






 Author Affiliations
Author Affiliations
Abstract
Background: Timely initiation of antenatal care (ANC) is crucial for clinical practices, including routine hypertension screening, fetal heart sound detection, illness identification, eradicating inequalities, providing psychological support, and postpartum family planning. However, the timely start and coverage of prenatal care differ throughout continents, nations, regions, and even within an area. Therefore, this study aims to determine the pooled prevalence of timely initiation of antenatal care and its associated factors.
Methods: The studies were searched in various databases such as PubMed, MEDLINE, ScienceDirect, Embase, Google Scholar, Cochran Library, Africa Journal of Online, and university repository. Found 23 research publications, and data was extracted using Microsoft Excel 365 and analyzed using the STATA 17 version. Heterogeneity (I2) was found, and a random effect model was used to determine the pooled prevalence of timely prenatal care commencing. Related factors were also investigated.
Result: The overall pooled prevalence of timely initiation of antenatal care among the pregnant women in Ethiopia was 37% (95% CI: 33–42), with statistical heterogeneity (I2 = 98.32%, p = 0.00). Good knowledge about antenatal care (OR=2.2, 95% CI: 1.78-2.62), a secondary education or above (OR=2.32, 95% CI: 1.49-3.14), received advice and counseling (OR= 95% CI:1.76-3.23), planned pregnancy (OR=3.8, 95% CI:2.30-5.30), primigravida (OR=2.21, 95% CI:1.73-2.269), urban residence (OR=2.59, 95% CI: 1.56-3.62) and pregnancy recognition urine test (OR=3.17; 95% CI:1.88-4.46) are the associated of timely initiation of antenatal care.
Conclusion: The study indicates that timely antenatal care initiation is low, linked to factors like anticipatory counseling knowledge, education, being a primigravida, urban living, pregnancy detection, planned pregnancy, wealth index, and medical guidance. Regular monitoring and evaluation are needed to reduce complications and improve birth preparedness.
Keywords
Timely initiation, Antenatal care, Pregnant women, Associated factors, Systematic review, Meta-analysis, Prevalence.
Introduction
Antenatal care is care given to pregnant women during the antenatal period that may be essential to their health and the health and wellness of their unborn children.[1] While pregnancy is a normal physiological process, about 5–20 percent of pregnancies end in difficulties that raise the mother’s and/or the fetus’s mortality or morbidity.[2] Previously, focused antenatal care was recommended for four visits, with the first visit starting in the first trimester of the pregnancy.[3] Currently, to lower perinatal mortality and enhance women’s experiences with care, the 2016 World health organization (WHO) suggested new ANC models with a minimum of eight encounters in which the first contact is recommended less than 12 weeks, which is considered timely initiation of antenatal care.[4] The number of ANC visits and coverage increases with timely ANC initiation. This, in turn, helps pregnant women become more aware of the danger signs that arise both during pregnancy and the postpartum period, further contributing to the reduction of mortality and morbidity in both the mother and her unborn child.[5]
ANC is a care given during pregnancy and a pregnancy-related service that offers a foundation for critical health-related tasks like early illness prevention, screening, and diagnosis. It has been proven that ANC can save lives when used in a timely and suitable manner, employing evidence-based approaches.[6] Furthermore, it helps to decrease complications during gestation, labor, delivery, and the postpartum period. ANC aims to identify pregnant women at high risk and provide special care for the mother and baby.[7,8] The quality of ANC care was very important in preventing and reducing the complications occurring among the mother and baby.[9] Besides this quality of antenatal care, coverage lagged in low-income countries when compared to high-income countries. Additionally, the timely initiation of antenatal care was more prevalent in high-income countries than in low-income countries.[10]
The timely initiating rate of the ANC over the world from 1990 to 2013 was 58.6% and accounted for about 84.8 percent of high-income countries and 48.1.0 percent of low-income countries, respectively.[11] Furthermore, the study reveals that the overall timely ANC initiation rate was 92.5% in the United States of America,[12] and 11% in Bangladesh.[13] In Sub-Saharan Africa, it was 38 percent, with a range of 14.5 percent in Mozambique to 68.6 percent in Liberia.[14] This variation might be due to the fact that the extent to which the recommended ANC interventions are implemented, need to be introduced, or require higher-quality delivery will differ across countries.[15]
In Ethiopia, the timely initiation of ANC care ranged between 20% and 65.9%.[16,17] Furthermore, according to the final result of the 2019 Ethiopian mini-demographic survey, roughly 28% of pregnant women began prenatal treatment within the first trimester of their pregnancy.[18] The timing and actual coverage of ANC care varied across the continent and between countries due to several factors, including socio-economic conditions, healthcare infrastructure, cultural norms, and socio-demographic factors.[19-22] Various studies show that knowledge of pregnant women, sociodemographic characteristics (age, residence, education level, occupation, wealth index), obstetrical and medical factors (parity, prior experience, recognition of the pregnancy test, birth experience), and getting advice from a health care provider were all associated with the timely initiation of ANC.[23-28]
The WHO recommendation of ANC within the first 12 weeks helps to timely initiation of ANC was important for good clinical practices, which are defined as routine screening for hypertensive illnesses throughout pregnancy by frequent blood pressure monitoring, fetal heart detection, timely identification of illness, elimination of inequalities, provision of psychological support, postpartum family planning, and birth preparedness counselling.[29-31]
Timely initiation of ANC is an essential component in guaranteeing the best possible health outcomes for both the mother and the newborn.[32] Despite its importance, previous studies reveal variation in the prevalence of timely initiation of ANC and associated factors between regions and within a region.[16,19,26,27,29,33-35] Generally, there is a lack of compressive understanding of the timely initiation of antenatal care and associated factors that may increase the complexity of assessing it. Thus, to close these information gaps and provide a comprehensive description of the prevalence and contributing factors, a systematic review and meta-analysis are necessary. Our study was conducted using preferred reporting items for systematic review and meta-analysis statement (PRISMA) guideline.[36] By conducting an extensive examination of the existing data, this study aims to bridge this information gap and contribute to the existing literature by providing incisive suggestions for researchers, healthcare practitioners, and policymakers to encourage and promote the timely beginning of ANC.
Methodology
Study design and setting: This systematic review and meta-analysis were conducted in Ethiopia to assess the pooled prevalence and factors associated with the timely initiation of ANC among pregnant women. Ethiopia is a country found in East Africa with a total population of more than 120 million and is currently working on decreasing maternal and neonatal mortality by following the recommendations of the WHO. The study was not registered on PROSPERO.
Reporting: This systematic review and meta-analysis followed the PRISMA criteria.[36]
Selection and eligibility criteria
Inclusion criteria: The Population, Intervention, Comparison, and Outcome (PICO) tools were utilized by the authors to establish the inclusion and exclusion criteria for this systematic and meta-analysis. All studies conducted in Ethiopia on the timely initiation of ANC among pregnant women were included in this analysis. Included were studies with relevant data on prevalence, related variables, sample size, and outcome.
Study design: Cross-sectional studies were included.
Language: All research conducted in the English language.
Publication condition and time: published and unpublished studies between 2014 and 2024 were included.
Population: Pregnant women
Outcome variable: Timely initiation of ANC
Exposure: factors associated with the timely initiation of ANC.
Exclusion criteria: We exclude studies that were qualitative, of poor quality, had unintended results, were duplicated, or lacked full length. Furthermore, not included was research on delayed initiation.
Searching strategies: The search for research articles was conducted from January 1 to February 10, 2024, using different databases such as PubMed, MEDLINE, ScienceDirect, Cochrane Library, Embase, Google Scholar, and the African Journal of Online. In the starting point, a compressive search was performed using the title “Timely Initiation of Antenatal Care (ANC) AND Associating Factors among the Pregnant Women Attending Antenatal Care Clinic in Ethiopia” and the keywords “Timely Initiation”, “Early Initiation”, “Antenatal Care (ANC)”, “Pregnant Women”, “Associated Factors”, “Predictors,” “Attending Antenatal Care Clinic”, “Health Care Facilities” and “Ethiopia”). The Boolean operations “OR” and “AND” are used independently or in combination to connect the keyword and concept to establish search terms. Furthermore, Addis Ababa and Jimma University institutional repository searches were performed.
The population, exposure, comparison, and outcome statements were employed in this review. Population: pregnant women attending antenatal care at health facilities in Ethiopia. Exposure: associated factors (variables) such as demographic factors, obstetrical factors, knowledge, and information-related factors. Comparison: the reference group mentioned in every primary study finding. Outcome: timely initiation of ANC among pregnant women.
Data extraction: Data extraction was done by four authors (SHN, GT, DD, and SHT) independently using different databases using a piloted data extraction spread sheet on Microsoft Excel that included contents of data such as author name, year of publication, study area, study design, sample size, prevalence, associated variables, and study population. The relevance of the retrieved papers to the study issue is evaluated by screening them using their titles and abstracts. The studies that met the inclusion requirements were moved to the next step. The discrepancy between reviewers can be resolved through discussion and re-evaluation.
