







 Author Affiliations
Author Affiliations
Abstract
Background: Recent advancements in cardiac anesthesia have significantly reshaped the specialty, ensuring hemodynamic stability, organ protection, and pain control during complex cardiac surgeries.
Objective: The aim of this study is to systematically review and synthesize recent clinical trial evidence on advancements in cardiac anesthesia with a focus on intraoperative monitoring technologies, pharmacologic innovations, organ protection strategies, and patient-centered outcomes to inform and guide future anesthetic practices in cardiac surgery.
Methods: A systematic literature search was conducted on PubMed and Google Scholar to identify clinical trials and randomized controlled trials related to cardiac anesthesia published between January 2020 and June 2025. After identifying 33,888 articles and assessing eligibility using the scale for the assessment of narrative review articles (SANRA) scoring, 9 studies were included, following the preferred reporting items for systematic reviews and meta-analyses (PRISMA) 2020 guidelines for methodological transparency.
Results: 9 randomized studies found that pupillometry-guided analgesia reduced opioid use by 47.2% and improved intraoperative hemodynamic stability. Remifentanil showed dose-dependent nociceptive suppression, but higher doses increased vasopressor requirements. Benzodiazepine-free protocols reduced postoperative delirium risk. Dexmedetomidine provided stable sedation during electrophysiology procedures. N-acetylcysteine provided hepatic protection and reduced intensive care unit (ICU) stay in valve surgery. Sevoflurane preserved renal function better than total intravenous anesthesia (TIVA) in pediatric patients. The wide-awake local anesthesia no tourniquet (WALANT) technique reduced bleeding complications during cardiac device implantation.
Conclusion: Innovations in cardiac anesthesia have improved patient care through individualized, multimodal, and technology-supported approaches. Future developments should standardize monitoring protocols, refine anesthetic agents, and integrate advanced training techniques.
Keywords
Cardiac anesthesia, Cardiac surgery, Pediatric cardiac anesthesia, Anesthetic innovation, Anesthesiology.
Introduction
Cardiac anesthesia is an important and developing area of anesthesiology that supports patients during complex heart surgeries. It involves managing unique challenges like the effects of cardiopulmonary bypass (CPB), protecting the heart and other organs, and maintaining stable blood flow and pressure throughout surgery. In the last ten years, improvements in drugs, medical devices, patient safety measures, and training techniques have significantly improved the practice and outcomes of cardiac anesthesia.[1] Cardiac anesthesia is a specialized branch of anesthesia focused on managing patients undergoing heart surgery, covering the preoperative, intraoperative, and postoperative phases. Preoperatively, a detailed assessment of the patient’s overall health and cardiac status is essential. Intraoperatively, techniques like transesophageal echocardiography (TEE) are used to guide surgical decisions and monitor heart function in real time. Postoperative care emphasizes effective pain control, where ultrasound-guided regional anesthesia has emerged as a valuable technique to minimize opioid use and enhance patient comfort during recovery.[2]
Anesthetic care during cardiac surgery must carefully manage the balance between blood circulation, the heart’s oxygen needs, and protection of the brain, especially when using CPB.[3] A variety of anesthetic agents are used, including volatile anesthetics, opioids, and intravenous drugs. However, there is no single preferred method, as each patient’s condition requires a different approach. Newer agents like propofol and ultra-short-acting opioids have broadened the options available to anesthesiologists. Volatile anesthetics are still widely used, particularly for their ability to protect the heart during periods of reduced blood flow and reperfusion.[4] One notable advancement in cardiac anesthesia pharmacology is the introduction of remimazolam, a new ultra-short-acting benzodiazepine. It provides reliable sedation with stable blood pressure and heart function. Remimazolam is currently being studied for its use in cardiac catheterization procedures and major heart surgeries. Early findings suggest that it may reduce the need for vasopressors and support faster patient recovery.[5,6]
