






 Author Affiliations
Author Affiliations
Abstract
Objectives: The respective study aimed to assess organizational dehumanization and its impact on the work capacity of the paramedics of Pakistan Ordinance Factory (POF) Hospital, Wah Cantt.
Methodology: A cross–sectional study was conducted in the POF hospital for 6 months. Data was collected through a standard questionnaire. The calculated sample size was 137 (p =35%). But available paramedics were only 100 under our inclusion criteria. The data was analyzed using the Statistical Package for the Social Sciences (SPSS) version 25.
Results: The results showed that the majority of the staff (59%) included were females, while 41% were males. The majority of the staff were in the age bracket of 25-35 years. The majority of the employees had 3-8 years of work experience. 96% of the staff responded positively to dehumanization according to our scale. 93% of the employees had a significant effect on their work capacity due to dehumanization trends in the workplace. Our results show significant levels of dehumanization and a reduction of work capacity.
Conclusion: This research concludes that dehumanization is an important workplace issue faced by paramedics. Also, its significant impact on the work capacity of paramedics should be addressed seriously by the relevant authorities in departments and the administration of the hospital. This step will improve the outcome of the work and overall have a good impact on patient care.
Keywords
Dehumanization, Paramedics, Work impact, Work capacity, Workplace.
Introduction
The word ‘dehumanization’ means to deprive a person or group of people of positive human qualities. Dehumanization in organizational contexts refers to the experience of employees feeling objectified, treated as tools, or denied personal identity for the organization’s goals. It impacts an individual’s identity at his or her workplace.[1]
Organizational dehumanization is relevant as it significantly impacts the quality of work environments and employee well-being. It can lead to a range of negative outcomes, such as emotional exhaustion and decreased job satisfaction. It has an impact on inner motivation and commitment, making individuals less resilient in the face of job demands and more susceptible to burnout. As the workplace increasingly mechanizes tasks, employees may feel emotionally isolated, perceiving their contributions as undervalued. Thus, this issue is essential not only to safeguard mental health but also to sustain a positive work ethic and optimal performance levels, emphasizing the necessity of humane, supportive, and interactive work environments to mitigate these negative effects.[2]
Dehumanization in the field of medicine is an important subject to study as doctors, nurses, and other paramedics are at higher risk of facing this issue. Paramedics suffer from this issue due to their long, strenuous working hours, extreme work pressure, and the difficult nature of the job involving the care of multiple patients. So, nurses and paramedics need to be provided with a positive environment at the workplace, ensuring no paramedic suffering with the mental health issue and state of being treated as a tool at his/her workplace.[2]
In contrast to our above-mentioned discussion, now we proceed towards the idea of a healthy work environment. A healthy work environment is one where employees feel respected, supported, and valued, fostering a culture of open communication and collaboration. It promotes physical and mental well-being by prioritizing work-life balance, safety, and mutual respect. In such an environment, individuals are empowered to perform their best while feeling emotionally secure and motivated. The physical and behavioral aspects are the two facets of a healthy working climate. The priority refers to the factors that are linked to the ability of employees to remain physically associated with their workplaces. While the etiquette of office bearers is influenced by the behavioral aspects of the environment, the workplace environment plays an important role in shaping the behaviors of employees individually.[3]
Consequently, employees’ motivation to work hard, their efficiency, and performance are shaped by the influence of the quality of the workplace. Workers’ levels of willingness to keep motivated, creative, engaged with colleagues, and loyal to their jobs are all influenced by the factors of the workplace environment.[4] The unfavorable relationships that employees have with others in their workplace, such as those involving organizational obstruction, abusive supervision, organizational unfairness, and aggression started by coworkers, have been the subject of previous research.[5]
Additionally, it is believed that organizational dehumanization is a significant predisposing factor to unfavorable workplace outcomes such as low job satisfaction.[6] When we categorically discuss the impact of dehumanization on health workers, we must consider some research that has been previously conducted on this topic. Dehumanization can be particularly detrimental to mental health when it occurs in contexts where individuals are already vulnerable, such as in the workplace, educational institutions, or healthcare settings.[7] The importance of this study is that we can comprehend how dehumanization and the workplace affect employees’ work capacity, as it leads to demotivation, reduces job satisfaction, and disengagement. It not only affects work capacity but also affects mental and physical health (anxiety, depression, cardiovascular system diseases). It disrupts social connections and teamwork in the working environment. It leads to poor communication, misunderstandings, and errors.
Standardized measurement of dehumanization can inform strategies to promote person-centered care, improve patient outcomes, and enhance healthcare professionals’ well-being.[8] Despite its significant implications for mental health, dehumanization remains an understudied and under-addressed issue in clinical practice, highlighting the need for further research and development of effective interventions.[9] We agree to the statement that dehumanization is quite an understudied topic in Pakistan overall. Since hospitals and health care workers are an integral part of our society, we would like to put some effort into studying the impact of this big problem on their lives and evaluating the changes that can be brought to improve their lives at work.[10]
The purpose of our research is to investigate the impact of organizational dehumanization on the work capacity of medical staff. Our research work is invested in finding how this phenomenon affects their mental or physical health, which leads to decreased or poor work capability.