Data quality assessment: We have used the Newcastle Ottawa Scale (NOS) of a cross-sectional study design to assess the quality of the article.[37] The scale has Selection, comparability, and outcome or exposure are the three aspects that each component has, and a maximum score of nine points is possible for each (eight items in total). A score of 0–2 is regarded as low quality, a score of 3–5 as moderate quality, and a score of 6 or more as good or high quality. The quality of the article was evaluated independently by three authors (BM, GW, and MY). SHN and DD worked together to settle any disputes. After the data extraction process, SHN and SHT combined the data and prepared it for statistical analysis.
Characteristics of study: This systematic review and meta-analysis included 21 studies conducted in Ethiopia on a total population of 21758, which ranged from 239 to 6645. The included studies were cross-sectional and were conducted among pregnant women attending antenatal care in public health facilities in Ethiopia on the timely initiation of ANC. The prevalence of timely initiation of ANC ranges from 20% to 65.9% (Table 1).
| Authors | Year | Study Area | Prevalence | Sample size | Study design | Quality |
| Edessa A et al.[20] | 2023 | Oromia | 30.50% | 344 | CS | Good |
| Lema Abate et al.[38] | 2022 | EDHS | 31% | 3065 | CS | Good |
| Girmatsion Fisseha et al.[39] | 2015 | Tigray | 32.70% | 410 | CS | Good |
| Cheru Kore et al.[21] | 2021 | Addis Ababa | 47.60% | 334 | CS | Moderate |
| Berhanu Teshome et al.[16] | 2021 | EDHS | 20% | 6645 | CS | Good |
| Alemwork Getninet et al.[22] | 2021 | Amhara | 31.50% | 820 | CS | Good |
| Tsigereda Abebe et al.[40] | 2017 | Addis Ababa | 26.10% | 422 | CS | Good |
| Megersa, Getu et al.[41] | 2017 | Oromia | 37% | 334 | CS | Moderate |
| Samuel Hailu et al.[17] | 2022 | Oromia | 65.90% | 401 | CS | Good |
| M Dembelu, et al.[18] | 2016 | SNNPR | 39% | 255 | CS | Moderate |
| Hanna Gulema et al.[23] | 2017 | Addis Ababa | 42% | 979 | CS | Good |
| Girma Tufa et al.[42] | 2020 | Oromia | 57.80% | 377 | CS | Moderate |
| Azimeraw Arega et al.[28] | 2021 | Amhara | 44.20% | 804 | CS | Good |
| Teshome Abuka et al.[24] | 2016 | SNNPR | 35.40% | 369 | CS | Moderate |
| Dagmawit Tessema et al.[19] | 2022 | SNNPR | 34.30% | 348 | CS | Moderate |
| Berhanu G. et al.[26] | 2019 | EDHS | 27.50% | 386 | CS | Moderate |
| Workaferu Fetene et al.[43] | 2023 | Amhara | 40% | 748 | CS | Good |
| E Ambaye et al.[44] | 2022 | Amhara | 48.60% | 592 | CS | Good |
| Mekdes Kondale et al.[29] | 2016 | SNNPR | 27.10% | 249 | CS | Moderate |
| TW Gudayu et al.[45] | 2014 | Amhara | 35.40% | 407 | CS | Good |
| Toffik Redi et al.[46] | 2019 | Oromia | 41.90% | 375 | CS | Moderate |
| Kasiye Shiferaw et al.[25] | 2021 | EDHS | 26.80% | 2855 | CS | good |
| Gebreamlak Gidey et al.[33] | 2017 | Tigray | 41% | 239 | CS | Moderate |
Table 1: Characteristics of studies
SNNPR: Southern Nation Nationalities of people region
Measure outcome of Interest: The main outcome of this study was to estimate the overall pooled prevalence of timely initiation of ANC among pregnant women attending antenatal care in Ethiopia. The next outcome was determining the factors associated with timely ANC using an adjusted pooled odds ratio with a 95% confidence level. When it begins before 12 weeks of gestation, it is considered timely to initiate when it starts before 12 weeks of gestational age.
Data analysis: After relevant data has been extracted from studies using Microsoft Excel 2019, the authors synthesize and analyze the data using “statistics” and “data” (STATA) version 17 software. The primary studies were summarized and presented in a frost plot and table. We have computed the standard error of the prevalence of timely initiation of antenatal care for every primary research study. We identify the presence of heterogeneity I2 among the studies, which is interpreted as a percentage of total variation between studies. Heterogeneity can be considered low, moderate, and high if I2 = 25, I2 = 50, and I2 = 75, respectively. The statistical test analysis reveals that there is considerable heterogeneity among the studies (I2 = 98.04%, P = 0.00). A random effect model was used with the Der Simonian-Lair approach to estimate the pooled effect.[47]
Publication bias: Egger’s correlation weight and Begg’s regression intercept test were used to examine publication bias at the 5% significance level.[48] A funnel plot was used to indicate the symmetrical distribution of the studies. Subgroup analysis was carried out based on regions and publication by classifying to decrease the random variation among estimated points of primary studies (Figure 1).
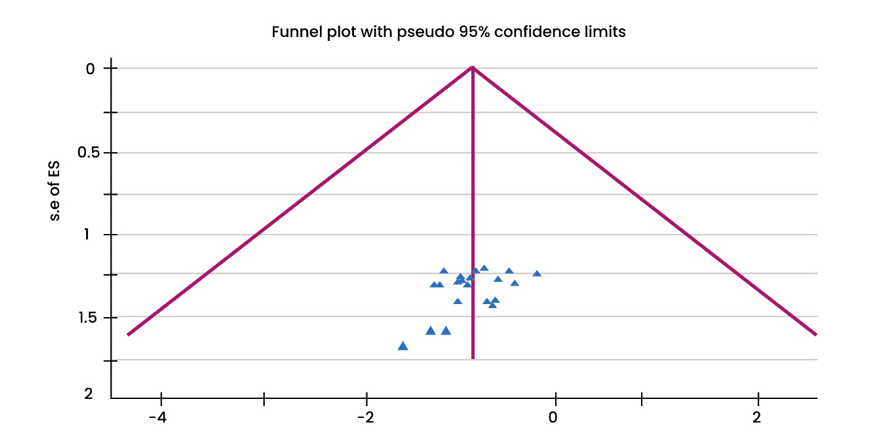
Figure 1: Funnel plot to show the distribution of studies publication bias on the timely initiation of ANC among pregnant women,2024
Results
Initially, we obtained 560 entries from the databases of PubMed, MEDLINE, ScienceDirect, Embase, Google Scholar, Cochran Library, and the Africa Journal of Online, together with 5 records from the university repository. 432 records were eliminated due to duplication. 133 records were obtained after the authors assessed the lack of relevant abstracts and titles. 57 of the remaining 133 were removed after their relevance was assessed. After that, the authors analyzed and appraised 76 complete texts to determine the inclusion criteria. In conclusion, these systematic reviews and meta-analyses comprised 23 research papers deemed pertinent (Figure 2).
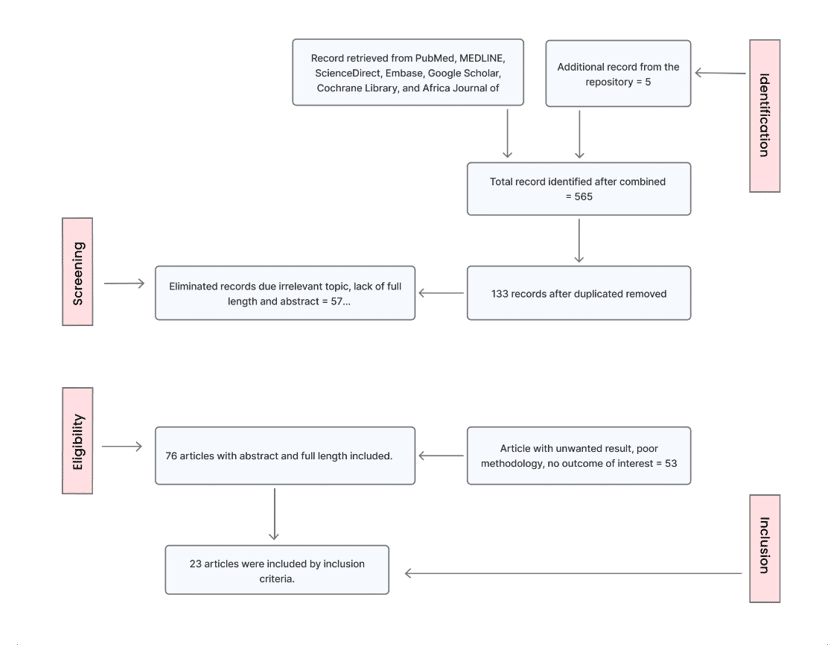
Figure 2: Flow chart illustrates the selection of research articles using PRISMA checklist, 2024
Prevalence of timely initiation of ANC: The overall pooled prevalence of timely initiation of ANC among pregnant women in Ethiopia was 37% (95% CI: 33-42). The statistical heterogeneity observed was I2=98.32%, p=0.00 (Figure 3).
