






 Author Affiliations
Author Affiliations
Abstract
Pituitary apoplexy is an endocrine emergency that occurs due to hemorrhage or infarction of the pituitary gland, predominantly in pituitary adenomas where the mass outgrows its blood supply. We present a case of a 15-year-old female who was unexpectedly diagnosed with pituitary apoplexy. The patient clinically presented with headache, vomiting, fever, visual disturbances, ophthalmoplegia, dizziness, and abdominal pain. Her history further reveals irregular menstruation in the previous two months. Clinical examination, however, was insignificant for any neurological or visual field deficits. In this age group, typical culprits include an infectious agent causing meningitis, a space-occupying lesion, a vascular event such as a ruptured arteriovenous malformation, or trauma. Lab investigations revealed isolated low morning cortisol and ACTH serum levels. To rule out the differentials, a lumbar puncture and CT scan were done. Both were reported as normal. An MRI was ordered as a further step, which showed a mild increase in the size of the pituitary gland with heterogeneous enhancement and curvilinear hyperintensity in the floor of the sella, suggesting hemorrhage within the gland. This case highlights that a diagnosis of pituitary apoplexy does not necessitate the presence of an underlying mass in the pituitary and that it could occur in adolescence.
Keywords
Pituitary apoplexy, Pituitary adenoma, Hypopituitarism, Adrenal insufficiency, Headache.
Introduction
A disorder known as pituitary apoplexy is caused by hemorrhage or infarction of the pituitary gland.
The term ”apoplexy” refers to abrupt damage to the nervous system caused by a gland infarction brought on by ischemia or hemorrhagic alteration [1].
The anterior pituitary is typically the first part to suffer damage since it receives most of its blood supply via the low-pressure portal circulation, which makes it more vulnerable to infarction [2]. The condition in question typically develops because of an underlying pituitary adenoma, and its presentation can range from being asymptomatic to having acute episodes of headache, altered mental status, visual disturbances, gastrointestinal upset, and hormonal abnormalities in the glands controlled by the pituitary [3]. We present a case of a 15-year-old female who was unexpectedly diagnosed as a case of pituitary apoplexy despite the lack of a causative pituitary mass.
Case Presentation
A 15-year-old pubertal girl was brought to the emergency department by her parents with complaints of vomiting, headache, fever, dizziness, and abdominal pain. The headache started two weeks ago, was severe in nature, awakening the patient from sleep, localized in the parietal area, and associated with symptoms of dizziness, blurry vision, and photophobia. She described a feeling of pain that was electrical in nature whenever she tried moving her eyes. She used Paracetamol and Ibuprofen every four hours for relief. Nausea started 3 days ago, while vomiting occurred twice in the past day. Vomiting was non-projectile, non-bilious, and not associated with food intake. As per the fever, the mother did not measure it or find any pattern; she just reported that her daughter was warm to the touch. Her abdominal pain was mild and non-localizing. Upon review of the systems, other notable symptoms included irregular menstrual cycles over the past two months. However, there was no reported neck stiffness, seizure, syncope, or galactorrhea. Her medical history is significant for a dental procedure complicated by localized oral infection two months before this visit, which necessitated multiple hospital admissions and antibiotic treatment. The patient was under significant stress due to upcoming exams in school.
On clinical examination, she was oriented, conscious, and her vitals were stable. No focal deficits were identified upon neurological examination. Ophthalmological examination revealed no change from her baseline visual acuity and no limitations of her visual field. The abdomen was soft, and no tenderness or guarding was elicited. Pubertal development was appropriate for her age.
Case Management
On the first day of admission, aside from basic investigation, the following was done. Lumbar puncture was unremarkable, and Meningitis/Encephalitis (ME) Panel (Multiplex PCR) detected no organisms. CT without contrast revealed no acute intracranial abnormality. On the second day, an MRI brain with contrast (MRA) was ordered, which showed a pituitary gland height of about 09-10 mm, with findings suggesting hemorrhage within the gland. On the third day of admission, MRI of the sella T1 sequence showed a mild increase in the size of the pituitary gland with heterogeneous enhancement and curvilinear hyperintensity in the floor of the sella, suggesting hemorrhage within the gland. Areas of infarct, however, were not seen (image 1).
