnostics (IVDs) for community settings and health facilities without laboratories,
Disease-Specific IVDs for community settings and health facilities without laboratories, General IVDs for clinical laboratories, and Disease-Specific IVDs for clinical laboratories. However, inadequate effort has been made to integrate this guideline into comprehensive national policies, guidelines, and strategies, hindering the implementation and monitoring of the recommendations. A 2023 study found that out of 48 African countries, only one had a National Essential Drug List, while twenty-five others had national test menus.[14] Without integrated and responsive national guidelines, translating recommendations into reality in the health facilities will remain a far-fetched dream. On the other hand, widespread unavailability and inaccessibility of diagnostic tests pose an imminent threat to healthcare service delivery and patients’ health outcomes.
Even when diagnostic tests are available, accessing them is still mired in various challenges. In our study, we found that the average turnaround time of test results is around 7 hours. In addition, outsourced tests tend to have a turnaround time of more than two hours, as shown in Figure 3. A study done in Kenya in 2019 revealed that the average turnaround time for common diagnostic tests was 21.5 hours.[15] This is three times the average turnaround time of our study. However, unlike this study, which used a time-motion study, we relied on respondents’ reports, which are prone to recall bias.
Furthermore, while the Kenyan study measured the time starting from the order, our respondents reported starting from the time they gave the sample. However, prolonged turnaround time delays timely diagnosis and treatment, potentially worsening health outcomes and exacerbating patient dissatisfaction.
In addition, 13.77% of patients who use digital health tools reported facing outsourcing of diagnostic tests, compared to only 6.12% who reported not facing outsourcing. Most digital health users use digital tools to search for information or contact healthcare professionals, which highlights the limited application of digital tools in healthcare service delivery. Commonly listed digital tools used for health-related purposes include web search, call and text, social media, and mobile apps, as shown in Figure 6 (annex). This leads to an assumption that digital health users are more informed than non-users and therefore have strong opinions and awareness about services and diagnostic test accessibility. Consequently, they are more likely to report encountering outsourcing of diagnostic tests than not. Therefore, we can assume that the availability and accessibility of information to digital health users contribute significantly to this finding. Nevertheless, digital technologies present enormous opportunities and capabilities to leverage in addressing health care challenges in resource-constrained settings, including diagnostic test inaccessibility. A study done in 2019 showed that mobile health and electronic health interventions significantly support diagnosis in Sub-Saharan Africa.[16] This includes an ECG mobile application detecting fibrillation in Kenya, and an interactive app monitoring complete abortion in South Africa. This solidifies the potential of digital health interventions to address diagnostic test inaccessibility and other healthcare challenges in Africa.
Underfunded and overcrowded public health facilities are exposed to multifaceted challenges. Affordability of services in public health facilities makes them the primary choice for economically marginalized and underserved communities. However, this comes with a huge cost. 42.8% of our respondents reported that they encountered outsourcing of diagnostic tests in public health facilities, while only 6.63% reported the same in private facilities. In addition, challenges such as delays in results, result mismatches, and unprofessionalism are rampant in public health facilities. Moreover, almost all patients in public and private health facilities outsource diagnostic tests by searching for facilities where the test is available in person.
Inaccessibility of diagnostic tests occurs against a backdrop of multiple factors. Our exploration revealed interesting factors that contribute to the outsourcing of diagnostic tests. Married individuals are 2.9 times more likely to face the outsourcing of diagnostic tests than single individuals. This might be due to married individuals seeking healthcare services more frequently for themselves and their families. Patients encounter the outsourcing of diagnostic tests an average of 6.15 times in public facilities. Public facilities also have multiple and severe problems associated with their laboratory services. Patients who receive their test results between four and eight hours are 2.9 times more likely to face outsourcing. This reveals an even more interesting fact: outsourced tests have a longer turnaround time than in-house tests. However, the most extreme turnaround times, which are beyond 24 hours, are more likely to occur inside the facilities. Since the study was conducted in public health facilities, this might suggest that private facilities have relatively shorter turnaround times than public health facilities. Digital health users are 4.0 times more likely to face outsourcing. This might be due to strong opinions and high awareness and expectation levels of digital health users with access to up-to-date information. A study done in 2022 showed that access to diagnostic tests through eHealth has a high acceptability rate and follow-up testing or treatment after a positive result for STIs.[17] This study reveals that digital health users are more aware of the issues and open to further engagement. Fast and easy access to information with digital tools plays a large role in this.