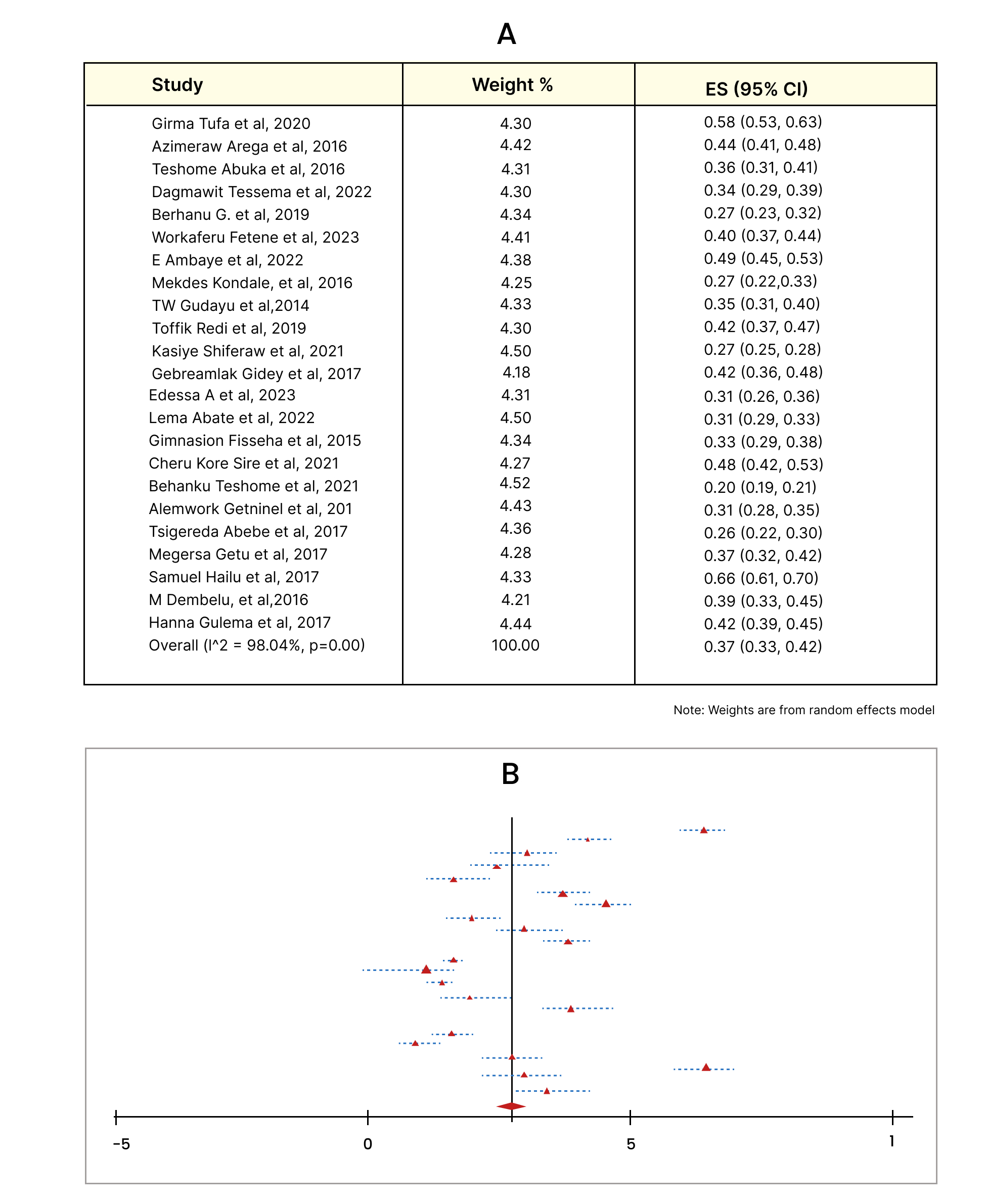
Figure 3: The overall pooled prevalence of timely initiation of ANC among pregnant women attending antenatal care in Ethiopia in 2024
Factors associated with Timely initiation of ANC: Our study shows that pregnant women who have good knowledge about antenatal care were 2.2 times more likely to timely initiate ANC care than women who have poor knowledge (OR = 2.2, 95% CI: 1.78–2.62) (Figure 4).
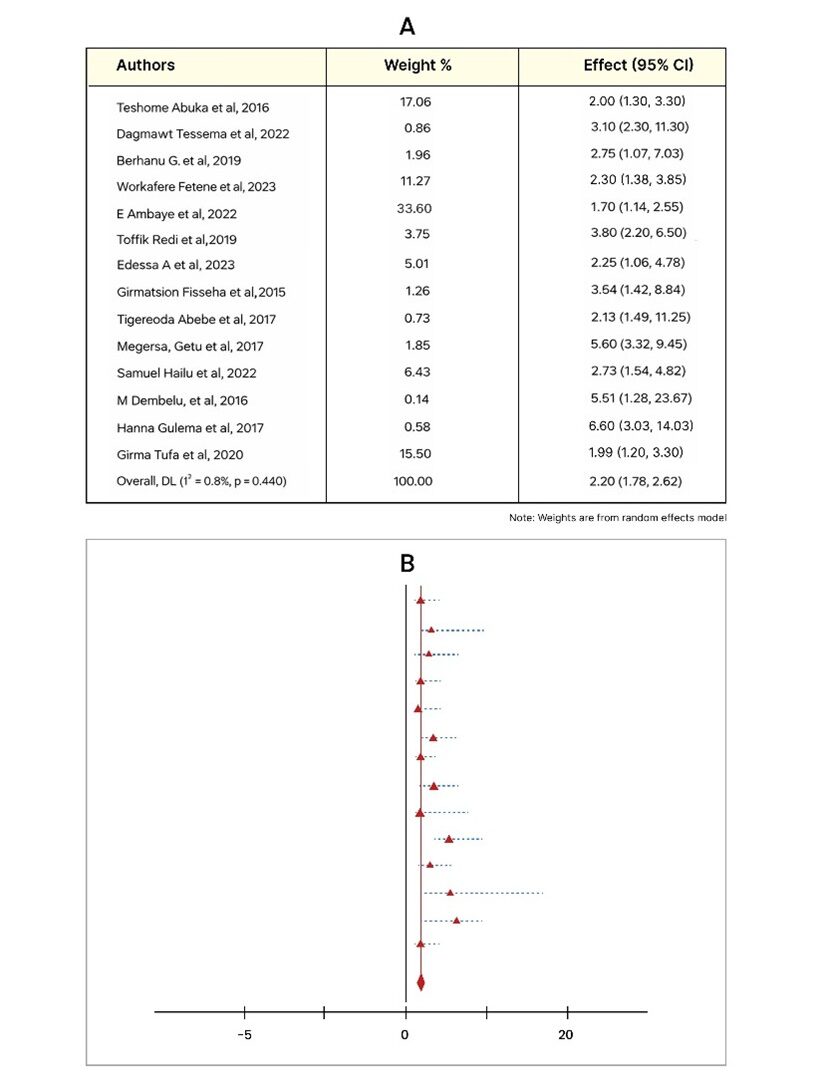
Figure 4: Forest plot for the association between knowledge and timely initiation of ANC among pregnant women, 2024
Pregnant women with a secondary education or above were 2.3 times more likely to start ANC on time than those with less education (OR=2.32, 95% CI: 1.49-3.14) (Figure 5).
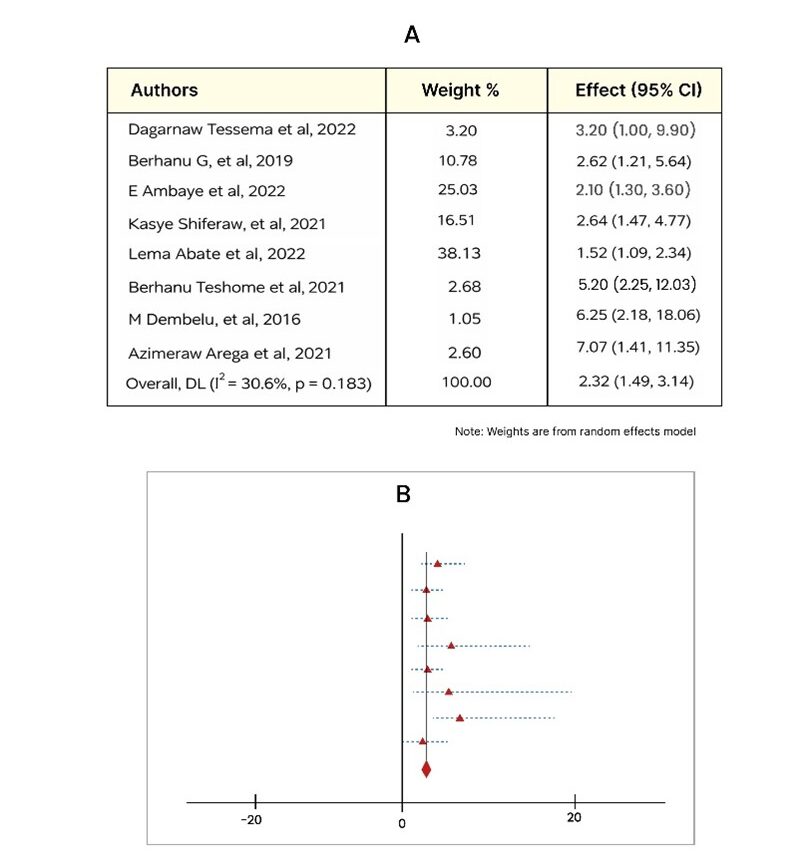
Figure 5: Frost plot that shows an association between secondary education or above and timely initiation ANC among pregnant women, 2024
As illustrated in Figure 6, eight studies revealed a positive correlation between health care providers’ guidance and t,herefore, pregnant women’s timely ANC begins. Women who received advice and counseling from their healthcare provider were 2.5 times more likely to timely commence ANC than their counterparts who did not receive such advice and counseling (OR = 95% CI: 1.76-3.23).