Methodology
Objective: To determine Dehumanization among Paramedics and Its Impact on Work Capacity.
Study design: Cross-sectional study
Setting: Pakistan Ordinance Factory Hospital, Wah Cantt.
Duration of study: 6 months, after the approval of the synopsis from the Institutional Review Board (IRB) / Ethical Review Board (ERB).
Sample size: Sample size is calculated using the World Health Organization (WHO) sample size formula, taking “P = 35%”, z² = 1.96², alpha = 0.08, and the sample size is 137.
Sampling technique: Convenient sampling
Sample selection
Inclusion criteria: All the Paramedics of POF Hospital.
Exclusion criteria: Generic Nursing students, internees, and residents.
Data collection procedure: A pre-tested eleven-item Organizational Dehumanization scale will be used for collecting the responses, in which each item is scored on a 5-point Likert scale, with score “1” depicting strongly disagree and score “5” depicting strongly agree. The first part of the questionnaire includes socio-demographic data: Gender, Age, Education, and Working experience. The impact of dehumanization on work capacity will be measured by using a self-structured four-item questionnaire in which each item is scored on a 5-point Likert scale, with score “1” depicting strongly disagree and score “5” depicting strongly agree, which is constructed after a thorough literature search. The questionnaire will be distributed and filled out by the paramedics themselves.
