






 Author Affiliations
Author Affiliations
Abstract
Background: Adolescent pregnancy and childbirth are serious social and public health concerns that have a negative impact on maternal health. Newborns born to adolescent mothers have a higher risk of death in their first year of life. Hence, the objective of this study was to analyse the promising strategies and best practices influencing adolescent mothers’ utilization of maternal health care in Nigeria and other similar settings in Africa.
Methods/Design: This study employs a literature review approach, sourcing data from peer-reviewed journals, grey literature, and secondary reports. A comprehensive search strategy incorporating keywords related to promising strategies and best practices influencing adolescent mothers’ utilization of maternal health care was employed. The geographical focus extends to West African countries with similar contexts.
Results: Several promising strategies and best practices were identified, including the Basic Healthcare Provision Fund (BHCPF), the Midwife Service Scheme (MSS), the Subsidy Reinvestment and Empowerment Programme (SURE-P), Maternal and Child Health (MCH), Community-Based Health Insurance Scheme (CBHIS), Community Health Education Programs (CHEP), and the OMOMi App. These initiatives prioritize underserved populations, aiming to enhance maternal health-seeking behaviour and maternal healthcare service utilization.
Discussion: While these strategies show promise in improving maternal health outcomes among pregnant mothers, including adolescent mothers, sustained efforts, adequate funding mechanisms, and consistent implementation are crucial for lasting progress in reducing maternal mortality and enhancing maternal well-being in Nigeria and similar African settings.
Conclusion: Adolescent pregnancy and its associated health challenges require adolescent-friendly comprehensive strategies and best practices to promote maternal health-seeking behaviour and the utilization of maternal healthcare services (MHS).
Keywords
Adolescent mothers, Maternal healthcare services, Best practices, Nigeria, Maternal mortality ratio.
Introduction
Adolescent pregnancy and childbirth are serious social and public health concerns that have a negative impact on maternal health. Adolescent mothers, for instance, are more likely to have fatal pregnancy problems.[1-4] Compared to women between 20 and 24 years old, they have a 1.5 times higher risk of dying during delivery.[2-4] Due to their higher risk of illness than newborns of older mothers, children born to them are more likely to die before their first birthday.[5-8] Additionally, the majority of adolescent women who have young children drop out of school, which puts them at higher risk for future unemployment and poverty.[9]
An important metric of maternal health is the maternal mortality ratio (MMR).[4,10,11] The Nigerian government and some agencies have done a lot to reduce MMR in Nigeria; however, MMR is still high.[12-17] There are no precise statistics on adolescent MMR in Nigeria due to the inclusion of adolescents with women of reproductive age.[18,19] Furthermore, with approximately 6,202 deaths recorded, or almost 31% of deaths per 100,000 girls documented in 2018, pregnancy-related complications are the first main cause of mortality among teenage mothers worldwide and the third leading cause of death in Nigeria.[20,21]
The majority of these pregnancy-related problems may be avoided, and it has been demonstrated that receiving MHS results in better maternal health outcomes.[20-22]
MHS: It includes antenatal care (ANC), skilled birth delivery, and postnatal care (PNC).[23,24] ANC helps identify risks and complications associated with pregnancy and provides information about their management.[25] The use of ANC predicts skilled birth delivery and PNC, meaning a woman who registered and used ANC is likely to have skilled birth delivery and follow-up for PNC.[26-28]
Adolescent mothers who attend ANC by skilled birth attendants will possibly have enough information about the significance of skilled birth delivery. Consequently, it is an essential approach for reducing maternal mortality.[29-31] However, this age group is said to exhibit very poor maternal health-seeking behaviour. Research shows that even in places where the services are freely available and affordable, this age group exhibits very poor maternal health-seeking behaviour despite the elevated risk they confront.[3,5,32] In other words, the use of health facility services is not always guaranteed by their availability. Adolescent mothers will reduce the risk associated with their pregnancy and achieve better maternal health outcomes if they improve their health-seeking behaviour and increase their use of MHS as needed.
MHS coverage: According to the National Health Management Information System (NHMIS), ANC and PNC coverage are generally below the set national target (NT).[49,50]. The set NT for ANC and PNC coverage in Nigeria is 80%, while the NT for skilled birth attendance (SBA) is 57%. The recorded data for four ANC coverage ranges from 49.1% in 2016, 56.8% in 2018, 19.1% in 2020, and 15.1% in May 2021.[16,33-35]
For SBA coverage, the data shows an increase in SBA from 43.3% in 2018 to 90.4% in 2020 and 70.71% as of May 2021. Though the value is above 57 percent, which is the set NT for SBA coverage, the data might not be nationally representative because NHMIS data are service data that are mainly generated from government institutions, and important data from the private sector may be missing.[36]
Sustainable development goal (SDG): SDG 3.1 calls for every country to have no greater than 140 per 100,000 MMR towards a global reduction of MMR to less than 70 per 100,000 live births by 2030.[37,38] A satisfactory utilization of MHS is crucial in lowering maternal mortality and achieving the SDG 3 objective.[3,5,32,39] To effectively reduce maternal mortality to 70 per 100,000 live births by 2030, it is very necessary to analyse the successful strategies and best practices that impact adolescent mothers’ use of maternal health care in Nigeria and other similar settings in Africa.
Methodology
Information sources and search methods: The study used a review of the literature. Peer-reviewed journals were first extracted from the Elsevier and PubMed (Medline) databases. Afterwards, Google and Google Scholar were used to find peer-reviewed and grey literature (both published and unpublished), and snowballing was used to find papers about strategies and best practices that affect adolescent mothers’ usage of maternal health care.