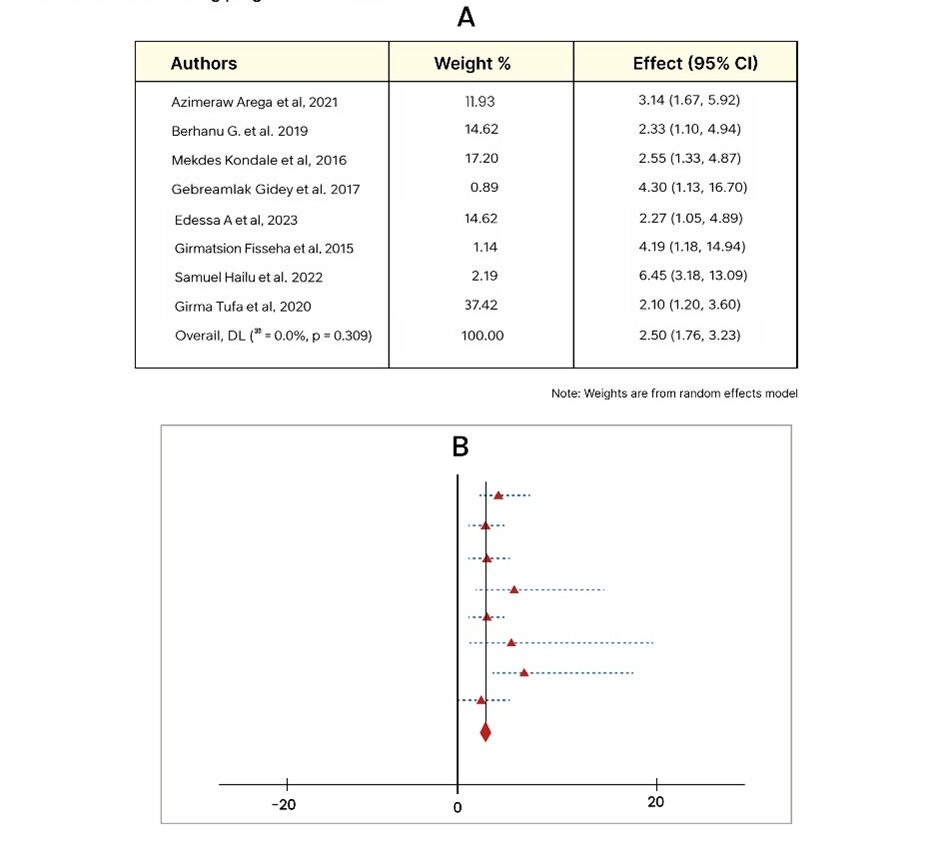
Figure 6: The Frost plot shows the association between counseling received from their healthcare and the timely initiation of ANC among pregnant women in 2024
According to the five studies analyzed, planned pregnancy has a significant association with the timely initiation of ANC. Therefore, the overall estimate of the pooled prevalence odds ratio shows that pregnant women who had planned their pregnancy were 3.8 times more likely to timely initiate ANC than those who had not planned their pregnancy (OR = 3.8, 95% CI: 2.30–5.30) (Figure 7).
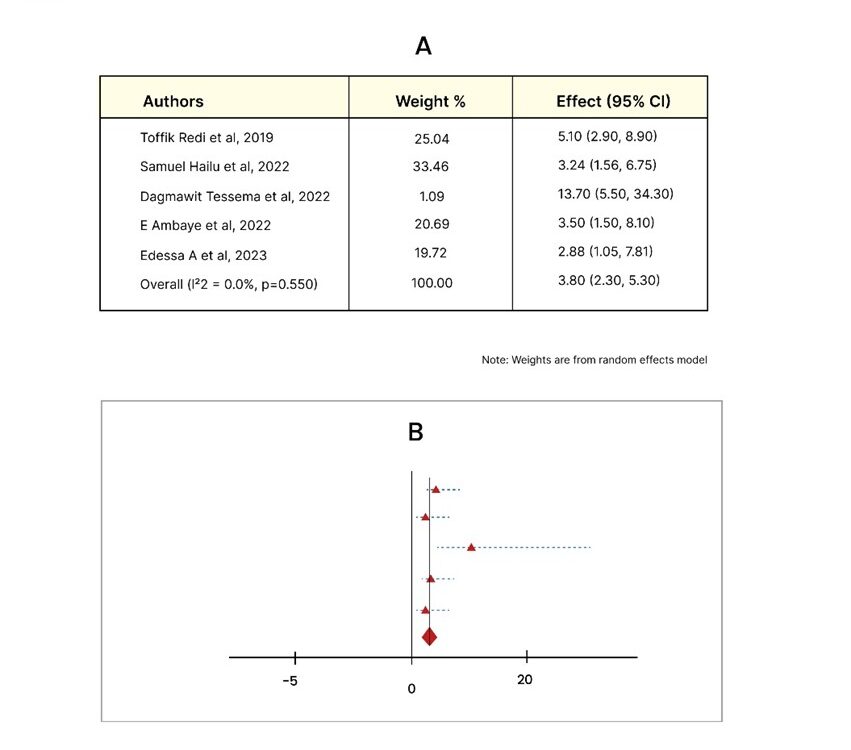
Figure 7: The frost plot of planned pregnancy and timely initiation of ANC among the pregnant women, 2024
As illustrated in Figure 8, women who confirmed their pregnancy via urine test at health care facilities were 3.17 times more likely to initiate ANC than women who confirmed their pregnancy through a missed period (OR = 3.17; 95% CI: 1.88–4.46).
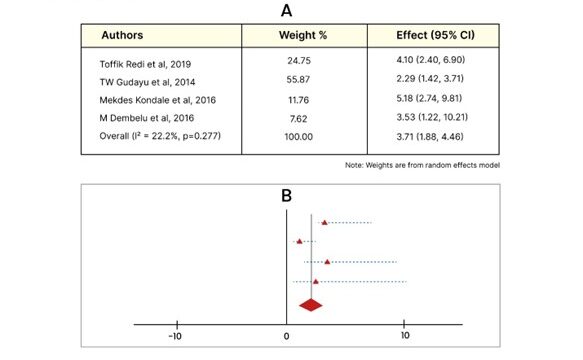
Figure 8: Frost plot of confirmed pregnancy via urine test association with timely initiation of ANC among pregnant women, 2024
Furthermore, Pregnant women who primigravida where 2.21 times more likely start ANC on time than multipara pregnant women (OR= 2.21, 95% CI:1.73-2.269) (Figure 9).
