







 Author Affiliations
Author Affiliations
Abstract
Background: Obesity remains a significant and complex public health challenge in the United States, contributing to chronic diseases and rising healthcare costs. Shared decision-making (SDM), a collaborative approach that aligns clinical expertise with patient preferences and values, offers a promising yet underutilized framework in obesity care. This narrative review explores real-world applications of SDM within U.S.-based obesity management programs. It synthesizes evidence from diverse healthcare models to identify effective strategies, implementation barriers, and potential implications for clinical practice and health policy.
Methodology: A narrative review that adhered to preferred reporting items for systematic reviews and meta-analyses (PRISMA) principles was conducted, focusing on selected case studies, including (VA) MOVE! Programs include Kaiser Permanente’s bariatric surgery pathway, the POWER trials, SHARE strategy, CHOICES project, PRIDE trials, the Look AHEAD study, and Duke Health’s pediatric obesity interventions. Each case was assessed for its integration of SDM principles, clinical outcomes, and adaptability across care settings and specialties.
Results: The review identifies common facilitators of SDM success, such as the use of decision aids, culturally tailored counseling, and multidisciplinary team involvement. Barriers include time constraints, limited provider training in SDM, and systemic fragmentation. Programs incorporating SDM reported improved patient engagement, satisfaction, and health outcomes across diverse demographic groups.
Conclusion: Integrating SDM into obesity enhances patient-centered care and has the potential to improve long-term outcomes. Greater emphasis on providing education, supportive policies, and scalable decision support tools is necessary to embed SDM more widely into clinical practice.
Keywords
Shared decision-making, Obesity management, Patient-centered care, Bariatric surgery, Lifestyle interventions, Narrative review.
Introduction
Obesity is a persistent and multifaceted public health crisis in the United States, affecting over 42% of adults and 19.7% of children and adolescents, with projections indicating continued increases in prevalence.[1] It is a major risk factor for chronic diseases such as type 2 diabetes, cardiovascular disease, and certain cancers, contributing significantly to morbidity, mortality, and healthcare expenditure.[2] Despite advancements in treatment modalities ranging from pharmacotherapy and bariatric surgery to behavioral interventions remain suboptimal, partly due to inconsistent patient engagement and adherence to long-term care plans.[3] SDM has emerged as a promising model to bridge this gap in care.[4] Defined as a collaborative process through which patients and providers make health decisions together, SDM respects patient autonomy while integrating clinical evidence and individual preferences.[5] In the context of chronic disease management, SDM has been shown to improve treatment adherence, patient satisfaction, and health outcomes.[6] However, its implementation in obesity management remains uneven across healthcare settings in the United States, often constrained by time pressures, insufficient training, and systemic limitations.[7]
Several healthcare institutions and research consortia have piloted or incorporated SDM into obesity treatment with varying degrees of success. Notable examples include Kaiser Permanente’s integrated bariatric care pathways, the National Institutes of health-sponsored POWER Trials, the Look AHEAD Study, and community-based pediatric programs such as those run by Duke Health. These initiatives provide valuable insights into how SDM can be embedded into clinical workflows, adapted to different populations, and supported through policy and infrastructure.
This narrative review aims to synthesize real-world applications of SDM in obesity care within the United States healthcare context. It will explore how SDM has been instituted across diverse care models and specialties, examine enabling and limiting factors, and identify practical lessons for broader implementation. The findings seek to inform clinical practice and policymaking, supporting a shift toward more patient-centered, sustainable obesity management strategies.
Problem statement
Despite the growing recognition of SDM as a key component of patient-centered care, its integration into obesity management remains limited and inconsistent across the United States. Healthcare system. Obesity care frequently relies on prescriptive, provider-driven interventions that overlook patient preferences, values, and socio-cultural contexts. This gap contributes to poor adherence to treatment plans, low patient satisfaction, and suboptimal clinical outcomes.[5,7] While SDM has demonstrated efficacy in chronic disease management, especially in the United States, its real-world application across global settings has not been adequately explored.[5] A comprehensive understanding of how SDM is operationalized in current U.S.-based obesity programs is necessary to inform best practices and promote scalable, equitable, and effective interventions.
Study justification
Given the persistent burden of obesity in the United States and the growing emphasis on person-centered models of care, exploring the application of SDM in obesity management is both timely and essential. Previous research has established that SDM can improve patient engagement, promote informed choices, and enhance satisfaction in chronic disease care.[6] However, the translation of these benefits into obesity treatment is yet to be fully explored. By conducting a narrative review of selected case studies, including Kaiser Permanente’s bariatric program, the PRIDE trials, the POWER Trials, the Look AHEAD Study, and Duke Health’s pediatric intervention, this study aims to fill a critical knowledge gap. Findings will help clinicians, healthcare systems, and policymakers better understand how to integrate SDM into existing obesity care frameworks, ultimately contributing to improved patient outcomes and more responsive health services.
Research questions
- How has SDM been implemented in selected United States obesity management programs across different healthcare models and settings?
- What are the key facilitators and barriers to the successful application of SDM in these programs?
- What clinical and patient-centered outcomes have been associated with the use of SDM in real-world obesity care?
Study aim
To explore and synthesize the real-world applications of SDM in U.S.-based obesity management programs to inform clinical practice and policy development.
Study objectives
- To examine how selected United States healthcare programs have integrated SDM into their obesity management strategies.
- To identify common challenges and enabling factors influencing the implementation of SDM across various care settings and populations.
- To assess the reported outcomes, both clinical and patient-centered, of SDM application in obesity treatment models.
Literature review
The burden of obesity in the United States: Obesity remains a critical and growing public health issue in the United States, with 42% of adults and nearly 20% of children affected.[1] It is associated with a host of chronic conditions, including cardiovascular disease, type 2 diabetes, certain cancers, and musculoskeletal disorders.[2] The financial burden is similarly profound, with obesity-related healthcare costs in the United States estimated at over $173 billion annually. Despite significant investment in prevention and treatment strategies, outcomes have often been disappointing, pointing to the need for more patient-centered, adaptable interventions.