The concept of opioid-free anesthesia (OFA) has recently gained interest, especially for its potential to lower the risk of postoperative opioid dependence. In cardiac surgery, adjuvant medications like ketamine, lidocaine, and dexamethasone have been used effectively as part of OFA protocols to manage pain and reduce reliance on opioids.[7] Congenital cardiac anesthesia, especially in pediatric patients, involves unique challenges due to complex and variable heart physiology. Large databases like the Congenital Cardiac Anesthesia Society–Society of Thoracic Surgeons Congenital Heart Surgery Database (CCAS-STS CHSD) have played a key role in improving clinical practices by providing insights into quality measures, transfusion strategies, and operating room efficiency.[8] Data from this database have shown that postoperative hematocrit levels above 42% are associated with higher rates of complications and mortality, emphasizing the need for careful transfusion management. Furthermore, operational metrics like anesthesia ready time have been analyzed to identify causes of delays and improve care delivery in pediatric cardiac surgery.[9]
In addition to advancements in medication, improving safety and workflow in cardiac anesthesia has become a major focus. Systematic reviews have highlighted the effectiveness of strategies such as preoperative briefings, intraoperative checklists, and structured postoperative handovers. These safety tools have been linked to lower mortality rates, reduced need for blood transfusions, and better communication among surgical teams, especially in high-risk cardiac surgery settings.[10] As part of ongoing quality improvement efforts, defining specific metrics for congenital cardiac anesthesia has been proposed to support national benchmarking and guide local, data-driven improvements in patient care.[11] Cardiac anesthesiologists are playing an increasingly active role in newer procedures such as minimally invasive cardiac surgeries and transcatheter interventions.[12] These procedures require specialized skills, including one-lung ventilation, TEE, and regional anesthesia. To meet these demands, innovative training approaches have been developed. For example, wearable eye-tracking technology is being used to enhance TEE training by providing objective feedback on where trainees focus their attention and how they develop technical skills.[13]
An important but often overlooked aspect of cardiac anesthesia is the assessment of right ventricular (RV) function. Although left ventricular function has traditionally received more attention, RV dysfunction is now known to significantly affect patient outcomes, especially during and after CPB. However, evaluating RV function remains difficult, as there are no standardized tools available for use during surgery that match the accuracy of cardiac MRI. Current research is focused on improving real-time assessment through enhanced echocardiographic techniques and biomarker-based tools to support better clinical decision-making.[14] Cardiac anesthesia continues to evolve alongside innovations in cardiovascular care. Emerging technologies such as gene therapy for refractory angina, wireless pacing-defibrillator devices, and advanced extracorporeal systems for organ protection are shaping the future of high-risk cardiac procedures. These advances not only improve patient survival but also influence the way anesthetic techniques are planned and delivered during complex interventions.[15]
Methodology
A systematic literature search was conducted using the PubMed and Google Scholar databases to identify clinical trials and randomized controlled trials related to cardiac anesthesia. The search strategy included the term “Cardiac Anesthesia” and applied filters for clinical trials, randomized controlled trials, human studies, English language, and inclusion of both male and female participants.
Inclusion criteria:
- Studies classified as clinical trials or randomized controlled trials (RCTs)
- Involving human participants
- Published in English
- Reporting on both male and female subjects
- Falling within the defined time frame from January 1, 2020, to June 30, 2025.
Exclusion criteria:
- Books, editorials, commentaries, letters, documents, and book chapters
- Case reports, case series, and narrative reviews
- Animal or in vitro studies
- Non-English publications
- Studies outside the specified publication window
- Articles without a reported results section
- Studies not directly relevant to cardiac anesthesia
A total of 33,888 articles were found; after applying the inclusion-exclusion criteria, 8,025 references were downloaded from PubMed and Google Scholar. Before the screening process began, 7,766 records were removed for various reasons, leaving 259 records for screening. Out of these, 104 records were excluded based on title and abstract screening. The remaining 155 records were sought for retrieval; however, 127 could not be retrieved, leaving 28 full-text articles for eligibility assessment. These 28 reports were evaluated against predefined criteria, including the SANRA scoring system. Nineteen articles were excluded due to SANRA scores being below 10. Ultimately, 9 studies met all inclusion criteria and were included in the final review.
Ultimately, 9 studies met all eligibility criteria and were included in the final review. The entire study selection process adhered to the PRISMA 2020 guidelines. A visual summary of the selection process is provided in the PRISMA flow diagram, ensuring a transparent and reproducible methodology (Figure 1).
