






 Author Affiliations
Author Affiliations
Abstract
Background: Diabetes mellitus is a long-term disease that needs intensive self-management measures that include medication adherence, checking of blood sugar, calorie intake, physical exercise, and care of the feet. It has been acknowledged that social support provided by family, peers, and healthcare providers is one of the factors that can help to strengthen self-care behavior and positively affect diabetes outcomes.
Aim: The study aimed to assess the role of social support in overcoming challenges in diabetes self-care management among patients attending a tertiary care hospital in Swat.
Methodology: The design used was a descriptive cross-sectional design. The sample consisted of 100 adults with Type 1 or Type 2 diabetes recruited in the study using convenience sampling from the tertiary care hospital. The structured questionnaire that was used to gather data included demographic characteristics, self-care practices, and social support measures. The level of correlation between social support and self-care behaviors was determined using descriptive statistics, frequencies, percentages, and Pearson’s coefficient of correlation.
Results: Results showed that 60% of the participants have moderate social support, whereas 25 percent have high social support. Most of the participants had moderate self-care practices with blood glucose monitoring and medication adherence, having greater adherence levels than physical activity and foot care. There were also significant positive relationships between overall social support and self-care behaviors (r = 0.60, p < 0.001), and emotional support demonstrated the best correlation.
Conclusion: Social support is critical in promoting self-management with diabetes. It is suggested that interventions based on emotional, informational, and practical support of family, peers, and healthcare providers can enhance adherence and health outcomes.
Keywords
Diabetes, Social support, Self-care, Emotional support, Practical support, Informational support, Chronic disease management.
Introduction
Social support is a need-based provision of emotional support, informational support, instrumental support, and appraisal support by family members, friends, peers, and medical workers to individuals who are struggling with a health issue. Diabetes self-management encompasses life activities performed by diabetic individuals to manage the level of blood glucose, which involves medication compliance, dietary compliance, exercise, blood glucose monitoring, and foot care. Chronic illness defines long-term health conditions, whereby management and changes in lifestyle are necessary. Glycemic control refers to the process of keeping the level of blood glucose within the recommended concentrations to avoid complications. Social support is a psychosocial resource that has the potential of modifying health behaviors, coping capacity, and disease outcomes among individuals with diabetes.[1,2]
Diabetes mellitus is one of the most common chronic conditions in the world. It has been estimated by the International Diabetes Federation that over 530 million adults in the world have diabetes, and the number is projected to be more than 640 million by the year 2030.[2] Urbanization, sedentary lifestyles, food changes, and hereditary vulnerability contribute a lot to the prevalence of type 2 diabetes in South Asia.[3] Pakistan is one of the countries with the highest prevalence of diabetes, where one in four adults in some areas is affected by this disease.[4] Ineffective management of glycemic control has continued to be a cause of microvascular and macrovascular complications, elevated hospitalization, disability, and early mortality.[5]
Self-care behaviors are important in the management of diabetes as they require patients to engage in consistent self-care practices. Self-care involves knowledge, motivation, the ability to deal with problems, and long-term change of lifestyle. Financial constraints, ignorance, mental turmoil, and limited access to healthcare make many people unable to maintain a healthy diet, physical activity, and medication compliance, and glucose monitoring.[6] Poor self-care habits have been closely linked with the unmanaged presence of glucose levels in the bloodstream and worsening of complication factors like nephropathy, neuropathy, retinopathy, and cardiovascular disease.[7]
Diabetes is often complicated by psychological issues. Depression, nervousness, and distress related to diabetes have adverse effects on adherence to treatment regimens and self-management behavior.[8] Emotional burnout and helplessness can lower incentives to follow rigid lifestyle patterns. Coping capacity is also weakened by social isolation and the absence of supportive relationships. Patients who lack good family or community support show worse metabolic results when compared to those with good interpersonal networks.[9]
Social support plays an important role in the management of chronic diseases. Emotional support increases self-confidence and strength. Adherence is enhanced by the help of instrumental support, e.g., medication reminders, meal preparation, and clinic visits. Healthcare providers provide informational support that enhances knowledge and self-efficacy. Research has shown that patients who receive regular family engagement as well as peer support have improved glycemic control and a reduced level of HbA1c.[10] Favorable settings enable better behavioral choices and long-term lifestyle modifications.