Operational definition: The total score on the Eleven-item Dehumanization scale ranges from 11 to 55. Taking 11 as the lowest and 55 as the highest level of Dehumanization. The impact of Dehumanization on Work Capacity is scored by taking four as the lowest and 20 as the highest score of impact on work capacity.
Data analysis: SPSS version 25 will be used for analysis. Frequencies and percentages will be presented in the form of Pie charts and frequency tables.
Results
The results showed that the gender distribution was 59% females and 41% males. These results are represented in Figure 1 below.
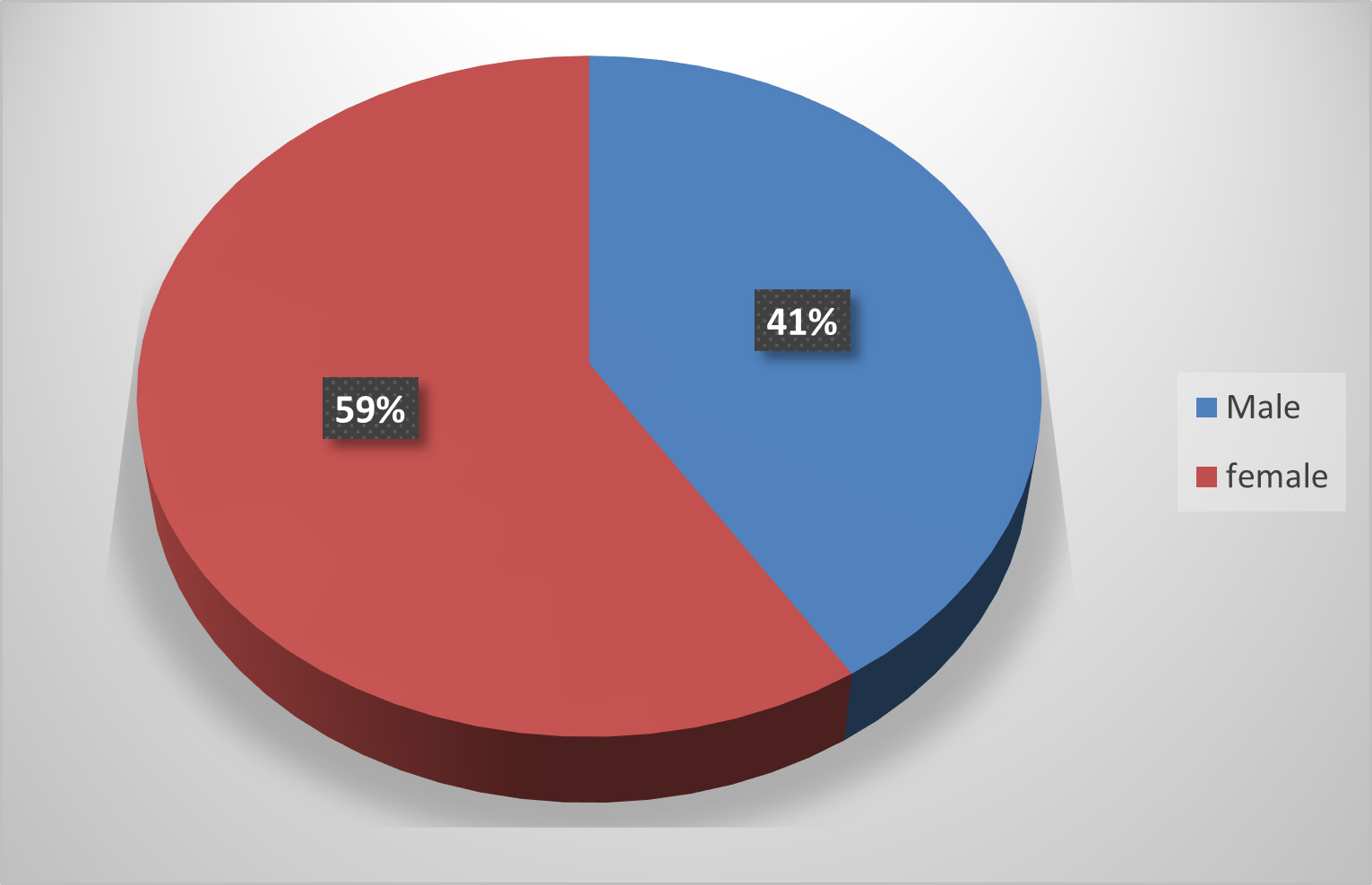
Figure 1: Gender distribution of paramedics
The age distribution graph in Figure 2 shows that most of the paramedics had an age range of 25-35 years, with a percentage of 76% paramedics in this age group (Figure 2).
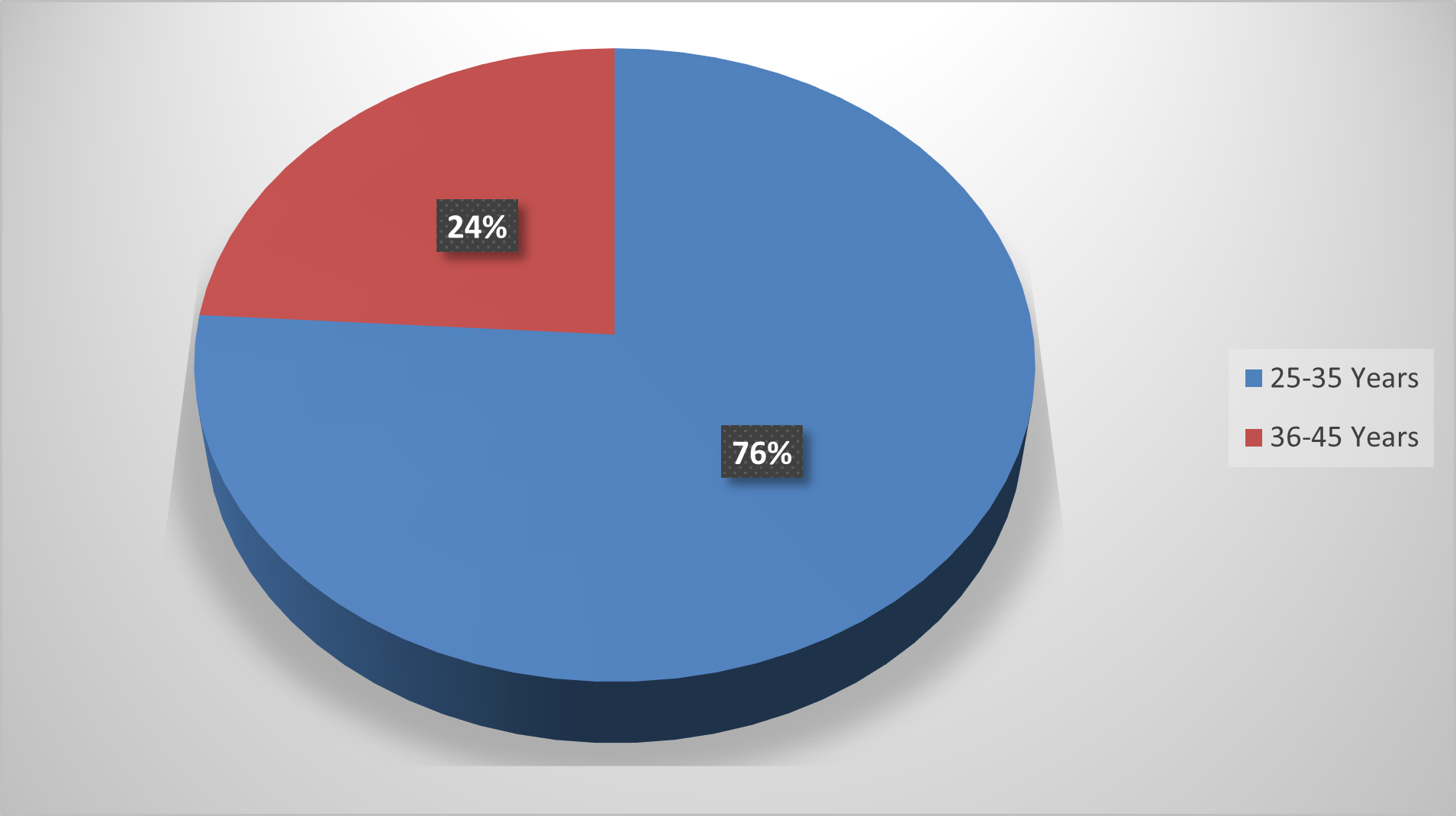
Figure 2: Age distribution of paramedics
The work experience duration was most of the time in the range of 3-8 years, with 67% paramedics in this range. These results are shown in Figure 3 below.