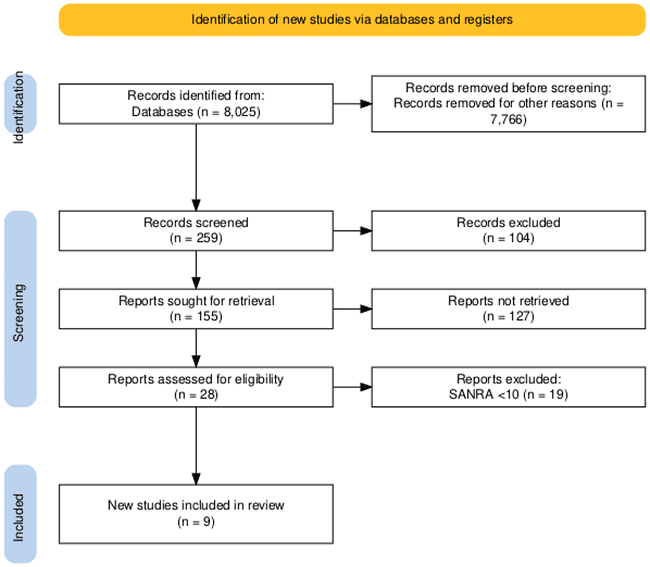
Figure 1: PRISMA flow diagram
Results
Optimizing opioid use during cardiac anesthesia has become a key area of interest. Randomized trials have shown that pupillometry-guided analgesia can significantly reduce the number of opioids used during surgery while maintaining stable anesthesia and hemodynamics. Compared to standard protocols, this approach led to a 47.2% reduction in sufentanil usage and an 81.8% decrease in infusion rates, with no cases of intraoperative awareness or complications. Additionally, patients in the pupillometry group required 56% less intraoperative noradrenaline, indicating more stable physiological conditions. Although postoperative opioid use remained similar, these patients reported 45% less pain within 48 hours after surgery, suggesting that pupillometry may help reduce opioid-induced hyperalgesia.[16]
Karunakaran KD et al. demonstrated through functional near-infrared spectroscopy (fNIRS) that cortical nociception monitoring during cardiac procedures revealed a dose-dependent suppression of brain responses to painful stimuli with remifentanil. Patients administered high-dose remifentanil showed markedly reduced cortical activity in both the somatosensory and prefrontal cortices, indicating effective central analgesia despite general anesthesia. Furthermore, nonpainful auditory stimuli elicited lower cortical responses in these patients, pointing to a broader suppression of sensory processing under remifentanil. However, higher vasopressor use was noted in the high-dose groups, aligning with the established cardiovascular side effects of opioids in cardiac anesthesia.[17]
Spence et al. conducted a large multicenter trial to examine the effects of benzodiazepine-free anesthesia on cognitive outcomes after cardiac surgery. The study found no significant difference in the overall rate of postoperative delirium between patients managed with liberal versus restrictive benzodiazepine use (14.0% vs. 14.9%). However, a per-protocol analysis showed that patients who completely avoided benzodiazepines had a modest but statistically significant reduction in delirium risk (adjusted odds ratio (OR) 0.90, 95% confidence interval (CI) 0.82 to 0.99). These findings suggest that while avoiding benzodiazepines may not eliminate delirium risk across all patients, tailored sedation strategies could offer cognitive benefits, particularly for older adults undergoing cardiac surgery.[18]
Hassan R et al. conducted research in Malaysia and compared remifentanil and dexmedetomidine infusions for monitored anesthesia care in 120 patients undergoing electrophysiology procedures. Although remifentanil is not commonly used alone in local practice, patients in the remifentanil group (Group R) showed significantly higher levels of alertness and elevated vital signs, including mean arterial pressure, heart rate, and both systolic and diastolic blood pressures (p < 0.01 for all), compared to the dexmedetomidine group. Oxygen saturation and respiratory rates were similar between groups. However, dexmedetomidine was associated with more stable hemodynamics and fewer adverse events. Patient satisfaction scores were comparable across both groups. These results suggest that dexmedetomidine may be a safer and more effective option for sedation during electrophysiology procedures in cardiac anesthesia, especially when minimizing cardiovascular instability is essential.[19]
Beyond cognitive and pain-related outcomes, organ protection during cardiac surgery has emerged as a critical focus of research. A study evaluating the effects of N-acetylcysteine (NAC) in patients undergoing double-valve cardiac surgery demonstrated significant benefits in liver protection. Patients who received NAC showed notably lower postoperative liver enzyme levels and bilirubin, with hyperbilirubinemia reported in only 6.6% compared to 46.6% in the control group (p = 0.005). In addition to hepatic protection, NAC use was linked to shorter durations of mechanical ventilation (p = 0.0465) and reduced ICU length of stay (p = 0.0431). Although not statistically significant, favorable trends were also observed in reducing postoperative atrial fibrillation and acute kidney injury. These findings suggest that NAC may offer promising multi-organ protection during cardiopulmonary bypass, supporting its further investigation in cardiac anesthesia practice.[20]