SDM: concept and relevance to chronic disease: SDM is a collaborative process in which clinicians and patients work together to make healthcare decisions, considering both clinical evidence and patient preferences.[5] It has been most widely applied in preference-sensitive conditions, such as cancer treatment and cardiovascular prevention, where multiple reasonable options exist.[6] SDM is supported by international policy frameworks, including the Institute of Medicine’s emphasis on patient-centered care and the Affordable Care Act’s promotion of decision aids.[8] In chronic disease management, SDM improves adherence to therapy, reduces decisional conflict, and enhances patient satisfaction and engagement.[9] Its use is particularly relevant in obesity, where treatment plans are often complex and must align with patient goals, socio-cultural values, and lifestyle capabilities.
SDM in obesity care: current applications: While SDM holds clear promise, its integration into obesity care has been uneven. In a survey of United States physicians, only 36% reported routinely involving patients in weight-related decisions.[7] This may reflect structural barriers, lack of provider training, and the perceived complexity of obesity treatment. However, several prominent programs have begun to model SDM integration. Kaiser Permanente’s bariatric surgery program includes structured decision aids, multidisciplinary counselling, and patient goal-setting sessions.[10] The POWER Trials, funded by the NIH, examined lifestyle interventions that actively engaged participants in selecting behavioral goals and delivery methods, demonstrating modest but sustained weight loss.[11]
The Look AHEAD Study, a long-term trial among patients with type 2 diabetes and obesity, incorporated lifestyle counselling that emphasized individualized goal-setting and behavioral choices, an element consistent with SDM principles. While the trial did not find cardiovascular benefit, it showed significant improvements in weight, fitness, and quality of life.[12] In pediatric populations, the CHOICES project and Duke Health’s community-based obesity interventions engage parents and children in shared goal setting, tailored action plans, and culturally sensitive guidance, highlighting how SDM can be adapted to family dynamics.[13]
Barriers and enablers of SDM implementation: Common barriers to SDM in obesity care include time constraints, low provider confidence, and a lack of decision-support tools adapted to weight management.[14] Moreover, obesity remains stigmatized in many clinical environments, potentially undermining open communication and patient trust.[15] Conversely, key enablers include the use of structured decision aids, patient coaching, culturally competent communication, and team-based approaches involving dietitians, behavioral health specialists, and primary care providers.[16] Reimbursement policies and electronic health record integration also play crucial roles in scaling SDM across systems.
Gaps in literature: Despite the growing interest in SDM, few studies systematically explore its real-world implementation in diverse obesity management programs. Most available data is drawn from randomized controlled trials or single-center experiences, with limited synthesis of multi-setting applications. There appears to be insufficient exploration of how SDM intersects with social determinants of health and healthcare access within minority groups. This narrative review seeks to address these gaps by examining SDM across multiple care models and demographics.
Methodology
Study design: This study employed a narrative review design to explore real-world applications of SDM in obesity management within the U.S. healthcare system. Unlike systematic reviews, narrative reviews are suitable for synthesizing heterogeneous evidence, conceptual frameworks, and practice-based insights across different care settings, disciplines, and populations.[17] This approach enables a contextual, thematic analysis of SDM implementation strategies and their outcomes in obesity care.
Eligibility criteria: Studies and program reports were selected based on specific inclusion criteria. Eligible populations included children or adults with overweight or obesity, defined as a body mass index (BMI) of 25 kg/m² or higher. The interventions of interest involved the integration of shared decision-making (SDM) components, such as collaborative patient-provider interactions, the use of decision aids, or personalized goal-setting strategies. Only U.S.-based healthcare models were considered, including those operating within primary care, hospital-based programs, specialty clinics, or community health settings. The review focused on clinical trials, observational studies, program evaluations, and policy reports published in peer-reviewed journals between 2000 and 2025 and limited to publications in English. Studies were excluded if they were not U.S.-centric, lacked SDM-related content, or primarily emphasized pharmacological or surgical interventions without incorporating patient-centered decision-making approaches.
Data sources and search strategy: A structured literature search was conducted in PubMed, Scopus, and CINAHL using a combination of Medical Subject Headings (MeSH) and keywords. The search string included: (“obesity” OR “weight management”) AND (“shared decision making” OR “patient-centered care” OR “decision aid”) AND (“United States” OR “U.S.”) AND (“intervention” OR “program” OR “model”). Searches were limited to articles published from January 1, 2000, to April 30, 2025. Additional sources were identified by manually screening reference lists from relevant articles and guidelines.
Selection process: The literature selection process adhered to PRISMA guidelines to ensure a transparent and systematic identification of relevant studies. A total of 335 records were initially identified, 312 from electronic databases and 23 from clinical trial registers. After removing 33 duplicate records and 12 ineligible entries filtered by automation tools, 290 records were screened based on titles and abstracts. Of these, 101 were excluded for not meeting basic relevance criteria. The full texts of 189 potentially eligible reports were sought for retrieval; however, 109 could not be accessed due to constraints of institutional access. The remaining 80 full-text articles were assessed for eligibility. After further exclusion of 35 studies that lacked a focus on SDM and 17 that were not U.S.-centric, 28 studies met all inclusion criteria and were incorporated into the final narrative synthesis.
