







 Author Affiliations
Author Affiliations
Abstract
Introduction: Intrahepatic cholangiocarcinoma (IHCC), the second leading cause of liver-related mortality, carries a poor prognosis. Although its incidence has risen over the past two decades, mortality trends remain underexplored. This study aims to analyze national and regional variations in IHCC-associated mortality among U.S. adults.
Methodology: Death certificate data from the Centers for Disease Control and Prevention (CDC) Wide-ranging Online Data for Epidemiologic Research (WONDER) database were analyzed for IHCC-related deaths in adults over 25 years from 1999 to 2020. Age-adjusted mortality rates (AAMR) per 100,000 and annual percentage change (APC) were calculated using Joinpoint regression, stratified by age, year, gender, race, region, urbanization, and place of death.
Results: Between 1999 and 2020, 113,350 adults over age 25 died from IHCC. AAMR rose from 1.5 in 1999 to 3.1 in 2020 (APC = 3.55). Men experienced slightly higher mortality than women, with AAMRs in 2020 of 3.6 and 2.8, respectively. Non-Hispanic (NH) Asian and Pacific Islanders had the highest AAMR (3.2), followed by NH American Indians and Alaska Natives (2.7), Hispanics (2.7), NH Whites (2.3), and NH Blacks (2.3). Regional differences were notable, with the Northeast highest at 2.6, followed by the Midwest and West (2.5 each), and the South (2.1). Metropolitan areas had a higher AAMR (2.4) compared to non-metropolitan areas (2.1).
Conclusion: IHCC-related mortality in U.S. adults over 25 increased from 1999 to 2020, highest among those over 85, men, NH Asian and Pacific Islanders, in the Northeast, and metropolitan areas. These trends highlight the urgent need for early detection and targeted therapies to reduce the growing burden.
Keywords
Intrahepatic cholangiocarcinoma, Liver cancer mortality, Age-adjusted mortality rate, Annual percentage change, Joinpoint regression.
Introduction
Cholangiocarcinoma, a rare form of biliary tract cancer originating from the epithelial lining of the biliary tract, accounts for 3% of gastrointestinal cancers and is the second-most prevalent type of liver cancer.[1,2] Although it can originate anywhere along the biliary tree, the incidence is highest at the point of hepatic duct bifurcation.[3] Moreover, anatomically, cholangiocarcinoma is subdivided into IHCC, originating from the intrahepatic biliary ducts, and extrahepatic cholangiocarcinoma (ECC), originating from the biliary tract outside the liver.[4-6] Each subtype presents with varying symptoms, predominantly based on the location of origination, site of spread, and stage of the cancer.[3]
Over the last three decades, the incidence of IHCC has increased in the United States. This increase can be linked to associated risk factors, such as infections like hepatitis B, hepatitis C, and Fasciola hepatica (liver fluke); gastrointestinal diseases like primary biliary sclerosis, biliary stones or cysts, and inflammatory bowel disease; lifestyle factors like alcohol and tobacco use, diabetes, and obesity; and genetics.[1,7,8] Even with a low incidence, the delayed presentation and diagnosis make IHCC a fatal condition, with a five-year survival rate of 25%.[2,8,9]
Past epidemiological researchers have found a significant increase in IHCC incidence.[10-12] These studies were also able to highlight the gender and racial disparities in the incidence of IHCC, with males, African Americans, and Asians showing the highest prevalence.[13] However, its effect on mortality is yet to be explored. Moreover, identifying these disparities can help understand the factors leading to an upward trend in mortality rate and can pave the way for timely interventions to tackle the growth. Herein, we sought to explore the mortality associated with IHCC from 1999 to 2020 in adults over 25 based on demographics.
Methodology
Study setting and population: In our descriptive study, mortality data related to IHCC were extracted from the US CDC WONDER database. We conducted disease-specific analyses using the International Statistical Classification of Diseases and Related Health Problems-10th Revision (ICD-10) code C22.1, which is standard for identifying malignant neoplasm of the intrahepatic bile duct. This ICD-10 code was similarly used by Javle et al. for their 2022 analysis.[11] The CDC WONDER database is regularly updated with cause-of-death information from death certificates across all 50 states and the District of Columbia. In our study, Intrahepatic cholangiocarcinoma was considered the cause of death for all individuals whose death certificate listed it as a direct underlying cause of death. Using this ICD-10 code, we retrieved mortality data in adults aged 25 years and above, spanning from 1999 to 2020. Given the deidentified nature of the publicly available dataset, our study is exempt from Institutional Review Board approval. However, we adhered to strengthening the reporting of observational studies in epidemiology (STROBE) guidelines.[14]
Data abstraction: We analyzed disparities in data based on year, age, gender, race/ethnicity, geographical region, place of death, and urban-rural classification. Race/ ethnicity categories include Hispanics or Latinos, Black or African Americans, Whites, Asians and Pacific Islanders, and Native American Indians. The location of death was categorized into medical facilities (inpatient, outpatient, emergency room, death on arrival, or unknown status), home, hospice, and nursing home/long-term care facilities. Additionally, the CDC WONDER database enabled the classification of mortality by census regions (Northeast, Midwest, South, and West), census divisions (New England, Pacific, Mountains, West North Central, West South Central, East South Central, East North Central, South Atlantic, and Mid Atlantic), and states.[15] The 2013 urbanization classification scheme employed by the National Center for Health Statistics divided geographical areas into urban (large metropolitan areas with a population equal to or greater than 1 million), medium/small metropolitan (areas with a population between 50,000 and 999,999), and rural (population less than 50,000).[16] This classification relies on the data reported on death certificates, as has been used in prior analyses on the WONDER database.[14]
Statistical analysis: The CDC database provided intrahepatic cholangiocarcinoma (IHCC)-related mortality as AAMR and crude mortality rates. The AAMR was obtained per 100,000 individuals, while the crude rate was calculated by dividing the number of IHCC-related deaths by the corresponding US population for each respective year.[17] The APC in AAMR and a 95% Confidence Interval of change were determined using the Joinpoint Regression Program (Joinpoint V 4.9.0.0, National Cancer Institute).[18] This model identifies annual variation in the AAMR by fitting long-linear regression models to periods where changes occurred. An APC was deemed increasing or decreasing if the slope indicating the change in mortality was significantly different from zero, as determined by two-tailed t-tests. Statistical significance was defined as P<0.05.