A randomized clinical trial in pediatric cardiac anesthesia compared the effects of sevoflurane with TIVA in children under two years undergoing congenital heart surgery with cardiopulmonary bypass. While there was no significant difference in postoperative serum troponin I levels, a marker of heart muscle injury, between the two groups (median 10.5 ng/mL vs. 11.0 ng/mL, p = 0.336), sevoflurane was associated with better kidney outcomes. Children in the sevoflurane group had higher urine output on the second postoperative day (800 mL vs. 541 mL, p = 0.034) and lower serum urea levels (24 mg/dL vs. 36 mg/dL, p = 0.030), indicating possible renal protection. These results suggest that sevoflurane may help preserve kidney function in pediatric cardiac anesthesia without increasing cardiac risk. Further research is needed to confirm these benefits in larger and more diverse pediatric populations.[21]
The use of the WALANT technique during cardiac implantable electronic device (CIED) implantation in patients maintained on uninterrupted antithrombotic therapy (ATT). In this study involving 46 patients, those who received WALANT using lidocaine with adrenaline experienced significantly fewer bleeding complications than those who received lidocaine alone. Specifically, the WALANT group required no intra-pocket pro-hemostatic agents (0% vs. 45%, p = 0.0002), had less need for pressure dressings (12.5% vs. 68%, p = 0.0002), and developed smaller postoperative hematomas (median 3.7 cm² vs. 46 cm², p = 0.0004). Importantly, no major adverse effects or device-related infections were reported. These results suggest that WALANT may be a safe and effective anesthetic approach in cardiac anesthesia, particularly for reducing bleeding risks without interrupting ATT. Larger studies are needed to confirm its long-term safety and clinical benefits.[22]
Zhou Y et al. evaluated the hemodynamic effects of different doses of ciprofol compared to etomidate in 209 patients undergoing cardiac surgery. Participants were divided into four groups: etomidate (0.2 mg/kg) and ciprofol at doses of 0.2, 0.3, or 0.4 mg/kg. After induction, all groups experienced reductions in heart rate (HR), mean arterial pressure (MAP), stroke volume (SV), and cardiac output (CO), with the declines occurring earlier in the higher dose ciprofol groups (0.3 and 0.4 mg/kg, p < 0.05). Importantly, the 0.2 mg/kg ciprofol group showed hemodynamic responses similar to etomidate, including significantly lower norepinephrine requirements (p < 0.05) and minimal changes in stroke volume and cardiac output. Although systemic vascular resistance (SVR) increased slightly in all groups, the differences were not statistically significant. The rates of hypotension and bradycardia were also comparable across all groups. These findings indicate that low dose ciprofol (0.2 mg/kg) may be a safe and effective induction agent in cardiac anesthesia, offering stable hemodynamics similar to etomidate.[23]
Recent studies in cardiac anesthesia highlight significant advancements in monitoring and analgesia techniques. The novel wavelet transforms cardiorespiratory coherence (WTCRC) algorithm showed greater sensitivity to nociception and antinociception than traditional metrics like heart rate and blood pressure. It detected an 82% increase in nociception during stimuli and a 50% decrease after anesthetic boluses. Other studies supported the use of remimazolam for stable sedation and pupillometry-guided analgesia for opioid reduction. Improvements in TEE training and right ventricular monitoring further enhanced intraoperative decision-making. Overall, these innovations contribute to safer, more individualized anesthesia care during cardiac surgeries.[24]