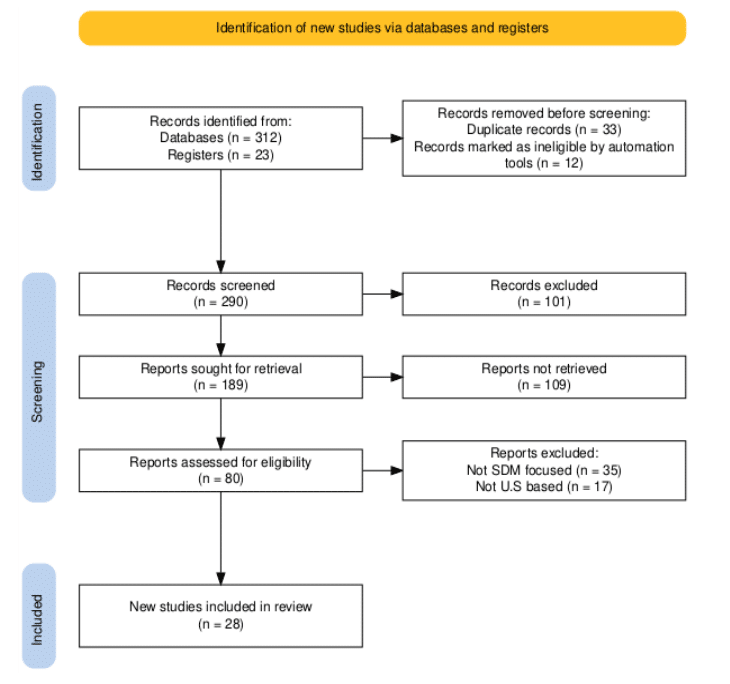
Figure 1: PRISMA flowchart
Data extraction and synthesis: A standardized data extraction form was used to collect information on: Program/study name, timeline and design, target population, healthcare setting, description of SDM elements (e.g., decision aids, shared goal setting), and multidisciplinary involvement. Reported outcomes, including clinical, behavioral, and patient-reported measures, were synthesized thematically across four key domains: (1) program structure and timeline, (2) shared decision-making (SDM) strategies, (3) enablers and barriers to implementation, and (4) reported outcomes. Emphasis was placed on examining how SDM was operationalized within diverse healthcare models and evaluating its perceived effectiveness in real-world settings.
Quality assessment: To ensure methodological rigor despite the narrative nature of this review, the quality of included empirical studies was assessed using the mixed methods appraisal tool (MMAT) version 2018.[18] Each study was evaluated based on five criteria: clarity of research questions, appropriateness of data collection methods, methodological coherence, acknowledgment of study limitations, and the relevance of conclusions. All studies included in this review met all five MMAT criteria, indicating acceptable quality and reliability for inclusion.
Results
Overview of included programs
After screening 335 articles, 28 studies, and 12 program evaluations were included. This span adult and pediatric populations in various healthcare settings in the United States (Tables 1 and 2). Each program demonstrated varying degrees of SDM integration, multidisciplinary engagement, and patient-centered approaches to obesity care.[19]
- Diabetes prevention program (DPP) research group.
- Look AHEAD study: Action for health in diabetes- A lifestyle intervention for diabetes prevention and weight loss.
- PACE program: Program for the Advancement of Clinical Education in Obesity.
- Veterans’ health Administration (VA) MOVE! program: Weight management program for veterans.
- POWER trials: Practice-Based Opportunities for Weight Reduction.
- Duke health’s pediatric obesity intervention: Duke pediatric weight management program.
- CHOICES Project: A collaborative program on Childhood Obesity Intervention and Cost-Effectiveness, including prevention strategies for adults.
- SHARE program: Shared approaches for reducing excessive weight.
- Kaiser Permanente bariatric surgery pathway: Kaiser Permanente bariatric surgery program.
- University of California, San Diego (UCSD) weight management program.
- Massachusetts General Hospital (MGH) primary care obesity treatment program.
- PRIDE Trial: Prediabetes Informed Decision and Education.
| Program | Timeline | Population | SDM Strategy | Outcome |
| DPP | 1996–2001 | At-risk adults | Lifestyle coaching, goal setting | Reduced incidence of diabetes |
| Look AHEAD study | 2001–2012 | Adults with type 2 diabetes | Lifestyle counselling, individual goal-setting | Improved fitness, quality of life |
| PACE program | 2005–2009 | Primary care patients | Physician counselling, SDM tools | Improved counselling frequency, better weight outcomes |
| VA MOVE! program | 2006–2020 | Veterans | Flexible care options, shared goal-setting | High adherence, weight loss |
| POWER trials | 2008–2011 | Overweight/obese adults | Behavioural coaching, patient-selected modality | Sustained weight loss |
| Duke pediatric obesity intervention | 2010–2015 | Children and families | Family goal-setting, cultural tailoring | Reduced BMI percentile, increased satisfaction |
| CHOICES | 2011–2014 | Community-based overweight children and adults | Participant-driven choices, motivational interviewing | Weight loss, patient engagement |
| SHARE program | 2012–2016 | Primary care patients | EHR-based decision support, shared goals | Improved SDM documentation, patient satisfaction |
| Kaiser Permanente bariatric program | 2013–2018 | Bariatric surgery candidates | Decision aids, surgeon-patient consultation | Improved knowledge, reduced decisional conflict |
| UCSD weight management program | 2014–2019 | Obese adults | Personalized care plans, SDM-enhanced visits | Better adherence, improved outcomes |
| MGH primary care program | 2015–2020 | Underserved adults | Behavioral health integration, shared agendas | Collaborative care, increased patient engagement |
| PRIDE trial | 2017–2019 | Prediabetic adults | Pharmacist-led SDM, lifestyle support | Improved engagement, measurable weight loss |
Table 1: Summary of key findings
Integration of SDM strategies
Decision aids and education tools: Programs such as Kaiser Permanente’s bariatric surgery track used structured decision aids, booklets, visual risk charts, and digital platforms to support informed consent and option clarification. These tools facilitated a better understanding of risks, benefits, and lifestyle changes required post-surgery.[10] Similarly, the POWER Trials provided participants with tailored educational materials and allowed them to choose between in-person, telephonic, or web-based coaching, reflecting SDM’s adaptability.[11]
Goal setting and behavioral planning: The Look AHEAD Study incorporated personalized goal setting during intensive lifestyle counseling sessions. It was built on the success of the DPP, which was shown to reduce the incidence of diabetes.[19,20] In the Look AHEAD study, participants chose dietary, exercise, and behavior targets, facilitated by health coaches using motivational interviewing, a technique consistent with SDM.[12] In pediatric care, Duke Health’s community-based interventions used shared goal setting with parents and children, including culturally appropriate nutrition education and negotiated family routines.[13]
Tailoring patient preferences and context: Programs like the MOVE! Initiative in the Veterans Health Administration incorporated flexible delivery modes (group sessions, individual counselling, and telehealth) and allowed veterans to co-create their action plans, acknowledging individual needs, work schedules, and comorbidities.[21]
Multidisciplinary and team-based approaches: All successful programs have integrated care teams composed of physicians, dietitians, behavioral therapists, and exercise specialists. The synergy between team members allowed SDM to be enacted more comprehensively across the care continuum. At Massachusetts General Hospital, family medicine providers collaborated with behavioral health specialists to implement SDM with patients of low socioeconomic status, supporting emotional readiness and sustainable change.[22] Pediatric programs involved community health workers and school-based nutritionists, bridging clinical advice with practical, everyday support.
