






 Author Affiliations
Author Affiliations
Abstract
Cerebral venous sinus thrombosis (CVST) in children is a rare vascular disorder that presents with nonspecific symptoms, leading to a delay in diagnosis and treatment. The estimated annual incidence is up to 7 cases per million among children. To our knowledge, no case has been previously reported in Cambodia; therefore, we report our first case to share with our colleagues. A 2-year-old boy of Cambodian origin presented with a fever for two days, three episodes of partial seizures involving the right hand, tonic and jerking without vomiting. Past medical history was not remarkable. On physical examination, a non-toxic appearance and full alertness with normal neurologic examination were observed with low-grade fever of 38ºC. Initial blood analyses showed a high level of D-dimer to 1735 mg/L, a hemoglobin level of 11.1 g/dL, and an increased platelet count of 737 x109/L, white blood cell count of 20×10⁹/L, neutrophils of 12 x109/L and lymphocytes of 6 x109/L. Activated partial thromboplastin time (APTT), prothrombin time (PT), and International normalized ratio (INR) were 41.4, 11 seconds, and 0.84, respectively. Cerebral computed tomography (CT) scan with contrast shows a 5 mm CVST. This toddler was treated with oral Warfarin (direct oral anticoagulant), and the progression over the past 6-month monitoring showed normal neurological development and normal milestones for age, whereas laboratory profiles showed varying levels of D-dimer. This case gives insight into one of the many presentations in hopes of early detection and a good outcome.
Keywords
Cerebral Venous Sinus Thrombosis (CVST), Cerebral Computed Tomography (CT) scan, D-dimer, Vascular Disorder, Seizure, Acute Maxillary Sinusitis.
Introduction
CVST in children is a rare and life-threatening cerebrovascular condition, and with increased clinical awareness and improved neuroradiological techniques, the disease can now be diagnosed more frequently and at earlier stages. The incidence of childhood CVST occurs between 0.4 and 0.7 children per 100,000 children per year [1]. The incidence is higher among neonates (30–50%) compared to other pediatric age groups. There is a male predominance, with boys accounting for approximately two-thirds of all cases in children [2]. As reported in the literature, the early diagnosis and treatment of CVST could reduce the mortality rate to 5–15% [3]. There is a male predominance, with boys accounting for approximately two-thirds of all cases in children [4]. The early diagnosis of CVST is crucial since the risk of acute complications and long-term sequelae can be substantially reduced if appropriate treatment is initiated within the first few hours. In recent years, with the widespread application of magnetic resonance imaging (MRI), especially magnetic resonance venography (MRV) technology, the diagnostic rate of this disease has continuously improved [5]. To our knowledge, no case has been previously reported in Cambodia; therefore, we would like to report the first case to share with our colleagues.
Case Presentation & Management
A 2-year-old boy of Cambodian origin presented to the department of pediatric hematology and immunology with a 2-day history of fever, three episodes of partial seizures involving the right hand, tonic and jerking without vomiting. Past medical history was not remarkable. His physical examination on arrival revealed a non-toxic appearance, fully alert, Glasgow coma score (GCS) 15/15, low grade fever 38ºC, with normal vital signs, and no signs of neurological impairment or meningeal involvement were detected. Initial laboratory investigations revealeda high level of D-dimer with 1735 mg/L. The other results of blood work were summarily given in table 1.
| Blood Work | Patient test results | Reference Range |
| Complete blood count | ||
| White blood cells | 20 | 5-15 x 109/L |
| Neutrophils | 12 | 1-7 x109/L |
| Lymphocyte | 6 | 6-9 x 109/L |
| Hemoglobin | 11.1 | 11-14 g/dl |
| Hematocrit | 32 | 34-40 % |
| Platelet count | 737 | 200-490 x 109/L |
| Hemostatic screening | ||
| APTT | 41.4 | 26-36 secs |
| PT | 11 | 10-16 secs |
| INR | 0.84 | 0.9-1.3 |
| Fibrinogen | 4 | 4 g/L |
| BT | 8 | 2-7 secs |
| D-dimer | 1735 | <500 mg/L |
| FVIII | 80 | 50-150% |
| FIX | 150 | 50-150% |
| Inflammatory marker | ||
| CRP | 48 | < 6 mg/L |
Table 1: Initial laboratory investigations
Cerebral CT scan with contrast shown as axial, coronal, and sagittal thickness of 5 mm, consistent with CVST, and maxillary sinusitis (Figure 1).