Search strategies: Various keyword combinations were utilized by the researcher throughout the literature search. The target audience, promising strategies, and best practices were considered when searching for the key phrases utilizing Boolean operators. The search criteria were best practices that affect adolescent mothers’ use of maternal health care in Nigeria and other West African countries with comparable environments. The precise keywords and search tactics are shown in the annex below.
| Promising strategy and practices |
OR |
Keywords | Country/Region |
| BHCPF
Payment for performance (P4P) CBHIS CHEP SURE-P OMOMiApp
|
AND | ||
| “promising strategies”
“promising practices” “youth-friendly services” “adolescent-friendly services” “effective intervention” |
Nigeria
Ghana Rwanda Senega Malawi Kenya, Uganda West Africa Africa sub-Saharan Africa |
||
Table 1: Search terms and keywords for promising strategies and practices
Quality assessment and risk of bias: This study does have certain limitations. Because only English-language papers were reviewed, the study may include some linguistic bias. As a result, crucial information may be absent from African nations speaking other official languages but sharing comparable features. Additionally, only a few publications included information specifically for adolescents between the cited age ranges of 15 and 19. Finally, because the evaluation is based solely on information gathered from the literature that is already in circulation, the researcher is unable to verify the accuracy of the material they have gathered. Despite these limitations, this study’s merit resides in its capacity to further general understanding. Additionally, the use of various internationally recognized and country-specific secondary data reports ensured the validity of the results.
Results
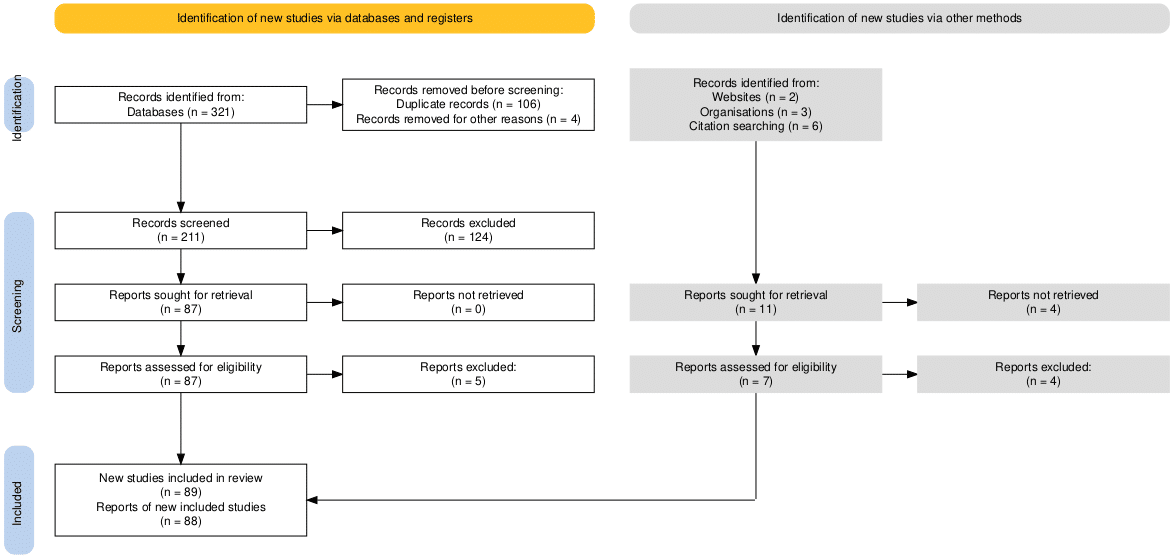
Figure 1: PRISMA 2020 Flow chart
Nearly all the discussed best practices to improve health-seeking behavior and utilization of MHS were generally for women of reproductive age (15-45), of which adolescent mothers are included.
BHCPF Nigeria: The BHCPF is funded by the federal and state governments of Nigeria. Former president Goodluck Jonathan ratified it in the National Health Bill in 2014, and President Muhammadu Buhari ratified it in the 2019 fiscal budget. It is a portion of the National Health Act of 2014 that seeks to enhance financing for the healthcare industry.[40-42]
BHCPF is the one per cent fund earmarked for health financing purposes from the federal government consolidated revenue fund (CRF), alongside contributions from the private sector and donors. This earmarked fund is allocated to the implementing gatekeepers at different percentages to purchase a basic minimum package of health services (BMPHS) for its citizens. Allocation of 50 per cent to the National Health Insurance Scheme (NHIS), 45 per cent to the National Primary Health Care Development Agency (NPHCDA), and the remaining 5 per cent to the National Emergency Medical Treatment Committee (NEMTC).[43,44]
The essential MHS covered by the basic package includes prenatal care, skilled delivery, and postpartum care; immunization and treatment for malaria, pneumonia, measles, and dysentery in children under five; treatment for malaria in adults; screenings for hypertension and diabetes; and family planning.
The BHCPF identity card is the sole requirement, and getting one is simple, as it is available at all licensed primary health centers (PHCs) across all 36 states of Nigeria, including the federal capital territory (FCT) of Abuja.[22,40-42]
BHCPF is a promising plan since it intends to provide free, minimal basic healthcare to the impoverished and most vulnerable people in Nigeria, intending to improve the country’s health system, achieve universal health coverage, and further improve health service indicators like the MMR.[12,45-47] Adolescent mothers would greatly benefit from this package, especially those who are vulnerable and underprivileged in rural regions. The success and sustainability of the programme, however, may be affected by the government’s poor political will, feeble financial management, and accountability, which can discourage donors from financially supporting the country’s healthcare system.[40,42,43,48,49]
P4P Rwanda: P4P, a financial performance incentive, encourages Rwandans to utilize mother and child health services more regularly.[50-52] P4P was launched nationally to increase worker productivity and commitment to improving mother and child health outcomes.[51,52]
It covers religious organizations as well as public and corporate entities. The number of reproductive, maternity, newborn, and child health (RMNCH) indicators that have improved determines the incentives that participating health facilities get. The importance of RMNCH is increased at the district and village levels by P4P, which compensates community health practitioners based on recommendations made.
