







 Author Affiliations
Author Affiliations
Abstract
Epileptic seizures are among the most common and disabling symptoms in patients with brain tumours, especially gliomas, often severely impacting quality of life and complicating oncologic management. This review synthesizes current evidence on brain tumour–related epilepsy (BTRE) treatment, focusing on antiseizure medication (ASM) choices, withdrawal timing, and surgical outcomes. A systematic search of PubMed and Google Scholar (2015–2025) identified five high-quality studies. Data show that seizure recurrence after ASM withdrawal remains significant, with up to 47% relapsing within three years, even after extended seizure-free periods. Comparative studies indicate that levetiracetam is associated with lower treatment failure rates than valproic acid, mainly due to fewer uncontrolled seizures, although both drugs have notable side effect profiles. Newer-generation ASMs like lacosamide and perampanel demonstrate high responder rates and acceptable tolerability but require monitoring for psychiatric and behavioural effects. Surgical resection remains a cornerstone of treatment, offering long-term seizure freedom for many; over half of patients undergoing surgery successfully withdrew from ASMs altogether. These findings highlight that optimal seizure management in BTRE demands an individualized, multidisciplinary strategy that considers tumour type, seizure risk, drug interactions, and patient preferences. Ultimately, careful ASM selection, timely withdrawal decisions, and integration of surgical interventions are essential to balancing seizure control with maintaining cognitive function and quality of life.
Keywords
Brain tumor–related epilepsy, Antiseizure medications, Gliomas, Seizures, Seizure recurrence, Quality of life.
Introduction
Epileptic seizures are one of the most frequent and burdensome symptoms in patients with brain tumours, especially gliomas. Seizures not only serve as a common initial presentation in these patients but also persist as a major clinical challenge throughout the disease trajectory.[1] The risk of developing epilepsy among patients with brain tumours varies widely and depends on factors such as tumour type, grade, and location. For example, while high-grade gliomas like glioblastomas carry a seizure incidence of around 20–50%, diffuse low-grade gliomas can be highly epileptogenic, with up to 80% or more of patients experiencing seizures at some point during their illness. This stark variation underscores the complexity of managing BTRE.[2]
BTRE is not simply a coexisting condition but can significantly worsen patients’ quality of life, affect cognitive function, and complicate oncological management.[3] In fact, for many patients with slow-growing tumours like low-grade gliomas, uncontrolled seizures may pose a greater threat to functional independence and daily living than the tumour itself. Seizures can lead to social isolation, unemployment, and psychological distress, further amplifying the already substantial burden imposed by the tumour.[4]
Standard-of-care for managing seizures in glioma patients involves ASM once a seizure occurs. However, the treatment landscape is far from straightforward. While ASMs can be highly effective, they are often accompanied by a range of adverse effects that can significantly impair cognitive function, mood, and overall well-being.[5] In intensively monitored clinical settings, adverse effects may occur in up to 90% of patients on ASMs, and approximately 15–20% of patients discontinue therapy due to intolerable side effects. This delicate balance between controlling seizures and minimizing treatment-related toxicity demands careful, individualized decision-making.[6]
The choice of ASM in BTRE is further complicated by potential pharmacokinetic interactions with chemotherapeutic agents and corticosteroids. Many older-generation ASMs, such as phenytoin and carbamazepine, are strong inducers of cytochrome P450 (CYP450) enzymes, which can accelerate the metabolism of chemotherapy drugs, potentially undermining their efficacy.[7] This pharmacological interplay is especially concerning in patients receiving complex multimodal therapy that includes surgery, radiation, and systemic treatments.[8]
Newer-generation ASMs, such as levetiracetam, lacosamide, and perampanel, have emerged as preferable options for many brain tumour patients. Levetiracetam has gained widespread use due to its favourable pharmacokinetic profile, characterized by minimal hepatic metabolism, absence of enzyme induction or inhibition, and relatively predictable plasma levels. Its broad-spectrum efficacy makes it suitable for various seizure types encountered in BTRE.[9] Nonetheless, levetiracetam is not without its challenges; psychiatric and behavioural side effects, including irritability and depression, are common and frequently lead to treatment discontinuation.[10]
Valproic acid, another commonly used ASM in glioma patients, has a long-established history as a broad-spectrum agent. Its additional role as a histone deacetylase inhibitor sparked interest in its potential antitumoral properties, particularly in combination with standard chemoradiotherapy.[11] However, despite promising preclinical data, clinical studies have not consistently demonstrated survival benefits associated with valproic acid use in glioma patients. Moreover, valproic acid’s inhibitory effect on CYP450 enzymes can increase the bioavailability and potentially the toxicity of concomitant chemotherapy, requiring vigilant monitoring.[12,13]