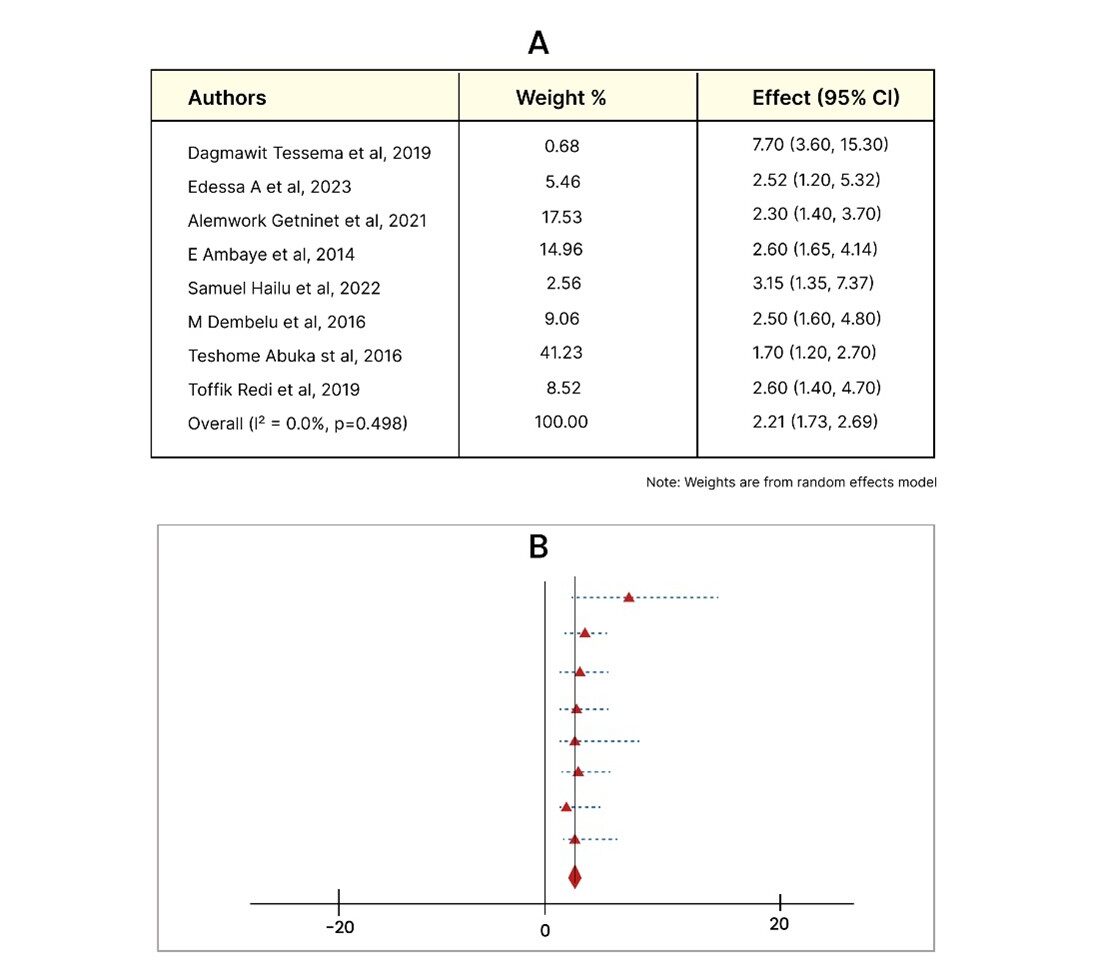
Figure 9: Frost plot shows the association between primigravida and timely initiation of ANC among the pregnant women, 2024
Finally, three studies were pooled and show an association between urban residence and timely initiation among pregnant women. Therefore, pregnant women who reside in urban areas were 2.59 times more likely to initiate ANC timely than those living in rural areas (OR = 2.59, 95%; CI: 1.56-3.62) (Figure 10).
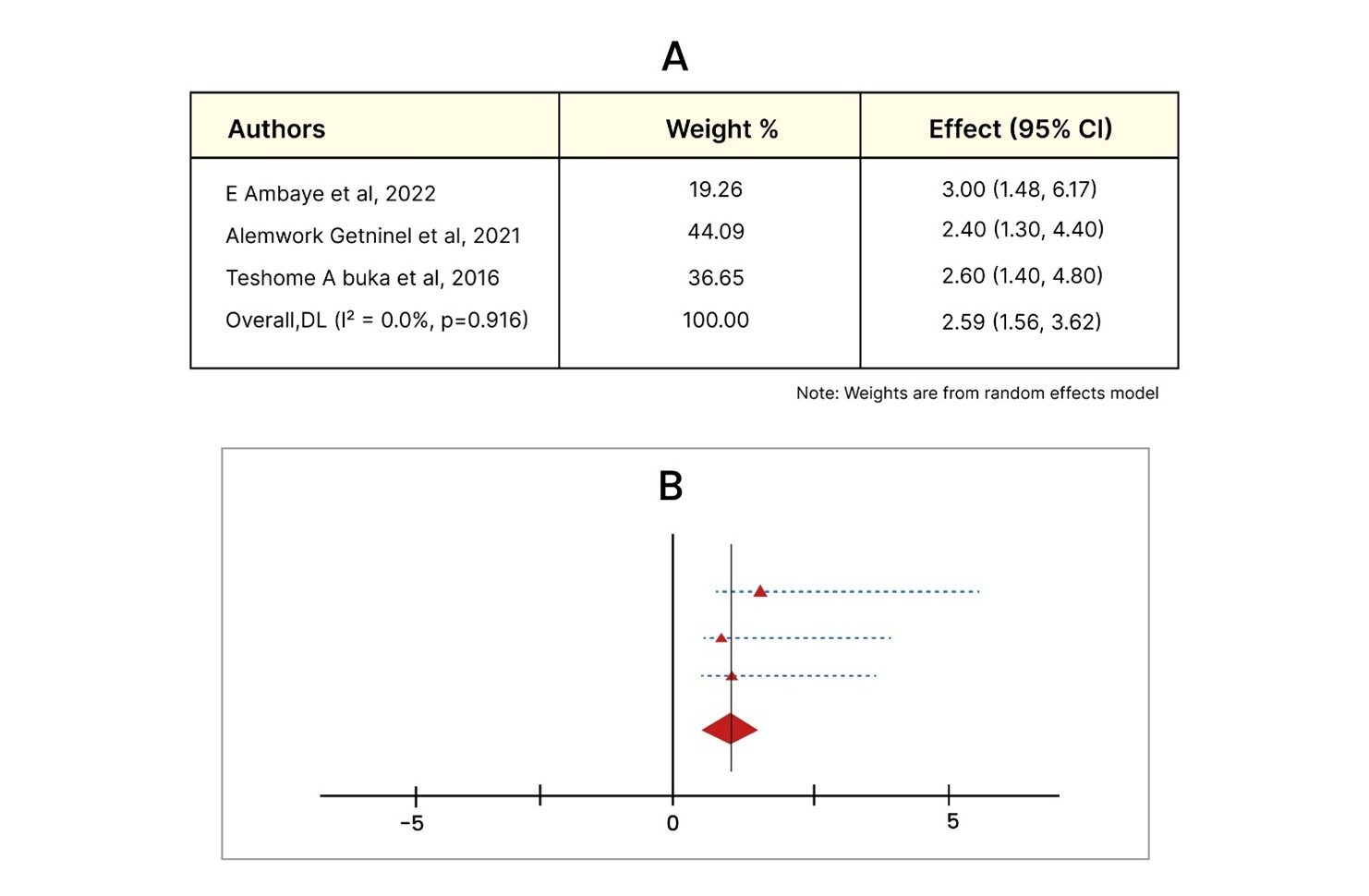
Figure 10: Frost plot of pooled odds ratio shows an association between urban residence and timely initiation among pregnant women, 2024
Discussion
This systematic review and meta-analysis examined the pooled prevalence and factors associated with the timely initiation of ANC among pregnant women in Ethiopia. According to this study, the overall pooled prevalence of timely initiation of ANC among pregnant women was 37% (95% CI).[33-42] Although the factors that were associated with the timely initiation of ANC were knowledge of pregnant women on ANC, urban residence, secondary educational level and above, planned pregnancy, primigravida, advice on ANC, and pregnancy recognition with a urine test. The pooled prevalence of this study was consistent with studies in Asela (37%), Wolayita Sodo (39%), Amhara region (40%), Gondar (35%), Cameroon, demographic health survey conducted in sub-Saharan Africa systematic review in 19 African countries (37%) and south Asia.[41-52] This might be due to data taken from the same study population, and sometimes the study population shares common associated factors. But the prevalence of timely initiation of ANC was lower when compared to the study conducted in Bule Hora, Ethiopia (57%), Fantale Oromia (65.9%), and Addis Ababa (47%).[17,21,42] This is because the previous studies were conducted in urban areas among pregnant mothers. Another possible reason could be the data analysis method used in this study and previous studies.
Furthermore, the prevalence of this study was lower than that of the study in Afghanistan (66.9%), low-middle-income countries (49.9%), Sudi-Arabia (75%), and the United Kingdom (79.2%).[13,52-54] This is because of the social and economic differences, political factors, and lack of living standards in Ethiopia and those countries. Another possible reason might be the need to improve maternal and child healthcare services in those countries through community training. This is supported by research conducted on ANC improvement training in the community.[55] The prevalence of this meta-analysis was higher than the study conducted in Ambo Oromia (30.5%), the demographic health survey of Ethiopia (20%).[16,44] This might be a difference in the sample size used for the study. The previous study had only a single prevalence, but the pooled prevalence of different studies included people from different regions. It is also lower than the study conducted in Nigeria (24%), Uganda (17%), and Bangladesh (22.2%).[56,57] The variation might be due to differences in access to health care facilities in Ethiopia compared to those in other countries, differences in cultural practices and knowledge of ANC, and differences in the level of application of WHO recommendations.
We have found that the knowledge of pregnant women was a significant factor associated with the timely initiation of antenatal care. This is congruent with studies conducted in Ethiopia, Zambia, and Nigeria.[17,19,23,24,27,28,43,44,49,58,59] Having good knowledge about pregnancy has a positive association with the timely initiation of ANC.[60] This is because having good knowledge makes a mother understand the importance of antenatal care for herself and her unborn baby. When mothers are aware of the potential complications of pregnancy, they are more likely to seek care. Our study agrees with previous studies conducted in Ethiopia, Ghana, Uganda, Cameroon, and a systematic review in Africa.[16,19,26,28,50,51,61-63] This study revealed that pregnant women with secondary education and above were more likely to initiate ANC on time when compared to women who were not educated. Having a formal education helps women make decisions about their health and gives them better access to health care facilities.[14,62] The possible explanation for this is that educated women have a better understanding of the recommendation of timely initiation of antenatal care rather than delaying. Additionally, compared to uneducated women, educated women have better access to reading material and media that provide health-related knowledge to initiate antenatal care on time.