The availability and effectiveness of social support are determined by cultural and socioeconomic contexts. Family participation in health decision-making is the key aspect in collectivist societies. Poverty, a shift to migration, and evolving family structures could restrict the old support system. The poor health literacy and stigma associated with chronic disease can lessen family open communication.[11] Peer groups and structured diabetes education programs have demonstrated favorable results in terms of increasing coping mechanisms and self-care adherence.[12]
The health care systems of low and middle-income countries have resource shortages that limit individual guidance and follow-up. Informal networks are a source of practical and emotional support to patients. The reinforcement of social support systems can provide another, more cost-effective solution, which is to improve self-care in diabetes and avoid complications. The research on social support as a coping resource in managing diabetes offers the researcher evidence in formulating patient-based interventions to deal with biomedical and psychosocial aspects of chronic illness.[13]
Methodology
This was done using a quantitative descriptive cross-sectional study design that investigated social support as a means of overcoming barriers in self-management of diabetes. The research was conducted in Saidu Group of Teaching Hospital (SGTH), which is a teaching hospital of tertiary care that offers specialization in offering services to patients with Type 1 and Type 2 diabetes. The study setting was chosen to be the outpatient diabetes clinics since they offer frequent follow-ups, education, and counseling services, within which the patients communicate with their healthcare providers and their family members about the management of the disease. The population of the study was the adult diabetic patients visiting the outpatient clinics with a diagnosis of diabetes for at least six months and participating in self-care practices, including medication taking, self-monitoring, food management, and exercise. One hundred subjects were recruited. In the study, the OpenEpi sample size calculator was used to compute the sample size with a 95% degree of confidence, 5% margin of error, and an estimated population of 250 diabetic patients. The eligible and consenting participants were recruited by utilizing a convenience sampling method. Inclusion criteria: Adults diagnosed with diabetes who engage in self-care activities and receive social support from family, peers, or healthcare providers.
Exclusion criteria: Individuals without a confirmed diabetes diagnosis or those with severe cognitive/psychiatric conditions that impair self-care participation.
Data collection procedure: Data collection was done with the ethical approval of the Institutional Review Board of SGTH. Hospital administration was given official consent. The diabetes clinics were used to approach eligible patients and give them comprehensive details about the purpose and processes of the study. Each participant signed an informed consent form written before being enrolled. A structured questionnaire with four parts, including socio-demographic information, self-management practices, perceived barriers to self-management, and the degree of social support (emotional, informational, and instrumental) were used to collect the data. The questionnaires were self-administered or were assisted by interviewers where required. Immediately, completed forms were scanned to determine their completeness. Anonymity and confidentiality were ensured.
Data analysis procedure: The data were coded and entered into the statistical package for the social sciences (SPSS) version 25 to be analyzed. Demographic characteristics, social support levels, and self-care behaviors were summarized with the help of descriptive statistics, such as frequencies, percentages, means, and standard deviations. The inferential statistics were used to investigate the relationships between social support and self-care practices of diabetes. Statistical relationships were established by means of chi-square tests and the Pearson correlation coefficient. Any p-value of less than 0.05 was deemed to be statistically significant.
Results
Demographic characteristics of participants: A total of 100 participants with Type 1 or Type 2 diabetes who were on an outpatient diabetes clinic at SGTH were used in the study, and the demographic details of the study participants are given in Table 1. Most of the respondents were in the 31-45 age group (40%), 46-60 years (35%), and 18-30 years (25%). Women were slightly more in the sample, consisting of 55% of the whole. Concerning diabetes, 42 percent of respondents were aged 510 years, 38 percent were less than five years, and 20 percent were more than 10 years. The levels of education were also mixed, with 45 percent of them having a graduate degree or higher, 35 percent possessing a diploma or intermediate level education, and 20 percent possessing a primary or secondary education. Fifty percent of those under study were working, three out of five were not, and the remaining 20 percent were retired.