Recent retrospective and prospective studies have explored the retention and treatment failure rates of various ASMs to inform clinical practice better. Retention rates, which encompass both efficacy and tolerability, are increasingly recognized as meaningful outcomes when evaluating ASM effectiveness, alongside traditional endpoints like seizure freedom.[14] Studies comparing levetiracetam and valproic acid in glioma patients have yielded mixed results, with some suggesting similar seizure control but notable differences in side effect profiles and treatment discontinuation rates.[15]
Beyond initial ASM selection, there is growing interest in when and whether it is appropriate to withdraw ASMs in glioma patients who achieve prolonged seizure freedom. In non-brain tumour–related epilepsy, guidelines often recommend considering ASM withdrawal after a minimum of two years of seizure freedom.[16] However, robust data to guide this decision-making in BTRE patients remains limited. Available evidence suggests that the risk of seizure recurrence after ASM withdrawal is not negligible, even in carefully selected patients. For example, one prospective study in grade 2 and 3 glioma patients reported a seizure recurrence rate of 26% within 1.5 years following ASM discontinuation.[16] Similarly, retrospective studies in adults and children with brain tumours have shown recurrence rates ranging from 19% to 27% after withdrawal, highlighting the need for caution.[17]
It remains unclear whether the length of seizure freedom prior to withdrawal influences the likelihood of recurrence in this population. Understanding this relationship is critical, as many glioma patients balance seizure control with the desire to minimize medication burden and side effects.[18] Shared decision-making that incorporates patient values, preferences, and individualized risk profiles is essential when considering ASM withdrawal.[19]
Another important consideration is the impact of BTRE on cognitive function and neuropsychological outcomes. Seizures themselves, along with the effects of ASMs and the underlying tumour, can contribute to cognitive decline. Moreover, the neurocognitive effects of ASMs vary considerably between drugs. For instance, older enzyme-inducing ASMs are more likely to exacerbate cognitive slowing and memory impairment compared to newer non-enzyme–inducing agents. These effects must be weighed carefully, particularly in patients with pre-existing deficits related to tumour location or treatment.[20]
In recent years, novel ASMs such as perampanel have emerged as promising options for BTRE management. Perampanel, a selective, non-competitive AMPA receptor antagonist, has shown efficacy as an add-on therapy for focal-onset seizures.[21] Its long half-life, good oral bioavailability, and predictable pharmacokinetics make it an attractive choice, although side effects such as dizziness, aggression, and mood changes require monitoring. Randomized controlled trials and real-world studies continue to evaluate its safety and effectiveness in brain tumour populations.[22]
Ultimately, seizure management in brain tumour patients requires a comprehensive, multidisciplinary approach that integrates neurology, oncology, and neuropsychology expertise. Optimal outcomes depend not only on selecting the most appropriate ASM but also on addressing broader factors such as tumour control, cognitive preservation, and patient quality of life.[23] Advances in surgical techniques, imaging, and precision medicine hold promise for improving seizure outcomes in these patients. However, more high-quality research is needed to fill gaps in evidence, particularly regarding the long-term comparative effectiveness of different ASMs, the timing and criteria for withdrawal, and strategies to mitigate neurocognitive side effects.[24]
Methodology
A systematic literature search was conducted using PubMed and Google Scholar databases according to the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines. The search included publications from January 1, 2015, to June 30, 2025, and was limited to studies published in English.
Inclusion criteria:
- Clinical trials, observational studies, and randomized controlled trials
- Studies involving human subjects
- Articles published in English
- Studies including female and male participants
- Studies published between January 1, 2015, and June 30, 2025
Exclusion criteria:
- Books, commentaries, editorials, letters, documents, and book chapters
- Case reports, case series, and literature reviews
- Articles published in languages other than English
- Animal studies and in vitro (laboratory) studies
- Articles published before January 1, 2015, or after June 30, 2025
- Studies lacking a reported results section
The initial search yielded a total of 8,027 articles. After applying the inclusion and exclusion criteria, 1,987 references PubMed and Google Scholar. Prior to the screening phase, 1,935 records were excluded for various reasons, including duplication, irrelevance, or insufficient data. The remaining 52 records were screened based on titles and abstracts. Of these, 29 were excluded for not meeting the inclusion criteria.
Following initial screening, 23 full-text reports were sought for retrieval, but 10 could not be accessed due to unavailability or incomplete data. Thirteen full-text articles were assessed for eligibility based on predefined criteria, including methodological quality. During this phase, eight studies were excluded for scoring below 10 on the scale for the assessment of narrative review articles (SANRA) checklist, indicating low quality. Ultimately, 5 studies met all inclusion criteria and were included in the final review.