Conclusion
Accessing diagnostic tests remains a major hurdle for patients in resource-constrained settings. We found that 52% of patients experience outsourcing of diagnostic tests, and many are required to visit multiple facilities to access tests. In addition, we identified that marital status, health facilities category, turnaround time, and digital health use are factors associated with experiencing outsourcing. Access to diagnostic tests has serious implications for health outcomes, and this study focused on assessing access to diagnostic tests from a patient’s perspective. However, we solely relied on patients’ reports, and future studies should integrate patients’ reports with facility data to provide a more comprehensive understanding. This study can facilitate dialogue for policy revision in low-resource healthcare settings and shed light on the untapped potential of digital technologies to address these challenges.
References
- Genet Akal C, Andualem T. A Cross-Sectional Study to Assess Capacity of Health Facility Laboratories in Zone One of Afar Regional State, Ethiopia. J Trop Med. 2018;2018:9274127. doi:10.1155/2018/9274127
PubMed | Crossref | Google Scholar - Desalegn DM, Abay S, Taye B. The availability and functional status of focused antenatal care laboratory services at public health facilities in Addis Ababa, Ethiopia. BMC Res Notes. 2016;9(1):403. doi:10.1186/s13104-016-2207-z
PubMed | Crossref | Google Scholar - Getachew A, Cheneke W, Asres Y, Bekele S, Kebede E. Assessment of Coverage and Quality of Selected Clinical Chemistry Tests among Medical Laboratories of Health Facilities in Jimma Zone, South West Ethiopia. J Trop Med. 2019;2019:5954313. doi:10.1155/2019/5954313 PubMed | Crossref | Google Scholar
- Yadav H, Shah D, Sayed S, Horton S, Schroeder LF. Availability of essential diagnostics in ten low-income and middle-income countries: results from national health facility surveys. Lancet Glob Health. 2021;9(11):e1553-e1560. doi:10.1016/S2214-109X(21)00442-3 PubMed | Crossref | Google Scholar
- Abera RG, Abota BA, Legese MH, Negesso AE. Patient satisfaction with clinical laboratory services at Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia. Patient Prefer Adherence. 2017;11:1181-1188. doi:10.2147/PPA.S132397 PubMed | Crossref | Google Scholar
- Msangeni HA, Kamugisha ML, Sembuche SH, et al. Prospective study on severe malaria among in-patients at Bombo regional hospital, Tanga, north-eastern Tanzania. BMC Infect Dis. 2011;11:256. doi:10.1186/1471-2334-11-256
PubMed | Crossref | Google Scholar - Kebede Y, Fonjungo PN, Tibesso G, et al. Improved Specimen-Referral System and Increased Access to Quality Laboratory Services in Ethiopia: The Role of the Public-Private Partnership. J Infect Dis. 2016;213 Suppl 2(Suppl 2):S59-64. doi:10.1093/infdis/jiv576 PubMed | Crossref | Google Scholar
- Petti CA, Polage CR, Quinn TC, Ronald AR, Sande MA. Laboratory medicine in Africa: a barrier to effective health care. Clin Infect Dis. 2006;42(3):377-382. doi:10.1086/499363 PubMed | Crossref | Google Scholar
- Olliaro P, Nkeramahame J, Salami O, et al. Advancing Access to Diagnostic Tools Essential for Universal Health Coverage and Antimicrobial Resistance Prevention: An Overview of Trials in Sub-Saharan Africa. Clin Infect Dis. 2023;77(Suppl 2):S125-S133. doi:10.1093/cid/ciad326 PubMed | Crossref | Google Scholar
