






 Author Affiliations
Author Affiliations
Abstract
Objective: To determine the prevalence of bronchiolitis in children up to 2 years of age presenting to Tehsil Headquarter (THQ) Hospital Dogar, Central Kurram.
Study design: A retrospective study.
Duration and place of study: The study was conducted in THQ Hospital Dogar over a one-year period from January to December 2024.
Methodology: This retrospective study reviewed and analyzed medical records of 600 children aged 0–24 months who were clinically diagnosed with bronchiolitis at Tehsil Headquarter Hospital Dogar during the specified period. Data collected included demographic variables such as age and gender, seasonal variations, hospitalization rates, intensive care unit (ICU) admissions, need for mechanical ventilation, mortality, and average length of hospital stay. For statistical analysis, patients were further categorized into three distinct age groups to identify risk distribution and trends more accurately.
Results: The findings revealed that bronchiolitis cases showed a clear seasonal pattern, with the highest incidence during winter months (40%). The majority of affected children were infants aged 3–5 months (50%). Hospitalization was required in 66.7% of patients, while 25% needed ICU admission. Among these, 10% required mechanical ventilation, and the mortality rate was recorded at 2.5%. The lowest case numbers were observed during the summer season.
Conclusion: Bronchiolitis remains a common respiratory illness in young infants, particularly those between 3 and 5 months of age, with a marked peak during winter. Strengthening preventive measures, early recognition, and effective management strategies are essential to minimize hospitalizations and reduce disease burden in this vulnerable population.
Keywords
Bronchiolitis, Infants, Prevalence, Hospitalization, Seasonal Variation, Respiratory Infection, Respiratory synctional virus.
Introduction
Bronchiolitis, primarily caused by the respiratory syncytial virus (RSV), is a leading cause of respiratory distress in infants and young children, imposing a significant burden on healthcare systems, particularly in developing countries. Globally, RSV is responsible for substantial morbidity and mortality among children under five years of age, with one in every 50 deaths in this age group attributable to the virus.[1] In Pakistan, lower respiratory tract infections are a major contributor to pediatric morbidity and mortality, accounting for approximately 20% to 30% of all deaths in children under five.[2] The burden is especially pronounced in rural areas where access to healthcare is limited, exacerbating the impact of these infections.[3] Despite the high prevalence, there is a paucity of comprehensive data on the epidemiology of bronchiolitis in Pakistan, particularly in underserved regions. A study conducted in Karachi highlighted the significant mortality burden of RSV in early infancy, emphasizing the need for targeted interventions.[4] The objective of this study is to determine the prevalence and epidemiological characteristics of bronchiolitis among children up to two years of age at THQ Hospital Dogar, Central Kurram. Understanding local trends is crucial for developing targeted interventions aimed at the prevention and effective management of bronchiolitis in this region.
Methodology
A retrospective analysis was conducted on medical records of 600 children aged 0–24 months diagnosed with bronchiolitis at Tehsil Headquarter Hospital Dogar between January 1 and December 31, 2024. The age distribution was as follows: 3–5 months (300 cases, 50%), 6–15 months (150 cases, 25%), and 16–24 months (150 cases, 25%). Collected data encompassed age, gender, seasonal variation, hospitalization rate, length of stay, ICU admissions, and mortality. Patients were categorized into the specified age groups to analyse seasonal trends, and descriptive statistics were utilized to summarize the findings. This methodological approach aligns with similar studies conducted in Karachi, Pakistan, which have investigated the epidemiology and clinical spectrum of RSV-associated hospitalizations in children, highlighting the significance of age distribution and seasonal patterns in bronchiolitis cases.[5] Additionally, research from India has examined the clinical profiles and outcomes of bronchiolitis in children under two years, emphasizing the importance of detailed data collection on demographics and clinical outcomes.[6] Furthermore, studies in the United Arab Emirates have assessed epidemiology, seasonality, comorbidities, treatment patterns, and healthcare resource utilization in pediatric RSV infections, underscoring the value of comprehensive data analysis in understanding disease burden.[5-7]
Results
Bronchiolitis cases were most common in infants aged 3-5 months (50%), followed by 6-15 months (25%) and 16-24 months (25%). The incidence peaked in winter (November–January, 40%) and was lowest in summer (June–August). Out of the total cases, 66.7% (400) required hospitalization, with 25% (100) admitted to the ICU. Among hospitalized cases, 10% (40) needed mechanical ventilation, and the mortality rate was 2.5% (15 cases).