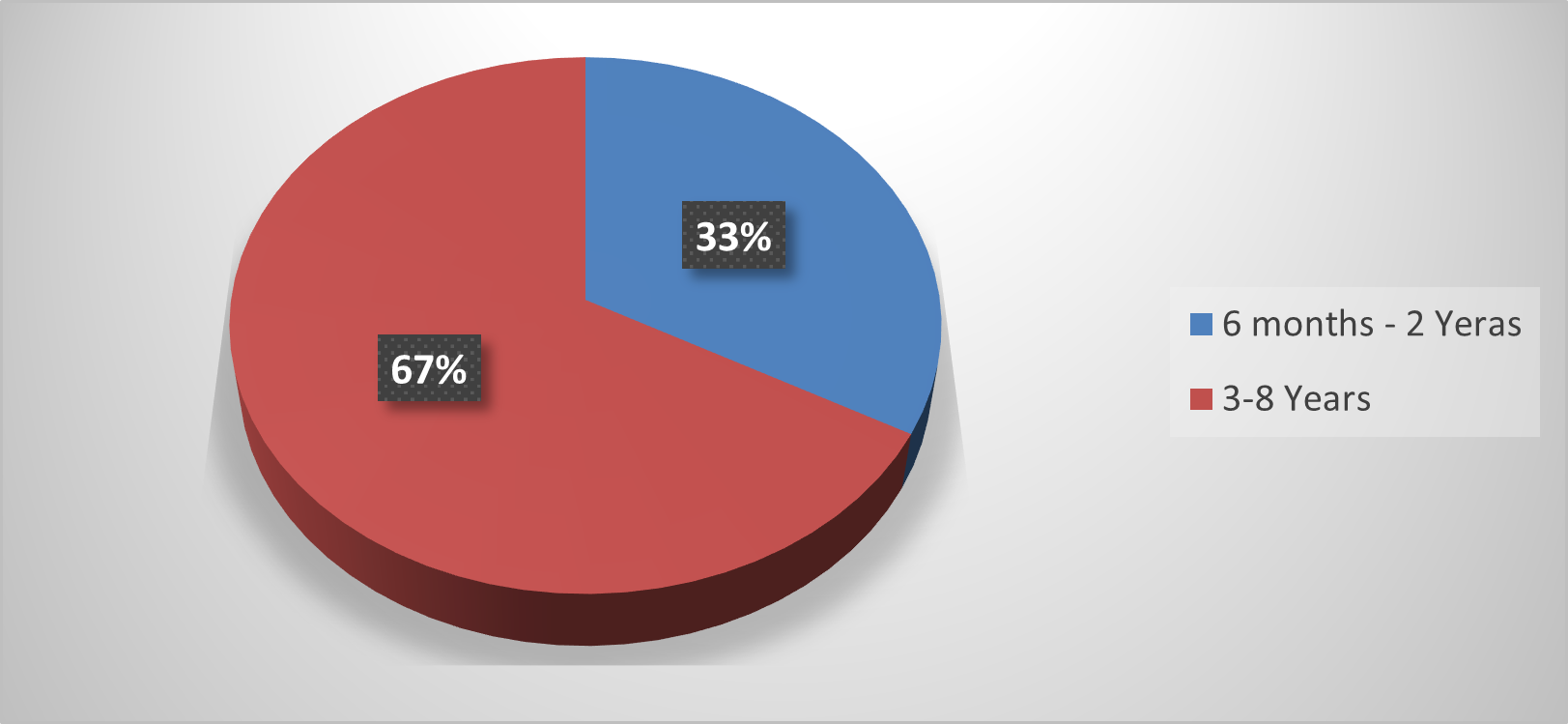
Figure 3: Duration of experience of paramedics
72% of the employees were from the General Nursing category while 28% were from the Generic Nursing category (Figure 4).
