







 Author Affiliations
Author Affiliations
Abstract
Laparoscopic cholecystectomy, being a minimally invasive surgical procedure, has largely replaced open cholecystectomy in the treatment of diseased gallbladders in recent years. However, several complications can occur with this procedure, with vascular complications accounting for 0.8%. Hepatic artery pseudoaneurysm is a rare but serious and often lethal complication secondary to injury to the arterial wall, causing bleeding in adjacent tissues and thus forming a hematoma. We present such a rare complication in a young female later managed by embolization.
Keywords
Pseudoaneurysm, Post cholecystectomy, Embolization, Hepatic artery, Cholecystitis, Biliary dyskinesia.
Introduction
Laparoscopic cholecystectomy, being a minimally invasive surgical procedure, has largely replaced open cholecystectomy in the treatment of diseased gallbladders in recent years. Indications commonly include acute or chronic cholecystitis, biliary dyskinesia, symptomatic cholelithiasis, gallstone pancreatitis, gallbladder polyps/masses, or acalculous Cholecystitis. Apart from a larger number of advantages, including shortened hospital stay and recovery of the patient, reduced morbidity, and smaller incision, several complications can occur with this procedure. Vascular complications are rare and account for 0.8% of the cases.[1] The cause is either direct trauma or thermal injury. Hepatic artery pseudoaneurysm is a rare but serious and often lethal complication secondary to injury to the arterial wall, causing bleeding in adjacent tissues and thus forming a hematoma.[2] This complication is usually not encountered at the time of surgery, and it often presents later. Leaking pseudoaneurysm is a potentially lethal complication and requires urgent intervention.
Case Report
We present a case of a 28-year-old female who presented to us with symptoms of melena, hematochezia, and hematemesis for the last 2 months. She also had associated right hypochondrial pain. She had a recent history of a cesarian section 3 days back. History of laparoscopic cholecystectomy for symptomatic gallstones dates 8 months back. The procedure was uneventful, and the patient was discharged after stabilization.
On presentation, laboratory findings included a complete blood count (CBC) showing a total leukocyte count (TLC) of 12,610 cells/mL with 87% neutrophils. Hemoglobin was 6.5 g/dL, creatinine 0.2 g/dL, and C-reactive protein (CRP) was elevated to 117.2. Total bilirubin was 12.51 g/dL with direct bilirubin of 8.89 g/dL, and alkaline phosphatase was 270.
Subsequently, she underwent computed tomography (CT) abdomen and pelvis with contrast, which showed a lobulated saccular dilatation of the right hepatic artery, suggesting pseudoaneurysm formation (Figure 1). It was found in close proximity to surgical clips within the gallbladder fossa. There was also associated moderate intrahepatic ductal dilatation with ducts containing hyperdense material, like blood products.

Figure 1: CT abdomen axial maximum intensity projection images
Afterwards, she underwent a celiac angiography. Access was made through the right common femoral artery with cannulation of the coeliac axis and hepatic artery. It redemonstrated a large, narrow neck pseudoaneurysm arising from the right hepatic artery just before the trifurcation (figure 2).
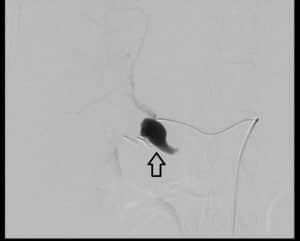
Figure 2: Angiography pre coiling
Selective catheterization of right hepatic artery branches distal to the pseudoaneurysm was done with the microcatheter-guidewire combination. Embolization of distal branches as well as the segment proximal to the pseudoaneurysm was done with multiple microcoils. Post-embolization angiogram showed flow stasis in the pseudoaneurysm without any anterograde or retrograde filling (Figure 3).
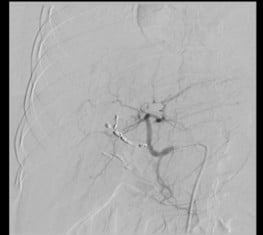
Figure 3: Angiography post-coiling
Discussion
Vascular complications secondary to laparoscopic cholecystectomy include occlusions, transactions, lacerations, and pseudo aneurysms.[3] About 25% of the cases with bile duct injuries have an association with vascular complications.[4] Occurrence of pseudoaneurysm after laparoscopic cholecystectomy is found commonest in right hepatic artery (documented in 0.6% of the cases) followed by common hepatic artery and cystic artery.[2] The actual incidence might be higher than known, as subclinical and smaller pseudoaneurysms thrombose and resolve on their own.