Results
Annual trends for IHCC mortality: Between 1999 and 2020, a total of 113,350 adults aged 25 and older died from IHCC in the United States. During this time, the AAMR increased steadily from 1.4 per 100,000 in 1999 to 2.8 per 100,000 in 2020. The average yearly increase in deaths was 3.55% (95% confidence interval (CI), 3.34 to 3.72), showing a clear upward trend over the years (Figure 1).
IHCC-associated mortality stratified by age: Older adults had higher death rates, and every age group (except the youngest) showed a consistent increase over time. Among adults aged 85 and older, the crude mortality rate rose from 8.9 in 1999 to 14.3 in 2020 (APC 1.86%, 95% CI, 1.47 to 2.26). For those aged 75–84, it increased from 6.9 to 13.7 (APC 3.21%, 95% CI, 3.02 to 3.40), and for ages 65–74, from 4.0 to 8.7 (APC 3.94%, 95% CI, 3.72 to 4.16). Similarly, mortality rose from 1.8 to 4.3 in those aged 55–64 (APC 4.34%, 95% CI, 4.07 to 4.62), from 0.6 to 1.3 in the 45–54 group (APC 3.84%, 95% CI, 2.84 to 4.83), and from 0.2 to 0.4 in those aged 35–44 (APC 4.35%, 95% CI, 3.50 to 5.21). The youngest age group (25–34) showed no meaningful change, with a steady rate of 0.1 and an APC of 0.01% (95% CI, –0.92 to 0.96) (Supplemental tables 1 and 2).
| Category | N | Rate per 100,000 (95% CI) |
| Entire cohort | 113350 | 2.4 (2.3-2.4) |
| Sex Men Women |
57545 55805 |
2.4 (2.3-2.4) 2.1 (2.1-2.1) |
| Race Asian Black or African American White Native Americans Hispanics |
6057 10421 85599 740 10318 |
3.2 (3.1-3.3) 2.3 (2.2-2.3) 2.3 (2.3- 2.3) 2.7 (2.5-2.9) 2.7 (2.7-2.8) |
| US census region Northeast Midwest South West |
23875 26485 37214 25757 |
2.6 (2.5-2.6) 2.5 (2.4-2.5) 2.1 (2.1- 2.1) 2.5 (2.5-2.5) |
| Age group 25-34 35-44 45-54 55-64 65-74 75-84 85 + years |
634 2545 9359 23234 32512 30459 14607 |
0.1 (0.1-0.1) 0.3 (0.3-0.3) 1.0 (1.0-1.0) 3.0 (3.0-3.1) 6.4 (6.3-6.4) 10.2 (10.1-10.3) 12.2 (12.0-12.4) |
Supplemental table 1: Demographic Differences in IHCC-related mortality, 1999-2020
| Race | Northeast | Midwest | South | West |
| Asian | 2.3 (2.1-2.4) | 2.3 (2.1-2.5) | 1.8 (1.7-1.9) | 3.1 (3.0-3.2) |
| Black of African American | 2.3 (2.2-2.4) | 2.1 (2.1-2.2) | 1.9 (1.8-1.9) | 2.0 (1.9-2.2) |
| White | 3.2 (3.1-3.2) | 2.9 (2.8-2.9) | 2.5 (2.5-2.5) | 2.7 (2.6-2.7) |
| Native Americans | 1.1 (0.7-1.6) | 1.9 (1.6-2.3) | 1.5 (1.2-1.7) | 3.1 (2.8-3.4) |
| Hispanics | 1.8 (1.7-1.9) | 1.5 (1.4-1.6) | 1.6 (1.6-1.7) | 1.9 (1.8-1.9) |
Supplemental table 2: AAMR per 100,000 according to race by region, 1999-2020
IHCC-associated mortality stratified by place of death: Place of death data were available for almost all patients. The most common place of death was the decedent’s home (44.2%, n = 50,156), followed by hospitals (30.6%, n = 34,692), hospice facilities (9.9%, n = 11,255), and nursing homes or long-term care centers (9.9%, n = 11,252). A smaller number died in other locations (5.1%, n = 5,757), and the place of death was unknown for only 0.2% (n = 238).
IHCC-associated mortality stratified by gender: Men consistently had higher IHCC-related death rates than women. Among men, the AAMR increased from 1.7 in 1999 to 3.6 in 2020, with an average AAMR of 2.7 and an APC of 3.70% (95% CI, 2.95 to 4.46). For women, the AAMR rose from 1.4 to 2.8 over the same period, with an average AAMR of 2.1 and an APC of 3.55% (95% CI, 3.34 to 3.77) (Figure 1).