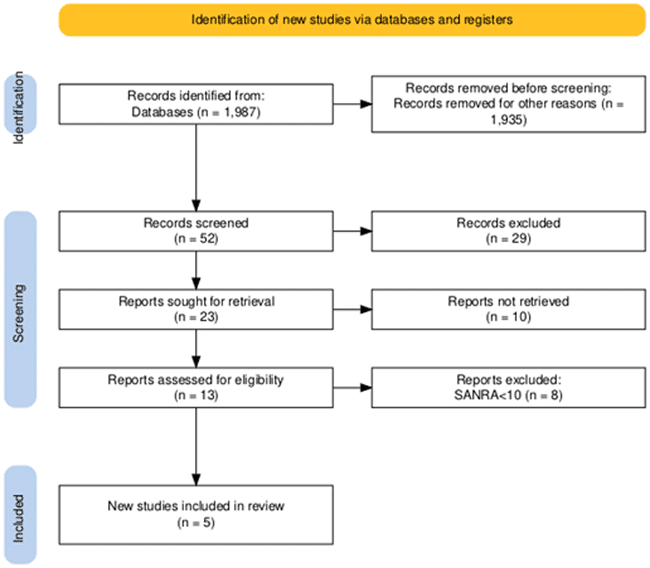
Figure 1: PRISMA flow diagram
Results
Effect of timing of ASM discontinuation on seizure recurrence in glioma patients
Van der Meer PB et al., demonstrated that 185 patients who stopped ASM treatment, 109 (59%) were included: 31% (34/109) were seizure-free for less than 12 months, 29% (32/109) for 12–24 months, and 39% (43/109) for at least 24 months after their last antitumour therapy. Most patients were over 40 years old, male, had grade 2 glioma, underwent surgery and radiotherapy, had focal to bilateral tonic-clonic seizures, used ASM monotherapy, and never had status epilepticus. Sex differed significantly: the long-term group had fewer males (44% (19/43)) than the medium-term group (78% (25/32), p=0.003); other group comparisons were not significant.
The reasons for stopping ASM varied. Most patients discontinued first-line monotherapy with levetiracetam or valproic acid (62% short-term, 69% medium-term, 49% long-term). Median seizure-free time before withdrawal was 6.4 months (Interquartile range (IQR) 4.7–9.6) for short-term, 16.5 months (IQR 13.6–19.4) for medium-term, and 40.6 months (IQR 32.6–52.0) for long-term. Median time from first seizure to withdrawal increased from 15.9 months (IQR 8.3–24.4) in the short-term to 62.1 months (IQR 45.0–101.9) in the long-term group. Median progression-free survival was 38.8 months (95% confidence interval (CI) 13.4–64.2) short-term, 80.7 months (95% CI 45.4–116.0) medium-term, and 121.1 months (95% CI 102.2–140.1, p=0.015) long-term. By tumour grade, median progression-free survival (PFS) was 93.5 months (IQR 59.8–127.3) for grade 2, 116.1 months (IQR 83.7–148.5) for grade 3, and 34.6 months (IQR 13.9–55.3 p=0.025) for grade 4 glioma. During follow-up, 12% (4/34) short-term, 6% (2/32) medium-term, and 9% (4/43) long-term patients received additional antitumour treatment.
Within 36 months, recurrent seizures occurred in 47% (16/34) short-term, 31% (10/32) medium-term, and 44% (19/43) long-term patients. The 12-month cumulative incidence was 31% (95% CI 16–47%) short-term, 17% (95% CI 6–32%) medium-term, and 27% (95% CI 15–42%, p=0.345) long-term. Recurrent seizure risk did not differ significantly between short- and medium-term (adjusted hazard ratio (aHR)=0.65 (95% CI 0.29–1.46)) or short- and long-term groups (aHR=1.04 (95% CI 0.52–2.09)). Tumour progression at seizure recurrence was similar across groups (19% short-term, 30% medium-term, 16% long-term, p=0.653). By glioma grade, 39% (36/92) of grade 2/3 and 53% (9/17) of grade 4 patients had a recurrence; the 12-month cumulative incidence was 22% (95% CI 14–31%) for grade 2/3 and 42% (95% CI 18–64%, p=0.058) for grade 4. Risk of recurrence was higher in grade 4 glioma (unadjusted hazard ratio (uHR)=3.01 (95% CI 1.47–6.17)), with tumour progression more common at recurrence (56% grade 4 vs. 11% grade 2/3, p=0.003).
Most patients restarted ASM within 3 months of a recurrent seizure: 73% (11/15) short-term, 90% (9/10) medium-term, and 79% (15/19) long-term; delays were mostly due to patient concerns. The 12-month cumulative incidence of restarting ASM was 21% (95% CI 9–37%) short-term, 17% (95% CI 6–32%) medium-term, and 25% (95% CI 13–39%) long-term. There were no significant differences in restart rates between groups (short- vs. medium-term aHR=0.88 (95% CI 0.37–2.06); short- vs. long-term aHR=1.36 (95% CI 0.64–2.91)). ASM was restarted in 86% (31/36) of grade 2/3 and 89% (8/9) of grade 4 patients.[25]
Effect of lacosamide on seizure control and quality of life in patients with brain tumors
Rudà R et al. studied a total of 93 patients from 24 sites in Italy, the UK, the Netherlands, Germany, France, and Spain; all received at least one dose of lacosamide (SS). Seventy-nine patients (84.9%) completed the study; 14 (15.1%) discontinued. The full analysis set (FAS) included 87 patients. All but one patient received ≤400 mg/day of lacosamide.