- Regional Committee for Africa. Regional Strategy on Diagnostic and Laboratory Services and Systems, 2023–2032 for the WHO African Region: Report of the Secretariat. 2023. Regional strategy on diagnostic and laboratory services and systems, 2023–2032 for the WHO African Region: report of the Secretariat
- Umer A, Mohammed H, Yazie B, et al. Assessment of Availability of Tracer Drugs and Basic Diagnostics at Public Primary Health Care Facilities in Ethiopia During COVID-19 Pandemic. Ethiop J Health Sci. 2023;33(Spec Iss 2):135-142. doi:10.4314/ejhs.v33i2.7S PubMed | Crossref | Google Scholar
- Kibirige D, Kampiire L, Atuhe D, et al. Access to affordable medicines and diagnostic tests for asthma and COPD in sub Saharan Africa: the Ugandan perspective. BMC Pulm Med. 2017;17(1):179. doi:10.1186/s12890-017-0527-y
PubMed | Crossref | Google Scholar - World Health Organization. The selection and use of essential in vitro diagnostics: report of the third meeting of the WHO Strategic Advisory Group of Experts on In Vitro Diagnostics, 2020 (including the third WHO model list of essential in vitro diagnostics). 2021. The selection and use of essential in vitro diagnostics: report of the third meeting of the WHO Strategic Advisory Group of Experts on In Vitro Diagnostics, 2020 (including the third WHO model list of essential in vitro diagnostics)
- Koster W, Mutegi EM, Ocen F, et al. Contexts for developing of national essential diagnostics lists. Lessons from a mixed-methods study of existing documents, stakeholders and decision making on tier-specific essential in-vitro diagnostics in African countries. PLOS Glob Public Health. 2023;3(5):e0001893. doi:10.1371/journal.pgph.0001893 PubMed | Crossref | Google Scholar
- Mwogi T, Mercer T, Tran DNT, Tonui R, Tylleskar T, Were MC. Therapeutic turnaround times for common laboratory tests in a tertiary hospital in Kenya. PLoS One. 2020;15(4):e0230858. doi:10.1371/journal.pone.0230858
PubMed | Crossref | Google Scholar - Bervell B, Al-Samarraie H. A comparative review of mobile health and electronic health utilization in sub-Saharan African countries. Soc Sci Med. 2019;232:1-16. doi:10.1016/j.socscimed.2019.04.024 PubMed | Crossref | Google Scholar
- Versluis A, Schnoor K, Chavannes NH, Talboom-Kamp EP (2022) Direct Access for Patients to Diagnostic Testing and Results Using eHealth: Systematic Review on eHealth and Diagnostics. J Med Internet Res. 2022;24(1):e29303 doi: 10.2196/29303 PubMed | Crossref | Google Scholar
Acknowledgments
Not reported
Funding
Not reported
Author Information
Asnake Amelo
Department of Digital Business and Innovation
IE Business School, Madrid, Spain
Email: asnakeargeta42@gmail.com
Author Contribution
Asnake Argeta Amelo drafted and wrote the manuscript.
Ethical Approval
The health research ethics were maintained. Patients were informed about the details of the study, and informed consent was taken prior to enrolling them in the study. Participants were involved only after giving their consent, and no coercion, manipulation, or any unethical measures were taken to force participants. All responses were coded to maintain the confidentiality and privacy of the respondents for the information given.
Conflict of Interest Statement
The author declares no conflict of interest.
Guarantor
None
DOI
Cite this Article
Asnake A. The Assessment of the Accessibility of Diagnostic Tests and Associated Factors in Public Health Facilities in Hawassa, Ethiopia. medtigo J Med. 2025;3(1):e3062314. doi: 10.63096/medtigo3062314 Crossref