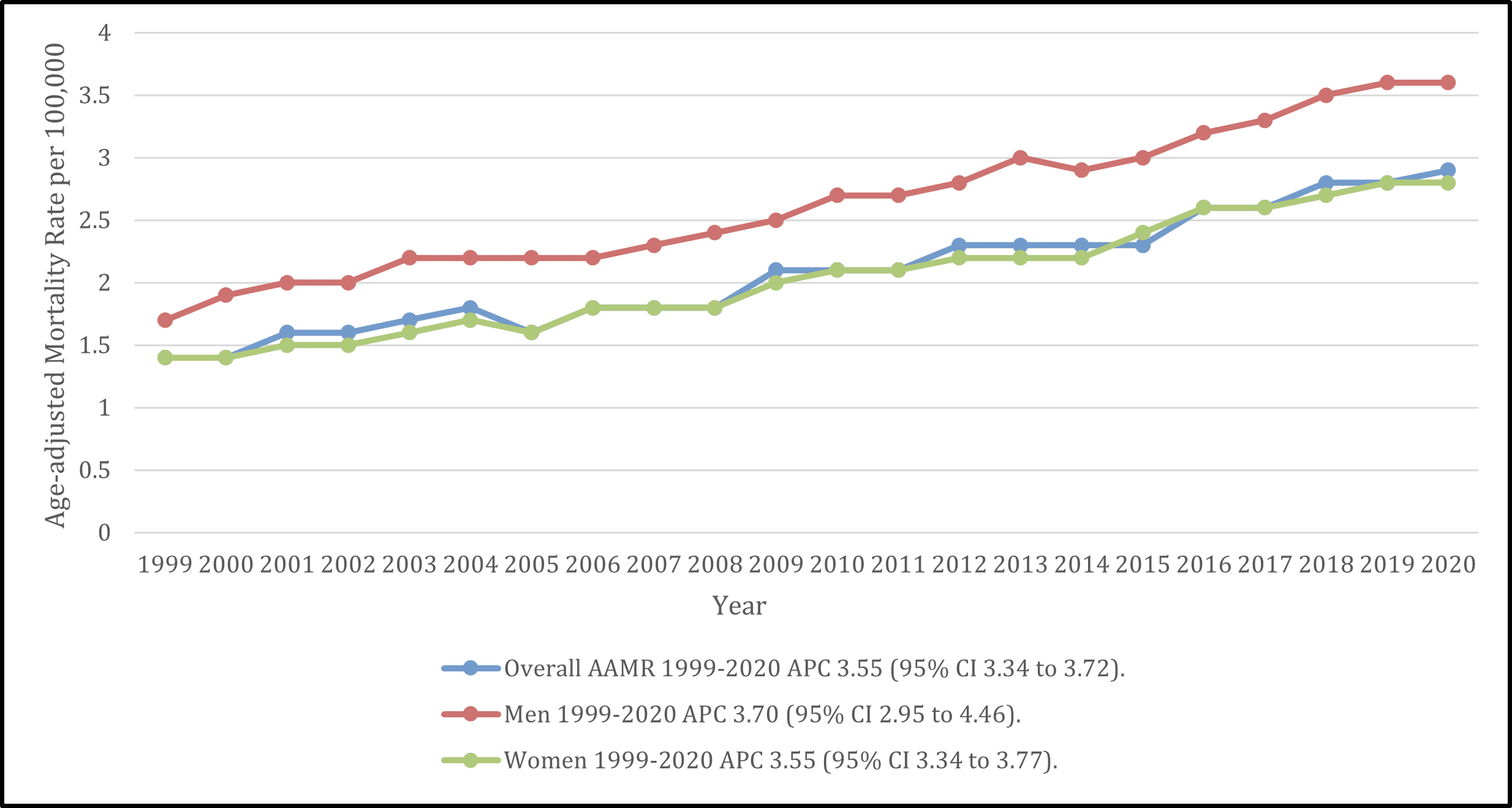
Figure 1: Year and gender stratified AAMR per 100,000 adults in the United States from 1999 to 2020
IHCC-associated mortality stratified by race/ethnicity: Although IHCC-related mortality increased across all racial and ethnic groups from 1999 to 2020, the highest trends were observed among NH Asian and Pacific Islanders. In this group, the AAMR rose from 2.2 per 100,000 in 1999 to a peak of 3.6 in 2020, with an APC of 1.96% (95% CI, 1.43 to 2.49). NH American Indians and Alaska Natives had the highest starting AAMR at 3.2 in 2001, which slightly declined to 2.9 in 2020, with a non-significant APC of 0.48% (95% CI, –1.02 to 2.00). Among Hispanic and Latino individuals, the AAMR increased from 1.8 in 1999 to 3.2 in 2020 (APC 2.98%; 95% CI, 2.63 to 3.33). NH Whites showed a rise in AAMR from 1.5 to 3.1 (APC 3.52%; 95% CI, 3.32 to 3.73), while NH Blacks or African Americans had the lowest overall AAMR, increasing from 1.3 to 3.1 during the study period, but with the highest APC at 4.16% (95% CI, 3.78 to 4.53) (Figure 2).
Further analysis by sex revealed that NH American Indian and Alaska Native men had the highest race- and gender-specific AAMR at 2.36 per 100,000, followed by NH Asian and Pacific Islander men (2.33). NH American Indian and Alaska Native women had an AAMR of 1.93, while NH Asian or Pacific Islander women had a rate of 1.70. Among NH Whites, men had an AAMR of 1.67 compared to 1.26 in women. NH Black or African American men had an AAMR of 1.63, slightly higher than their female counterparts at 1.25 (Supplemental Table 3).