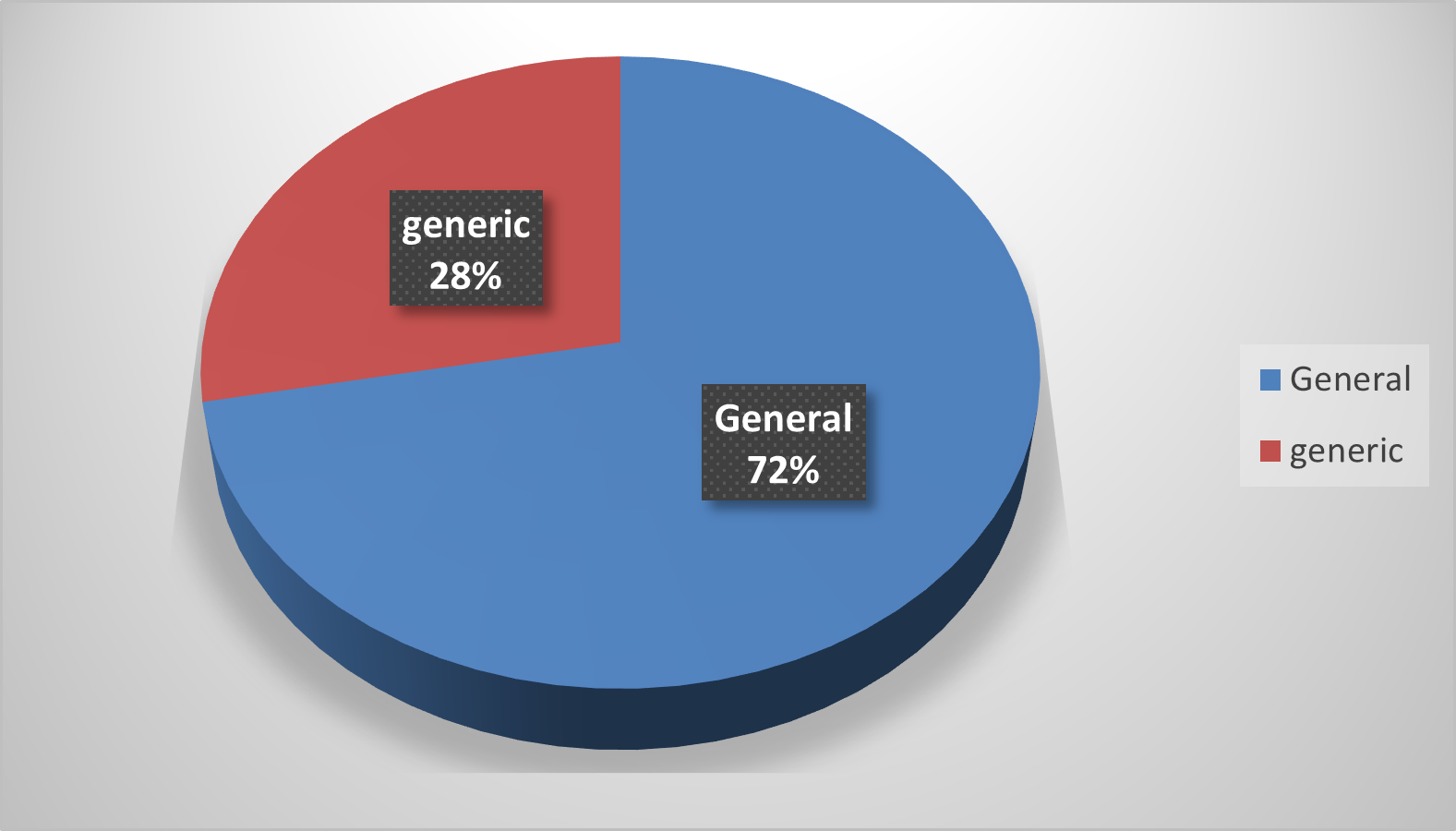
Figure 4: Educational background of paramedics
Dehumanization percentage and work impact percentages were found to be positive in 96% and 93% of paramedics (figures 5 and 6).