The percentages of women giving birth and visiting hospitals, as well as the correct use of a partograph, are among the indicators. Using a database, users may also keep track of their objectives concerning the efficiency of other service providers. Additionally, systems for monitoring development and preventing corruption were put in place.
This strategy promotes competition between the institutions, improving health facility performance and reducing out-of-pocket expenses. Additionally, it improves the utilization of maternal healthcare, especially for expertly delivered newborns. The practices show a 23% increase in hospital-based birth deliveries among participating health facilities and an estimated standard deviation of 0.157 in ANC quality, according to Rwanda’s prenatal care practice guidelines.[50,51,53] Considering the accomplishments recorded with this program in African countries with similar characteristics, a great number of adolescent mothers would profit from it. The progress accomplished is not only dependent on P4P operations, because other concurrent initiatives in place pursue the same objective. This makes it difficult to attribute the success percentage (%) only to P4P initiatives.
CBHIS Nigeria: There are different ways through which insurance may improve MHS and maternal health outcomes. It reduces the cost of MHS and ensures affordability, thereby increasing the utilization of the MHS by pregnant women. In the long run, the increased use of MHS should help in reducing MMR.[54]
This voluntary program, called CBHIS, has been shown to effectively promote domestic resource pooling and avert catastrophic medical costs, especially for the underprivileged and the poor. The goal is to guarantee the availability and accessibility of services at reasonable prices, not to make a profit.[55] CBHIS offers complete disease coverage and has a standardized benefits package, particularly at the municipal level. It has the potential to foster community growth and provide systems for holding healthcare professionals accountable. In Senegal, however, there are differences in the coverage of MHS that are provided by the CBHI. Almost half of the scheme covers prenatal care, 60% covers normal birth, and 26% covers complex deliveries, including caesarean sections.
CBHI has been revealed to boost the use of skilled birth attendants and the demand for MHS. For instance, a study from Rwanda shows that CBHI-insured members were three (3) times more likely to deliver using an SBA than their uninsured counterparts, who possibly used home delivery. Other studies on CBHI schemes show evidence related to some African countries, such as Senegal, Mali, and Nigeria.[54,56-59]
A few African nations provided proof of the success of this plan.[49,56,59-67] For example, Rwanda, which increased its social insurance coverage from 3% to 91%, has one of the greatest systems in sub-Saharan Africa.[51,62] Ghana also employs social health insurance programs to make sure that all its inhabitants are insured. The program offers equal benefits and financial safety.[53,68] Also, CBHIS has historically been implemented with a 50% success rate in various states of Nigeria, including Lagos, Kwara, and Anambra.[55]
Financial sustainability is a challenge without sufficient community involvement due to the potential for default payments and poor participation in underprivileged groups. To make the effect more noticeable, the government may need to step in by subsidizing the payment for the underprivileged and vulnerable populations, including adolescent mothers.[53,67,69-71]
Community Health Education Programs (CHEP) Nigeria: In 96 randomly selected communities in the northern region, between 2013 and 2015, researchers conducted a study in collaboration with the Planned Parenthood Federation of Nigeria (PPFN) to determine the effects of community health education on the uptake of MHS and pregnancy outcomes. CHEP, Safe Birth Kits, CORPs, and Community Drama and CORPs are the three CHEP provides.[72]
Community health educator programmes: Community resource people (CORPs) will knock on the doors of pregnant women who relatives and neighbours have identified as needing this intervention. The resource person discusses the poor use of MHS, the lack of confidence that pregnant women have in medical professionals, the value of a healthy diet throughout pregnancy, and the advantages of a competent delivery.[72]
Safe birth kits and CORPs: This package guarantees a secure, sterile delivery setting and tools. To prevent infection during labour, assist the underprivileged, and allay concerns about the absence of delivery equipment at the facilities, the CORPs make sure that pregnant women in their third trimester receive sterile birth kits.[72]
Community drama and CORPs: A variety of dramas are also included in this package, in addition to the CORP program. The drama frequently makes social commentary regarding how men’s autonomy and the influence of mothers-in-law affect pregnant women’s decision-making and health-seeking behaviour. The drama aims to challenge societal conventions and dispel myths about birthing in facilities.[72]
As a result of these treatments, mothers’ attitudes and understanding of MHS improved in 2016. In areas that get the three sets of community education programs, the use of prenatal care is enhanced.
MSS Nigeria: To address the lack of human resources, the MSS was established in 2009 and entails the recruitment and placement of experienced birth attendants in underserved rural areas.[13-73-76] The initiative is overseen by the NPHCDA and is supported by a unique MDG-DRG (Debt Relief Gains) Account.[12,14,47,77,78]
To deploy newly qualified, jobless, and retired midwives to specific primary healthcare institutions in neglected rural regions, the 36 states of Nigeria signed a memorandum of understanding (MoU). The goal is to decrease mother and child mortality further and expand the use of SBA.[12,77]
With MSS initiatives, progress has been made. For instance, it increases the number of health professionals available in rural areas and enhances the general results for maternal health. [12,45,77,79] However, the program’s advantages have not been felt equally across the nation. This program has difficulties, including inadequate MoU implementation in certain states, midwives’ retention, and sustainability concerns. Additionally, the midwives were responsible for certain states putting the MoU into effect, which caused the majority to quit their jobs.