| Age group | Female | Male |
| 25-34 years | 0.1 (0.1-0.1) | 0.1 (0.1-0.1) |
| 35-44 years | 0.3 (0.3-0.3) | 0.3 (0.3-0.3) |
| 45-54 years | 0.9 (0.9-1.0) | 1.1 (1.1-1.1) |
| 55-64 years | 2.7 (2.6-2.7) | 3.4 (3.4-3.5) |
| 65-74 years | 5.5 (5.4-5.6) | 7.4 (7.2-7.5) |
| 75-84 years | 8.9 (8.8-9.1) | 11.9 (11.8-12.1) |
| 85 years and above | 10.7 (10.5-11.0) | 15.2 (14.9-15.6) |
Supplemental table 3: AAMR per 100,000 according to age, 1999- 2020
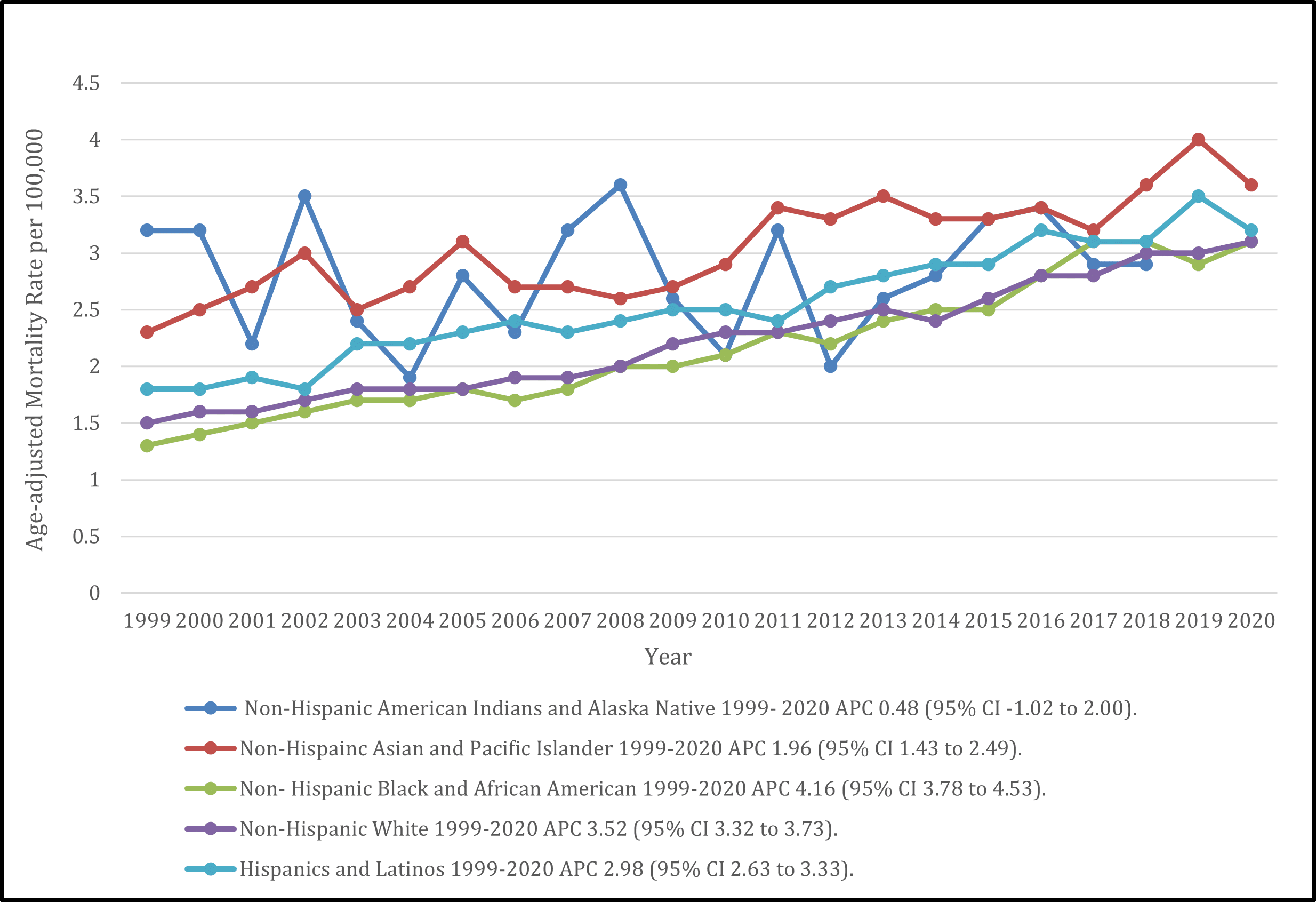
Figure 2: Race-stratified IHCC-related AAMR per 100,000 adults in the United States, 1999-2020
IHCC-associated mortality stratifies by geography: Regional differences were also seen. The Northeast had the highest IHCC-related mortality, with an average AAMR of 2.6, increasing from 1.6 in 1999 to 3.5 in 2020 (APC 3.70%, 95% CI, 3.46 to 3.93). The Midwest had an AAMR of 2.5 (1.5 in 1999 to 3.4 in 2020; APC 3.79%, 95% CI, 3.56 to 4.02), and the West also had an AAMR of 2.5 (1.6 to 3.3; APC 3.25%, 95% CI, 3.00 to 3.49). The South had the lowest mortality with an average AAMR of 2.1, increasing from 1.4 to 2.8 (APC 3.02%, 95% CI, 2.68 to 3.38) (Figure 3).
Among census divisions, New England showed the highest mortality, with an average AAMR of 2.77. Rates in this division rose from 1.7 in 1999 to a peak of 4.3 in 2019, followed by a slight decline to 3.8 in 2020 (APC 4.48%, 95% CI, 3.96 to 5.00). Within New England, New Hampshire had the highest rate, rising from 2.6 in 2001 to 5.0 in 2020. Massachusetts followed (1.6 to 4.0), along with Rhode Island (2.9 to 3.9), and Connecticut (1.6 to 3.6). Maine, however, saw a decrease, from 2.8 in 2001 to 2.2 in 2020.