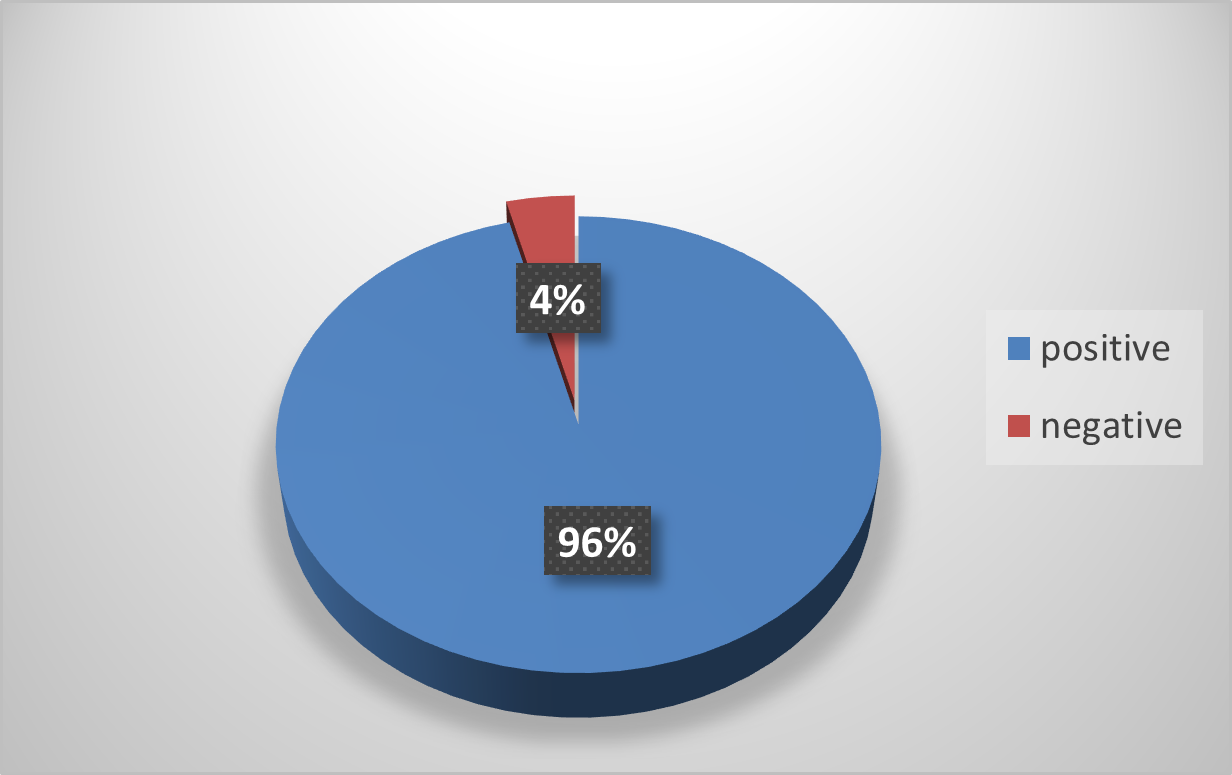
Figure 5: Dehumanization levels among paramedics
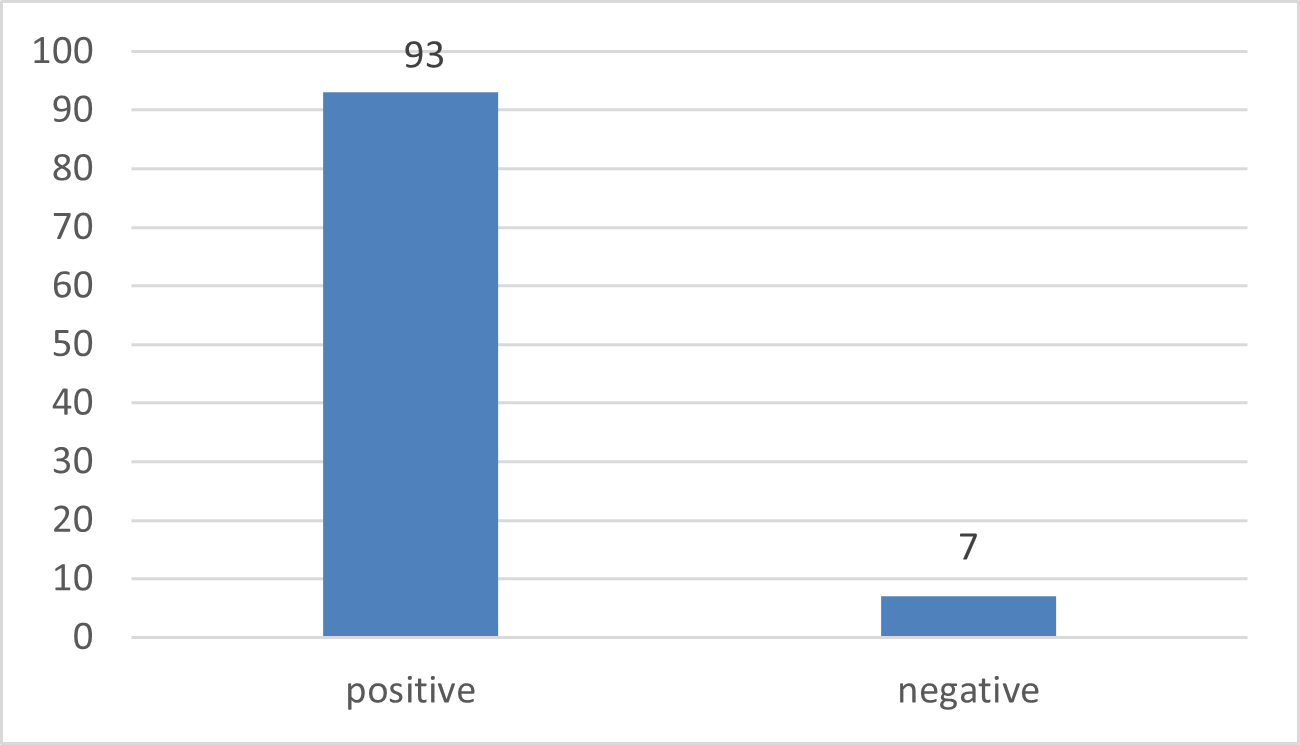
Figure 6: Impact on work capacity
Discussion
In our study on organizational dehumanization, the percentage of female employees was 59% and the percentage of male employees was 41%. A similar result was seen in the research conducted in Crete, Greece, on self-dehumanization in healthcare settings, because the majority of the paramedics are females.[6] The majority of the employees were in the age bracket of 25-35 years. Similar results were seen in the research conducted in Egypt in Ain Shams University Hospitals, where moderate levels of dehumanization were linked to a younger age of the employees.[9]
Through our study, we aimed to assess the effects of dehumanization on our paramedics, who are an important part of the health care setting. Other similar researches also agree with the importance of this phenomenon, as one of our reference research states that in recent years, the scientific community has shown an increased interest in the phenomenon of dehumanization, which has extensively been examined in the field of social psychology known that healthcare professionals, and especially doctors and nurses, frequently have to face this particularly difficult task.[6] The majority of the employees had 3-8 years of work experience. 72% of the employees were from the General Nursing category, while 28% were from the Generic Nursing category. These different categories were mentioned due to the difference in the nature of work and practice of both degrees. General Nursing employees have more work experience in the hospital setting as compared to Generic Nursing employees due to their student placements in hospitals. This point is unique to our research and not categorically mentioned by any reference research.
In our study 96% of the employees showed significant levels of dehumanization. This shows the alarming level of dehumanization among the paramedics, which hinders their job and work quality. It has a strong impact on the mental well-being of the staff members. A similar result was seen in research conducted at the Department of Psychology, Florida State University, which found that dehumanization was linked to anxiety, depression, and mental stress.[10] These results show extreme levels of discrimination against paramedics. While moderate levels of dehumanization were recorded in reference research conducted in Ain Shams Cardiovascular Hospital, this was due to the young age and shorter work experience of the employees. Extreme workloads increased psychological stress among employees.[9]