In line with earlier research, systematic review in Africa, Ethiopia , Guinea, Ghana, our study also showed that women who planned their pregnancies were more likely to start prenatal care on time than those who didn’t.[17,19,27,38,44,49,62,64] This may be because women who have planned their pregnancies may receive assistance from their partners to prepare physically, psychologically, and emotionally. This allows them to make prompt contact with a healthcare practitioner to begin antenatal care. According to our research, women who resided in urban areas were twice as likely to start ANC on time as women who lived in rural areas. This is consistent with studies conducted in Ethiopia, Uganda, Zambia, Benin, and a systematic review in Africa.[44,51,66-68] Maybe because women tend to reside in urban regions closer to healthcare facilities than in rural ones. More women in urban areas than in rural ones have greater access to informative and instructional campaigns.
Different literature conducted elsewhere shows that primipara mothers were more likely to initiate ANC than multipara. This is because primigravida mothers are more likely to experience mild pregnancy disorders, pregnancy signs and symptoms, and complications, which prompts them to seek medical attention as soon as possible to begin prenatal care on time.[44,46,51] Our research also found that women with the highest wealth index were more likely than those with the lowest wealth index to start ANC on time. This is aligned with the research that was done. This was consistent with a study conducted in Ethiopia, Sub-Saharan Africa, Nigeria, and Pakistan.[14,38,65,66,69-71] This may be because the wealthiest women have better access to health information and education, are able to afford health insurance, and have a choice of healthcare providers and facilities. Furthermore, they can afford to travel to medical facilities, even those that are far away.
Additionally, our study shows that women who confirm their pregnancy by a urine test at a health facility are more likely to start antenatal care on time than women who confirm their pregnancy by signs, symptoms, and a pregnancy test at home. This agrees with results from prior research in Ethiopia, Nigeria, and South Africa.[72,73] This may be because starting antenatal care is made easier when a pregnancy is detected at a health facility, which tends to increase understanding, which could encourage them to prioritize their unborn child’s health as well as their own and seek care as soon as possible. Furthermore, if a pregnancy has been confirmed, there can be a suggestion to begin prenatal care. Finally, the results of our study showed that pregnant women who received guidance and support from their healthcare professionals had a higher likelihood of starting ANC on time than those who did not. This is consistent with research findings from Ethiopia, Madagascar, and Malawi.[38,45,49,65,74,75] This could be because learning more from medical professionals has raised awareness of the significance of prenatal care. Women who seek help from healthcare providers are also better satisfied in terms of health information and problem detection. This is supported by the study conducted on health education on antenatal care.[76]
Limitation: No PROSPERO registration is available for this study. Studies that follow lengthy periods of time are scarce, which could impact data analysis.
Conclusion
The evidence suggests that the timely initiation of antenatal care was relatively low. Timely prenatal care initiation was linked to anticipatory counseling knowledge, a secondary education or higher educational attainment, being a primigravida, living in an urban area, detecting pregnancy through a urine test at a medical facility, planning pregnancy, having a higher wealth index, and receiving guidance and recommendations from medical professionals. Regardless of those factors, regular monitoring and evaluation are needed in addition to health education and applying the new recommendations of the WHO 2016 guidelines practically by administrators, health care providers, policymakers, and other stakeholders.
References
- World Health Organization. Antenatal care coverage at least four visits (%). Global Health Observatory. Antenatal care coverage at least four visits (%)
- Bornstein J. Chapter 39. Benign Disorders of the Vulva & Vagina. In: DeCherney AH, Nathan L, Laufer N, Roman AS, eds. CURRENT Diagnosis & Treatment: Obstetrics & Gynecology. 11th ed. The McGraw-Hill Companies; 2013. Benign Disorders of the Vulva & Vagina
- Nwabueze CO, Okeke CC, Nwevo CO, et al. Assessing focused antenatal care awareness and utilization among pregnant women in Enugu State, Nigeria: A cross-sectional survey. Cureus. 2023;15(5):e38403. doi:10.7759/cureus.38403 PubMed | Crossref | Google Scholar
- Alkema L, Chou D, Hogan D, et al; United Nations Maternal Mortality Estimation Inter-Agency Group collaborators and technical advisory group. Global, regional, and national levels and trends in maternal mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the UN Maternal Mortality Estimation Inter-Agency Group. Lancet. 2016;387(10017):462-474. doi:10.1016/S0140-6736(15)00838-7
PubMed | Crossref | Google Scholar - World Health Organization. Antenatal care services goals and principles. 2016. Antenatal care services goals and principles
- Richard M. WHO recommendations on antenatal care for a positive pregnancy experience in Kenya. SSRN Electron J. 2019. doi:10.2139/ssrn.3449460 Crossref | Google Scholar
- Dash B. Maternal and Child Health Care. A Comprehensive Textbook of Community Health Nursing. 2017:282–282. Maternal and Child Health Care
- Dembelu M, Samuel A, Andarge K, Tamirat S, Kolcha M. Assessment of timely initiation of first ANC visit and associated factors among pregnant mothers in Wolayita Soddo public health facilities, Soddo Town, Wollayita Zone, SNNPR, Ethiopia. 2016:39-59. Assessment of timely initiation of first ANC visit and associated factors among pregnant mothers in Wolayita Soddo public health facilities, Soddo Town, Wollayita Zone, SNNPR, Ethiopia
- Lawn JE, Blencowe H, Waiswa P, et al. Stillbirths: rates, risk factors, and acceleration towards 2030. Lancet. 2016;387(10018):587-603. doi:10.1016/S0140-6736(15)00837-5 PubMed | Crossref | Google Scholar
- Arsenault C, Jordan K, Lee D, et al. Equity in antenatal care quality: an analysis of 91 national household surveys. Lancet Glob Health. 2018;6(11):e1186-1195. doi:10.1016/S2214-109X(18)30389-9 PubMed | Crossref | Google Scholar
- Moller A-B, Petzold M, Chou D, Say L. Early antenatal care visit: a systematic analysis of regional and global levels and trends of coverage from 1990 to 2013. Lancet Glob Health. 2017;5(10):e977-983. doi:10.1016/S2214-109X(17)30325-X PubMed | Crossref | Google Scholar
- Ayoola AB, Nettleman MD, Stommel M, Canady RB. Time of pregnancy recognition and prenatal care use: a population-based study in the United States. Birth. 2010;37(1):37-43. doi:10.1111/j.1523-536X.2009.00376.x
PubMed | Crossref | Google Scholar - Sarker BK, Rahman T, Rahman T, Rahman M. Factors associated with the timely initiation of antenatal care: findings from a cross-sectional study in Northern Bangladesh. BMJ Open. 2021;11(12):e052886. doi:10.1136/bmjopen-2021-052886 PubMed | Crossref | Google Scholar
- Alem ZZ, Yeshaw Y, Liyew AM, et al. Timely initiation of antenatal care and its associated factors among pregnant women in sub-Saharan Africa: A multicountry analysis of Demographic and Health Surveys. PLoS One. 2022;17(1):e0262411. doi:10.1371/journal.pone.0262411 PubMed | Crossref | Google Scholar
- Otundo R, Martin M. WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience in Kenya. SSRN. 2019. WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience in Kenya
- Woldeamanuel BT, Belachew TA. Timing of first antenatal care visits and number of items of antenatal care contents received and associated factors in Ethiopia: multilevel mixed effects analysis. Reprod Health. 2021;18(1):233. doi:10.1186/s12978-021-01275-9 PubMed | Crossref | Google Scholar
- Hailu S. Timely initiation of antenatal care and associated factors among pregnant women who attend antenatal care at public health facilities of Fentale district, Oromia region, Ethiopia. 2022. Timely initiation of antenatal care and associated factors among pregnant women who attend antenatal care at public health facilities of Fentale district, Oromia region, Ethiopia
- Ethiopian Mini Demographic and Health Survey. Ethiopia Mini Demographic and Health Survey 2019. 2021. Ethiopia Mini Demographic and Health Survey 2019