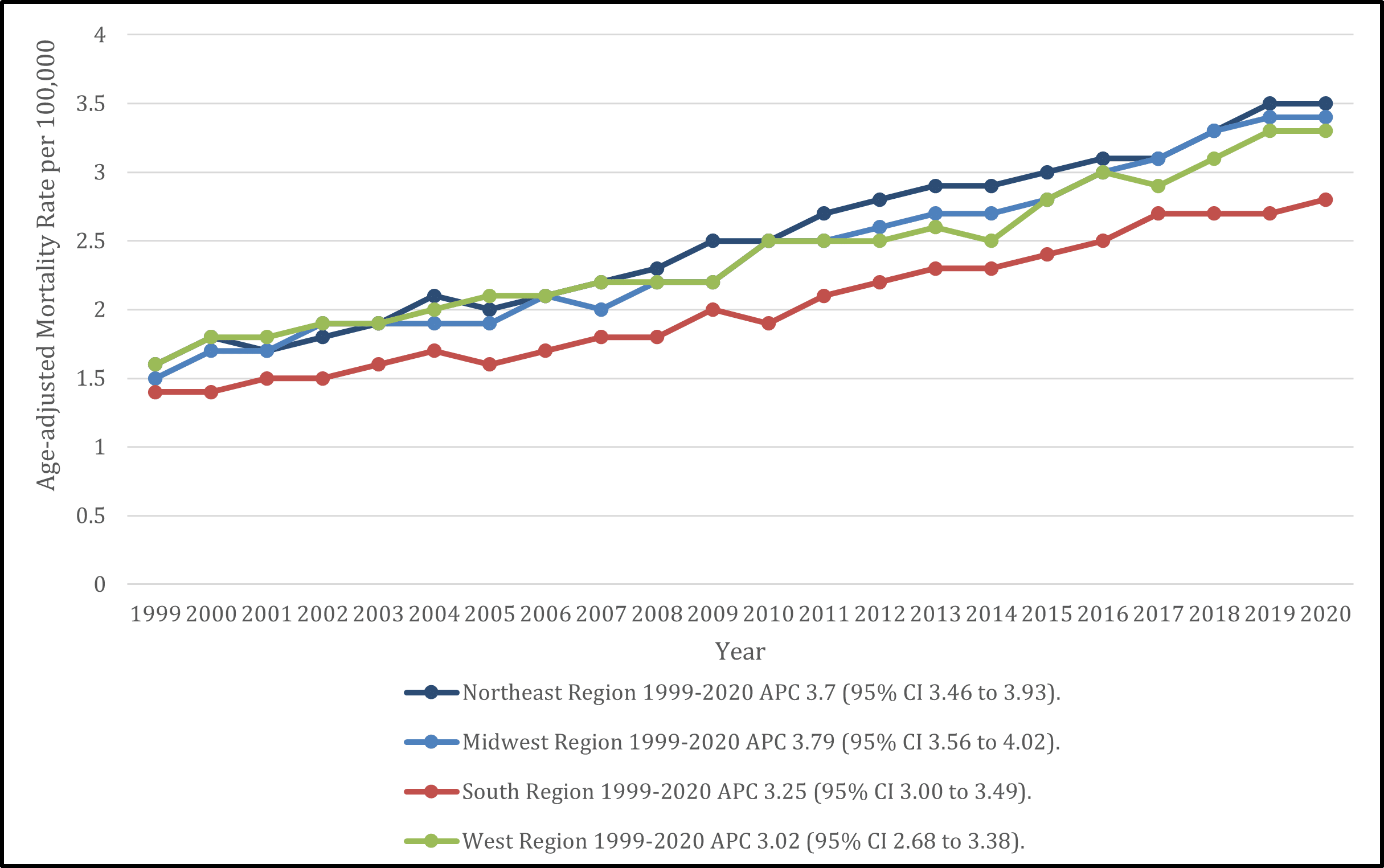
Figure 3: Census region stratified IHCC-related AAMR per 100,000 adults in the United States, 1999-2020
Among census divisions, New England depicted the highest mortality rate (overall AAMR = 2.77), which rose gradually from 1.7 in 1999 to 4.3 in 2019, followed by a fall to 3.8 the preceding year (APC = 4.48, 95% CI 3.96 to 5.00). In the New England division, New Hampshire topped the mortality list with an AAMR increasing from 2.6 in 2001 to 5.0 in 2020, followed by Massachusetts (AAMR 1.6 in 1999 and 4 in 2020, Rhode Island (AAMR 2.9 in 1999 and 3.9 in 2020), Connecticut (AAMR 1.6 in 1999 and 3.6 in 2020) and Maine (AAMR 2.8 in 2001 and 2.2 in 2020) (Figure 4).
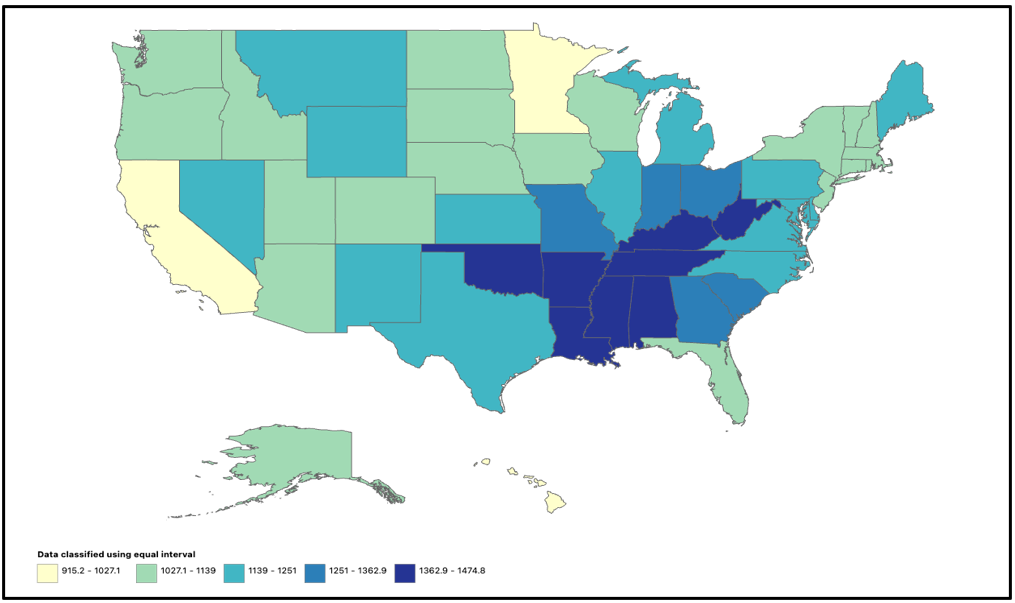
Figure 4: States stratified age-adjusted mortality rate per 100,000 adults in the United States, 1999-2020
Urbanization status also affected IHCC-related mortality. In metropolitan areas, the AAMR rose from 1.5 in 1999 to 3.2 in 2020 (APC 3.65%, 95% CI, 3.49 to 3.80), while in non-metropolitan areas it increased from 1.4 to 2.7 (APC 3.45%, 95% CI, 3.16 to 3.74). Although both areas experienced steady increases, cities consistently had higher death rates than rural regions.