| Variables | Categories | Frequency (n) | Percentage (%) |
| Age (years) | 18–30 | 25 | 25 |
| 31–45 | 40 | 40 | |
| 46–60 | 35 | 35 | |
| Gender | Male | 45 | 45 |
| Female | 55 | 55 | |
| Duration of diabetes | < 5 years | 38 | 38 |
| 5–10 years | 42 | 42 | |
| >10 years | 20 | 20 | |
| Education level | Primary/Secondary | 20 | 20 |
| Diploma/Intermediate | 35 | 35 | |
| Graduate or above | 45 | 45 | |
| Occupation | Employed | 50 | 50 |
| Unemployed | 30 | 30 | |
| Retired | 20 | 20 |
Table 1: Demographic characteristics of participants
Table 2 indicates the levels of social support that are reported by the participants. Comprehensively, 60 percent of the respondents stated that their social support was moderate, 25 percent stated that their social support was high, and 15 percent stated that their social support was low. The most reported support was emotional support moderate (50%), then informational support (55%), and practical support (45%). The results indicate that although the majority of participants were given some level of social support, there is still inconsistency in the nature and quality of support that was given.
| Type of support | Low | Moderate | High | Total (%) |
| Emotional support | 20 | 50 | 30 | 100 |
| Informational support | 25 | 55 | 20 | 100 |
| Practical support | 30 | 45 | 25 | 100 |
| Overall social support | 15 | 60 | 25 | 100 |
Table 2: Levels of social support reported by participants
Table 3 sums up the self-care practices of participants. Virtually, 60% of all respondents had moderate adherence to recommended self-care practices, 20% of them were good adherents, and 20 percent poor adherents. 30% of the participants were able to perform blood glucose monitoring sufficiently, and medication adherence was greater, with 25% of the participants demonstrating good behaviors. There was concern regarding diet control and foot care, where just 20% and 15 percent of the respondents were practicing well, respectively. The least followed practice was physical activity, with 35% indicating that they were poor at this. These results also suggest that there are lapses in the regular adoption of the key self-care behavior of diabetes.
| Self-care practice | Poor | Moderate | Good | Total (%) |
| Blood glucose monitoring | 20 | 50 | 30 | 100 |
| Medication adherence | 15 | 60 | 25 | 100 |
| Diet control | 25 | 55 | 20 | 100 |
| Physical activity | 35 | 50 | 15 | 100 |
| Foot care | 30 | 55 | 15 | 100 |
| Overall self-care score | 20 | 60 | 20 | 100 |
Table 3: Self-care practices among participants
The relationship between social support and self-care practices is presented in Table 4. Pearson correlation analysis revealed a significant positive relationship between overall social support and self-care practices (r = 0.60, p < 0.001). Emotional support demonstrated the strongest correlation with self-care (r = 0.62, p < 0.001), followed by informational support (r = 0.55, p < 0.001) and practical support (r = 0.48, p = 0.002). These findings indicate that higher levels of social support are associated with better adherence to self-care behaviors among diabetic patients, emphasizing the importance of supportive networks in promoting effective disease management.
| Variables | r-value | p-value |
| Emotional support & self-care | 0.62 | <0.001 |
| Informational support & self-care | 0.55 | <0.001 |
| Practical support & self-care | 0.48 | 0.002 |
| Overall social support & self-care | 0.60 | <0.001 |
Table 4: Relationship between social support and self-care practices (Pearson’s correlation)
Table 5 underlines the problems that participants had to face when keeping up with diabetes self-management. 30% of the participants cited the lack of family support as a major barrier. Lack of knowledge on management of diseases was encountered by 25% of the participants, and lack of finances was experienced by 20%. The prevalence of emotional stress or low motivation was marked by 15%, and hardship in reaching healthcare services was marked by 10%. These results imply that individual and social influences are the causes of difficulties in the effective management of self-care, and specific solutions to these limitations are required.