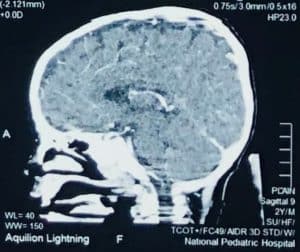
Figure 1: Image CT scan at first diagnosis
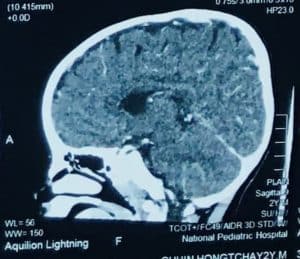
Figure 2: Image CT scan after 6-month treatment
This toddler was definitively diagnosed with CVST and treated with oral Warfarin in loading dose (0.2 mg/kg/dose twice daily) for 2 days, then maintenance dose given 0.1 mg/kg/day (50% initial dose) during 4-months, and the progression of the patient over the next 6-month monitoring was normal neurological development and normal milestones for age whereas laboratory profiles had varying levels of D-dimer. A cerebral CT scan performed 4 months later revealed a partial recanalization of the right transverse and sigmoid sinus, a mild improvement in the appearance of the right mastoid inflammation, and an enhancement of the right preauricular soft tissues. After 6 months, the imaging CT scan did not show soft tissue involvement, which showed further improvement of the venous sinus thrombosis (Figure 2).
Discussion
CVST in children is a rare vascular disorder that presents with nonspecific symptoms, leading to a delay in diagnosis and treatment. The estimated annual incidence is up to 7 cases per million among children [6]. Clinically, patients are presented with variable symptoms ranging from headache to seizure and coma in severe cases. Visual impairment due to an increase in intracranial pressure and generalized neurological deficits are reported to be more common in children [7]. In our case, the clinical manifestations were fever, headache, vomiting associated with partial seizures expressing right-hand tonic and jerking, which were nonspecific symptoms.
The etiology of childhood CVST is multifactorial, in which 33% to 99% of patients have inherited or acquired prothrombotic risk factors. The most well-known acquired prothrombotic risk factors, along with the accompanying diseases, include catheters, infection, dehydration, chronic inflammatory diseases, nephrotic syndrome, and malignancies [8], In our present case, presented with acute maxillary sinusitis, which was the most likely risk factor for CVST. Inherited thrombophilia risk factors are known as antithrombin deficiency, protein C and protein S deficiency, Factor V Leiden and prothrombin G20210A mutations, hyper homo-cysteinemia, elevated circulating levels of factors II, VIII, IX, XI, and fibrinogen, and high lipoprotein (a) level [9]. In our case, (fibrinogen, factor VIII, factor IX) were performed, and the results were normal. The other recommended tests are not available in Cambodia.
Neuroimaging showed thrombosis in more than 1 sinus, and overall thrombosis was located mainly in deep compared to superficial sinuses, 70% vs. 30%, respectively [10]. As in our reported case, cerebral TDM with contrast showed axial, coronal, and sagittal thickness of 5 mm, consistent with CVST. Sinusitis of the bilateral ethmoid and inferior sagittal sinus thrombosis was suggested.
The most recommended treatment for CVST without significant intracranial hemorrhage includes anticoagulation treatment initially with either unfractionated heparin (UFH) or low-molecular-weight heparin (LMWH) for these children [11]. This initial therapy is followed by LMWH for 6 weeks to 3 months in neonates and LMWH or oral anticoagulant therapy for 3 to 6 months in children. Oral Warfarin had been initiated in our patient and continued for at least six months with a goal INR of 2–3. Our patient showed significant clinical, laboratory (Table 2), and radiological improvement following administration.
| Date | Platelet count
(x109/L) |
INR | PT
(Seconds) |
APTT
(Seconds) |
D-Dimer
(mg/L) |
| Reference Range | 200-490 | 0.9-1.3 | 10-16 | 26-36 | <500 |
| 21-12-2023 | 737 | 0.8 | 11 | 41.4 | 1735 |
| 26-01-2024 | 766 | 0.9 | 14 | 29 | 234 |
| 28-02-2024 | 639 | 1.0 | 11 | 28 | 149 |
| 18-03-2024 | 436 | 1.1 | 14 | 32 | 98.4 |
| 29-04-2024 | 440 | 1.5 | 13 | 30 | 98.2 |
| 10-05-2024 | 420 | 2.0 | 12 | 28 | 98.0 |
| 07- 08-2024 | 467 | 0.8 | 11 | 30 | 140 |
Table 2: Progression of laboratory parameters on follow-ups
Conclusion
CVST is a rare phenomenon with an ambiguous clinical presentation, which includes but is not limited to seizures, vomiting, hemiparesis, and the impact on cranial nerves, creating a challenge for physicians to diagnose, especially in the limited setting of investigative facilities like Cambodia. This current case gives insight into how early detection and treatment resulted in a good outcome for the patient.