SURE-P: The SURE-P was set up by the Nigerian government as a follow-up initiative to MSS from October 2012 to April 2015. It covers both the supply and demand sides. It involves the recruitment and training of midwives, and community extension workers and the provision of necessary infrastructure to the accredited PHCs on the supply side, while on the demand side, it involves the introduction of conditional cash transfers (CCT) to pregnant mothers on the account that they register for ANC, have skilled birth delivery and attend PNC.[50,55,80]
SURE-P increased the Midwifery Service Scheme to lower maternal and infant mortality. The goal is to renovate or establish primary healthcare facilities, enhance secondary healthcare facilities to act as referral centres, increase demand for and use of services through CCT, and offer the much-needed human resources in neglected areas.[15,50,55,80,81]
One state from each geographical zone was used in the study to determine SURE-P’s benefits, and the results revealed that the initiative increased the number of prenatal visits and skilled deliveries in the institutions that were chosen. The program’s success is also credited to community engagement, which involves utilizing village health professionals to motivate women to have skilled births. Following the introduction of SURE-P, an evaluation revealed an improvement in maternal health indicators, including a jump of 32.1% in skilled birth deliveries and a 36.3% increase in the number of pregnant women attending four prenatal care consultations.[15,50,55,80,81]
OMOMi app Nigeria: MOBicure, a company using technology to solve serious health challenges in Nigeria, launched the OMOMi app. Omomi in the Yoruba language means “my child,” and it was launched to prevent maternal deaths in childbirth and help women with life-saving information from health professionals regarding their health and that of their child. The app is in use in Nigeria and has subscribers in many African countries, including Ghana, Tanzania, and Kenya.[82,83]
It provides women with pertinent information on maternal health, enhances maternal outcomes, and assists women in making educated decisions about their health and families. Additionally, considering Nigeria’s estimation of about 200 million mobile phone users and over 90 million subscribers at the end of January 2021, employing such an app in all parts of the country may be a successful tactic in getting pregnant adolescents to utilise MHS.[82-86]
However, because this software requires internet access, many moms, particularly those in rural regions, who may have benefited from it, may choose not to enroll because of their lack of knowledge and their financial situation.[82,87]
Discussion
As presented above Nigeria has made several initiatives to increase the use of maternity healthcare and decrease the MMR. The disadvantaged communities in certain states or geopolitical areas are the major benefactors of the strategies’ success rates. According to the reviews of the examined best practices, to significantly improve adolescent mothers’ health-seeking behaviour and use of maternal health care, combining one or two of these therapies that are adolescent-friendly and specifically directed towards adolescent mothers’ needs is necessary,
Most of the documented promising strategies and best practices were generally for women of reproductive age (15-45), which includes adolescent mothers, but not solely for adolescent mothers. Also, some of the presented strategies struggle with ineffective implementation, financial instability, poor political will for continuity and sustainability concerns. Officials must thus seek sustainable financing sources to ensure the program’s continuation. Also, the Adolescent-friendly MHS section needs to be put in place to meet adolescent-specific needs. In addition, the government may have to intervene by subsidizing the payment for the poor and vulnerable groups, especially Adolescent moms because they are more prone than older mothers to become unwell or even die while carrying a child.
The efforts to improve the use of maternal health care are promising since they are targeted at the disadvantaged population, but they are not long-term solutions. National programs that seek to provide access to quality reproductive health information and services for adolescents and young people never address the difficulties associated with inadequate utilization of maternal health care by adolescent mothers. Therefore, authorities need to bring back and scale up past initiatives that record successful increases in the use of MHS and investigate sustainable sources of funding existing ones to guarantee the durability of present initiatives.
The evaluated promising strategies and best practices highlight the potential to improve adolescent mothers’ use of MHS and their habit of seeking maternal health care. By giving disadvantaged and marginalized people priority, programs such as the BHCPF, the MSS, and the SURE-P Maternal and MCH have shown potential.
The BHCPF, MSS, and SURE-P MCH were best practices and successful programs to promote teenage mothers’ use of maternal health care in Nigeria. It tracks success rates while concentrating on impoverished and vulnerable groups. These findings support the assertions of academics like Abimbola et al., Abubarka and colleagues who contend that if there is enough political will and access to the necessary resources, the initiatives will significantly increase the uptake of MHS, decrease MMR, and improve maternal health outcomes in Nigeria.[77,88]
These methods provide insights into how tailored interventions might favourably affect the health-seeking behaviours of adolescent mothers; however, they are not without difficulties. It is crucial to stress that these programs’ long-term viability and efficacy depend on reliable funding sources, continuous application, and a persistent dedication to meeting the healthcare requirements of adolescent mothers. In other words, policymakers should be encouraged to sufficiently devote themselves to adolescent health as it has tremendous economic potential for Nigeria, considering this age group is youth with high productive power. They need to explore sustainable sources of generating funds to sustain the existing promising strategies to improve adolescent mothers’ utilization of MHS.
The National policies, maternal healthcare strategies and interventions to target adolescent mothers, especially those in underserved regions should be put in place to help reduce the inequity gap in accessing MHS and improve their health outcomes. Also, there should be an advocate for more capital spending on health and continuous release of earmarked funds for BHCPF at the primary health care.
Conclusion
In conclusion, while all stated strategies represent encouraging steps toward enhancing maternal health outcomes in Nigeria, MHS that are more specific to adolescent mothers’ needs are required. Continued efforts and deliberate investments will be required to achieve lasting progress in lowering maternal mortality and enhancing maternal well-being in the region.