| Author/Study | Sample size | Intervention | Comparator | Key outcomes | Statistical results |
| Bartholmes F et al.[16] (Pupillometry-guided analgesia) | Not specified | Pupillometry-guided sufentanil | Standard analgesia | 47.2% reduction in sufentanil use; 81.8% lower infusion rates; 56% less intraoperative noradrenaline; 45% less pain at 48 hrs | No intraoperative awareness or complications |
| Karunakaran KD et al.[17] (fNIRS) | Not specified | High-dose remifentanil | Lower doses | Reduced cortical activity in somatosensory & prefrontal cortex; Increased vasopressor use | Qualitative results, no precise p-values |
| Spence et al.[18] (Benzodiazepine-free anesthesia) | Multicenter, large trial | Benzodiazepine avoidance | Liberal use | Delirium rate: 14.0% vs 14.9%; Per-protocol OR 0.90 (95% CI 0.82–0.99) | p significant |
| Hassan R et al.[19] (Remifentanil vs Dexmedetomidine) | 120 | Remifentanil | Dexmedetomidine | Higher alertness & vitals with remifentanil; More stable hemodynamics with dexmedetomidine | p < 0.01 for vitals |
| Ram Kiran KS et al.[20] (NAC for organ protection) | Not specified | NAC during double-valve surgery | Control | Hyperbilirubinemia: 6.6% vs 46.6% (P = 0.005); Shorter ventilation and ICU stay | p = 0.005, 0.0465, 0.0431 |
| Barelli JVG et al.[21] (Pediatric anesthesia) | Children <2 yrs | Sevoflurane | TIVA | Higher urine output (800mL vs 541mL, p = 0.034); Lower serum urea (24 vs 36 mg/dL, p = 0.030) | p = 0.034, 0.030 |
| Laish-Farkash A et al.[22] (WALANT for CIED) | 46 | WALANT (lidocaine + adrenaline) | Lidocaine alone | No pro-hemostatic agents needed (0% vs 45%); Less pressure dressings & hematomas | p = 0.0002, 0.0004 |
| Zhou Y et al.[23] (Ciprofol vs Etomidate) | 209 | Ciprofol (0.2–0.4 mg/kg) | Etomidate | Low-dose ciprofol (0.2mg/kg) is stable as etomidate; Lower norepinephrine use | P < 0.05 |
| Brouse CJ et al.[24] (WTCRC algorithm) | Not specified | WTCRC monitoring | Standard metrics | 82% increase in detection in nociception; 50% reduction post-bolus | No p-values |
Table 1: Summary of recent studies on cardiac anesthesia
Discussion
The evolution of cardiac anesthesia in recent years highlights a growing emphasis on personalized and physiology-driven strategies to optimize perioperative outcomes. The reviewed studies collectively demonstrate how emerging tools and pharmacologic innovations are transforming the landscape of intraoperative monitoring, analgesia, and organ protection during cardiac surgeries. One of the most significant trends is the integration of objective analgesia monitoring tools such as pupillometry and fNIRS, which allow for real-time titration of opioids based on patient-specific nociceptive responses. These technologies not only reduce intraoperative opioid consumption but also contribute to more stable hemodynamics and lower postoperative pain scores [16,17]. Other studies have validated the role of nociceptive monitors like analgesia nociception index (ANI) and nociception level index (NOL) in improving opioid dosing precision during cardiac surgeries, further supporting multimodal analgesia approaches [24,25].
In parallel, sedation strategies have evolved, with remimazolam gaining attention for its hemodynamic stability and rapid recovery profile. While benzodiazepine-free protocols have shown modest benefits in reducing delirium, tailored regimens that avoid overuse may be more pragmatic in high-risk populations [18,26]. Dexmedetomidine has also been recognized for its neuroprotective and anti-inflammatory properties, especially valuable in minimizing perioperative stress and delirium in elderly cardiac surgery patients [27]. The adoption of OFA and adjunctive agents like ketamine, lidocaine, and dexamethasone reflects a broader shift toward minimizing opioid dependence. The safety and efficacy of OFA have been increasingly demonstrated in both adult and pediatric cardiac populations [7,28].