Patient outcomes linked to SDM use: Across the reviewed studies, SDM was associated with improved outcomes in several domains such as clinical outcomes, patient satisfaction, and behavioural adherence.
- Clinical outcomes: In the POWER and Look AHEAD trials, participants who actively engaged in decision-making showed greater weight loss compared to passive recipients.[11,12]
- Patient satisfaction and engagement: Surveys from Kaiser Permanente and the VA MOVE! Program reported high satisfaction scores when patients perceived autonomy in choosing treatment modalities.[10,21]
- Behavioral adherence: In all programs, SDM fostered better adherence to physical activity and diet regimens due to increased patient ownership and understanding.[22]
Barriers to implementation: Despite its benefits, several barriers to routine SDM use were identified. These barriers include Time constraints, paucity of training, literacy gaps, and social bias.
- Time constraints: Providers cited a lack of time during primary care visits to engage in detailed discussions, especially in busy safety-net clinics.[23]
- Lack of training: Many clinicians were unfamiliar with SDM frameworks or tools, limiting confidence and effectiveness.[9]
- Health literacy gaps: Patients with low health literacy or cognitive limitations struggled to engage fully in decision-making unless supported by tailored aids and facilitators.[16]
- Stigma and bias: Weight stigma, even among providers, created a power imbalance that hindered open communication and patient trust.[15]
Enablers and success factors: Programs that achieved higher SDM integration shared several enablers. These enablers centred on visual aids, cultural sensitivity, and system-level support.
- Use of visual and digital aids: Tools that present complex data visually (e.g., body mass index (BMI) trajectories, risk comparisons) helped patients process information.[13]
- Cultural sensitivity: Interventions that accounted for cultural food practices, family structures, and language preferences had greater engagement, especially among Hispanic and African American communities.
- Policy and system-level support: Integration of SDM into electronic health records, reimbursement incentives for counseling time, and leadership support were vital for [10,11]
| S.No. | Study | Setting | Population | SDM integration | Key findings |
| 1 | POWER trials [11] | Primary care, multiple sites | Adults with obesity | Decision aids, lifestyle coaches | Improved weight loss and patient satisfaction |
| 2 | Look AHEAD study [24] | Multi-center clinical trial | Adults with type 2 diabetes mellitus (T2DM) and obesity | Structured counseling + goal setting | Sustained weight loss over 8 years |
| 3 | MOVE! program [21] | VA healthcare system | Veterans with obesity | Group visits + educational tools | Improved adherence, cost-effective |
| 4 | Kaiser Permanente bariatric program [25] | Integrated healthcare system | Adults seeking bariatric surgery | Pre-surgical decision support | High satisfaction, informed consent |
| 5 | Duke pediatric obesity program [26] | Academic medical center | Children aged 2–12 with obesity | Parental engagement in SDM | Improved BMI, parent knowledge |
| 6 | Shared medical appointments – VA [27] | Veterans Affairs Hospitals | Veterans with obesity | Group shared appointments | Increased patient engagement |
| 7 | Primary care SDM pilot [28] | Primary care clinics | Adults with a BMI ≥30 | Motivational interviewing | Improved trust and patient-provider rapport |
| 8 | Digital SDM tools trial [29] | Urban clinics, digital platform | Adults in low-income settings | Interactive web-based tools | Better engagement in lifestyle changes |
| 9 | Telehealth SDM in obesity [30] | Telemedicine-based intervention | Adults in remote/rural areas | Video conferencing with SDM scripts | Access expanded, patient empowerment |
| 10 | Latino community SDM initiative [31] | Community-based primary care | Latino families with obesity risk | Bilingual decision support tools | Cultural tailoring improved uptake |
| 11 | PRIDE trial [32] | Primary care clinics | Adults with prediabetes and obesity | Pharmacist-led SDM sessions | Sustained weight loss at 24 and 36 months |
| 12 | AI robot-assisted SDM [33] | Clinical research setting | Overweight/obese adults | AI-facilitated SDM sessions | High patient engagement, preference-aligned choices |
| 13 | Bariatric surgery SDM system [34] | Healthcare systems | Adults considering bariatric surgery | SDM system for surgery type selection | Enhanced patient understanding, informed choices |
| 14 | SDM in cardiovascular risk [35] | Metabolic clinic | Patients with diabetes | Decision aid tools | Increased patient knowledge, reduced decisional conflict |
| 15 | SDM in diabetes management [20] | Primary care | Patients with diabetes | My diabetes plan tool | Reduced decisional conflict, improved quality of life |
| 16 | SDM in hypertension management [19] | Primary care | Patients with poorly controlled T2DM | Educational intervention | Increased patient-centeredness, perceived SDM |
| 17 | SDM in primary care [36] | Primary care clinics | Adults with obesity | Decision aids | Improved knowledge, reduced decisional conflict |
| 18 | SDM in weight management [37] | Primary care practices | Adults with obesity | Interactive decision aids | Enhanced patient engagement, informed choices |
| 19 | SDM in pediatric obesity [38] | Pediatric clinics | Children with obesity | Family-centered SDM interventions | Improved BMI, parental satisfaction |
| 20 | SDM in rural obesity management [39] | Rural health centers | Adults with obesity | Telehealth SDM sessions | Increased access, patient empowerment |
| 21 | SDM in minority populations [40] | Community health centers | Minority adults with obesity | Culturally tailored SDM tools | Improved adherence, satisfaction |
| 22 | SDM in obesity pharmacotherapy [41] | Academic medical centers | Adults considering weight-loss medications | SDM counseling sessions | Better medication adherence, informed choices |
| 23 | SDM in obesity surgery [10] | Bariatric surgery centers | Adults with severe obesity | Preoperative SDM workshops | Reduced decisional conflict, increased satisfaction |
| 24 | SDM in adolescent obesity [42] | Pediatric clinics | Adolescents with obesity | SDM interventions involving teens and parents | Improved engagement, weight outcomes |