Additionally, another research study in the service industry showed that increased levels of depression, anxiety, and substance abuse have been linked with dehumanization and meta-dehumanization as well.[11] A similar study on dehumanization conducted by the Applied Psychology department at the University of Padova revealed that less stressed nurses were more effective in delivering their duties towards patients overall. This shows that the dehumanization of employees directly influences their patients’ care and the outcome of the disease in general.[8]
We further evaluated the work capacity of the paramedics as well. 93% of the employees had an impact on their work capacity, which was reduced due to extreme patterns of workload and mental stress from the work environment. One of the reference research studies conducted in Greece also found that dehumanization affecting the work quality of the healthcare worker may result in aggressive behaviour development among employees.[6] In a similar study conducted in the service industry, it was identified that dehumanization may result in employees hiding knowledge due to lower energy levels and an extreme work routine.[12]
This study also identifies methods to address dehumanization. Focused obligation for constructive change (FOCC) refers to the orientation of employees in which they feel responsible for bringing progressive changes in the organization. FOCC is used as a valuable resource that is used as a shield against losses experienced by dehumanization practices.[11] Our study identifies dehumanization as an important issue that needs attention, as it directly influences patient care and well-being.
Limitations: The sample size available was smaller according to the inclusion criteria, which limits the accuracy of the results. Also, the available gender distribution was not equal, which limits assessment in male paramedics.
Conclusion
This research concludes that dehumanization is an important workplace issue faced by paramedics. Also, its significant impact on the work capacity of paramedics should be addressed seriously by the relevant authorities in departments and the administration of the hospital. This step will improve the outcome of the work and overall have a good impact on patient care.