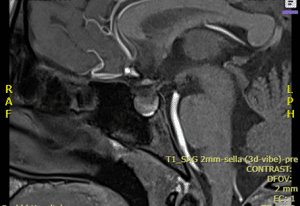
Figure 1: MRI of the sella T1 sequence showed a mild increase in the size of the pituitary gland with heterogeneous enhancement and curvilinear hyperintensity in floor of sella, suggesting hemorrhage within the gland. However, areas of infarct were not seen.
Lab investigations revealed isolated low morning cortisol and ACTH serum levels, suggesting secondary adrenal insufficiency. Other investigations done included: TSH: 5.7 IU/mm (high), Estradiol 430 pg/ml (high), while Prolactin, LH, FSH, Growth hormone, IGF1, T4, POCT Glucose Capillary Random were all normal. According to the imaging results and lab values, the patient was diagnosed with pituitary apoplexy with secondary adrenal insufficiency. Therefore, the patient was started on substitutive steroids (IV dexamethasone 4 mg BD and fludrocortisone 100 mcg OD), pain-control medications, and metoclopramide for her vomiting.
The plan entails serial imaging assessments to monitor significant alterations in size or signal intensities compared to the initial imaging. The patient is to be managed conservatively with close follow-up because her neuro-ophthalmological symptoms are mild and stable; therefore, they do not necessitate immediate surgical decompression. Upon relief of symptoms, the patient was discharged with the same medication plan and given a follow-up appointment one week after in the endocrinology department and to be followed in the ophthalmology department as well. Lab investigations are to be requested routinely for adjustment of doses and medications.
Discussion
Pituitary neoplasms are incredibly uncommon in children and adolescents (1:1.000,000), and less than 10% of them are diagnosed. Approximately 97% of all adenomas in individuals under 20 years old release hormones, and 16% cause pituitary apoplexy (PA) [4]. However, in the case we are discussing, there is no evidence of any pituitary neoplasm that predisposes to the apoplexy noted. Therefore, we believe that it is of great significance as it is unusual to diagnose this condition without a predisposing lesion and its extreme scarcity in this age group.
In cases of pituitary apoplexy, presentation may be asymptomatic or include headache with or without visual involvement [4]. Headache, being the most common symptom, endures a wide variety of differentials, which are more common than apoplexy and should be ruled out. These differentials include subarachnoid hemorrhage, bacterial meningitis, cerebral ischemia, cavernous sinus thrombosis, and migraine [5]. On the first day of admission, investigations including lumbar puncture and Meningitis/Encephalitis (ME) Panel were done to exclude meningitis since, in addition to the patient’s symptoms, there was a query of fever reported by the parents but had not been recorded in the hospital. Initial brain imaging by CT was done to exclude masses, intracranial hemorrhages, and other vascular lesions. The lumbar puncture also did not reveal blood in the CSF as evidence of subarachnoid hemorrhage. In another study, however, pituitary apoplexy may cause xanthochromia and mimic the clinical presentation of subarachnoid hemorrhage [6]. Pituitary apoplexy should be considered even in the presence of clinical or laboratory findings indicative of an infection. Distinguishing between pituitary abscess and PA is challenging. The type of headache, elevated CRP, endocrinological status, fever, and imaging may provide some clues, but they do not serve as clear-cut distinguishing factors between the two conditions [7,8,9].
The pituitary gland is well-known for being the master gland of the endocrine system; therefore, if it suffers from any dysfunction, the hormonal status of the body should be assessed [10]. In our case, the most critical clinical problem in pituitary apoplexy is the decreased secretion of ACTH, as it would lead to adrenal crisis due to a lack of secretion of cortisol [11]. Initial symptoms of adrenal insufficiency are non-specific, including nausea, vomiting, and abdominal pain. In this case, a differential diagnosis of acute abdomen was excluded using abdominal X-ray and ultrasound, indicating that the underlying cause of gastrointestinal symptoms is probably linked to adrenal insufficiency. ACTH deficiency should be highly suspected in patients with pituitary apoplexy as it necessitates instant treatment with stress doses of hydrocortisone [4]. Considering the patients’ secondary adrenal insufficiency, there’s a likelihood of necessitating lifelong steroid replacement therapy. Additionally, she faces heightened susceptibility to infertility.
Conclusion
In summary, pituitary apoplexy represents an urgent endocrine condition resulting from hemorrhage or infarction of the pituitary gland, typically associated with pituitary adenomas. However, our case study illustrates a rare occurrence in a 15-year-old female without a history of pituitary masses. Suspect pituitary apoplexy even in the absence of a prior history of pituitary mass. Suspect it in any age group. Assess for symptoms and signs produced locally due to the pressure effect and systemically due to endocrine control. The initial imaging may be inconclusive; therefore, you should utilize advanced imaging. Measure the hormonal activity of the pituitary and replace any deficiency.