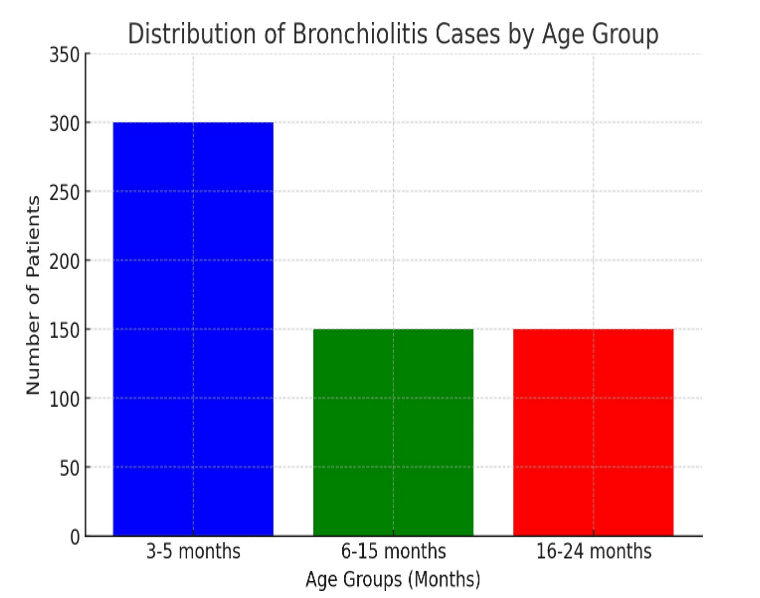
Figure 1: Distribution of bronchiolitis cases by age group
Discussion
Our findings align with both national and global data, indicating that bronchiolitis primarily affects infants under six months and peaks during winter months. A study in Mardan, Pakistan, reported that 56.5% of bronchiolitis cases occurred in infants younger than six months, with increased incidence during winter and spring.[8] Similarly, research in Karachi identified RSV as a significant contributor to infant mortality, particularly in those under six months.[3] These patterns underscore the need for preventive measures, such as maternal RSV immunization. The recent World Health Organization (WHO) prequalification of the first maternal RSV vaccine offers a promising strategy to protect infants during their most vulnerable early months.[9] Additionally, promoting breastfeeding and ensuring timely medical interventions are crucial to mitigating the impact of bronchiolitis on pediatric healthcare systems.
Conclusion
Bronchiolitis significantly impacts children under two in Central Kurram, particularly infants aged 3-5 months, with peak incidence during winter months. This pattern aligns with studies in Multan, Pakistan, where the highest cases occurred from December to February.[10] Preventive strategies are crucial to reducing hospitalizations. Implementing good hygiene practices, such as regular hand washing and cleaning of toys and surfaces, can mitigate virus transmission.[11] Additionally, avoiding exposure to tobacco smoke is essential, as passive smoking increases the risk of bronchiolitis.[12] Furthermore, administering the RSV vaccine during pregnancy can protect infants during their first six months, reducing severe bronchiolitis cases.[12,13] These interventions can effectively decrease bronchiolitis-related hospitalizations in the region.