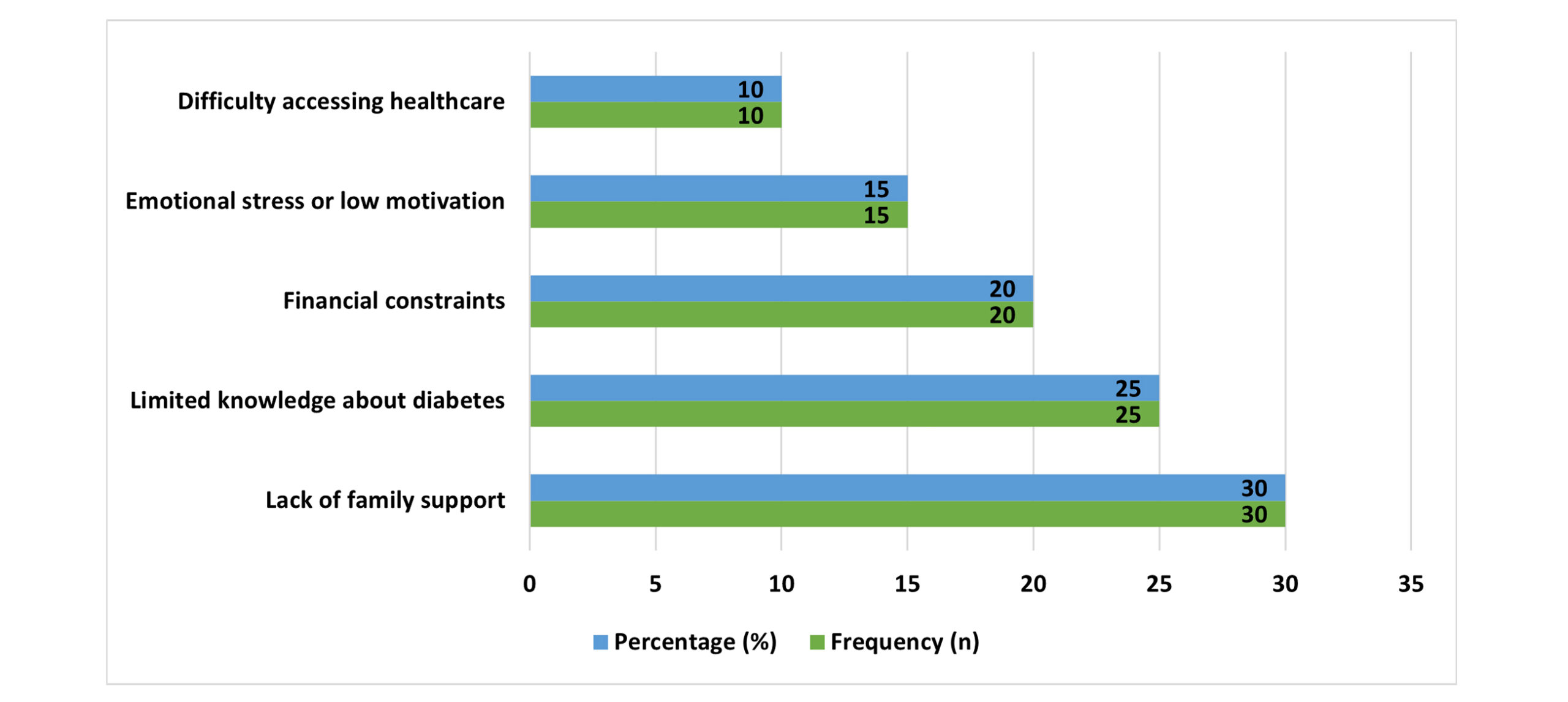
Figure 1: Challenges in diabetes self-care reported by participants
Discussion
This paper has found that social support is a crucial factor in ensuring proper self-care management of diabetes. The respondents with greater emotional, informational, and practical support levels showed considerably more effective compliance with the blood glucose monitoring, medication, dietary regulation, physical activity, and foot care behavior. The findings are in line with earlier studies that have reported that social support has a positive association with better self-management behaviors of diabetes.[14,15] Emotional support and physical help were found to boost the confidence and desire to maintain behavioral change in patients in the long term, supporting the significance of interpersonal contacts in chronic disease management.