Patients had a mean age of 44.5 (Standard deviation (SD) 14.7) years; only one was younger than 18. Median time since tumor diagnosis was 2 years, with 75.3% having a Karnofsky score >80. Most had low-grade glioma (84; 90.3%); other diagnoses included grade 3 glioma, suspected glioma (3), meningioma (3), craniopharyngioma (1), and unverified tumor (1). During treatment, 20.4% received antineoplastic therapy, 16.1% radiotherapy, and 8.6% had surgery. Median baseline seizure frequency was five per 28 days (range 1–280). All were on antiepileptic drugs (AEDs) at baseline, mostly levetiracetam monotherapy (48.4%).
In the FAS, 86 patients had seizure data: 76.7% were 50% responders, and 34.9% were seizure-free at 6 months. Median change in seizure frequency per 28 days was −2.9 (Q1–Q3: −9.1, -0.9); median percent change was 85.2% (−100, -55.5). In the SS (N=93), 71.0% were 50% responders and 32.3% seizure-free; seven patients had missing data.
In the FAS, 64.5% (49/76) improved on PGIC, 22.4% had no change, and 13.2% worsened; clinician global impression of change (CGIC) showed 64.2% (52/81) improved, 23.5% no change, and 12.3% worsened. In the SS, patient global impression of change (PGIC) showed 52.7% improved, 18.3% no change, and 10.8% worsened (18.3% missing); CGIC showed 55.9% improved, 20.4% no change, and 10.8% worsened (12.9% missing).
Among 80 patients with confirmed low-grade glioma, 75.0% were responders and 33.8% seizure-free; 65.3% improved on PGIC, 20.8% had no change, and 13.9% worsened. Of 33 patients with tumor treatment, 81.8% were responders and 36.4% seizure-free; without tumor treatment (n=53), 73.6% were responders and 34.0% seizure-free. PGIC improvement was similar (63.3% with treatment; 65.2% without).
In the FAS, mean (SD) changes at 6 months were: EuroQol 5 dimensions, 5 levels (EQ-5D-5L), +1.3 (16.4); utility score, −0.01 (0.20). MD Anderson symptom inventory–brain tumor module (MDASI-BT) changes were core severity, +0.1 (1.3); module severity, −0.1 (1.6); total severity, 0.0 (1.2); mean interference, −0.5 (2.4).
At month 6, 67.8% in the FAS and 63.4% in the SS remained on lacosamide. Kaplan-Meier estimated 6-month retention was 92.0% (95% CI 86.2–97.7) for the FAS and 86.0% (95% CI 79.0–93.1) for the SS. In the SS, 7.5% discontinued due to lack of effectiveness (5.4% ADR; 2.2% lack of efficacy); in the FAS, 5.7% discontinued (3.4% ADR; 2.3% lack of efficacy).[26]
Effect of adjunctive perampanel (PER) on seizure burden and patient outcomes in brain tumor–related epilepsy
According to the study conducted by Maschio et al., 26 BTRE patients were enrolled with focal seizures (16 males, mean age 47.5 years): 8 low-grade gliomas, 8 high-grade gliomas, 7 glioblastomas, 2 meningiomas, and 1 metastasis. Eleven were on AED monotherapy (PB:1, LTG:1, OXC:1, ZNS:1, LEV:7) and 15 on polytherapy. During follow-up, 16 received chemotherapy and 11 radiotherapy; no other treatments changed. Disease progression was observed in 11 patients (42.3%).
Five patients dropped out: 3 due to disease progression, 2 due to side effects (aggressiveness; vertigo/aggressiveness). The mean daily PER dose was 6.6 mg in the 21 who completed follow-up and 6.4 mg in the intention-to-treat (ITT) group.
In the 21 who completed 6 months, mean monthly seizures dropped from 10.8 ± 15.03 to 1.7 ± 4.34 (p=0.01). In the ITT population (26 patients, last follow-up 2.4 months), seizures reduced from 10.6 ± 14.27 to 2.3 ± 5.3 (p=0.004). The 6-month responder rate was 95.2%: seven were seizure-free, 13 had ≥50% reduction, and one was stable.
Quality of life (QOLIE) scores in 14 patients showed no significant change (baseline 61.2 ± 18.1 vs. 64.5 ± 20.7; p=0.42). Neuropsychological tests in nine patients also showed no significant differences, remaining within normal ranges. Mood evaluation (Symptom checklist (SCL-90)) in nine patients showed a significant decrease in psychosomatic symptoms (0.70 ± 0.4 to 0.47 ± 0.4; p=0.05) but no other significant changes. AEP scores showed no significant difference (45.0 ± 12.4 to 41.7 ± 12.3; p=0.14).
No significant correlations were found between seizure reduction and tumor histology (p=0.73), surgery extent (p=0.47), chemotherapy (p=0.21), radiotherapy (p=0.61), progression (p = 0.65), isocitrate dehydrogenase (IDH)1 status (p=0.77), or O6-Methylguanine-DNA methyltransferase (MGMT) methylation (p=0.95).