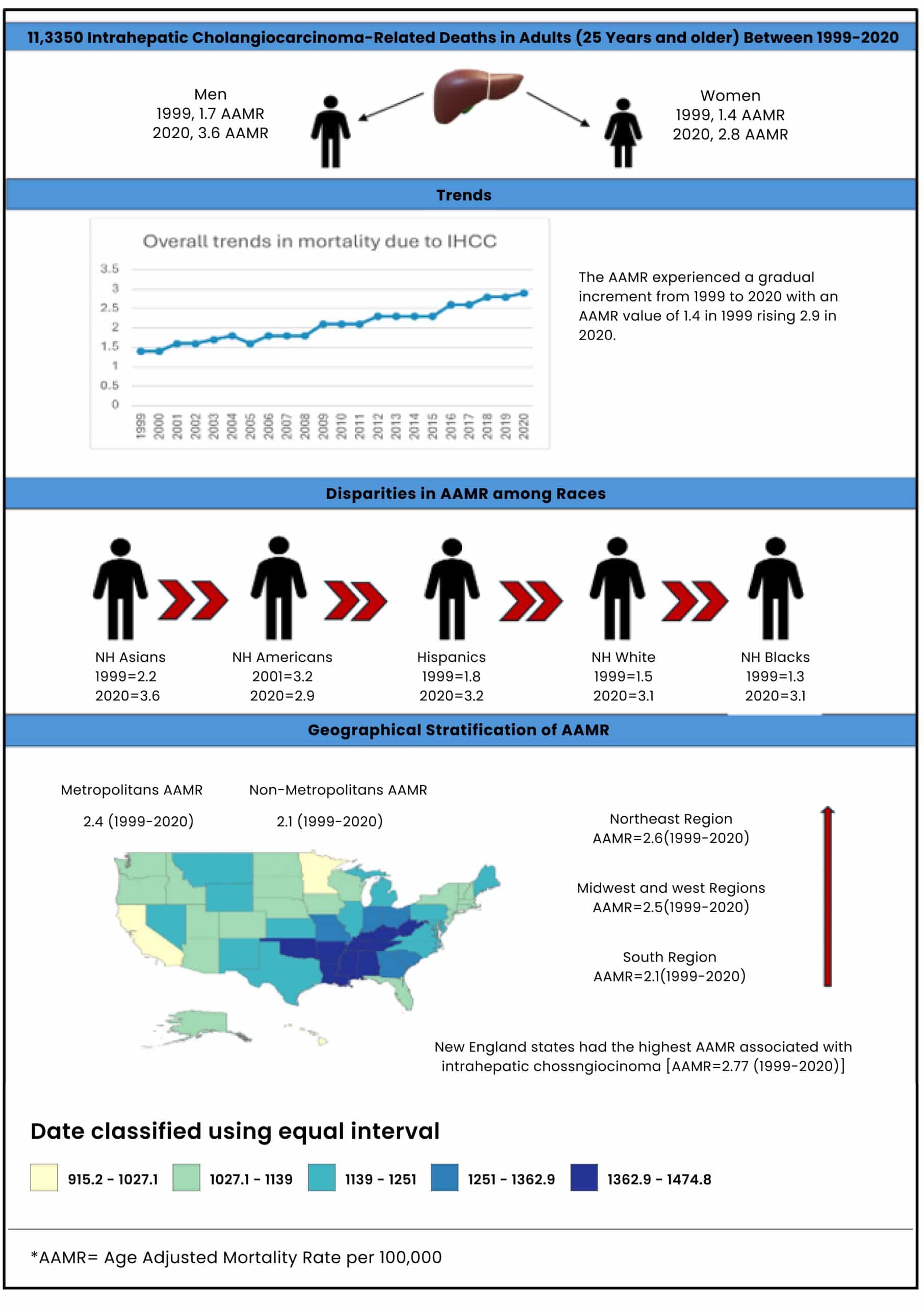
Figure 5: Central illustration of disparities in mortality trends associated with IHCC in adults of the United States between 1999 and 2020
Discussion
Previous literature reviewing hepatic cholangiocarcinoma and predominantly intrahepatic cholangiocarcinoma is sparse, yet it has discovered IHCC as the most common subtype. Therefore, our study analyzing the 20-year mortality trends from the CDC found several key findings.
Firstly, we found a rising trend in overall mortality, with several deaths being higher in 2020 as compared to those in 1999. Our results were supported by a 2022 study by Jiang et al., which depicted an upward trend in IHCC mortality and incidence from 2000 to 2018.[19] These findings raised a suspicion that the widely quoted rate of 2000-3000 yearly incidence of cholangiocarcinoma (CCA) might be due to the underestimation of the real disease burden. Our speculations are paralleled by a CDC article of 2016 by Yao et al, which demonstrated an increasing mortality of IHCC between 1999 and 2014 and a consistent rise in incidence of CCA, as per the Surveillance, Epidemiology, and End Results Program (SEER) database.[3] These rising trends can be explained by the rise in comorbidities like obesity and diabetes mellitus, which are directly and indirectly associated with the risk of developing biliary tract cancers.
Another notable finding of our study was that the mortality rate increases with an increase in age, reaching a maximum in adults over the age of 85 years. This finding is consistent with the study of 2021 by Burton et al., which demonstrated a higher mortality of liver cancers in adults over 50 years of age, with an average age of patients with IHCC being higher than that of other forms of liver cancer.[7] On the contrary, Koshiol et al. found a decrease in mortality associated with all biliary tract carcinomas in adults over the age of 80 years.[9] An increase in life expectancy in the US and a rise in the older population can be the reason behind these rising trends. In light of these results, there is a need to apply adequate and early diagnostic measures so that IHCC-related life expectancy can be improved.
Moreover, our analysis has shown higher mortality rates for males as compared to females, although the difference in mortality rates is not significant; however, this finding is consistent with multiple studies focusing on epidemiological trends for intrahepatic cholangiocarcinoma.[20] A 2016 study by Yao et al., considering data from National Center for Health Statistics (NCHS) database between years 1993 to 1997 depicted no major difference in mortality rates for females and males, with age-adjusted mortality rate for IHCC in men increasing from 0.78 per 100,000 for the period 1993- 1997, and that for women increased from 0.12 to 0.57 per 100,000 over the same period.[3] The study of Jiang et al.[19] While studying incidence-based mortality rates using the SEER database for the time period 2000-2018, we show a very minor difference in APCs among males and females, with APCs of 6.4 (95% CI 4.8-8.1) for males and 6.3 (95% CI 5.0-7.6 for females.