References
- Rubbab UE, Khattak SA, Shahab H, Akhter N. Impact of Organizational Dehumanization on Employee Knowledge Hiding. Front Psychol. 2022;13:803905. doi:10.3389/fpsyg.2022.803905
PubMed | Crossref | Google Scholar - Jenkins TA, Robison M, Joiner TE. Dehumanization and mental health: clinical implications and future directions. Curr Opin Behav Sci. 2023;50(101257):101257. doi:10.1016/j.cobeha.2023.101257
Crossref | Google Scholar - Zhenjing G, Chupradit S, Ku KY, Nassani AA, Haffar M. Impact of Employees’ Workplace Environment on Employees’ Performance: A Multi-Mediation Model. Front Public Health. 2022;10:890400. doi:10.3389/fpubh.2022.890400
PubMed | Crossref | Google Scholar - Liu Z, Chen C, Cui H, Hu Y. The relationship between nurses’ social network degree centrality and organizational citizenship behavior: The multiple mediating effects of job satisfaction and work engagement. Heliyon. 2023;9(9):e19612. doi:10.1016/j.heliyon.2023.e19612
PubMed | Crossref | Google Scholar - Abou Zeid MAG, Khedr MA, Rayan HN, Mostafa B, El-Ashry AM. The relationship between organizational dehumanization and work engagement: the mediating effect of nurses’ work stress. BMC Nurs. 2024;23(1):193. doi:10.1186/s12912-024-01841-z
Crossref | Google Scholar - Capozza D, Falvo R, Boin J, Colledani D. Dehumanization in medical contexts: An expanding research field. 2016;23:545-559. doi:10.4473/TPM23.4.8
Crossref | Google Scholar - Ibrahim R, Aly E-S, Wahba N, Abdel-Aleem M, Aleem A. Nurses’ passion for work: its relation to organizational dehumanization, exploitative leadership, and deviant behaviors during the COVID-19 pandemic. Assiut Sci Nurs J. 2024;11:56-77. doi:10.21608/ASNJ.2023.180482.1470
Crossref | Google Scholar - Roupa A, Patelarou A, Fradelos EC, et al. Validation of Two Instruments for the Measurement of Dehumanization and Self-Dehumanization in Healthcare Settings. Nurs Rep. 2024;14(3):2246-2265. doi:10.3390/nursrep14030167
PubMed | Crossref | Google Scholar - Christoff K. Dehumanization in organizational settings: some scientific and ethical considerations. Front Hum Neurosci. 2014;8:748. doi:10.3389/fnhum.2014.00748
PubMed | Crossref | Google Scholar - Haider A, Fatima T, Zia M. Organizational dehumanization and job anxiety: moderating role of passion: a conservation of resource theory perspective. J Innov Res Manag Sci. 2024;5:1-21. doi:10.62270/jirms.v5i2.71
Crossref | Google Scholar - Fontesse S, Demoulin S, Stinglhamber F, de Timary P, Maurage P. Metadehumanization and Self-dehumanization are Linked to Reduced Drinking Refusal Self-Efficacy and Increased Anxiety and Depression Symptoms in Patients with Severe Alcohol Use Disorder. Psychol Belg. 2021;61(1):238-247. doi:10.5334/pb.1058
PubMed | Crossref | Google Scholar - Brison N, Caesens G. The Relationship Between Workplace Ostracism and Organizational Dehumanization: The Role of Need to Belong and its Outcomes. Psychol Belg. 2023;63(1):120-137. doi:10.5334/pb.1215
PubMed | Crossref | Google Scholar
Acknowledgments
We acknowledge the research department of Wah Medical College, Wahcantt, for allowing us to conduct this research project. We also extend our gratitude to the dean of Wah Medical College, Prof. Dr. Musarat Ramdan, for the issuance of the official IRB letter in support of our research work.
Funding
No funding was taken for the research work.
Author Information
Corresponding Author:
Zoha Rehman
Department of Medicine
Final year MBBS student, Wah Medical College, Wah Cantonment, Punjab, Pakistan
Email: [email protected]
Co-Authors:
Sadia Nadeem
Department of Community Medicine
Assistant Professor, Wah Medical College, Wah Cantonment, Punjab, Pakistan
Zavata Afnan, Urooj Niaz, Zeeshan Hussain
Department of Medicine,
Final year MBBS student, Wah Medical College, Wah Cantonment, Punjab, Pakistan
Hira Akbar
Department of Medicine,
Second Year MBBS student, Wah Medical College, Wah Cantonment, Punjab, Pakistan
Authors Contributions
Prof. Dr. Sadia Nadeem served as the mentor for the research project, contributing significantly to data analysis and writing the methodology section. Zoha Rehman organized the manuscript and was responsible for writing the introduction and discussion sections. Zavata Afnan, Urooj Niaz, Hira Akbar, and Zeeshan Hussain contributed to the literature search and data collection for the research project.
Ethical Approval
Ethical approval for this study was granted by the Institutional Review Board (IRB) of Wah Medical College (Ref: WMC/ERC/IRB/097), dated May 23, 2025. The study was approved under certificate number ERC/IRB no. 0097 and is valid for three years, in accordance with institutional guidelines.
Conflict of Interest Statement
The authors declare no conflict of interest.
Guarantor
None
DOI
Cite this Article
Rehman Z, Nadeem S, Afnan Z, Niaz U, Akbar H, Hussain Z. Organizational Dehumanization and Its Impact on Work Capacity of Paramedics: A Cross-Sectional Study Conducted at POF Hospital, Wah Cantt. medtigo J Neurol Psychiatry. 2025;2(3):e3084232. doi:10.63096/medtigo3084232 Crossref