Organ protection, particularly hepatic and renal, remains a key concern during cardiopulmonary bypass. The use of NAC has shown promising results, reducing hepatic dysfunction and ventilator days [19]. Sevoflurane, despite debates around its role in myocardial protection, may offer renal benefits in pediatric cardiac surgery [21]. These findings align with earlier studies showing sevoflurane’s potential to reduce oxidative stress and inflammation during ischemia-reperfusion injury [29]. Hemodynamic stability during induction and maintenance remains critical. Novel agents like ciprofol demonstrate dose-dependent effects, with lower doses matching the stability of etomidate, a standard cardiac induction agent [23]. These findings are consistent with earlier research showing ciprofol’s favorable cardiovascular profile in non-cardiac settings [30].
Finally, advancements in minimally invasive techniques, real-time imaging (TEE), and precision training (wearable eye-tracking for TEE guidance) reflect the expanding role of anesthesiologists in hybrid procedures and catheter-based interventions [13]. Studies support that structured simulation-based learning improves anesthetic proficiency in transcatheter aortic valve replacement (TAVR), extracorporeal membrane oxygenation (ECMO), and robotic cardiac surgery, underscoring the importance of training modernization [12].
This review is subject to several limitations. Many included RCTs were single-center studies with small to moderate sample sizes, limiting the generalizability of findings. Heterogeneity in outcome measures and anesthetic protocols across studies further complicates direct comparisons. Additionally, long-term postoperative outcomes, including quality of life and neurocognitive impacts, were underreported.
Future research should prioritize large-scale, multicenter RCTs with standardized protocols for anesthetic techniques and nociception monitoring. There is also a need for robust studies assessing long-term outcomes and the cost-effectiveness of implementing these innovations in routine clinical practice.
Conclusion
Cardiac anesthesia has undergone a substantial transformation in recent years, driven by technological innovation, refined pharmacology, and a strong commitment to individualized care. The current evidence supports the incorporation of real-time nociceptive monitoring, selective use of novel sedatives like remimazolam and dexmedetomidine, and multimodal strategies for organ protection and opioid reduction. Additionally, specialized training methodologies and expanded anesthesiologist roles in minimally invasive procedures reflect the specialty’s dynamic future.
As the field continues to evolve, future research should focus on developing standardized intraoperative monitoring protocols, validating novel anesthetic agents across diverse populations, and enhancing simulation-based learning for complex cardiovascular interventions. Strengthening these areas will further improve patient outcomes, safety, and recovery in cardiac anesthesia.
References
- Hamid A. Anesthesia for cardiac catheterization procedures. Heart Lung Vessel. 2014;6(4):225-231.
Anesthesia for cardiac catheterization procedures - Ramachandran G, Sundar AS, Venugopal V, Shah HD, Dogra N. Recent advances in cardiac anaesthesia. Indian J Anaesth. 2023;67(1):78-84. doi:10.4103/ija.ija_972_22
PubMed | Crossref | Google Scholar - O’Gara BP, Beydoun NY, Mueller A, Kumaresan A, Shaefi S. Anesthetic Preferences for Cardiac Anesthesia: A Survey of the Society of Cardiovascular Anesthesiologists. Anesth Analg. 2023;136(1):51-59. doi:10.1213/ANE.0000000000006147
PubMed | Crossref | Google Scholar - Sun Y, Sun X, Wu H, Xiao Z, Luo W. A review of recent advances in anesthetic drugs for patients undergoing cardiac surgery. Front Pharmacol. 2025;16:1533162. doi:10.3389/fphar.2025.1533162
PubMed | Crossref | Google Scholar - Ripoll JG, Orjuela RB, Kanaparthi A, et al. Remimazolam in cardiac anesthesia: Analysis of recent data. J Cardiothorac Vasc Anesth. 2025;39(1):273-285. doi:10.1053/j.jvca.2024.08.030