One of the mechanisms of injury to the hepatic artery is described as close contact of surgical clips to the artery and its segmental branches, as seen in our case. It has been similarly described by Srinivasaiah et al.[5] and Milburn et al.[6] In many cases, clips are often seen in close proximity to the developed pseudoaneurysm, and they may reach up to 7 cm in diameter. Biliary leakage and subsequent infection are also an established cause due to cytotoxic and fibrolytic properties of bile acids. Other causes are described as either direct injury to the walls of vessels or thermal injury during electrocautery. Some other documented causes of hepatic artery pseudoaneurysms include liver surgery, infection with abscess formation, trauma to the abdomen, or interventional procedures, including biliary stenting or liver biopsy. The range of potential methods of injury explains the time and mode of presentation of pseudo-aneurysm.
Clinical presentation of the symptoms often ranges from a few days to months, with a much later presentation of about 13 months described by Milburn et al.[6] In our case, symptoms were encountered after a period of six months. Commonest of the presenting complaints is haemobilia due to rupture of pseudoaneurysm in the biliary tract, presenting as upper gastrointestinal bleeding and melena in 90% of the cases, abdominal pain in 70%, and jaundice in 60%. The classic Quincke’s triad, comprising melena, jaundice, and right upper quadrant pain, is seen in 20 to 40% of the patients.[7] Patients can also present with intraperitoneal rupture with acute abdomen and anemia. Mortality rate of up to 50% has been reported consequent to rupture of a pseudo-aneurysm.[8]
On ultrasound, a pulsatile hypoechoic mass can be seen within the liver, with Doppler flow showing bidirectional flow. Upper gastrointestinal (GI) endoscopy is often the first investigation in cases of upper GI bleed; however, they are commonly inconclusive.[9] Contrast-enhanced CT can demonstrate pseudo-aneurysm formation or hemorrhage, which can sometimes be missed on endoscopic retrograde cholangiopancreatography (ERCP). The modality with the most reliable diagnostic outcome is celiac and spinal muscular atrophy (SMA) angiography.
The preferred treatment modality is trans-arterial embolization with a very high success rate (about 85%); however, rebleeding from pseudo-aneurysm can happen, and a repeated procedure or open surgical intervention for ligation or excision of pseudo-aneurysm is sometimes needed.[10,11] Compared to the traditional method of laparoscopy, robotic-assisted surgery can prevent vascular and bile duct injuries. Utilization of steel coils for embolization purpose is generally recommended, however no significant difference in the success rate between the embolization materials Is documented.[12] One aspect of the prevention of such iatrogenic complications is knowledge about the anatomical variations of cystic and hepatic arteries, which are found in up to 50% of cases.[13]
Conclusion
Formation of pseudo-aneurysm after laparoscopic cholecystectomy is recognized and sometimes a lethal complication, often presenting as upper gastrointestinal bleeding, a few weeks after the intervention. Knowledge of this outcome is important, given the non-specificity of clinical signs and symptoms. Angiographic and endovascular management has shown decreased morbidity and good clinical outcomes.
References
- Finley DS, Hinojosa MW, Paya M, Imagawa DK. Hepatic artery pseudoaneurysm: a report of seven cases and a review of the literature. Surg Today. 2005;35(7):543-547. doi:10.1007/s00595-005-2987-6
PubMed | Crossref | Google Scholar - Christensen T, Matsuoka L, Heestand G, et al. Iatrogenic pseudoaneurysms of the extrahepatic arterial vasculature: management and outcome. HPB (Oxford). 2006;8(6):458-464. doi:10.1080/13651820600839993
PubMed | Crossref | Google Scholar - Rivitz SM, Waltman AC, Kelsey PB. Embolization of a hepatic artery pseudoaneurysm following laparoscopic cholecystectomy. Cardiovasc Intervent Radiol. 1996;19(1):43-46. doi:10.1007/BF02560147
PubMed | Crossref | Google Scholar - Yelle JD, Fairfull-Smith R, Rasuli P, Lorimer JW. Hemobilia complicating elective laparoscopic cholecystectomy: a case report. Can J Surg. 1996;39(3):240-242.