References
- Li Y, Wang X, Blau DM, et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: a systematic analysis. Lancet. 2022;399(10340):2047-2064. doi:10.1016/S0140-6736(22)00478-0
PubMed | Crossref | Google Scholar - Naz R, Gul A, Javed U, Urooj A, Amin S, Fatima Z. Etiology of acute viral respiratory infections common in Pakistan: A review. Rev Med Virol. 2019;29(2):e2024. doi:10.1002/rmv.2024
PubMed | Crossref | Google Scholar - Kazi AM, Aguolu OG, Mughis W, et al. Respiratory Syncytial Virus-Associated Mortality Among Young Infants in Karachi, Pakistan: A Prospective Postmortem Surveillance Study. Clin Infect Dis. 2021;73(Suppl_3):S203-S209. doi:10.1093/cid/ciab488
PubMed | Crossref | Google Scholar - Frigati L, Greybe L, Andronikou S, Eber E, Sunder B Venkatakrishna S, Goussard P. Respiratory infections in low and middle-income countries. Paediatr Respir Rev. 2025;54:43-51. doi:10.1016/j.prrv.2024.08.002
PubMed | Crossref | Google Scholar - Ali A, Yousafzai MT, Waris R, et al. RSV associated hospitalizations in children in Karachi, Pakistan: Implications for vaccine prevention strategies. J Med Virol. 2017;89(7):1151-1157. doi:10.1002/jmv.24768
PubMed | Crossref | Google Scholar - B S, Gr S, Premkumar B, Elizabeth J. Clinical Profile and Outcome of Bronchiolitis in Children With 1-24 Months of Age. Cureus. 2024;16(9):e69640. Published 2024 Sep 18. doi:10.7759/cureus.69640
PubMed | Crossref | Google Scholar - Joury J, Al Kaabi N, Al Dallal S, et al. Retrospective Analysis of RSV Infection in Pediatric Patients: Epidemiology, Comorbidities, Treatment, and Costs in Dubai (2014-2023). J Health Econ Outcomes Res. 2024;11(2):133-144. Published 2024 Nov 5. doi:10.36469/001c.123889
PubMed | Crossref | Google Scholar - Khan MQ, Ullah K, Suleman M, Khan MK, Khan MA, Shah K. Epidemiology and risk factors analysis of children with bronchiolitis admitted to Nicu of mardan medical complex. Journal of Population Therapeutics & Clinical Pharmacology. 2023;30(18):1752-1758. doi:10.53555/jptcp.v30i18.3347
Crossref - WHO prequalifies first maternal respiratory syncytial virus vaccine. World Health Organization.
WHO prequalifies first maternal respiratory syncytial virus vaccine - Shah T, Iqbal S, Saleem I. Seasonality of bronchiolitis in hospitalized children Multan, Pakistan. Eur Respir J. 2015;46(suppl 59):PA1335. doi:10.1183/13993003.congress-2015.PA1335
Crossref - Sherri Gordon CLC. 6 pediatric specialists tell us how to prevent RSV. Parents. 2025.
6 Pediatric Specialists Tell Us How to Prevent RSV - Asthma + Lung UK. Bronchiolitis. 2025.
Bronchiolitis - Asthma + Lung UK. How can I prevent bronchiolitis? 2025.
How can I prevent bronchiolitis?
Acknowledgments
We sincerely thank Tehsil Headquarter Hospital Dogar for granting us access to the medical records.
Funding
This research was self-funded by the authors without any external financial assistance. All costs related to data collection, analysis, and manuscript preparation were personally covered by the researchers. No institutional or external grants were received for this study.
Author Information
Corresponding Author:
Bilal Noor
Department of Pediatrics
THQ Hospital Central Kurram Dogar, Kurram, Pakistan
Email: Bilalzk261@gmail.com
Co-Authors:
Mohammad Ibrahim
Department of Hospital Administration
Naseerullah Baber Hospital Peshawar, Pakistan
Hamid Iqbal
Department of Pediatric Medicine
PMO Nasir Ullah Babar Memorial Hospital, Peshawar, Pakistan
Muhammad Suliman
Department of Pathology
THQ Hospital Central Kurram Dogar, Kurram, Pakistan
Rabya Gul
Department of Community Medicine
Gandhara Medical University, Peshawar, Pakistan
Naveed Iqbal
Department of Dentistry
Ayub Medical College, Abbottabad, Pakistan
Authors Contributions
Dr. Bilal Noor led the study design and provided overall supervision of the project. Dr. Hamid Iqbal was responsible for data collection. Muhammad Suliman performed the statistical analysis. Burhan U Din contributed to the drafting of the manuscript. Sadia Nasir provided critical review and oversight throughout the study.
Ethical Approval
Ethical approval for the study was granted by the hospital Ethical Committee of THQ Hospital, Central Kurram Dogar (Ref No:0825). Data was collected after taking written consent from the parents of the enrolled children in our study.
Conflict of Interest Statement
The authors declare no conflicts of interest.
Guarantor
None
DOI
Cite this Article
Noor B, Ibrahim M, Suliman M, Iqbal H, Gul R, Iqbal N. Prevalence of Bronchiolitis in Children up to Two Years of Age Presented to Tehsil Headquarter Hospital Dogar, Central Kurram. medtigo J Med. 2025;3(3):e3062339. doi:10.63096/medtigo3062339 Crossref