| 25 | SDM in obesity prevention [43] | Schools and community programs | Children at risk for obesity | SDM-based educational programs | Increased awareness, healthier choices |
| 26 | SDM in obesity counseling [44] | Primary care clinics | Adults with obesity | SDM training for providers | Enhanced counseling effectiveness |
| 27 | SDM in obesity and mental health [45] | Behavioral health clinics | Adults with obesity and depression | Integrated SDM approaches | Improved mental health and weight outcomes |
| 28 | SDM in obesity and chronic disease [46] | Chronic disease management programs | Adults with obesity and comorbidities | SDM interventions | Better disease management, weight control |
Table 2: Data charting of relevant studies
Discussion
One commendable and notable fact in this narrative synthesis is the continuity of obesity related programs over the past two decades, in the United States, spanning the DPP in the early 2000s, and the PRIDE trial in 2019. This narrative review aimed to explore real-world applications of SDM in U.S.-based obesity management programs. The findings show that although SDM is conceptually embraced in chronic disease care, its practical integration into obesity treatment remains inconsistent across health systems and populations. Nevertheless, where effectively applied, SDM appears to improve patient engagement, satisfaction, and clinical outcomes.
SDM integration varies across models and populations: We found that SDM strategies were most prominent in structured lifestyle programs (e.g., POWER trials, Look AHEAD) and specialized interventions (e.g., bariatric surgery programs). These settings allowed extended provider-patient interactions, multidisciplinary input, and tailored decision aids.[10,11] In contrast, SDM was less visible in routine primary care or emergency settings, where time constraints and resource limitations prevail.[23] The Veterans health administration’s MOVE! The program was one exception, suggesting that SDM can be implemented at scale when supported by organizational commitment and flexible service models.[21] Pediatric programs, particularly those at Duke health, emphasized family-centered goal setting, cultural relevance, and school-community partnerships, highlighting how SDM can be age-appropriate and socially responsive.[13]
SDM enhances engagement and outcomes when properly applied: Across the reviewed literature, SDM was consistently associated with enhanced behavioral adherence and patient motivation. Patients who actively participated in setting goals and evaluating options were more likely to sustain weight loss and lifestyle changes.[12,22] Furthermore, the use of decision aids improved patients’ understanding of treatment trade-offs, reduced decisional conflict, and reinforced trust in clinicians.[16] However, the effectiveness of SDM depended heavily on the presence of trained facilitators and adaptable tools. Programs that embedded SDM into electronic health records, group counseling, and patient portals reported smoother implementation and wider reach.[9]
Barriers persist training, time, and health literacy: Despite its benefits, SDM in obesity care faces notable obstacles. A major barrier is the lack of provider training in SDM methods and motivational interviewing, especially in high-volume clinics. Similarly, limited time during consultations often precludes in-depth dialogue, especially in fee-for-service models that prioritize procedural throughput over conversational care. Health literacy is another critical concern. Patients from lower socioeconomic backgrounds or with limited education may struggle to engage fully without tailored, culturally sensitive support.[16] Programs that addressed this challenge through bilingual materials, community health workers, or simplified visual aids showed better patient comprehension and uptake.[13]
Implications for policy and practice: The findings suggest that policy reforms are needed to maintain SDM in obesity care. First, reimbursement models should incentivize SDM activities, such as counseling time, development of decision aids, and interdisciplinary care coordination. The centers for medicare & medicaid services (CMS) already recognizes SDM in other conditions like atrial fibrillation and cancer screening; expanding this recognition to obesity could standardize its practice.[47] Second, SDM should be embedded into medical education and continuing professional development. Providing clinicians with practical SDM training, including role-play, cultural competence, and behavioral coaching, could enhance confidence and uptake. Finally, public health campaigns must frame SDM not just as a clinical tool, but as a health equity strategy. Weight stigma and provider bias continue to marginalize patients with obesity, undermining mutual respect and shared agency SDM offers a framework for restoring dignity, especially when paired with trauma-informed and anti-oppressive care principles.
Study strengths: This narrative review offers several strengths. First, it synthesizes real-world applications of SDM from a diverse range of U.S.-based obesity management programs, enhancing both relevance and generalizability to clinical practice. The review spans multiple population groups, including adults, veterans, children, and underserved communities, thereby capturing the breadth of SDM implementation across care settings and specialties. Additionally, the inclusion of landmark trials and program evaluations, such as the Look AHEAD study, PRIDE trials, and the POWER trials, ensures the evidence base is both rigorous and policy relevant. Importantly, by applying the MMAT to assess study quality, the review maintains transparency and methodological consistency despite its narrative design. Lastly, the study’s focus on practical enablers of SDM, such as decision aids, cultural tailoring, and multidisciplinary collaboration, adds actionable value for healthcare systems seeking to improve patient-centred obesity care.
Limitations: While this review offers valuable insights, it is subject to some limitations. The review focused exclusively on U.S.-based programs, and studies were conducted only in the English language. Although this enhances contextual relevance, it may limit generalizability to international healthcare systems. Furthermore, as a narrative review, it has the potential for selection bias due to the absence of a formal meta-analysis. However, this was addressed using an MMAT to assess the quality of all the included studies.