- Woldeamanuel BT, Belachew TA. Timing of first antenatal care visits and number of items of antenatal care contents received and associated factors in Ethiopia: multilevel mixed effects analysis. Reprod Health. 2021;18(1):233. doi:10.1186/s12978-021-01275-9 PubMed | Crossref | Google Scholar
- Edessa A, Dida N, Teferi E. Early initiation of antenatal care and its associated factors among antenatal care followers at public health facilities in Ambo town administration, Central Ethiopia. J Family Med Prim Care. 2023;12(1):67-75. doi:10.4103/jfmpc.jfmpc_725_22 PubMed | Crossref | Google Scholar
- Gudayu TW, Woldeyohannes SM, Abdo AA. Timing and factors associated with first antenatal care booking among pregnant mothers in Gondar Town; Northwest Ethiopia. BMC Pregnancy Childbirth. 2014;14:287. doi:10.1186/1471-2393-14-287 PubMed | Crossref | Google Scholar
- Alene A, Olayemi O, Berhane Y. Timing and factors associated with early antenatal visits among pregnant women in West Gojjam, Northwest Ethiopia. Afr J Midwifery Womens Health. 2021;15:1-11. doi:10.12968/ajmw.2020.0023
Crossref | Google Scholar - Gulema H, Berhane Y. Timing of first antenatal care visit and its associated factors among pregnant women attending public health facilities in Addis Ababa, Ethiopia. Ethiop J Health Sci. 2017;27(2):139-146. doi:10.4314/ejhs.v27i2.6 PubMed | Crossref | Google Scholar
- Abebo T, Alemu A. Assessment of timing of first antenatal care booking and associated factors among pregnant women who attend antenatal care at health facilities in Dilla town, Gedeo Zone, Southern Nations, Nationalities, and Peoples Region, Ethiopia, 2014. J Preg Child Health. 2016;3(3):1000258. doi:10.4172/2376-127X.1000258 PubMed | Crossref | Google Scholar
- Shiferaw K, Mengistie B, Gobena T, Dheresa M, Seme A. Adequacy and timeliness of antenatal care visits among Ethiopian women: a community-based panel study. BMJ Open. 2021;11(12):e053357. doi:10.1136/bmjopen-2021-053357 PubMed | Crossref | Google Scholar
- Gebresilassie B, Belete T, Tilahun W, Berhane B, Gebresilassie S. Timing of first antenatal care attendance and associated factors among pregnant women in public health institutions of Axum Town, Tigray, Ethiopia, 2017: a mixed design study. BMC Pregnancy Childbirth. 2019;19:1-11. doi:10.1186/s12884-019-2362-4
PubMed | Crossref | Google Scholar - Redi T, Seid O, Bazie GW, Amsalu ET, Cherie N, Yalew M. Timely initiation of antenatal care and associated factors among pregnant women attending antenatal care in Southwest Ethiopia. PLoS One. 2022;17(8):e0273152. doi:10.1371/journal.pone.0273152 PubMed | Crossref | Google Scholar
- Tesfu AA, Aweke AM, Gela GB, Wudineh KG, Beyene FY. Factors associated with timely initiation of antenatal care among pregnant women in Bahir Dar City, Northwest Ethiopia: cross-sectional study. Nurs Open. 2022;9(2):1210-1217. doi:10.1002/nop2.1162 PubMed | Crossref | Google Scholar
- Ketema T, Gurara M, Tumebo T, et al. Timing of first antenatal care visit and associated factors among pregnant women attending antenatal clinics in Halaba Kulito governmental health institutions, 2015. J Womens Health Care. 2016;5:308. doi:10.4172/2167-0420.1000308 Crossref | Google Scholar
- WHO recommendation on antenatal care for a positive pregnancy experience: summary. Lancet. 2018;387(10017):1-10. WHO recommendation on antenatal care for a positive pregnancy experience: summary
- Dennis ML, Benova L, Abuya T, et al. Initiation and continuity of maternal healthcare: examining the role of vouchers and user-fee removal on maternal health service use in Kenya. Health Policy Plan. 2019;34(2):120-131. doi:10.1093/heapol/czz004 PubMed | Crossref | Google Scholar
- Gross K, Alba S, Glass TR, Schellenberg JA, Obrist B. Timing of antenatal care for adolescent and adult pregnant women in south-eastern Tanzania. BMC Pregnancy Childbirth. 2012;12:16. doi:10.1186/1471-2393-12-16
PubMed | Crossref | Google Scholar - Gidey G, Hailu B, Nigus K, et al. Timing of first focused antenatal care booking and associated factors among pregnant mothers who attend antenatal care in Central Zone, Tigray, Ethiopia. BMC Res Notes. 2017;10(1):608. doi:10.1186/s13104-017-2938-5 PubMed | Crossref | Google Scholar
- Wolde HF, Tsegaye AT, Sisay MM. Late initiation of antenatal care and associated factors among pregnant women in Addis Zemen Primary Hospital, South Gondar, Ethiopia. Reprod Health. 2019;16(1):73. doi:10.1186/s12978-019-0745-2 PubMed | Crossref | Google Scholar
- Dinagde DD, Marami SN, Feyisa GT, Degefa BD. About half of Ethiopian midwifery professionals reported being dissatisfied with their jobs: a systematic review and meta-analysis. Eur J Obstet Gynecol Reprod Biol X. 2023;21:100277. doi:10.1016/j.eurox.2023.100277 PubMed | Crossref | Google Scholar
- Moher D, Shamseer L, Clarke M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4(1):1. doi:10.1186/2046-4053-4-1 PubMed | Crossref | Google Scholar
- Forte AJ, Guliyeva G, McLeod H, et al. The impact of optimism on cancer-related and postsurgical cancer pain: a systematic review. J Pain Symptom Manage. 2022;63(2):e203-211. doi:10.1016/j.jpainsymman.2021.09.008
PubMed | Crossref | Google Scholar - Abate L, Suleman S, Chernet Adeko A. Timing of the first antenatal care visit and associated risk factors in rural parts of Ethiopia. Int J Appl Res Public Health Manag. 2022;7(1):1-10. doi:10.4018/IJARPHM.20220101.oa1
Crossref | Google Scholar - Fesseha G. Predictors of timing of first antenatal care booking at public health centers in Mekelle City, Northern Ethiopia. J Gynecol Obstet. 2015;3(3):55-63. doi:10.11648/j.jgo.20150303.13 Crossref | Google Scholar
- Abebe T, Letta S, Gebrehanna E, Feyera B. Timely booking and factors associated with first antenatal care attendance among pregnant women in public health centers, Addis Ababa. J Gynecol Obstet. 2017;1:21-28. Timely booking and factors associated with first antenatal care attendance among pregnant women in public health centers, Addis Ababa
- Megersa G. Factors Associated with Timely First Antenatal Care Booking among Pregnant Women Attending Antenatal Clinics in Asella Town Public Health Institutions, Arsi Zone Oromia Regional State, Ethiopia, 2017 [master’s thesis]. Addis Ababa University; 2017. Factors Associated with Timely First Antenatal Care Booking among Pregnant Women Attending Antenatal Clinics in Asella Town Public Health Institutions, Arsi Zone Oromia Regional State, Ethiopia, 2017
- Tufa G, Tsegaye R, Seyoum D. Factors associated with timely antenatal care booking among pregnant women in remote area of Bule Hora District, Southern Ethiopia. Int J Womens Health. 2020;12:657-666. doi:10.2147/IJWH.S255009 PubMed | Crossref | Google Scholar
- Fetene W, Mekonnen A, Shiferaw Z, Genet A, Haile S. Timely initiation of first antenatal care visit and associated factors among pregnant women in the Amhara Region, North-west Ethiopia: a comparative cross-sectional study. Pan Afr Med J. 2023;44:51. doi:10.11604/pamj.2023.44.51.33997 PubMed | Crossref | Google Scholar
- Ambaye E, Regasa ZW, Hailiye G. Early initiation of antenatal care and its associated factors among pregnant women attending antenatal care at public health centres in Bahir Dar Zuria zone, Northwest Ethiopia, 2021: a cross-sectional study. BMJ Open. 2023;13(1):67-75. doi:10.1136/bmjopen-2022-068528 PubMed | Crossref | Google Scholar
- Gudayu TW, Woldeyohannes SM, Abdo AA. Timing and factors associated with first antenatal care booking among pregnant mothers in Gondar Town, North West Ethiopia. BMC Pregnancy Childbirth. 2014;14:287. doi:10.1186/1471-2393-14-287 PubMed | Crossref | Google Scholar
- Redi T, Seid O, Bazie GW, et al. Timely initiation of antenatal care and associated factors among pregnant women attending antenatal care in Southwest Ethiopia. PLoS One. 2022;17(8):e0273152. doi:10.1371/journal.pone.0273152 PubMed | Crossref | Google Scholar
- Higgins JPT, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539-1558. doi:10.1002/sim.1186 PubMed | Crossref | Google Scholar
- Sterne JA, Egger M. Funnel plots for detecting bias in meta-analysis: guidelines on choice of axis. J Clin Epidemiol. 2001;54(10):1046-1055. doi:10.1016/s0895-4356(01)00377-8 PubMed | Crossref | Google Scholar
- Fetene W, Mekonnen A, Shiferaw Z, Genet A, Haile S. Timely initiation of first antenatal care visit and associated factors among pregnant women in the Amhara Region, North-west Ethiopia: a comparative cross-sectional study. Pan Afr Med J. 2023;44:51. doi:10.11604/pamj.2023.44.51.33997 PubMed | Crossref | Google Scholar