Emotional support was found to be the most powerful predictor of self-care activities adherence. Those whose family members or peers provided them with reassurance, empathy, and inspiration experienced less difficulty in upholding recommended practices. The same has been observed in previous research studies that established that emotional support alleviates stress, increases coping skills, and leads to continuous practice of diabetes care routines.[3] In contrast, people who had less emotional support indicated that they had more challenges associated with self-care compliance, consistent with the findings that social isolation adversely impacts the outcomes of self-management of chronic diseases.[16] These findings indicate that the implementation of emotional support methods in patient-centered diabetes care models is significant.
There was a moderate relationship between informational support and the improvement of self-care practices. The adherence levels were higher among the participants who were structured on the matters of diet, exercise, and medication management. The latter is backed by the studies that have highlighted the importance of ongoing patient education and instructions in improving self-management outcomes of diabetes.[17] Nonetheless, a reduced percentage of respondents mentioned that they were provided with sufficient informational support, which implies the flaws in the provision of education in resource-constrained healthcare facilities. This is contrary to evidence of high-income countries, where structured programs of diabetes education are more commonly used.[18]
The self-care behaviors were also positively related to practical support, such as the need to take medication and do daily activities. Individuals who received practical assistance could more effectively execute tasks of complexity, like glucose monitoring and meal planning. Other studies of the past also emphasize the importance of instrumental support in enhancing compliance with treatment plans.[19] Nevertheless, practical support was less commonly reported than emotional support, which implies the necessity of organization-based family-focused interventions. Financial limitation, lack of knowledge, emotional stress, and lack of family support were some of the barriers identified by the participants. Similar results have been confirmed in studies that found socioeconomic and psychosocial determinants as obstacles to effective self-management of diabetes.[20] In the resource-scarce environment, where access to healthcare services and education is limited, these problems are only increased.[21]
The positive correlations among social support and self-care behaviors are in line with the social cognitive theory that highlights the effects of environmental and interpersonal factors on health behaviors.[22] Stronger family, peer, and community participation interventions can thus improve long-term adherence and self-efficacy. In general, the results prove that emotional, informational, and practical support play a significant role in overcoming the difficulties in managing self-care in diabetes. It is advised to incorporate social support mechanisms in routine diabetes care in order to enhance long-term health outcomes.
Recommendations:
- Caregivers and family members should be actively included in diabetes education programs by healthcare providers to increase the emotional and practical support of patients.
- Effective self-care requires guidance, peer experience, and motivation, which can be enhanced to be available in structured groups of peers in hospitals and community centers.
- Educational interventions ought to be centered on feasible and culturally focused strategies so that the patients are aware of medication management, dietary, exercise, and observation needs.
- The policy makers and hospital administrators ought to look at the programs that offer financial, educational, and emotional assistance to the patients with few support networks.
- New studies are needed on the longitudinal impacts of social support on self-care diabetes results and the interventions adapted to cultural and socioeconomic environments.
- They can introduce community-based interventions and telehealth programs to offer patients facing accessibility barriers with their continuous informational and practical support.
Conclusion
The research concluded that social support is an important aspect in the process of achieving effective diabetes self-care management. Emotional, informational, and practical support provided to the participants in greater amounts also led to improved self-care practices such as blood glucose monitoring, medication adherence, dietary control, physical activity, and foot care. The absence of support, low level of knowledge, low budget, and emotional stress were found to be the key obstacles to regular self-care. The results highlight that social support enhances self-efficacy, motivation, and confidence in handling diabetes, hence improving the overall health outcomes. Family, peers, and community support should be integrated into the diabetes care programs because they are the key to long-term adherence and minimization of complications.