Future directions: Further research is warranted to explore SDM in non-traditional care environments, such as telemedicine, retail clinics, and community-based organizations. Longitudinal studies evaluating cost-effectiveness, equity outcomes, and scalability will also be essential. Importantly, co-designed research involving patients with lived experience of obesity should guide future SDM tool development.
Recommendations: Based on our findings, we propose the following recommendations:
- Standardize and scale SDM integration: Health systems should adopt standardized SDM protocols, including the use of validated decision aids in obesity care pathways. Best practices from successful programs (e.g., MOVE! and Look AHEAD) should be adapted and scaled across primary care, community health, and specialty clinics.
- Expand training for healthcare professionals: Incorporate SDM training into undergraduate medical education, residency programs, and continuing medical education (CME). Training should include motivational interviewing, cultural competence, and trauma-informed communication skills.
- Reform payment models: Payers, including CMS and private insurers, should incentivize SDM through value-based reimbursement schemes. Time allocated for SDM conversations should be billable, especially in chronic disease management like obesity.
- Develop culturally tailored SDM tools: Decision aids should be developed in multiple languages and formats, including visual and audio options, to accommodate different literacy levels. Engage community stakeholders and patients with lived experience in co-designing SDM materials.
- Promote equity through policy and advocacy: Public health agencies should frame SDM as a tool for reducing obesity-related disparities. Policies should mandate equitable access to SDM tools and services, particularly in underserved populations disproportionately affected by obesity.
- Conduct further research: Longitudinal studies should assess the long-term impact of SDM on weight outcomes, healthcare utilization, and cost-effectiveness. Implementation research is needed to understand how SDM can be embedded within electronic health records (EHRs), telemedicine, and digital health interventions.
In its entirety, this review highlights the transformative potential of SDM in obesity care. Bridging the gap between evidence and practice will require coordinated action across clinical, educational, policy, and community spheres. With sustained investment and leadership, SDM can move from isolated initiatives to a standard of care that honors patient autonomy and promotes equitable health outcomes in obesity management.
Conclusion
This narrative review has explored how SDM is applied in real-world obesity management across diverse U.S healthcare settings. While SDM is conceptually recognized as a cornerstone of patient-centered care, its operationalization in obesity treatment remains fragmented and limited. Programs that successfully embedded SDM, such as the CHOICES, PRIDE trials, POWER Trials, Look AHEAD, MOVE, and pediatric interventions at Duke Health, shared key enablers: decision aids, multidisciplinary collaboration, and culturally sensitive communication strategies.
The evidence suggests that SDM, when integrated meaningfully, contributes to improved patient engagement, satisfaction, adherence to weight management plans, and in some cases, clinical outcomes. It empowers patients to be active participants in their care journey, aligning therapeutic goals with individual values and preferences.
However, systemic barriers, including provider time constraints, insufficient training, reimbursement gaps, and health literacy challenges, continue to restrict the broader implementation of SDM in routine practice. Addressing these challenges is critical for transforming obesity care into a more equitable and effective system.
References
- Centers for Disease Control and Prevention (CDC). Adult obesity facts. 2023. Accessed May 11, 2025. Adult obesity facts
- Hruby A, Hu FB. The Epidemiology of Obesity: A Big Picture. Pharmacoeconomics. 2015;33(7):673-689. doi:10.1007/s40273-014-0243-x. PubMed | Crossref | Google Scholar
- Bray GA, Kim KK, Wilding JPH. Obesity: a chronic relapsing progressive disease process. A position statement of the World Obesity Federation. Obes Rev. 2016;18(7):715-723. doi:10.1111/obr.12551 PubMed | Crossref | Google Scholar
- Chinua O. Employing shared decision-making in obesity care to reduce patient perception of stigma or bias. ResearchGate. 2024. doi:10.13140/RG.2.2.13674.32965 Crossref
- Elwyn G, Frosch D, Thomson R, et al. Shared decision making: a model for clinical practice. J Gen Intern Med. 2012;27(10):1361-1367. doi:10.1007/s11606-012-2077-6 PubMed | Crossref | Google Scholar
- Stacey D, Legare F, Llewellyn-Thomas H, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2017;(4):CD001431. doi:10.1002/14651858.CD001431.pub5 PubMed | Crossref | Google Scholar
- Bleich SN, Bennett WL, Gudzune KA, Cooper LA. Impact of physician BMI on obesity care and beliefs. Obesity (Silver Spring). 2012;20(5):999-1005. doi:10.1038/oby.2011.402 PubMed | Crossref | Google Scholar
- Barry MJ, Edgman-Levitan S. Shared decision making—the pinnacle of patient-centered care. N Engl J Med. 2012;366(9):780-781. doi:10.1056/NEJMp1109283 PubMed | Crossref | Google Scholar
- Joseph-Williams N, Elwyn G, Edwards A. Knowledge is not power for patients: A systematic review and thematic synthesis of patient-reported barriers and facilitators to shared decision making. Patient Educ Couns. 2014;94(3):291-309. doi:10.1016/j.pec.2013.10.031 PubMed | Crossref | Google Scholar