Between 1996 and 2013, 46 patients underwent brain surgery; 19 were excluded: two were older than 19 years, eight lacked confirmed neoplastic pathology, two had follow-up under one year, four did not have refractory epilepsy, and three had incomplete records. Thus, 27 patients were included.[27]
Effect of surgery on seizure control and AEDs withdrawal
Bernardino MR et al. demonstrated that before surgery, patients used an average of 3.6 AEDs; at surgery, this decreased to 2.1 drugs. Clinical characteristics, seizure details, drug regimens, and associated lesions. Invasive monitoring was used in two patients (7.4%), electrocorticography in 10 (37%), and motor area monitoring in two (7.4%). Resection was complete in 24 patients (88.8%); two had partial resection to preserve motor areas, and one with an anaplastic oligodendroglioma had incomplete resection due to tumor infiltration. Eleven patients (40.7%) underwent lesionectomy, seven (26%) extended lesionectomy, and nine (33.3%) temporal lobectomy with mesial structures removed.
Transient neurological deficits occurred in five patients (18.5%): headache and hemiparesis (1), hemiparesis (2), cranial nerve VI and VII paresis (1), and neuralgic headache (1). Tumor recurrence occurred in three patients (11.1%) requiring reoperation. One patient (3.7%) developed osteomyelitis, the only surgical complication. No intraoperative deaths occurred; one patient (3.7%) died two years post-op due to a high-grade tumor.
Mean seizure follow-up was 6.8 years (range 1.6–14.1). Only the first five years were analysed due to patient attrition. At one year, 25/27 patients were Engel class I; at five years, 19/21 remained class I. The two non-responders had the highest preoperative seizure frequency. Five patients (two gangliogliomas, three dysembryoplastic neuroepithelial tumors (DNETs)) had focal cortical dysplasia; all but one remained class I, with one relapsing to class IV by year ten.
Sixteen patients (59.2%) began AED withdrawal post-surgery; mean time to start was 3.2 years, median two years (range 1.7–7 years). Of these, 12 (44.4%) became drug-free, two (7.4%) remained in withdrawal with monotherapy, and two (7.4%) failed withdrawal due to seizure recurrence.[28]
Effect of levetiracetam vs valproic acid on treatment failure in brain tumor epilepsy
According to the study by van der Meer PB et al., out of 1,435 patients, 776 were treated with levetiracetam and 659 with valproic acid; 30% (437/1,435) required anticonvulsant polytherapy: 21% (302) received duo therapy (mainly levetiracetam plus valproic acid), 9% (126) triple therapy (commonly adding clobazam), and 1% (9) quadruple therapy. Treatment was stopped due to intolerable adverse effects in 18% (253) once, 6% (87) twice, and 1% (19) three times. A total of 858 patients were matched into two groups of 429. Non-matched patients were younger, had more surgeries, radiotherapy, systemic therapy, and psychiatric histories. First seizures occurred before histological diagnosis in 80% (687/858). Median overall survival did not differ significantly: 26.7 months (95% CI 21.4–32.0) for levetiracetam vs 26.9 months (95% CI 21.6–32.2) for valproic acid (p=0.699); median follow-up was 86.2 months (95% CI 76.2–96.2).
Treatment failure within 36 months occurred in 40% (173/429) of levetiracetam patients and 59% (253/429) of valproic acid patients, mainly due to uncontrolled seizures (19% vs 32%) or adverse effects (16% vs 17%). The cumulative incidence of treatment failure was significantly lower for levetiracetam (12 months: 33% vs 50%; p<0.001). Failure due to uncontrolled seizures (12 months: 16% vs 28%; p < 0.001) and other reasons (12 months: 3% vs 7%; p=0.004) favoured levetiracetam. No significant difference was found for failure due to adverse effects or seizure remission. Adverse effect failure was higher in females (19% vs 12%; p=0.043). Median dosage at failure for uncontrolled seizures was higher for levetiracetam (2,000 mg) than valproic acid (1,500 mg; p=0.005). No significant associations were found with MGMT status, tumor progression, or chemotherapy use.
Second-line monotherapy favoured levetiracetam over valproic acid for cumulative failure (12 months: 26% vs 44%; 36 months: 36% vs 66%; p=0.007). Tumor grade, temporal or frontal lobe involvement showed no significant differences. Recurrent seizure incidence was lower for levetiracetam (12 months: 54% vs 67%; p<0.001), with no differences by tumor grade or location.