References
- Alex-Ojei CA, Odimegwu CO, Ntoimo LFC. A qualitative investigation into pregnancy experiences and maternal healthcare utilisation among adolescent mothers in Nigeria. Reprod Health. 2023;20(1):1-12. doi.10.1186/s12978-023-01613-z PubMed | Crossref | Google Scholar
- World Health Organization. Adolescent pregnancy. WHO Fact Sheet. 2023. Adolescent pregnancy
- World Health Organization. Adolescent sexual and reproductive health and rights. World Health Organization. Sexual and Reproductive Health and Research (SRH)
- Folorunsho-Francis A. Nigeria’s maternal mortality rate worst in the world, Ehanire Healthwise. 2020. Nigeria’s maternal mortality rate worst in the world – Ehanire – Healthwise
- World Health Organization. Maternal mortality. 2023. Maternal mortality
- UNICEF. Maternal mortality rates and statistics. UNICEF Data. 2017. Maternal mortality rates and statistics – UNICEF DATA
- UNICEF. Child mortality. UNICEF Data. 2023. Child Mortality – UNICEF DATA
- Mekwunyei LC, Odetola TD. Determinants of maternal health service utilisation among pregnant teenagers in Delta State, Nigeria. Pan Afr Med J. 2020;37(81):1-17. Doi.10.11604/PAMJ.2020.37.81.16051 PubMed | Crossref | Google Scholar
- Idowu A, Olowookere SA, Abiola OO, Akinwumi AF, Adegbenro C. Determinants of skilled care utilization among pregnant women residents in an urban community in Kwara State, Northcentral Nigeria. Ethiop J Health Sci. 2017;27(3):291-298. doi.10.4314/ejhs.v27i3.11 PubMed | Crossref | Google Scholar
- Olonade O, Olawande TI, Alabi OJ, Imhonopi D. Maternal mortality and maternal health care in Nigeria: implications for socio-economic development. Open Access Maced J Med Sci. 2019;7(5):849. doi.10.3889/OAMJMS.2019.041 PubMed | Google Scholar
- Eto E. Government policy and initiatives on maternal mortality reduction in Nigeria. Electron Theses Diss.2016. “Government Policy and Initiatives on Maternal Mortality Reduction in N” by Enifome U. Eto
- Okpani AI, Abimbola S. The Midwives Service Scheme: A qualitative comparison of contextual determinants of the performance of two states in central Nigeria. Glob Health Res Policy. 2016;1(1):1-11. doi.10.1186/s41256-016-0017-4 PubMed | Crossref | Google Scholar
- Federal Government of Nigeria. Nigeria MNCH Country Summary, 2017. Nigeria MNCH Country Summary March 2017 1
- Guideline for the Administration, Disbursement and Monitoring of the Basic Healthcare Provision Fund. FMOH, Fed Repub Niger. 2020:1-71. PolicyVault.Africa | Guidelines for the Administration, Disbursement, Monitoring and Fund Management of the Basic Healthcare Provision Fund
- Federal Ministry of Health-Nigeria. Second National Strategic Health Plan: Ensuring Healthy Lives and Promoting the Well-being of the Nigerian Populace at All Ages. 2018. NSHDP-II-final-version-health-plan.pdf
- Federal Ministry of Health-Nigeria. MSDAT Platform. 2021. MSDAT Nigeria
- UNICEF Nigeria. The Situation of Women and Children in Nigeria.2020. Situation of women and children in Nigeria | UNICEF Nigeria
- Oyeyemi AL, Aliyu SU, Sa’ad F, et al. Association between adolescent motherhood and maternal and child health indices in Maiduguri, Nigeria: A community-based cross-sectional study. BMJ Open. 2019;9(3):e024017. doi.10.1136/bmjopen-2018-024017 PubMed | Crossref | Google Scholar
- Dafi M, Lackshman IM, Abeysinghe D, Jidda KI. Socio-cultural and health-seeking beliefs in maternal health care utilization among women in rural Nigeria. Int J Educ Soc Sci Res. 2018;1(1). (PDF) SOCIO-CULTURAL AND HEALTH-SEEKING BELIEFS IN MATERNAL HEALTH CARE UTILIZATION AMONG WOMEN IN RURAL NIGERIA | Semantic Scholar
- Odekunle FF. Maternal mortality burden: The influence of socio-cultural factors. Int J Health Sci Res. 2016;3(166):1-325. (PDF) Maternal Mortality Burden: The Influence of Socio-Cultural Factors Google Scholar
- Stephen AA, Joshua AO. Determinants of maternal utilization of health services and nutritional status in a rural community in southwest Nigeria. Afr J Reprod Health. 2016;20(2):72-85. doi.10.29063/ajrh2016/v20i2.8
PubMed | Crossref | Google Scholar - Akeju DO, Oladapo OT, Vidler M, et al. Determinants of health care-seeking behavior during pregnancy in Ogun State, Nigeria. Reprod Health. 2016;13(1):67-74. doi.10.1186/s12978-016-0139-7 PubMed | Crossref | Google Scholar
- Nuamah GB, Agyei-Baffour P, Mensah KA, et al. Access and utilization of maternal healthcare in a rural district in the forest belt of Ghana. BMC Pregnancy Childbirth. 2019;19(1):1-11. doi.10.1186/s12884-018-2159-5
PubMed | Crossref | Google Scholar - Rai RK, Singh PK, Singh L. Utilization of maternal health care services among married adolescent women: Insights from the Nigeria Demographic and Health Survey, 2008. Womens Health Issues. 2012;22(4):e407-e414. doi.10.1016/j.whi.2012.05.001 PubMed | Crossref | Google Scholar
- Mehari K, Wencheko E. Factors affecting maternal health care services utilization in rural Ethiopia: A study based on the 2011 EDHS data. Ethiop J Health Dev. 2013;27(1):16-24. doi.10.4314/EJHD.V27I1 Google Scholar
- Banke-Thomas OE, Banke-Thomas AO, Ameh CA. Factors influencing utilization of maternal health services by adolescent mothers in low- and middle-income countries: A systematic review. BMC Pregnancy Childbirth. 2017;17(1):1-14. doi.10.1186/s12884-017-1246-3 PubMed | Crossref | Google Scholar
- Mekonnen T, Dune T, Perz J. Maternal health service utilization of adolescent women in sub-Saharan Africa: A systematic scoping review. BMC Pregnancy Childbirth. 2019;19(1). doi.10.1186/s12884-019-2501-6
PubMed | Crossref | Google Scholar - Iacoella F, Tirivayi N. Determinants of maternal healthcare utilization among married adolescents: Evidence from 13 sub-Saharan African countries. Public Health. 2019;177:1-9. doi.10.1016/j.puhe.2019.07.002 PubMed | Crossref | Google Scholar