Considering the racial variation in mortality trends, we found a drastically higher mortality in Non-Hispanic (NH) Asian and Pacific islanders, while African Americans had the lowest age-adjusted mortality rate. Similar trends were found by Koshiol et al. in 2022, stating the highest incidence of biliary tract carcinoma in NH Asian and pacific islander.[9] Furthermore, a higher incidence of biliary tract carcinoma in NH Asians and Pacific Islanders was found in 2002 by Khan et al., further strengthening our conclusion. This variation in trend can be explained by variable utilization of health care by different racial groups.[21]
In addition to the above-mentioned variables, our study also focused on mortality trends in different geographical regions across the USA. Mortality trends in different census regions, census divisions, as well as metropolitan versus nonmetropolitan areas, were observed. The data obtained suggests that the Northeastern census region has the highest age-adjusted mortality rates among all census regions, while the Midwest region has shown the highest increase in AAMR with an APC of 3.79 (95% CI 3.56 to 4.02). The North England division of the Northeastern region has the highest age-adjusted mortality rates among all census divisions in the USA. A further state-wise analysis on the New England division revealed the highest age-adjusted mortality rates to be in New Hampshire, followed by Massachusetts, Rhode Island, Connecticut, and Maine (2.74). Data further reveals higher AAMRs in metropolitan areas (1.4 in 1999 to 2.7 in 2020) as compared to non-metropolitan areas and a persistent upward trend in mortality in both areas with metropolitan areas having an APC of 3.65 (95% CI 3.49 to 3.80) and non-metropolitan areas having an APC of 3.45 (95%CI 3.16 to 3.74). While literature regarding geographical trends in IH-CCA mortality is insufficient, a study by Yang et al discussing epidemiology of biliary tract cancers in the Olmstead county of Minnesota state in the Mid-West region of the USA from 1976 to 2008 does suggest increasing incidence in IH-CCA (sex adjusted incidence rates increasing from 0.3 to 2.1 per 100,000 person-years between 1976 and 2008) but mortality data was not reported in the study.
Another variable for which data were available was the place of death for IHCC-related mortality. Using the CDC WONDER database, our study found that most deaths occurred in the home setting, followed by hospital, hospice, nursing homes/long-term care facilities, in decreasing order. The severe nature of the malignancy may be the reason behind the disposition of many end-stage patients to home hospice, followed by subsequent death at the descendant’s home.
Limitations: There are several limitations associated with our study that need to be considered. Firstly, the data extraction from the CDC WONDER database relies solely on death certificates, which state IH-CCA as the underlying cause of death and use the appropriate ICD-10 code; there is an underlying possibility of misclassification of cause of death or its omission altogether. Moreover, data concerning races like American Indians, which conventionally may not utilize healthcare facilities, might be misrepresented as well, as depicted by the CDC WONDER having multiple years of unreliable data for this particular racial group. This left us with limited reliable data, which thus made the data pool for Native Americans, limiting the accuracy of our results. Similarly, data for the state of Vermont in the New England division presented the same issue and was subsequently excluded from the study as well.
Conclusion
Our study evaluates AAMRs across the years 1999-2020, and the data consistently reveal a rise in mortality related to IHCC in adults greater than 25 years of age in the USA. The highest AAMRs in adults above 85 years of age, men, NH Asian and Pacific Islanders, the Northeast region, and metropolitan areas are observed. IHCC, along with being the second most common primary liver cancer, is further associated with poor prognostic outcomes, and thus, this study serves to further press the need for improving diagnostic and treatment modalities of this disease.
References
- Gad MM, Saad AM, Faisaluddin M, et al. Epidemiology of Cholangiocarcinoma; United States Incidence and Mortality Trends. Clin Res Hepatol Gastroenterol. 2020;44(6):885-893. doi:10.1016/j.clinre.2020.03.024 PubMed | Crossref | Google Scholar
- Young AL, Prasad KR, Toogood GJ, Lodge JP. Surgical treatment of hilar cholangiocarcinoma in a new era: comparison among leading Eastern and Western centers, Leeds. J Hepatobiliary Pancreat Sci. 2010;17(4):497-504. doi:10.1007/s00534-009-0203-6 PubMed | Crossref | Google Scholar
- Yao KJ, Jabbour S, Parekh N, Lin Y, Moss RA. Increasing mortality in the United States from cholangiocarcinoma: an analysis of the National Center for Health Statistics Database. BMC Gastroenterol. 2016;16(1):117. doi:10.1186/s12876-016-0527-z PubMed | Crossref | Google Scholar
- Patel T. Worldwide trends in mortality from biliary tract malignancies. BMC Cancer. 2002;2:10. doi:10.1186/1471-2407-2-10 PubMed | Crossref | Google Scholar
- Nathan H, Pawlik TM, Wolfgang CL, Choti MA, Cameron JL, Schulick RD. Trends in survival after surgery for cholangiocarcinoma: a 30-year population-based SEER database analysis. J Gastrointest Surg. 2007;11(11):1488-1497. doi:10.1007/s11605-007-0282-0 PubMed | Crossref | Google Scholar
- Bertuccio P, Malvezzi M, Carioli G, et al. Global trends in mortality from intrahepatic and extrahepatic cholangiocarcinoma. J Hepatol. 2019;71(1):104-114. doi:10.1016/j.jhep.2019.03.013 PubMed | Crossref | Google Scholar
- Burton A, Tataru D, Driver RJ, et al. Primary liver cancer in the UK: Incidence, incidence-based mortality, and survival by subtype, sex, and nation. JHEP Rep. 2021;3(2):100232. doi:10.1016/j.jhepr.2021.100232 PubMed | Crossref | Google Scholar