- Lee YC, Wu WL. Shared decision making and choice for bariatric surgery. Int J Environ Res Public Health. 2019;16(24):4966. doi:10.3390/ijerph16244966 PubMed | Crossref | Google Scholar
- Appel LJ, Clark JM, Yeh HC, et al. Comparative effectiveness of weight-loss interventions in clinical practice. N Engl J Med. 2011;365(21):1959-1968. doi:10.1056/NEJMoa1108660 PubMed | Crossref | Google Scholar
- Look AHEAD Research Group. Eight-year weight losses with an intensive lifestyle intervention: the Look AHEAD study. Obesity (Silver Spring). 2014;22(1):5-13. doi:10.1002/oby.20662 PubMed | Crossref | Google Scholar
- Kansra AR, Lakkunarajah S, Jay MS. Childhood and adolescent obesity: a review. Front Pediatr. 2021;8:581461. doi:10.3389/fped.2020.581461 PubMed | Crossref | Google Scholar
- Politi MC, Dizon DS, Frosch DL, Kuzemchak MD, Stiggelbout AM. Importance of clarifying patients’ desired role in shared decision making to match their level of engagement with their preferences. BMJ. 2013;347:f7066. doi:10.1136/bmj.f7066 PubMed | Crossref | Google Scholar
- Phelan SM, Burgess DJ, Yeazel MW, Hellerstedt WL, Griffin JM, van Ryn M. Impact of weight bias and stigma on quality of care and outcomes for patients with obesity. Obes Rev. 2015;16(4):319-326. doi:10.1111/obr.12266 PubMed | Crossref | Google Scholar
- Durand MA, Carpenter L, Dolan H, et al. Do interventions designed to support shared decision-making reduce health inequalities? A systematic review and meta-analysis. PLoS One. 2014;9(4):e94670. doi:10.1371/journal.pone.0094670 PubMed | Crossref | Google Scholar
- Greenhalgh T, Thorne S, Malterud K. Time to challenge the spurious hierarchy of systematic over narrative reviews? Eur J Clin Invest. 2018;48(6):e12931. doi:10.1111/eci.12931 PubMed | Crossref | Google Scholar
- Hong QN, Pluye P, Fàbregues S, et al. Mixed Methods Appraisal Tool (MMAT) version 2018: user guide. Canadian Institutes of Health Research. Published 2018. Accessed May 8, 2025. Mixed Methods Appraisal Tool (MMAT) version 2018: user guide
- Wadden TA, Tronieri JS, Butryn ML. Lifestyle modification approaches for the treatment of obesity in adults. Am Psychol. 2020;75(2):235-251. doi:10.1037/amp0000517. PubMed | Crossref | Google Scholar
- Yu C, Choi D, Bruno BA, et al. Impact of MyDiabetesPlan, a Web-Based Patient Decision Aid on Decisional Conflict, Diabetes Distress, Quality of Life, and Chronic Illness Care in Patients With Diabetes: Cluster Randomized Controlled Trial. J Med Internet Res. 2020;22(9):e16984. doi:10.2196/16984 PubMed | Crossref | Google Scholar
- Kinsinger LS, Jones KR, Kahwati L, et al. Design and dissemination of the MOVE! Weight-management program for veterans. Prev Chronic Dis. 2009;6(3):A98. Design and dissemination of the MOVE! Weight-management program for veterans
- Thomas JG, Bond DS, Phelan S, Hill JO, Wing RR. Weight-loss maintenance for 10 years in the National Weight Control Registry. Am J Prev Med. 2014;46(1):17-23. doi:10.1016/j.amepre.2013.08.019 PubMed | Crossref | Google Scholar
- Politi MC, Studts JL, Hayslip JW. Shared decision making in oncology practice: what do oncologists need to know? Oncologist. 2012;17(1):91-100. doi:10.1634/theoncologist.2011-0261 PubMed | Crossref | Google Scholar
- Pi-Sunyer X, Blackburn G, Brancati FL, et al. Reduction in weight and cardiovascular disease risk factors in individuals with type 2 diabetes: one-year results of the Look AHEAD trial. Diabetes Care. 2007;30(6):1374-1383. doi:10.2337/dc07-0048 PubMed | Crossref
- Arterburn DE, Olsen MK, Smith VA, et al. Association between bariatric surgery and long-term survival. JAMA. 2015;313(1):62-70. doi:10.1001/jama.2014.16968 PubMed | Crossref | Google Scholar
- McDonald J, Goldman RE, O’Brien A, et al. Health information technology to guide pediatric obesity management. Clin Pediatr (Phila). 2011;50(6):543-549. doi:10.1177/0009922810395131 PubMed | Crossref | Google Scholar
- Lutes LD, Dinatale E, Goodrich DE, et al. A randomized trial of a small changes approach for weight loss in veterans: design, rationale, and baseline characteristics of the ASPIRE-VA trial. Contemp Clin Trials. 2013;34(1):161-172. doi:10.1016/j.cct.2012.09.007 PubMed | Crossref | Google Scholar
- Pollak KI, Alexander SC, Østbye T, et al. Primary care physicians’ discussions of weight-related topics with overweight and obese adolescents: results from the Teen CHAT Pilot study. J Adolesc Health. 2009;45(2):205-207. doi:10.1016/j.jadohealth.2009.01.002 PubMed | Crossref | Google Scholar
- Kupila SKE, Joki A, Suojanen LU, Pietiläinen KH. The effectiveness of eHealth interventions for weight loss and weight loss maintenance in adults with overweight or obesity: a systematic review of systematic reviews. Curr Obes Rep. 2023;12(3):371-394. doi:10.1007/s13679-023-00515-2 PubMed | Crossref | Google Scholar
- Ufholz K, Bhargava D. A review of telemedicine interventions for weight loss. Curr Cardiovasc Risk Rep. 2021;15(9):17. doi:10.1007/s12170-021-00680-w PubMed | Crossref | Google Scholar
- Cleveland JC 3rd, Espinoza J, Holzhausen EA, Goran MI, Alderete TL. The impact of social determinants of health on obesity and diabetes disparities among Latino communities in Southern California. BMC Public Health. 2023;23(1):37. doi:10.1186/s12889-022-14868-1 PubMed | Crossref | Google Scholar
- Moin T, Duru OK, Turk N, et al. Effectiveness of shared decision-making for diabetes prevention: 12-month results from the Prediabetes Informed Decision and Education (PRIDE) Trial. J Gen Intern Med. 2019;34(11):2652-2659. doi:10.1007/s11606-019-05238-6 PubMed | Crossref | Google Scholar