- Olayinka A, Joel A, Bukola D. Factors influencing utilization of antenatal care services among pregnant women in Ife Central LGA, Osun State, Nigeria. Adv Appl Sci Res. 2012;3(3):1309-1315. (PDF) Factors influencing utilization of antenatal care services among pregnant women in Ife Central Lga, Osun State Nigeria Google Scholar
- Adewemimo AW, Msuya SE, Olaniyan CT, Adegoke AA. Utilization of skilled birth attendance in Northern Nigeria: A cross-sectional survey. Midwifery. 2014;30:e7-e13. doi.10.1016/j.midw.2013.09.005 PubMed | Crossref | Google Scholar
- Olakunde BO, Adeyinka DA, Mavegam BO, et al. Factors associated with skilled attendants at birth among married adolescent girls in Nigeria: Evidence from the Multiple Indicator Cluster Survey, 2016/2017. Int Health. 2019;11(6):545-550. doi.10.1093/inthealth/ihz017 PubMed | Crossref | Google Scholar
- World Health Organization. Maternal mortality. WHO Fact Sheet. 2023. Maternal mortality
- Federal Ministry of Health. National RHP.2017. 9147562941489753121.pdf
- MSDAT Platform. 2021. MSDAT Nigeria
- Health Think Analytics. Adolescent pregnancies and its implications on the female child. Health Think Analytics. 2021. ADOLESCENT PREGNANCIES AND ITS IMPLICATIONS ON THE FEMALE CHILD – Health Think Analytics
- Oboko A. How lack of data, research hinders Nigeria healthcare system. Business Day NG. 2019. How lack of data, research hinders Nigeria healthcare system. Business Day NG
- World Health Organization. SDG Target 3.1: Maternal mortality By 2030, reduce the global maternal mortality ratio to less than 70 per 100,000 live births. WHO. 2023. SDG Target 3.1 | Maternal mortality: By 2030, reduce the global maternal mortality ratio to less than 70 per 100 000 live births
- UN Women. In focus: Women and the Sustainable Development Goals (SDGs): SDG 3-Good health and well-being. UN Women Headquarters. 2023. In focus: Women and the Sustainable Development Goals (SDGs): SDG 3: Good health and well-being | UN Women – Headquarters
- Lambonmung A, Acheampong CA, Langkulsen U. The effects of pregnancy: A systematic review of adolescent pregnancy in Ghana, Liberia, and Nigeria. Int J Environ Res Public Health. 2022;20(1). doi.10.3390/ijerph20010000
PubMed | Crossref | Google Scholar - Federal Ministry of Health, World Bank. Nigeria Basic Healthcare Provision Fund Project (The HUWE Project): Terms of reference for consultancy for external audit services to support the implementation of the BHCPF.2016 Nigeria – Basic Healthcare Provision Fund Project
- Premium Times. Basic Health Care Provision Fund: A slow start to a long journey. Premium Times.2021. Basic Health Care Provision Fund: A Slow Start to a Long Journey
- Makanjuola O, Van Vuuren U. How does BHCPF, Nigeria’s healthcare programme, work? ONE.2021. How does BHCPF, Nigeria’s healthcare programme, work? – ONE.org Africa
- Alawode G, Adewoyin AB, Abdulsalam AO, et al. The political economy of the design of the Basic Health Care Provision Fund (BHCPF) in Nigeria: A retrospective analysis for prospective action. Health Syst Reform. 2022;8(1). doi.10.1080/23288604.2022.2124601 PubMed | Crossref | Google Scholar
- The Official Gazette of the National Health Act. The Nigerian National Health Act. Off Gaz Natl Health Act.2014 Download The Official Copy Of The National Health Act 2014 (Pdf) – Public Health
- Okeke E, Abubakar IS, Pitchforth E, Setodji C. Better obstetrics in rural Nigeria: Evaluating the Midwives Service Scheme. Impact Evaluation Report 56. January 2017. doi.10.23846/ow41225 Google Scholar
- Abimbola S, Okoli U, Olubajo O, Abdullahi MJ, Pate MA. The Midwives Service Scheme in Nigeria. PLoS Med. 2012;9(5):e1001211. doi.10.1371/journal.pmed.1001211 PubMed | Crossref | Google Scholar
- World Health Organization. WHO | Nigeria Midwives Service Scheme. WHO. Maternal Health Unit
- Ibrahim ZA, Konlan KD, Moonsoo Y, et al. Influence of Basic Health Care Provision Fund in improving primary health care in Kano State: A descriptive cross-sectional study. BMC Health Serv Res. 2023;23(1):1-9. doi.10.1186/s12913-023-09708-w PubMed | Crossref | Google Scholar
- O O, F O, H I, et al. Assessment of a free maternal and child health program and the prospects for program re-activation and scale-up using a new health fund in Nigeria. Niger J Clin Pract. 2019;22(11):1516-1529. doi.10.4103/NJCP.NJCP_503_18 PubMed | Crossref | Google Scholar
- Nsofor IM, Ezeokoli AN, Akabike KO, Anya I, Ihekweazu C. An evaluation of the maternal and child health project of the Subsidy Reinvestment and Empowerment Programme (SURE-P MCH). EpiAfric. 2019 Microsoft Word – SURE P MCH FINAL REPORT_Final .docx
- Basinga P, Gertler PJ, Binagwaho A, Soucat AL, Sturdy J, Vermeersch CM. Effect on maternal and child health services in Rwanda of payment to primary health-care providers for performance: an impact evaluation. Lancet. 2011;377(9775):1421-1428. doi.10.1016/S0140-6736(11)60177-3 PubMed | Crossref | Google Scholar
- Rouyard T, Mano Y, Daff BM, et al. Operational and structural factors influencing enrolment in community-based health insurance schemes: An observational study using 12 waves of nationwide panel data from Senegal. Health Policy Plan. 2022;37(7):858-871. doi.10.1093/heapol/czac033 PubMed | Crossref | Google Scholar
- Nnamuchi O, Jude J, Uju O, Obuka B, Agu Helen Uchena. (PDF) Successes and Failures of Social Health Insurance Schemes in Africa-Nigeria versus Ghana and Rwanda: A Comparative Analysis. ResearchGate.2019;28(1):127-148. (PDF) Successes and Failures of Social Health Insurance Schemes in Africa-Nigeria versus Ghana and Rwanda: A Comparative Analysis Google Scholar
- Comfort AB, Peterson LA, Hatt LE. Effect of health insurance on the use and provision of maternal health services and maternal and neonatal health outcomes: A systematic review. J Heal Popul Nutr. 2013;31(4 SUPPL.2):81-105.