Treatment failure due to adverse effects occurred in 69 levetiracetam patients (110 events) and 75 valproic acid patients (116 events). Common adverse effects were agitation (19%) for levetiracetam and decreased platelets (14%) for valproic acid. Psychiatric adverse effects caused failure in all four levetiracetam patients with psychiatric history, but none on valproic acid. Grade 3/4 events and unresolved side effects were similar between groups.[29]
| Parameter | Study/Author | ||||
| Timing of ASM discontinuation | Lacosamide | Perampanel | Surgery | LEV vs VPA | |
| van der Meer PB et al.[25] | Rudà R et al.[26] | Maschio M et al.[27] | Bernardino MR et al.[28] | van der Meer PB et al.[29] | |
| Sample size | 109 patients | 93 enrolled (87 FAS) | 26 enrolled (21 completed) | 27 patients | 1,435 patients |
| Patient population | Glioma patients stopping ASM | Brain tumor-related epilepsy | BTRE with focal seizures | BTRE with surgery | Brain tumor epilepsy (matched) |
| Mean age (years) | Mostly >40 years | 44.5 (SD 14.7) | 47.5 | Not stated | Not stated |
| Tumor grade | Mostly Grade 2 gliomas | Mostly low-grade gliomas (90%) | Mixed: LGG, HGG, GBM | Various low-grade tumors | Mixed grades |
| Intervention | ASM withdrawal at various times | Lacosamide adjunctive therapy | Perampanel adjunctive | Tumor resection | Levetiracetam vs Valproic Acid |
| Seizure-free rate | Not fully seizure-free: Recurrence: 31–47% at 36 months | 34.9% seizure-free at 6 months | 33% seizure-free at 6 months | 88% Engel Class I at 1 yr | Failure due to seizures: 19% LEV vs 32% VPA |
| Responder rate (≥50% reduction) | – | 76.7% (FAS), 71% (SS) | 95.2% | Not reported | – |
| Seizure recurrence | 31–47% within 36 mo (higher in short-term & Grade 4) | – | Reduction from 10.6 to 2.3/months (p=0.004) | Two patients relapsed at 5 years | 40% LEV vs 59% VPA treatment failure |
| Tumor progression at recurrence | 11% Grade 2/3 vs 56% Grade 4 | – | 42% disease progression | 11% recurrence requiring reoperation | Not associated with treatment failure |
| Quality of life impact | Not reported | PGIC improved by 64.5% | QOLIE-31 no significant change | Not reported | Not reported |
| Adverse events (AEs) | Not specified | 5.4% discontinued due to AEs | 2 dropouts due to AEs | 1 surgical complication (osteomyelitis) | 18% stopped due to intolerable AEs (both groups) |
| Conclusion | Recurrence risk is higher if seizure-free <12 months; Grade 4 gliomas are at higher risk | Good retention (92% at 6 months, significant seizure reduction | Strong seizure reduction, no major QoL change | The majority achieved long-term seizure control | LEV had significantly lower treatment failure than VPA |
Table 1: Summary of included clinical studies
Discussion
Effective seizure management in patients with brain tumors requires balancing seizure control, treatment side effects, and overall quality of life. The study by van der Meer PB et al. highlights that the timing of ASM discontinuation significantly influences seizure recurrence risk.[30] While longer seizure-free intervals before withdrawal were associated with longer progression-free survival, recurrence rates within three years remained high across groups, 47% for short-term, 31% for medium-term, and 44% for long-term, emphasizing the ongoing risk, especially for patients with high-grade gliomas who showed greater recurrence and tumor progression at relapse.
Similarly, the comparative study on levetiracetam vs valproic acid, also by van der Meer PB et al., demonstrated that levetiracetam had a significantly lower treatment failure rate than valproic acid, mainly due to fewer uncontrolled seizures, although adverse effects led to discontinuation in both groups. These results underscore the importance of agent selection, particularly when balancing seizure control and tolerability.
Expanding therapeutic options, Rudà R et al. found that lacosamide provided meaningful seizure reduction, over 75% of patients were responders, and about a third achieved seizure freedom at six months with stable quality of life and high treatment retention. This reinforces lacosamide’s potential as a well-tolerated adjunct or alternative in tumor-related epilepsy. In line with this, Maschio M et al. reported a striking 95% responder rate and significant seizure reduction with adjunctive perampanel among patients with diverse brain tumors. However, improvements in quality of life were less pronounced, suggesting that while seizure burden can be lowered, broader supportive care remains critical.
Surgical management continues to play a pivotal role. In the study on surgery outcomes, gross total or extended resections resulted in high rates of long-term seizure freedom, with over 70% maintaining Engel class I status at five years. Importantly, more than half of patients attempted ASM withdrawal post-surgery, and nearly half successfully discontinued medication entirely, highlighting the potential for surgery to not only control seizures but also reduce lifelong dependence on ASMs.
Collectively, these findings illustrate that optimal seizure management in brain tumor patients demands an individualized, multidisciplinary approach. Careful selection of ASM, timing of withdrawal, use of newer agents like lacosamide and perampanel, and appropriate surgical intervention must be tailored to tumor type, progression risk, and patient-specific factors to balance seizure control, treatment burden, and quality of life.
Conclusion
Epileptic seizures remain one of the most significant challenges in brain tumor management, profoundly affecting patients’ quality of life and functional independence. Evidence across studies highlights that while newer-generation ASMs like levetiracetam, lacosamide, and perampanel show promising seizure control with acceptable tolerability, treatment decisions must be carefully individualized to minimize adverse effects and drug interactions with oncologic therapies. Surgical resection offers durable seizure freedom for many, allowing some patients to discontinue medication altogether. However, the risk of recurrence after ASM withdrawal remains notable, especially in high-grade tumors. Ultimately, successful seizure management in brain tumor patients requires a patient-centered, multidisciplinary approach, balancing optimal tumor control, seizure suppression, and preservation of neurocognitive function and quality of life.