References
- Vandenbroucke JP. Cerebral sinus thrombosis and oral contraceptives. BMJ. 1998;317(7150):483-484. doi:10.1136/bmj.317.7157.483 PubMed | Crossrefv | Google Scholar
- Ichord R. Cerebral sinovenous thrombosis. Front Pediatr. 2017;5:163. doi:10.3389/fped.2017.00163 PubMed | Crossref | Google Scholar
- Masuhr F, Einhaupl K. Treatment of cerebral venous and sinus thrombosis. Front Neurol Neurosci. 2008;23:132-143. doi:10.1159/000111375 PubMed | Crossref | Google Scholar
- Bektaş Ö, Teber S, Akar N, Çelik A, Başkaya MK. Cerebral sinovenous thrombosis in children and neonates: Clinical experience, laboratory, treatment, and outcome. Clin Appl Thromb Hemost. 2015;21(8):777-782. doi:10.1177/1076029614523491 PubMed | Crossref | Google Scholar
- Gao L, Xu W, Li T, Yu X, Cao S, Xu H, Zhang H. Accuracy of magnetic resonance venography in diagnosing cerebral venous sinus thrombosis. Thromb Res. 2018;167:64-73. doi:10.1016/j.thromres.2018.05.012
PubMed | Crossref | Google Scholar - Özcan A, Canpolat M, Doğanay S, Özkaya D, Küçük Ö. Cerebral sinus venous thrombosis and prothrombotic risk factors in children: A single-center experience from Turkey. J Pediatr Hematol Oncol. 2018;40(8):e369-e372. doi:10.1097/MPH.0000000000001149 PubMed | Crossref | Google Scholar
- Ferriero DM, Fullerton HJ, Bernard TJ, et al. Management of stroke in neonates and children: A scientific statement from the American Heart Association/American Stroke Association. Stroke. 2019;50(5):e51-e96. doi:10.1161/STR.0000000000000183 PubMed | Crossref | Google Scholar
- Bristol-Myers Squibb. Coumadin (warfarin sulfate). S. Food and Drug Administration. Revised October 2011. Accessed November 2019. Coumadin (warfarin sulfate)
- deVeber G, Andrew M, Adams C, et al. Cerebral sinovenous thrombosis in children. N Engl J Med.
2001;345(6):417-423. doi:10.1056/NEJM200108093450604 PubMed | Crossref | Google Scholar - Pfefferkorn T, Crassard I, Linn J, Dichgans M, Boukobza M, Bousser MG. Clinical features, course and outcome in deep cerebral venous system thrombosis: An analysis of 32 cases. J Neurol. 2009;256(12):1839-1845.
doi:10.1007/s00415-009-5206-3 PubMed | Crossref | Google Scholar - Medlock M, Olivero W, Hanigan W, Wright RM, Winek SJ. Children with cerebral venous thrombosis diagnosed with magnetic resonance imaging and magnetic resonance angiography. Neurosurgery. 1992;31(5):870-876. doi:10.1227/00006123-199211000-00007 PubMed | Crossref | Google Scholar
Acknowledgments
The authors would like to thank Dr. So Saran for his contribution to the image of the cerebral CT scan, and to Robyn Devenish for her help with the language in this manuscript. We express our gratitude to the patient and parents who kindly gave consent to this case presented in this paper.
Funding
Not applicable
Author Information
Corresponding Author:
Chin Soey
Department of Pediatric Hematology and Immunology
National Pediatric Hospital, Phnom Penh, Cambodia
Email: chinseuy52631@gmail.com
Co-Authors:
Chean Sophâl
Department of Pediatric Hematology and Immunology
National Pediatric Hospital, Phnom Penh, Cambodia
Robyn Devenish
Department of Laboratory
National Pediatric Hospital, Phnom Penh, Cambodia
Authors Contributions
All authors contributed to the conceptualization, investigation, and data curation by acquiring and critically reviewing the selected articles. They were collectively involved in the writing – original draft preparation, and writing – review & editing to refine the manuscript. Additionally, all authors participated in the supervision of the work, ensuring accuracy and completeness. The final manuscript was approved by all named authors for submission to the journal.
Informed Consent
Informed consent was provided to a child’s parents as they agreed to the case publication.
Conflict of Interest Statement
The authors declare that they have no competing interests.
Guarantor
Not reported
DOI
Cite this Article
Chin S, Chean S, Robyn D. Pediatric Cerebral Venous Sinus Thrombosis as a Rare Vascular Disorder in a Toddler: A First Case Report in Cambodia. medtigo J Med. 2024;2(3):e3062240. doi:10.63096/medtigo3062240 Crossref