References
- Hasan AA, Ismail A, Noor H. The Influence of Social Support on Self-Care Behavior among T2DM Patients. SAGE Open Nurs. 2024;10:23779608231219137. doi:10.1177/23779608231219137
PubMed | Crossref | Google Scholar - Al-Dwaikat T, Ali AM, Khatatbeh H. Self-Management Social Support in Type 2 Diabetes Mellitus: A Concept Analysis. Nursing Forum. 2023;2023:1-9. doi:10.1155/2023/1753982
Crossref | Google Scholar - Chen WJ, Lin LY. The Impact of Diabetes Self-Care, Healthy Lifestyle, Social Support, and Demographic Variables on Outcomes HbA1c in Patients With Type 2 Diabetes. Clin Med Insights Endocrinol Diabetes. 2025;18:11795514251331907. doi:10.1177/11795514251331907
PubMed | Crossref | Google Scholar - Da Moura Semedo C, Bath PA, Zhang Z. Social Support in a Diabetes Online Community: Mixed Methods Content Analysis. JMIR Diabetes. 2023;8:e41320. doi:10.2196/41320
PubMed | Crossref | Google Scholar - Busebaia TJA, Thompson J, Fairbrother H, Ali P. The role of family in supporting adherence to diabetes self-care management practices: An umbrella review. J Adv Nurs. 2023;79(10):3652-3677. doi:10.1111/jan.15689
PubMed | Crossref | Google Scholar - Hazime D, Burner E. Social support via Internet communication technology for diabetes self-management: a scoping review. Mhealth. 2024;10:18. doi:10.21037/mhealth-23-34
PubMed | Crossref | Google Scholar - Dinh TTH, Bonner A. Exploring the relationships between health literacy, social support, self-efficacy and self-management in adults with multiple chronic diseases. BMC Health Serv Res. 2023;23(1):923. doi:10.1186/s12913-023-09907-5
PubMed | Crossref | Google Scholar - Wang X, Zhang F, Ge Y, Ding Y, Liu T. The associations between social support, self-regulatory fatigue, and health-promoting behaviors among people with type 2 diabetes mellitus: a cross-sectional survey. Front Public Health. 2023;11:1281065. doi:10.3389/fpubh.2023.1281065
PubMed | Crossref | Google Scholar - Wong SKW, Soon W, Griva K, Smith HE. Identifying barriers and facilitators to self care in young adults with type 2 diabetes. Diabet Med. 2024;41(4):e15229. doi:10.1111/dme.15229
PubMed | Crossref | Google Scholar - Gray KE, Silvestrini M, Ma EW, Nelson KM, Bastian LA, Voils CI. Gender differences in social support for diabetes self-management: A qualitative study among veterans. Patient Educ Couns. 2023;107:107578. doi:10.1016/j.pec.2022.107578
PubMed | Crossref | Google Scholar - Zhang Q, Sun J, Bian H, et al. The relationship between hope level and self-management behaviors in Chinese patients with type 2 diabetes mellitus: a chain-mediated role of social support and disease perception. BMC Psychol. 2024;12(1):446. doi:10.1186/s40359-024-01939-8
PubMed | Crossref | Google Scholar - Saltar L, Sahar J, Rekawati E. Self-care behavior of type 2 diabetes patients with symptoms of peripheral neuropathy during the COVID-19 pandemic: a qualitative study. Int J Curr Sci Res Rev. 2023;6(2). doi:10.47191/ijcsrr/V6-i2-36
Crossref | Google Scholar - Hinds J, Greaves N, Harewood H. Diabetes self-management and social support during the COVID-19 pandemic: Perspectives of older adults living in Barbados. Dialogues Health. 2023;2:100111. doi:10.1016/j.dialog.2023.100111
PubMed | Crossref | Google Scholar - Hussain S, Dioso RPIII. Quality of Life in Patients with Permanent Colostomy: A Cross-Sectional Study at the Tertiary Care Hospital in Swat. medtigo J Med. 2025;3(2):e30623218. doi:10.63096/medtigo30623218
Crossref | Google Scholar - Tusubira AK, Nalwadda CK, Akiteng AR, et al. Social Support for Self-Care: Patient Strategies for Managing Diabetes and Hypertension in Rural Uganda. Ann Glob Health. 2021;87(1):86. doi:10.5334/aogh.3308