- Ahinkorah BO, Seidu AA, Budu E, et al. Factors associated with the number and timing of antenatal care visits among married women in Cameroon: evidence from the 2018 Cameroon Demographic and Health Survey. J Biosoc Sci. 2022;54(2):322-332. doi:10.1017/S0021932021000079 PubMed | Crossref | Google Scholar
- Abdo R, Demelash M, Seid AM, Mussema A. First trimester antenatal care contact in Africa: a systematic review and meta-analysis of prevalence and contributing factors. BMC Pregnancy Childbirth. 2023;23(1):742. doi:10.1186/s12884-023-06034-1 PubMed | Crossref | Google Scholar
- Zangmo K, Jigme D, Wangchuck O, et al. An assessment of antenatal care received by Bhutanese women: A retrospective review of maternal and child health handbooks. J Asian Midwives. 2021;8(2):7-16. An assessment of antenatal care received by Bhutanese women: A retrospective review of maternal and child health handbooks
- Zeleke AM, Gonete YA, Tassew WC, Ferede YA. Utilization of eight or more ANC contacts and determinants among healthcare providers in Ethiopia: systematic review and meta-analysis. AJOG Glob Rep. 2024;100418. doi:10.1016/j.xagr.2024.100418 PubMed | Crossref | Google Scholar
- Jiwani SS, Amouzou-Aguirre A, Carvajal L, et al. Timing and number of antenatal care contacts in low and middle-income countries: Analysis in the Countdown to 2030 priority countries. J Glob Health. 2020;10(1):010502. doi:10.7189/jogh.10.010502 PubMed | Crossref | Google Scholar
- Liabsuetrakul T, Oumudee N, Armeeroh M, et al. Improvement of early antenatal care initiation: The effects of training local health volunteers in the community. Health Serv Res Manag Epidemiol. 2018;5:2333392818761483. doi:10.1177/2333392818761483 PubMed | Crossref | Google Scholar
- Bbaale E. Factors influencing timing and frequency of antenatal care in Uganda. Australas Med J. 2011;4(8):431-438. doi:10.4066/AMJ.2011.729 PubMed | Crossref | Google Scholar
- Al Kibria GM, Crispen R. Disparities, distribution, and determinants in appropriate timely initiation, number, and quality of antenatal care in Bangladesh: evidence from Demographic and Health Survey 2017-18. PLoS Glob Public Health. 2023;3(8):e0002325. doi:10.1371/journal.pgph.000232 PubMed | Crossref | Google Scholar
- Sinyange N, Sitali L, Jacobs C, Musonda P, Michelo C. Factors associated with late antenatal care booking: population-based observations from the 2007 Zambia demographic and health survey. Pan Afr Med J. 2016;25:109. doi:10.11604/pamj.2016.25.109.6873 PubMed | Crossref | Google Scholar
- Oladokun A, Oladokun RE, Morhason-Bello I, Bello AF, Adedokun B. Proximate predictors of early antenatal registration among Nigerian pregnant women. Ann Afr Med. 2010;9(4):222-225. doi:10.4103/1596-3519.70959
PubMed | Crossref | Google Scholar - Bashir S, Ansari AH, Sultana A. Knowledge, attitude, and practice on antenatal care among pregnant women and its association with sociodemographic factors: a hospital-based study. J Patient Exp. 2023;10:23743735231183578. doi:10.1177/23743735231183578 PubMed | Crossref | Google Scholar
- Abebe GF, Alie MS, Girma D, Mankelkl G, Berchedi AA, Negesse Y. Determinants of early initiation of first antenatal care visit in Ethiopia based on the 2019 Ethiopia mini-demographic and health survey: a multilevel analysis. PLoS One. 2023;18(3):e0281038. doi:10.1371/journal.pone.0281038 PubMed | Crossref | Google Scholar
- Manyeh AK, Amu A, Williams J, Gyapong M. Factors associated with the timing of antenatal clinic attendance among first-time mothers in rural southern Ghana. BMC Pregnancy Childbirth. 2020;20(1):47. doi:10.1186/s12884-020-2738-0 PubMed | Crossref | Google Scholar
- Kisuule I, Kaye DK, Najjuka F, et al. Timing and reasons for coming late for the first antenatal care visit by pregnant women at Mulago hospital, Kampala Uganda. BMC Pregnancy Childbirth. 2013;13:121. doi:10.1186/1471-2393-13-121 PubMed | Crossref | Google Scholar
- Andrew EVW, Pell C, Angwin A, et al. Factors affecting attendance at and timing of formal antenatal care: results from a qualitative study in Madang, Papua New Guinea. PLoS One. 2014;9(5):e93025. doi:10.1371/journal.pone.0093025 PubMed | Crossref | Google Scholar
- Gudissa T, Gmariam A, Workneh D. Time of antenatal care booking and associated factors among pregnant women attending Ambo Town health facilities, Central Ethiopia. J Public Health Dev. 2015;3:103-106. Time of antenatal care booking and associated factors among pregnant women attending Ambo Town health facilities, Central Ethiopia
- Agha S, Tappis H. The timing of antenatal care initiation and the content of care in Sindh, Pakistan. BMC Pregnancy Childbirth. 2016;16(1):190. doi:10.1186/s12884-016-0979-8 PubMed | Crossref | Google Scholar
- Banda I, Michelo C, Hazemba A. Factors associated with late antenatal care attendance in selected rural and urban communities of the Copperbelt Province of Zambia. Med J Zambia. 2012;39:29-36. Factors associated with late antenatal care attendance in selected rural and urban communities of the Copperbelt Province of Zambia
- Ekholuenetale M, Nzoputam CI, Barrow A, Onikan A. Women’s enlightenment and early antenatal care initiation are determining factors for the use of eight or more antenatal visits in Benin: further analysis of the Demographic and Health Survey. J Egypt Public Health Assoc. 2020;95(1):13. doi:10.1186/s42506-020-00041-2
PubMed | Crossref | Google Scholar - Kitaw TA, Haile RN. Time to first childbirth and its predictors among reproductive-age women in Ethiopia: survival analysis of recent evidence from the EDHS 2019. Front Reprod Health. 2023;5:1165204. doi:10.3389/frph.2023.1165204 PubMed | Crossref | Google Scholar
- Belay DG, Alemu MB, Aragaw FM, Asratie MH. Time to initiation of antenatal care visit and its predictors among reproductive age women in Ethiopia: Gompertz inverse Gaussian shared frailty model. Front Glob Womens Health. 2023;4:917895. doi:10.3389/fgwh.2023.917895 PubMed | Crossref | Google Scholar
- Aliyu AA, Dahiru T. Predictors of delayed antenatal care (ANC) visits in Nigeria: secondary analysis of the 2013 Nigeria Demographic and Health Survey (NDHS). Pan Afr Med J. 2017;26:124. doi:10.11604/pamj.2017.26.124.9861
PubMed | Crossref | Google Scholar - Lamina M. The effect of urine pregnancy testing on timing of accessing antenatal care and abortion services in Western Nigeria. Open J Obstet Gynecol. 2013;3:486-492. doi:10.4236/ojog.2013.36089 Crossref | Google Scholar
- Morroni C, Moodley J. The role of urine pregnancy testing in facilitating access to antenatal care and abortion services in South Africa: a cross-sectional study. BMC Pregnancy Childbirth. 2006;6:26. doi:10.1186/1471-2393-6-26 PubMed | Crossref | Google Scholar
- Comfort AB, Juras RC, Bradley SE, et al. Do home pregnancy tests bring women to community health workers for antenatal care counselling? A randomized controlled trial in Madagascar. Health Policy Plan. 2019;34(8):566-573. doi:10.1093/heapol/czz080 PubMed | Crossref | Google Scholar
- Pell C, Meñaca A, Were F, et al. Factors affecting antenatal care attendance: results from qualitative studies in Ghana, Kenya, and Malawi. PLoS One. 2013;8(1):e53747. doi:10.1371/journal.pone.0053747
PubMed | Crossref | Google Scholar - Al-Ateeq MA, Al-Rusaiess AA. Health education during antenatal care: the need for more. Int J Womens Health. 2015;7:239-242. doi:10.2147/IJWH.S75164 PubMed | Crossref | Google Scholar
Acknowledgments
Not reported
Funding
Not reported
Author Information
Corresponding Author:
Shambel Negese Marami
Department of Midwifery
College of Health Science, Mattu University, Ethiopia
Email: [email protected]
Co-Authors:
Gemeda Wakgari Kitil, Shimalis Tadese Abebe, Gizu Tola Feyisa, Dagne Deresa Dinagde
Department of Midwifery
College of Health Science, Mattu University, Ethiopia
Authors Contributions
All authors contributed to the conceptualization, investigation, and data curation by acquiring and critically reviewing the selected articles. They were collectively involved in the writing – original draft preparation, and writing – review & editing to refine the manuscript. Additionally, all authors participated in the supervision of the work, ensuring accuracy and completeness. The final manuscript was approved by all named authors for submission to the journal.
Ethical Approval
Consent and ethical approval did not apply to this study. Since it is a meta-analysis and systematic review.
Conflict of Interest Statement
Not reported
Guarantor
None
DOI
Cite this Article
Shambel NM, Gemeda WK, Shimalis TA, et al. Systematic Literature Review and Meta-Analysis of Timely Initiation of Antenatal Care Among Pregnant Women in Ethiopia: Prevalence and Associated Factors. medtigo J Emerg Med. 2024;1(1):e3092116. doi:10.63096/medtigo3092116 Crossref