Crossref | Google Scholar - Muncan B, Bennett-Guerrero E. Remimazolam Use in Cardiac Anesthesia: A Narrative Review. J Cardiothorac Vasc Anesth. 2024;38(12):3179-3187. doi:10.1053/j.jvca.2024.07.045
Crossref | Google Scholar - Tang Z, Lin A, Liu H, Zhao M. What is new in cardiac anesthesia in 2024? J Anesth Transl Med. 2025;4(2):33-41. doi:10.1016/j.jatmed.2025.03.001
Crossref | Google Scholar - Hubbard RM, Buchbinder LB, Tobias JD, Zabala LM, Latham GJ, Gautam NK. The Anesthesiologist’s Perspective and Experience in Global Congenital Cardiac Surgery: Results of a Survey of the Congenital Cardiac Anesthesia Society Membership. Semin Cardiothorac Vasc Anesth. 2022;26(1):27-31. doi:10.1177/10892532211047641
PubMed | Crossref | Google Scholar - Njoku DB. Editorial. Curr Opin Anaesthesiol. 2025;38(3):215-216. doi:10.1097/ACO.0000000000001503
Crossref - O’Callaghan L, Ahern S, Doyle A. Safety interventions in cardiac anesthesia: A systematic review. Jt Comm J Qual Patient Saf. 2025;51(4):293-304. doi:10.1016/j.jcjq.2024.12.004
Crossref | Google Scholar - Brown ML, Dorste A, Adams PS, et al. Proposed Quality Metrics for Congenital Cardiac Anesthesia: A Scoping Review. Anesth Analg. 2025;140(2):397-408. doi:10.1213/ANE.0000000000007208
PubMed | Crossref | Google Scholar - White A, Patvardhan C, Falter F. Anesthesia for minimally invasive cardiac surgery. J Thorac Dis. 2021;13(3):1886-1898. doi:10.21037/jtd-20-1804
PubMed | Crossref | Google Scholar - Gorbaty B, Escuardo EV, Gherciuc A, Gherciuc S, Perry TE. Enhancing Transesophageal Echocardiography Training in Cardiac Anesthesia Fellows Using Wearable Eye-Tracking Technology. J Cardiothorac Vasc Anesth. doi:10.1053/j.jvca.2025.04.039
PubMed | Crossref | Google Scholar - Hori K, Watanabe R, Tsujikawa S, Hino H, Matsuura T, Mori T. Right Ventricular Dysfunction in Cardiac Anesthesia: Perioperative Assessment and Underlying Mechanisms. Rev Cardiovasc Med. 2025;26(2):26286. doi:10.31083/RCM26286
PubMed | Crossref | Google Scholar - Spence J, Mazer CD. Shaping the Future of Cardiac Anesthesia: Emerging Trends and Research Directions. Anesthesiol Clin. 2025;43(2):377-387. doi:10.1016/j.anclin.2025.02.008
PubMed | Crossref | Google Scholar - Bartholmes F, Malewicz NM, Ebel M, Zahn PK, Meyer-Frießem CH. Pupillometric Monitoring of Nociception in Cardiac Anesthesia. Dtsch Arztebl Int. 2020;117(49):833-840. doi:10.3238/arztebl.2020.0833
PubMed | Crossref | Google Scholar - Karunakaran KD, Kussman BD, Peng K, et al. Brain-based measures of nociception during general anesthesia with remifentanil: A randomized controlled trial. PLoS Med. 2022;19(4):e1003965. doi:10.1371/journal.pmed.1003965
Crossref | Google Scholar - Spence J, Devereaux PJ, Lee S, et al. Benzodiazepine-Free Cardiac Anesthesia for Reduction of Postoperative Delirium: A Cluster Randomized Crossover Trial. JAMA Surg. 2025;160(3):286–294. doi:10.1001/jamasurg.2024.6602
PubMed | Crossref | Google Scholar - Hassan R, Mutalib AA, Shang CY et al. Randomized single-blinded study comparing sedation effectiveness and hemodynamic stability of remifentanil vs dexmedetomidine infusion for electrophysiology procedures in patients of National Heart Institute cathlab. J Interv Card Electrophysiol. 2024;67(8):1735-1743. doi:10.1007/s10840-024-01884-x
PubMed | Crossref | Google Scholar - Ram Kiran KS, Trivedi V, Rajesh VSP, Sharma M, Haranal M, Pandya H. Role of Prophylactic N-Acetylcysteine Supplementation on Postoperative Outcomes in Patients Undergoing Elective Double-Valve Replacement (Aortic and Mitral Valve). Ann Card Anaesth. 2024;27(4):324-329. doi:10.4103/aca.aca_66_24
PubMed | Crossref | Google Scholar - Barelli JVG, Araujo DD, Zeferino SP, Dantas GM, Galas FB. Impact of anesthetic technique on troponin I levels in pediatric cardiac surgery: a randomized clinical trial. Braz J Anesthesiol. 2025;75(3):844603. doi:10.1016/j.bjane.2025.844603
PubMed | Crossref | Google Scholar - Laish-Farkash A, Yahud E, Rahkovich M, et al. Implanting Cardiac Electronic Devices with Uninterrupted Antithrombotic Therapy: A Novel Approach to Reduce Pocket Hematoma. Isr Med Assoc J. 2025;27(5):307-313.