PubMed | Google Scholar - World Bank Group. Nigeria Subsidy Reinvestment and Empowerment Programme (SURE-P): Maternal and Child Health Initiative. 2016. Nigeria Subsidy Reinvestment and Empowerment Programme (SURE-P): Maternal and Child Health Initiative
- Ly MS, Faye A, Ba MF. Impact of community-based health insurance on healthcare utilisation and out-of-pocket expenditures for the poor in Senegal. BMJ Open. 2022;12(12):1-9. doi.10.1136/bmjopen-2022-063035
PubMed | Crossref | Google Scholar - Agbo I, Onajole A, Ogunnowo B, Emechebe A. Community based health insurance as a viable option for health financing: An assessment of household willingness to pay in Lagos, Nigeria. J Public Heal Epidemiol. 2019;11(2):49-57. doi.10.5897/jphe2018.1089 Crossref
- Aregbeshola BS. A Tax-based, Noncontributory, Health-Financing System Can Accelerate Progress toward Universal Health Coverage in Nigeria. MEDICC Rev. 2018;20(4):40-45. doi.10.37757/MR2018.V20.N4.9. Crossref
- Elmusharaf K, Byrne E, O’Donovan D. Strategies to increase demand for maternal health services in resource-limited settings: challenges to be addressed. BMC Public Heal. 2015;15(1):1-10. doi.10.1186/S12889-015-2222-3
PubMed | Crossref | Google Scholar - Onwujekwe O, Ezumah N, Mbachu C, et al. Exploring effectiveness of different health financing mechanisms in Nigeria; what needs to change and how can it happen? BMC Health Serv Res. 2019;19(1):661. doi.10.1186/s12913-019-4512-4 PubMed | Crossref | Google Scholar
- Chankova S, Atim C, Hatt L. Ghana’s National Health Insurance Scheme. In: The Impact of Health Insurance in Low- and Middle-Income Countries. 2010:58-88. Ghana’s National Health Insurance Scheme (NHIS) Google Scholar
- Chemouni B. The political path to universal health coverage: Power, ideas, and community-based health insurance in Rwanda. World Dev. 2018;106:87-98. doi.10.1016/j.worlddev.2018.01.023 Crossref | Google Scholar
- World Health Organization; World Bank. Tracking universal health coverage country data. First Global Monitoring Report. 2015 Publication Item
- Odeyemi IA. Community-based health insurance programmes and the national health insurance scheme of Nigeria: Challenges to uptake and integration. Int J Equity Health. 2014;13(1):1-13. doi.10.1186/1475-9276-13-20
PubMed | Crossref | Google Scholar - Yusuf HO, Kanma-Okafor OJ, Ladi-Akinyemi TW, Eze UT, Egwuonwu CC, Osibogun AO. Health insurance knowledge, attitude, and the uptake of community-based health insurance schemes among residents of a suburb in Lagos, Nigeria. West Afr J Med. 2019;36(2):103-111. PubMed | Google Scholar
- Assan A, Takian A, Aikins M, Akbarisari A. Universal health coverage necessitates a system approach: An analysis of the Community-Based Health Planning and Services (CHPS) initiative in Ghana. Glob Health. 2018;14(1):1-10. doi.10.1186/s12992-018-0426-x PubMed | Crossref | Google Scholar
- Hafez R. Nigeria Health Financing System Assessment. World Bank; 2018. doi.10.1596/30174 Crossref
- Hackett K, Lenters L, Vandermorris A, et al. How can engagement of adolescents in antenatal care be enhanced? Learning from the perspectives of young mothers in Ghana and Tanzania. BMC Pregnancy Childbirth. 2019;19(1):1-12. doi.10.1186/S12884-019-2326-3 PubMed | Crossref | Google Scholar
- Bolaji B, Aregbeshola S. NHIS as a source of health financing towards UHC in Nigeria. Int Health Policies.2019 NHIS as a source of health financing towards UHC in Nigeria. Int Health Policies.2019
- World Health Organization. Financing for Universal Health Coverage: Dos and Don’ts. Health Financing Guidance Note No. 9. WHO; 2019. Financing universal health coverage: Do’s and don’ts – P4H Network
- McIntyre D, Kutzin J. Health Financing Guidance No. 1: Health Financing Country Diagnostic A Foundation for National Strategy Development. World Health Organization; 2016. iris.who.int/bitstream/handle/10665/204283/9789241510110_eng.pdf
- Leight J, Björkman Nyqvist M. Community-based strategies to reduce maternal mortality in Northern Nigeria. The Abdul Latif Jameel Poverty Action Lab. 2020 Community Based Strategies to Reduce Maternal Mortality in Northern Nigeria | The Abdul Latif Jameel Poverty Action Lab
- National Coalition of CSOs review Nigeria’s RMNCAH+N (GFF) Investment Case. ARFH Nigeria. 2021 National Coalition of CSOs review Nigeria’s RMNCAH+N (GFF) Investment Case – ARFH Nigeria
- Nigeria State Health Investment Project (NSHIP). Qualitative Study on Key Differentiating Factors for Performance Under the Performance-Based Financing (PBF) Approach. 2015:1-74. [PDF] Nigeria State Health Investment Project (NSHIP) Qualitative Study on Key Differentiating Factor for Performance Under Performance Based Financing (PBF) Approach | Semantic Scholar