PubMed | Crossref | Google Scholar - Zhao F, Suhonen R, Katajisto J, Leino-Kilpi H. Factors associated with subsequent diabetes-related self-care activities: The role of social support and optimism. Nurs Open. 2019;7(1):195-205. doi:10.1002/nop2.379
PubMed | Crossref | Google Scholar - Sarpooshi D, Mahdizadeh M, Jaferi A, Robatsarpooshi H, Haddadi M, Peyman N. The relationship between social support and self-care behavior in patients with diabetes mellitus. Fam Med Prim Care Rev. 2021;23:227-231. doi:10.5114/fmpcr.2021.105932
Crossref | Google Scholar - Arshi S, Kalhornia Golkar M, Ahadi H, Sedaghat M. The role of self-efficacy, hardiness, and coping strategies in predicting self-care behaviors in patients with type 2 diabetes. Prev Care Nurs Midwifery J. 2021;11(4):17-25. doi:10.52547/pcnm.11.4.17
Crossref | Google Scholar - Brew-Sam N, Chib A, Rossmann C. Differential influences of social support on app use for diabetes self-management – a mixed methods approach. BMC Med Inform Decis Mak. 2020;20(1):151. doi:10.1186/s12911-020-01173-3
PubMed | Crossref | Google Scholar - Yehualashet FA, Tegegne ET, Ayele AD, Takele WW. Do adult patients with diabetes mellitus living in rural part of Ethiopia and having poor social support have disproportionately poor self-care practice? A systematic review and meta-analysis. Prim Care Diabetes. 2021;15(4):642-652. doi:10.1016/j.pcd.2021.02.010
PubMed | Crossref | Google Scholar - Awang Ahmad NA, Sallehuddin MAA, Teo YC, Abdul Rahman H. Self-Care Management of Patients with diabetes: nurses’ perspectives. J Diabetes Metab Disord. 2020;19(2):1537-1542. doi:10.1007/s40200-020-00688-w
PubMed | Crossref | Google Scholar - Zare S, Ostovarfar J, Kaveh MH, Vali M. Effectiveness of theory-based diabetes self-care training interventions; a systematic review. Diabetes Metab Syndr. 2020;14(4):423-433. doi:10.1016/j.dsx.2020.04.008
PubMed | Crossref | Google Scholar
Acknowledgments
The authors would like to express their sincere gratitude to Dr. Shah Hussain, Principal/Associate Professor, Janbar College of Nursing, Swat, for his invaluable supervision, guidance, and support throughout the course of this study.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author Information
Corresponding Author:
Nasar Mian
Department of Nursing
National College of Nursing, Swat, Pakistan
Email: nasarmian819@gmail.com
Co-Authors:
Aftab Ahmad, Muhammad Faisal Iqbal, Hayat Ullah, Dawood Khan, Asmat Ullah,
Zafar Ali, Akhtar Ali
Department of Nursing
National College of Nursing, Swat, Pakistan
Shah Hussain
Department of Nursing
Janbar College of Nursing, Swat, Pakistan
Authors Contributions
Nasar Mian, Aftab Ahmad, and Muhammad Faisal Iqbal contributed to data collection and data analysis. Hayat Ullah, Dawood Khan, and Asmat Ullah contributed to data collection and literature review. Zafar Ali contributed to data collection and data organization. Akhtar Ali and Shah Hussain contributed to the analysis and interpretation.
Ethical Approval
Ethical Approval was obtained from the Saidu Teaching Hospital, Swat, Ref No SGTH/IRB/2026/11
Conflict of Interest Statement
The authors declare there is no conflict of interest.
Guarantor
Nasar Mian is the guarantor of this study and takes full responsibility for the integrity of the data and the accuracy of the data analysis.
DOI
Cite this Article
Mian N, Ahmad A, Iqbal MF, et al. Social Support as a Strategy to Overcome Challenges in Diabetes Self-Care Management. medtigo J Med. 2026;4(1):e3062421. doi:10.63096/medtigo3062421 Crossref