Hemobilia complicating elective laparoscopic cholecystectomy: a case report - Srinivasaiah N, Bhojak M, Jackson R, Woodcock S. Vascular emergencies in cholelithiasis and cholecystectomy: our experience with two cases and literature review. Hepatobiliary Pancreat Dis Int. 2008;7(2):217-220. Vascular emergencies in cholelithiasis and cholecystectomy: our experience with two cases and literature review
- Milburn J, Hussey J, Bachoo P, Gunn I. Right hepatic artery pseudoaneurysm thirteen months following laparoscopic cholecystectomy. EJVES Extra. 2007;13(1):1-3. doi:10.1016/j.ejvsextra.2006.09.005 Crossref | Google Scholar
- Sansonna F, Boati S, Sguinzi R, Migliorisi C, Pugliese F, Pugliese R. Severe hemobilia from hepatic artery pseudoaneurysm. Case Rep Gastrointest Med. 2011;2011:925142. doi:10.1155/2011/925142
PubMed | Crossref | Google Scholar - Stanley JC, Thompson NW, Fry WJ. Splanchnic artery aneurysms. Arch Surg. 1970;101(6):689-697. doi:10.1001/archsurg.1970.01340300045009 PubMed | Crossref | Google Scholar
- Parthenis DG, Skevis K, Stathopoulos V, Bellenis I, Vassilakopoulos T. Postlaparoscopic iatrogenic pseudoaneurysms of the arteries of the peritoneal and retroperitoneal space: case report and review of the literature. Surg Laparosc Endosc Percutan Tech. 2009;19(2):90-97. doi:10.1097/SLE.0b013e31819ca96b PubMed | Crossref | Google Scholar
- Tessier DJ, Fowl RJ, Stone WM, et al. Iatrogenic hepatic artery pseudoaneurysms: an uncommon complication after hepatic, biliary, and pancreatic procedures. Ann Vasc Surg. 2003;17(6):663-9. doi:10.1007/s10016-003-0075-1
PubMed | Crossref | Google Scholar - Davies O, Batt J, Bethune R, Courtney E. Hepatic artery pseudoaneurysm post laparoscopic cholecystectomy. JSM Clin Case Rep. 2014;2(5):1050. doi:10.47739/2373-9819/1050 Crossref
- Feng W, Yue D, ZaiMing L, et al. Iatrogenic hemobilia: imaging features and management with transcatheter arterial embolization in 30 patients. Diagn Interv Radiol. 2016;22(4):371-7. doi:10.5152/dir.2016.15295
PubMed | Crossref | Google Scholar - Benson EA, Page RE. A practical reappraisal of the anatomy of the extrahepatic bile ducts and arteries. Br J Surg. 1976;63(11):853-60. doi:10.1002/bjs.1800631105 PubMed | Crossref | Google Scholar
Acknowledgments
Not reported
Funding
This study was conducted without any external funding.
Author Information
Corresponding Author:
Namrah Khalid
Department of Diagnostic Radiology
Shifa International Hospital Islamabad, Pakistan
Email: namrahk8@gmail.com
Co-Authors:
Jamshed Anwar, Amna Mehboob, Hajra Sajjad, Ahmed Moqeet
Department of Radiology
Shifa International Hospital, Pakistan
Authors Contributions
All authors contributed to the conceptualization, investigation, and data curation by acquiring and critically reviewing the selected articles. They were collectively involved in the writing – original draft preparation, and writing – review & editing to refine the manuscript. Additionally, all authors participated in the supervision of the work, ensuring accuracy and completeness. The final manuscript was approved by all named authors for submission to the journal.
Informed Consent
Informed consent was obtained from the patient’s attendants for the publication of this case report.
Conflict of Interest Statement
The author declares no conflict of interest.
Guarantor
None
DOI
Cite this Article
Ahmed M, Namrah K, Jamshed A, Amna M, Hajra S. Post-Cholecystectomy Pseudoaneurysm of Hepatic Artery.
medtigo J Med. 2024;2(4):e30622459. doi:10.63096/medtigo30622459 Crossref