- Adewole IF, Adeyi O. Saving One Million Lives Programme for Results and Implementation in Nigeria: A Report. AMA. 2022;26(11s). Saving one million lives programme for results and implementation in Nigeria: A report | Adewole | African Journal of Reproductive Health
- The World Bank. Development Projects: Nigeria – Program to Support Saving One Million Lives (P146583).2022 Development Projects : Nigeria – Program to Support Saving One Million Lives – P146583
- Abimbola S, Okoli U, Olubajo O, Abdullahi MJ, Pate MA. The Midwives Service Scheme in Nigeria. PLoS Med. 2012;9(5):e1001211. doi.10.1371/journal.pmed.1001211 PubMed | Crossref | Google Scholar
- Alagbe J. NPHCDA deploys 1,181 midwives to primary health care centres. Punch Newspapers.2021. NPHCDA deploys 1,181 midwives to primary health care centres – Punch Newspapers
- Adewole DA, Adebayo AM, Obembe TA. Evaluation of the Midwives Service Scheme in a southwest Nigerian state: Policy implications for maternal and child health care programs. Int J Nurs Midwifery. 2019;11(June):54-60. doi.10.5897/IJNM2019.0363 Crossref | Google Scholar
- Onwujekwe O, Ensor T, Ogbozor P, et al. Was the Maternal Health Cash Transfer Programme in Nigeria sustainable and cost-effective? Front Public Health. 2020;8:582072. doi.10.3389/fpubh.2020.582072
PubMed | Crossref | Google Scholar - Subsidy Reinvestment and Empowerment Programme (SURE-P): Community Services Women and Youth Employment (CSWYE). OMOMi is leveraging digital technology to provide women with easy access to quality maternal health care | by Nigeria Health Watch | Medium
- Adepoju P. OMOMi is leveraging digital technology to provide women with easy access to quality maternal health care. Nigeria Health Watch. 2021 OMOMi is leveraging digital technology to provide women with easy access to quality maternal health care | by Nigeria Health Watch | Medium
- Akhimien C. OMOMi. One Young World. 2015. OMOMI | One Young World
- Ogbo E, Brown T, Gant J, Davis A, Sicker D. The impact of over-the-top services on preferences for mobile services: A conjoint analysis of users in Nigeria. J Inf Policy. 2021;11:403-443. doi.10.5325/JINFOPOLI.11.2021.0403
Crossref | Google Scholar - Kasali F, Adekola O, Akinyemi I, Ebo I, Balogun J. A model for ranking the usability attributes of mobile health applications in Nigeria (MCDM approach). Covenant J Informatics Commun Technol.2020;8(2):1-27. A Model for Ranking the Usability Attributes of Mobile Health Applications in Nigeria (MCDM Approach) | Covenant Journal of Informatics and Communication Technology
- Carter J, Sandall J, Shennan AH, Tribe RM. Mobile phone apps for clinical decision support in pregnancy: A scoping review. BMC Med Inform Decis Mak. 2019;19(1):1-13. doi.10.1186/s12911-019-0954-1 PubMed | Crossref | Google Scholar
- OMOMi is leveraging digital technology to provide women with easy access to quality maternal health care. Nigeria Health Watch. 2021. OMOMi is leveraging digital technology to provide women with easy access to quality maternal health care | by Nigeria Health Watch | Medium
- Abubakar I, Dalglish SL, Angell B, et al. The Lancet Nigeria Commission: investing in health and the future of the nation. Lancet. 2022;399(10330):1155-1200. doi.10.1016/S0140-6736(21)02488-0 PubMed | Crossref | Google Scholar
Acknowledgments
Not reported
Funding
The work had no special funding.
Author Information
Corresponding Author:
Olayinka Olutade-Babatunde
Department of Nursing
University of Benin Teaching Hospital, Benin City, Edo-State, Nigeria
Email: shindybabz@gmail.com
Co-Authors:
Anke van der Kwaak
Department of Sexual and Reproductive Health and Rights
KIT Royal Tropical Institute, Amsterdam, The Netherlands
Yusuf Sheku Tejan
Department of Community Health
Port Loko Regional Hospital, Ministry of Health, Freetown, Sierra Leone.
Bet-ini- N. Christian
Department of Clinical Services
Hospital Management Board, Uyo, Akwa-Ibom State, Nigeria
Authors Contributions
All authors contributed to the acquisition and critical review of the selected articles before arriving at the final manuscript, which was thoroughly written, examined, and approved for submission to the journal by all named authors.
Ethical Approval
Not applicable
Conflict of Interest Statement
The authors declare no conflicts of interest.
Guarantor
None
DOI
Cite this Article
Olutade-Babatunde O, van der Kwaak A, Tejan YS, Christian N. Promising Strategies and Practices to Promote Adolescent Mothers’ Health-Seeking Behaviour and Utilization of Maternal Healthcare Services in Nigeria. medtigo J Med. 2025;3(1):e3062315. doi:10.63096/medtigo3062315 Crossref