References
- Le VT, Nguyen AM, Pham TA et al. Tumor-related epilepsy and post-surgical outcomes: tertiary hospital experience in Vietnam. Sci Rep. 2023;13(1):10859. doi:10.1038/s41598-023-38049-1
PubMed | Crossref | Google Scholar - Prakash O, Lukiw WJ, Peruzzi F et al. Gliomas and seizures. Med Hypotheses. 2012;79(5):622-626. doi:10.1016/j.mehy.2012.07.037
PubMed | Crossref | Google Scholar - Mader MM, Deuter D, Sauvigny T, et al. Diffusion tensor imaging changes in patients with glioma-associated seizures. J Neurooncol. 2022;160(2):311-320. doi:10.1007/s11060-022-04139-9
PubMed | Crossref | Google Scholar - Berntsson SG, Merrell RT, Amirian ES, et al. Glioma-related seizures in relation to histopathological subtypes: a report from the glioma international case-control study. J Neurol. 2018;265(6):1432-1442. doi:10.1007/s00415-018-8857-0
PubMed | Crossref | Google Scholar - Ollila L, Roivainen R. Antiseizure medication choice in diffuse glioma: A single-center population-based experience. Epilepsia Open. 2025;10(3):705-716. doi:10.1002/epi4.70007
PubMed | Crossref | Google Scholar - Klein M, Engelberts NH, van der Ploeg HM et al. Epilepsy in low-grade gliomas: the impact on cognitive function and quality of life. Ann Neurol. 2003;54(4):514-520. doi:10.1002/ana.10712
PubMed | Crossref | Google Scholar - Blond BN, Detyniecki K, Hirsch LJ. Assessment of Treatment Side Effects and Quality of Life in People with Epilepsy. Neurol Clin. 2016;34(2):395-viii. doi:10.1016/j.ncl.2015.11.002
PubMed | Crossref | Google Scholar - Spina E, Pisani F, Perucca E. Clinically significant pharmacokinetic drug interactions with carbamazepine. An update. Clin Pharmacokinet. 1996;31(3):198-214. doi:10.2165/00003088-199631030-00004
PubMed | Crossref | Google Scholar - Newton HB, Wojkowski J. Antiepileptic Strategies for Patients with Primary and Metastatic Brain Tumors. Curr Treat Options Oncol. 2024;25(3):389-403. doi:10.1007/s11864-024-01182-8
PubMed | Crossref | Google Scholar - Ogunsakin O, Tumenta T, Louis-Jean S, et al. Levetiracetam Induced Behavioral Abnormalities in a Patient with Seizure Disorder: A Diagnostic Challenge. Case Rep Psychiatry. 2020;2020:8883802. doi:10.1155/2020/8883802
PubMed | Crossref | Google Scholar - Happold C, Gorlia T, Chinot O, et al. Does Valproic Acid or Levetiracetam Improve Survival in Glioblastoma? A Pooled Analysis of Prospective Clinical Trials in Newly Diagnosed Glioblastoma. J Clin Oncol. 2016;34(7):731-739. doi:10.1200/JCO.2015.63.6563
PubMed | Crossref | Google Scholar - Kerkhof M, Dielemans JC, van Breemen MS et al. Effect of valproic acid on seizure control and on survival in patients with glioblastoma multiforme. Neuro Oncol. 2013;15(7):961-967. doi:10.1093/neuonc/not057
PubMed | Crossref | Google Scholar - Khalili BF, Walbert T, Horbinski C, et al. Levetiracetam and valproic acid in glioma: antiseizure and potential antineoplastic effects. Future Oncol. 2025;21(4):483-491. doi:10.1080/14796694.2025.2450215
PubMed | Crossref | Google Scholar - Zeng Y, Wu X. Efficacy and tolerability of perampanel: a Chinese real-world observational study in epilepsy. Front Neurol. 2024;14:1286276. doi:10.3389/fneur.2023.1286276
PubMed | Crossref | Google Scholar - Thijs RD, Surges R, O’Brien TJ, Sander JW. Epilepsy in adults. Lancet. 2019;393(10172):689-701. doi:10.1016/S0140-6736(18)32596-0
PubMed | Crossref | Google Scholar - Jaafar F, Wazne J, Hmaimess G, et al. Prospective study of epilepsy with generalized tonic-clonic seizures alone: Clinical features, response to treatment, and likelihood of medication withdrawal. Epilepsia Open. 2024;9(4):1426-1436. doi:10.1002/epi4.12981
PubMed | Crossref | Google Scholar - Perucca P, Scheffer IE, Kiley M. The management of epilepsy in children and adults. Med J Aust. 2018;208(5):226-233. doi:10.5694/mja17.00951
PubMed | Crossref | Google Scholar - Moosa ANV. Antiepileptic Drug Treatment of Epilepsy in Children. Continuum (Minneap Minn). 2019;25(2):381-407. doi:10.1212/CON.0000000000000712
PubMed | Crossref | Google Scholar - Montori VM, Ruissen MM, Hargraves IG et al., Shared decision-making as a method of care. BMJ Evid Based Med. 2023;28(4):213-217. doi:10.1136/bmjebm-2022-112068