- Patel T. Increasing incidence and mortality of primary intrahepatic cholangiocarcinoma in the United States. Hepatology. 2001;33(6):1353-1357. doi:10.1053/jhep.2001.25087 PubMed | Crossref | Google Scholar
- Koshiol J, Yu B, Kabadi SM, Baria K, Shroff RT. Epidemiologic patterns of biliary tract cancer in the United States: 2001-2015. BMC Cancer. 2022;22(1):1178. doi:10.1186/s12885-022-10286-z PubMed | Crossref | Google Scholar
- Yang JD, Kim B, Sanderson SO, et al. Biliary tract cancers in Olmsted County, Minnesota, 1976-2008. Am J Gastroenterol. 2012;107(8):1256-1262. doi:10.1038/ajg.2012.173 PubMed | Crossref | Google Scholar
- Javle M, Lee S, Azad NS, et al. Temporal Changes in Cholangiocarcinoma Incidence and Mortality in the United States from 2001 to 2017. Oncologist. 2022;27(10):874-883. doi:10.1093/oncolo/oyac150 PubMed | Crossref | Google Scholar
- Beal EW, Tumin D, Moris D, et al. Cohort contributions to trends in the incidence and mortality of intrahepatic cholangiocarcinoma. Hepatobiliary Surg Nutr. 2018;7(4):270-276. doi:10.21037/hbsn.2018.03.16 PubMed | Crossref | Google Scholar
- Hucke F, Pinter M, Hucke M, et al. Changing Epidemiological Trends of Hepatobiliary Carcinomas in Austria 2010-2018. Cancers (Basel). 2022;14(13):3093. doi:10.3390/cancers14133093 PubMed | Crossref | Google Scholar
- Centers for Disease Control and Prevention (CDC). CDC WONDER: Multiple Cause of Death Data. Updated February 28, 2024. Accessed May 19, 2025. CDC WONDER: Multiple Cause of Death Data
- Ingram DD, Franco SJ. NCHS urban-rural classification scheme for counties. Vital Health Stat 2. 2012;(154):1-65. NCHS urban-rural classification scheme for counties
- Aggarwal R, Chiu N, Loccoh EC, Kazi DS, Yeh RW, Wadhera RK. Rural-Urban Disparities: Diabetes, Hypertension, Heart Disease, and Stroke Mortality Among Black and White Adults, 1999-2018. J Am Coll Cardiol. 2021;77(11):1480-1481. doi:10.1016/j.jacc.2021.01.032 PubMed | Crossref | Google Scholar
- Anderson RN, Rosenberg HM. Age standardization of death rates: implementation of the year 2000 standard. Natl Vital Stat Rep. 1998;47(3):1-20. Age standardization of death rates: implementation of the year 2000 standard
- National Cancer Institute-Division of Cancer Control & Population Sciences. Joinpoint Trend Analysis Software. Published April 16, 2025. Accessed May 19, 2025. Joinpoint Trend Analysis Software
- Jiang Y, Jiang L, Li F, et al. The epidemiological trends of biliary tract cancers in the United States of America. BMC Gastroenterol. 2022;22(1):546. doi:10.1186/s12876-022-02637-8 PubMed | Crossref | Google Scholar
- Nephew LD, Gupta D, Carter A, et al. Social determinants of health impact mortality from HCC and cholangiocarcinoma: a population-based cohort study. Hepatol Commun. 2023;7(3):e0058. doi:10.1097/HC9.0000000000000058 PubMed | Crossref | Google Scholar
- Khan SA, Taylor-Robinson SD, Toledano MB, Beck A, Elliott P, Thomas HC. Changing international trends in mortality rates for liver, biliary and pancreatic tumours. J Hepatol. 2002;37(6):806-813. doi:10.1016/s0168-8278(02)00297-0 PubMed | Crossref | Google Scholar
Acknowledgments
No acknowledgments
Funding
The authors involved in the formulation of this manuscript have not received any form of financial support from agencies in the public, commercial, or not-for-profit sectors.
Author Information
Corresponding Author:
Rohab Sohail
Department of Internal Medicine
Bayhealth Medical Center, Delaware, USA
Email: [email protected]
Co-Authors:
Ridda Khattak
Department of Internal Medicine
Bayhealth Medical Center, Dover, DE, USA
Ramsha Mumtaz
Department of Medicine
Rawalpindi Medical University, Rawalpindi, Punjab, Pakistan
Ansab Godil, Muhammad Ahsen Niazi
Department of Medicine
Dow Medical College, Karachi, Sindh, Pakistan
Sana Aijaz
Department of Medicine
Bahria University Medical College, Karachi, Sindh, Pakistan
Salman Sani
Department of Internal Medicine
Allama Iqbal Medical College, Lahore, Punjab, Pakistan
Myra Niaz
Department of Medicine
Shahida Islam Medical College, Lodhran, Punjab, Pakistan
Qazi M Zarlish
Department of Medicine
Ch Pervaiz Elahi Institute of Cardiology, Multan, Punjab, Pakistan
Mahnoor Jabeen
Department of Medicine
Karachi Medical and Dental College, Karachi, Sindh, Pakistan
Seemab Fatima
Department of Medicine
Services Institute of Medical Sciences, Lahore, Punjab, Pakistan
Adeel Ahmed
Department of Gastroenterology
University of Kentucky, Kentucky, USA
Authors Contributions
Rohab Sohail was responsible for topic search, formal screening using Google Scholar and PubMed, and data analysis. Ridda Khattak contributed by defining outcomes, extracting data, preparing figures, and writing the discussion. Ramsha Mumtaz worked on topic search, data extraction, and the results section. Ansab Godil was involved in topic search, drafting the introduction, and compiling the manuscript. Sana Aijaz contributed through topic search, formal screening, and assisting with the results. Muhammad Ahsen Niazi focused on topic search, the methods section, and general literature searches. Salman Sani was engaged in topic search, formal screening, and contributed to the discussion. Myra Niaz participated in the topic search and data extraction. Qazi M. Zarlish and Mahnoor Jabeen both contributed to the topic search and discussion. Seemab Fatima was responsible for manuscript writing, while Adeel Ahmed reviewed the manuscript.
Ethical Approval
Not applicable
Conflict of Interest Statement
The authors declare no conflict of interest.
Guarantor
The guarantor for the project is Syed Nazeer Mehmood, MD.
DOI
Cite this Article
Sohail R, Khattak R, Mumtaz R, et al. Temporal Trends and Disparities Related to Intrahepatic Cholangiocarcinoma Among Adults Living in the United States: A 1999 to 2020 Retrospective Analysis. medtigo J Med. 2025;3(2):e30623220. doi:10.63096/medtigo30623220 Crossref