Implanting Cardiac Electronic Devices with Uninterrupted Antithrombotic Therapy: A Novel Approach to Reduce Pocket Hematoma - Zhou Y, Liu Z, Li Q, et al. The Effects of Different Ciprofol Doses on Hemodynamics During Anesthesia Induction in Patients Undergoing Cardiac Surgery: A Randomized, Double-Blind, Controlled Study. Drug Des Devel Ther. 2025;19:1671-1679. doi:10.2147/DDDT.S505772
PubMed | Crossref | Google Scholar - Brouse CJ, Karlen W, Dumont GA, et al. Monitoring nociception during general anesthesia with cardiorespiratory coherence. J Clin Monit Comput. 2013;27(5):551-560. doi:10.1007/s10877-013-9463-4
PubMed | Crossref | Google Scholar - Edry R, Recea V, Dikust Y, Sessler DI. Preliminary Intraoperative Validation of the Nociception Level Index: A Noninvasive Nociception Monitor. Anesthesiology. 2016;125(1):193-203. doi:10.1097/ALN.0000000000001130
PubMed | Crossref | Google Scholar - Brown CH 4th, Laflam A, Max L, et al. The Impact of Delirium After Cardiac Surgical Procedures on Postoperative Resource Use. Ann Thorac Surg. 2016;101(5):1663-1669. doi:10.1016/j.athoracsur.2015.12.074
PubMed | Crossref | Google Scholar - Djaiani G, Silverton N, Fedorko L, et al. Dexmedetomidine versus Propofol Sedation Reduces Delirium after Cardiac Surgery: A Randomized Controlled Trial. Anesthesiology. 2016;124(2):362-368. doi:10.1097/ALN.0000000000000951
PubMed | Crossref | Google Scholar - Kharasch ED, Clark JD. Opioid-free Anesthesia: Time to Regain Our Balance. Anesthesiology. 2021;134(4):509-514. doi:10.1097/ALN.0000000000003705
PubMed | Crossref | Google Scholar - Van Allen NR, Krafft PR, Leitzke AS, et al. The role of Volatile Anesthetics in Cardioprotection: a systematic review. Med Gas Res. 2012;2(1):22. doi:10.1186/2045-9912-2-22
PubMed | Crossref | Google Scholar - Feins RH, Burkhart HM, Conte JV, et al. Simulation-Based Training in Cardiac Surgery. Ann Thorac Surg. 2017;103(1):312-321. doi:10.1016/j.athoracsur.2016.06.062
PubMed | Crossref | Google Scholar
Acknowledgments
Not reported
Funding
No funding
Author Information
Corresponding Author:
Samatha Ampeti, PhD
Department of Pharmacology
Kakatiya University, University College of Pharmaceutical Sciences, Warangal, TS, India
Email: [email protected]
Co-Authors:
Patel Nirali Kirankumar, Mansi Srivastava, Raziya Begum Sheikh, Shubham Ravindra Sali, Sonam Shashikala B V
Independent Researcher, Department of Content
Medtigo India Pvt Ltd, Pune, India
Authors Contributions
All authors contributed to the conceptualization, investigation, and data curation by acquiring and critically reviewing the selected articles. They were collectively involved in the writing – original draft preparation and writing – review & editing to refine the manuscript. Additionally, all authors participated in the supervision of the work, ensuring accuracy and completeness. The final manuscript was approved by all named authors for submission to the journal.
Ethical Approval
Not applicable
Conflict of Interest Statement
None
Guarantor
None
DOI
Cite this Article
Patel NK, Samatha A, Mansi S, Raziya BS, Shubham RS, Sonam SBV. Pharmacologic and Technologic Progress in Cardiac Anesthesia: Evidence from Recent Clinical Trials. medtigo J Anesth Pain Med. 2025;1(1):e3067118. doi:10.63096/medtigo3067118 Crossref