PubMed | Crossref | Google Scholar - Rektor I. Perampanel, a novel, non-competitive, selective AMPA receptor antagonist as adjunctive therapy for treatment-resistant partial-onset seizures. Expert Opin Pharmacother. 2013;14(2):225-235. doi:10.1517/14656566.2013.754883
PubMed | Crossref | Google Scholar - Seidel S, Wehner T, Miller D, et al. Brain tumor related epilepsy: pathophysiological approaches and rational management of antiseizure medication. Neurol Res Pract. 2022;4(1):45. doi:10.1186/s42466-022-00205-9
PubMed | Crossref | Google Scholar - Skaga E, Skretteberg MA, Johannesen TB, et al. Real-world validity of randomized controlled phase III trials in newly diagnosed glioblastoma: to whom do the results of the trials apply?. Neurooncol Adv. 2021;3(1):vdab008. doi:10.1093/noajnl/vdab008
PubMed | Crossref | Google Scholar - Vacher E, Rodriguez Ruiz M, Rees JH. Management of brain tumour related epilepsy (BTRE): a narrative review and therapy recommendations. Br J Neurosurg. 2025;39(1):4-11. doi:10.1080/02688697.2023.2170326
PubMed | Crossref | Google Scholar - Balestrini S, Mei D, Sisodiya SM et al. Steps to improve precision medicine in epilepsy. Mol Diagn Ther. 2023;27(6):661-672. doi:10.1007/s40291-023-00676-9
PubMed | Crossref | Google Scholar - van der Meer PB, Dirven L, Fiocco M, et al. Impact of timing of antiseizure medication withdrawal on seizure recurrence in glioma patients: a retrospective observational study. J Neurooncol. 2023;164(3):545-555. doi:10.1007/s11060-023-04450-z
PubMed | Crossref | Google Scholar - Rudà R, Houillier C, Maschio M, et al. Effectiveness and tolerability of lacosamide as add-on therapy in patients with brain tumor-related epilepsy: Results from a prospective, noninterventional study in European clinical practice (VIBES). Epilepsia. 2020;61(4):647-656. doi:10.1111/epi.16486
PubMed | Crossref | Google Scholar - Maschio M, Zarabla A, Maialetti A, et al. Perampanel in brain tumor-related epilepsy: Observational pilot study. Brain Behav. 2020;10(6):e01612. doi:10.1002/brb3.1612
PubMed | Crossref | Google Scholar - Bernardino MR, Funayama C, Hamad AP, et al. Refractory epilepsy in children with brain tumors. The urgency of neurosurgery. Arq Neuropsiquiatr. 2016;74(12):1008-1013. doi:10.1590/0004-282X20160157
PubMed | Crossref | Google Scholar - van der Meer PB, Dirven L, Fiocco M, et al. First-line antiepileptic drug treatment in glioma patients with epilepsy: Levetiracetam vs valproic acid. Epilepsia. 2021;62(5):1119-1129. doi:10.1111/epi.16880
PubMed | Crossref | Google Scholar - Avila EK, Tobochnik S, Inati SK, et al. Brain tumor-related epilepsy management: A Society for Neuro-oncology (SNO) consensus review on current management. Neuro Oncol. 2024;26(1):7-24. doi:10.1093/neuonc/noad154
PubMed | Crossref | Google Scholar
Acknowledgments
Not applicable
Funding
Not applicable
Author Information
Corresponding Author:
Samatha Ampeti
Department of Pharmacology
University college of Pharmaceutical Sciences, Kakatiya University, Warangal, India
Email: [email protected]
Co-Authors:
Sonam Shashikala BV, Mansi Srivastava, Shubham Ravindra Sali, Patel Nirali Kirankumar, Raziya Begum Sheikh
Independent Researcher
Department of Content, medtigo India Pvt Ltd, Pune, India
Authors Contributions
All authors contributed to the conceptualization, investigation, and data curation by acquiring and critically reviewing the selected articles. they were collectively involved in the writing – original draft preparation and writing – review & editing to refine the manuscript. Additionally, all authors participated in the supervision of the work, ensuring accuracy and completeness. The final manuscript was approved by all named authors for submission to the journal.
Ethical Approval
Not applicable
Conflict of Interest Statement
None
Guarantor
None
DOI
Cite this Article
Sonam SBV, Samatha A, Mansi S, Shubham RS, Patel NK, Raziya BS. Seizures in Brain Tumour. medtigo J Neurol Psychiatry. 2025;2(1):e3084216. doi:10.63096/medtigo3084216 Crossref