References
- Ranbir S, Baruah MP. Pituitary apoplexy. Indian J Endocrinol Metab. 2011;15(7):188. doi:10.4103/2230-8210.84862 PubMed | Crossref | Google Scholar
- Tilbrook A. Neuropeptides, stress-related. In: Elsevier eBooks; 2007:903-908. doi:10.1016/B978-012373947-6/00735-2 Crossref
- Mattke AF, Vender JR, Anstadt MR. Pituitary apoplexy presenting as Addisonian crisis after coronary artery bypass grafting. Tex Heart Inst J. 2002;29(3):193-199. Pituitary apoplexy presenting as Addisonian crisis after coronary artery bypass grafting PubMed | Google Scholar
- Zijlker H, Schagen S, Wit JM, Biermasz N, Van Furth W, Oostdijk W. Pituitary adenoma apoplexy in an adolescent: A case report and review of the literature. J Clin Res Pediatr Endocrinol. 2017;9(3):265-273. doi:10.4274/jcrpe.4420 PubMed | Crossref | Google Scholar
- Ohata H, Shinde B, Nakamura H, et al. Pituitary apoplexy in a puberal child: A case report and review of the literature. Interdiscip Neurosurg. 2021;25:101160. doi:10.1016/j.inat.2021.101160 Crossref | Google Scholar
- Choudhury M, Eligar V, DeLloyd A, Davies JS. A case of pituitary apoplexy masquerading as subarachnoid hemorrhage. Clin Case Rep. 2016;4(3):255-257. doi:10.1002/ccr3.488 PubMed | Crossref | Google Scholar
- Nordjoe YE, Igombe SRA, Laamrani FZ, Jroundi L. Pituitary abscess: Two case reports. J Med Case Rep. 2019;13(1). doi:10.1186/s13256-019-2280-8 PubMed | Crossref | Google Scholar
- St-Pierre GH, de Ribaupierre S, Rotenberg BW, Benson C. Pituitary abscess: Review and highlight of a case mimicking pituitary apoplexy. Can J Neurol Sci. 2013;40(1):118-120. doi:10.1017/S0317167100015055 PubMed | Crossref | Google Scholar
- Zheng K, Fei H, Bai Z, et al. Pituitary abscess misdiagnosed as pituitary adenoma stroke: Case report and literature review. Interdiscip Neurosurg. 2020;20:100574. doi:10.1016/j.inat.2019.100574 Crossref | Google Scholar
- Davis SW, Ellsworth BS, Millan MIP, et al. Pituitary gland development and disease. Curr Top Dev Biol. 2013;1-47. doi:10.1016/B978-0-12-416021-7.00001-8 PubMed | Crossref | Google Scholar
- Del Valle MM, De Jesus O. Pituitary apoplexy. StatPearls. Published August 23, 2023. Pituitary apoplexy
Acknowledgments
None to declare
Funding
None to declare
Author Information
Corresponding Author:
Sura Salahuddin Salih Al-Rawi
Department of Neurology
Dubai Medical College, Dubai, United Arab Emirates
Email: sss20190163@dmcg.edu
Co-Authors:
Ruqaya Mustafa Rashid AlSalihi, Malak Mohammed Abdulelah, Aya Mohammed Ali Al Sabbah
Department of Neurology
Dubai Medical College, Dubai, United Arab Emirates
Yasmine Mohamed Shawki Kamal Mohamed
Department of Neurology
Rashid Hospital, Dubai, United Arab Emirates
Authors Contributions
All authors contributed to the conceptualization, investigation, and data curation by acquiring and critically reviewing the selected articles. They were collectively involved in the writing – original draft preparation, and writing – review & editing to refine the manuscript. Additionally, all authors participated in the supervision of the work, ensuring accuracy and completeness. The final manuscript was approved by all named authors for submission to the journal.
Informed Consent
Informed consent for publication of this report was obtained from the patient’s mother.
Conflict of Interest Statement
None to declare
Guarantor
Not reported
DOI
Cite this Article
Al-Rawi SS, AlSalihi RR, Abdulelah MM, Al Sabbah AMA. Pituitary Apoplexy in an Adolescent. medtigo J Med. 2024;2(3):e3062235. doi:10.63096/medtigo3062235 Crossref