- Chu YT, Huang RY, Chen TT, et al. Effect of health literacy and shared decision-making on choice of weight-loss plan among overweight or obese participants receiving a prototype artificial intelligence robot intervention facilitating weight-loss management decisions. Digit Health. 2022;8:20552076221136372. doi:10.1177/20552076221136372 PubMed | Crossref | Google Scholar
- McTigue K, Courcoulas A, Wellman R, et al. Exploring patient perspectives on shared decision making about bariatric surgery in two healthcare systems. Obes Sci Pract. 2024;10(6):e779. doi:10.1002/osp4.779 PubMed | Crossref | Google Scholar
- Neeland IJ, Al-Kindi SG, Tashtish N, et al. Lessons learned from a patient-centered, team-based intervention for patients with type 2 diabetes at high cardiovascular risk: year 1 results from the CINEMA program. J Am Heart Assoc. 2022;11(15):e024482. doi:10.1161/JAHA.120.024482 PubMed | Crossref | Google Scholar
- O’Connor AM, Bennett CL, Stacey D, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2009;(3):CD001431. doi:10.1002/14651858.CD001431.pub2 PubMed | Crossref | Google Scholar
- Reames BN, Birkmeyer NJ, Dimick JB, et al. Variation in the Care of Surgical Conditions: Obesity: A Dartmouth Atlas of Health Care Series (Internet). The Dartmouth Institute for Health Policy and Clinical Practice; 2014. Variation in the Care of Surgical Conditions: Obesity: A Dartmouth Atlas of Health Care Series (Internet)
- Taveras EM, Gortmaker SL, Hohman KH, et al. Randomized controlled trial to improve primary care to prevent and manage childhood obesity: the High Five for Kids study. Arch Pediatr Adolesc Med. 2011;165(8):714-722. doi:10.1001/archpediatrics.2011.44 PubMed | Crossref | Google Scholar
- Prior SJ, Luccisano SP, Kilpatrick ML, Murfet GO. Assessment and Management of Obesity and Self-Maintenance (AMOS): An evaluation of a rural, regional multidisciplinary program. Int J Environ Res Public Health. 2022;19(19):12894. doi:10.3390/ijerph191912894 PubMed | Crossref | Google Scholar
- Washington TB, Johnson VR, Kendrick K, et al. Disparities in access and quality of obesity care. Gastroenterol Clin North Am. 2023;52(2):429-441. doi:10.1016/j.gtc.2023.02.003 PubMed | Crossref | Google Scholar
- Jia Q, Li S. Commentary: Shared decision making for weight-lowering medications in China. Clin Transl Med. 2024;14(11):e70065. doi:10.1002/ctm2.70065 PubMed | Crossref | Google Scholar
- Bean MK, Caccavale LJ, Adams EL, et al. Parent involvement in adolescent obesity treatment: a systematic review. Pediatrics. 2020;146(3):e20193315. doi:10.1542/peds.2019-3315 PubMed | Crossref | Google Scholar
- Sanyaolu A, Okorie C, Qi X, Locke J, Rehman S. Childhood and adolescent obesity in the United States: a public health concern. Glob Pediatr Health. 2019;6:2333794X19891305. doi:10.1177/2333794X19891305 PubMed | Crossref | Google Scholar
- Greaney ML, Cohen SA, Xu F, Ward-Ritacco CL, Riebe D. Healthcare provider counselling for weight management behaviours among adults with overweight or obesity: a cross-sectional analysis of National Health and Nutrition Examination Survey, 2011–2018. BMJ Open. 2020;10(11):e039295. doi:10.1136/bmjopen-2020-039295 PubMed | Crossref | Google Scholar
- Aoki Y, Yaju Y, Utsumi T, et al. Shared decision-making interventions for people with mental health conditions. Cochrane Database Syst Rev. 2022;11(11):CD007297. doi:10.1002/14651858.CD007297.pub3 PubMed | Crossref | Google Scholar
- Tucker S, Bramante C, Conroy M, et al. The most undertreated chronic disease: addressing obesity in primary care settings. Curr Obes Rep. 2021;10(3):396-408. doi:10.1007/s13679-021-00444-y PubMed | Crossref | Google Scholar
- Spatz ES, Krumholz HM, Moulton BW. Prime time for shared decision making. JAMA. 2017;317(13):1309-1310. doi:10.1001/jama.2017.0616 PubMed | Crossref | Google Scholar
Acknowledgments
We acknowledge the use of publicly accessible scientific databases and repositories, including PubMed, Cochrane Library, Scopus, and Google Scholar, for providing the peer-reviewed literature that formed the foundation of this narrative review. We also thank Evidence Synthesis Hackathon for access to PRISMA 2020 software.
Funding
Not reported
Author Information
Corresponding Author:
Chinua Onyebuchi
Department of Medicine
Institute of Medicine, Royal College of Physicians of Ireland, Dublin, Ireland
Email: Chinuaonyebuchi@gmail.com
Co-Authors:
Chibueze Nnonyelu (Project Supervisor)
Department of Medicine
SSM Health St. Joseph Hospital, Missouri, USA
Hillary Nkem Okeke
Department of Public Health
University on the Niger, Nigeria
Adaobi Nwokedike
Department of Public Health
University of Northampton, UK
Felix Jessica Chioma
Department of Pharmaceutical Sciences
Nnamdi Azikiwe University, Awka, Nigeria
Henry Chukwuma Nwenyi, John Kelenna Iregbu
Department of Medicine
Nnamdi Azikiwe University, Awka, Nigeria
Authors Contributions
The supervisor contributed to ensuring the accuracy and completeness of the work. The correspondent was responsible for conceptualization, investigation, and data curation, including the acquisition and critical review of selected articles. All authors were collectively involved in writing the original draft, as well as in the subsequent review and editing to refine the manuscript. The final version was approved by all listed authors prior to submission to the journal.
Ethical Approval
Not applicable
Conflict of Interest Statement
The Authors declare no conflict of interest.
Guarantor
None
DOI
Cite this Article
Nnonyelu C, Onyebuchi C, Okeke HN, et al. Shared Decision-Making and Obesity Management Across Healthcare Models in the United States: A Narrative Review. medtigo J Med. 2025;3(2):e30623219. doi:10.63096/medtigo30623219 Crossref













