






 Author Affiliations
Author Affiliations
Abstract
Background: Pediatric visual impairment is an underrecognized health disparity affecting developmental, educational, and social outcomes. Medical education offers limited exposure to visual impairment in the pediatric population. OptiKids Outreach was initiated by medical students at the University of Louisville School of Medicine to help educate students about children with visual impairment and their resilience.
Objective: To evaluate medical students’ early awareness, engagement, and support for children with visual impairment through “Resilience and Living with Vision Loss,” a patient-centered panel conducted by OptiKids Outreach and Visually Impaired Preschool Services.
Methodology: A novel pre- and post-panel survey tool evaluated 60 medical students in three key areas: (1) awareness, (2) engagement, and (3) support for visually impaired children. Students were evaluated before and after an in-person panel of families from Visually Impaired Preschool Services. Discussions included the lived experiences of childhood vision loss and barriers to access and education among healthcare providers. Data was analyzed using two-tailed paired t-tests, with statistical significance set at p < 0.05.
Results: Post-panel survey results demonstrated statistically significant improvements across all measured domains. Average awareness scores increased from 4.17 (standard deviation (SD) = 1.05) to 5.20 (SD = 0.82) (p < 0.001), engagement scores rose from 13.02 (SD = 3.03) to 16.58 (SD = 1.87) (p < 0.001), and support scores improved from 12.42 (SD = 3.25) to 16.51 (SD = 2.14) (p < 0.001).
Conclusions: Patient-centered panels like the OptiKids Outreach panel may serve as educational tools to enhance early medical student awareness, engagement, and support for visually impaired children.
Keywords
Visual Impairment, Disability awareness, Pediatric ophthalmology, Student engagement, Medical education.
Introduction
Vision impairment, particularly low vision and blindness, severely compromises quality of life when diagnosed in early childhood.[1] Measured in disability-adjusted life years (DALYs), childhood vision loss and blindness rank second only to cataracts in the global burden of eye disease and remain a priority for the World Health Organization.[2] As of 2017, 2.8% of children aged 1-14 years had distance and/or near vision impairment worldwide.[3] However, the prevalence of pediatric visual impairment may be higher due to underdiagnosis or undertreatment, particularly among children from those with lower healthcare access, such as low socioeconomic status or underrepresented racial groups.[4,5] These children are often underdiagnosed, use visual care less frequently, and are more likely to be lost to follow-up.[4,5] Delayed treatment in pediatric visual health results in poor maturation of vision.[6] These effects are particularly evident in school-aged children, as literacy skills among students with visual impairments are generally lower than those of their sighted peers, leading to slower reading speeds and increased visual fatigue during the school day (e.g., headaches, tiredness, or behavioral changes).[7] Given the visual consequences of delayed treatment, the role of medical education and community engagement becomes critical in addressing the gap in care and supporting these children.
Modern medical curricula provide students with limited exposure to pediatric ophthalmology.[8] Within the last five years, 20% of medical schools still do not mandate ophthalmology training or clinical exposure, and studies have shown that second- and fourth-year students commonly misdiagnose ocular conditions.[6,9] Over the past 50 years, U.S. medical schools have reduced preclinical ophthalmology instruction by half; in 2014, the average dedicated preclinical ophthalmology hours were just 12.5, compared to 25 hours in 1974.[9] This decrease in exposure to ophthalmology may leave future physicians less equipped to appropriately recognize and treat children with low vision, contributing to disparities in early detection and follow-up among school-aged children.[10]
OptiKids Outreach (OO) is a new student-led initiative at the University of Louisville School of Medicine (ULSOM), started in 2024, designed to bridge the gap between medical education and community-based support for visually impaired children. The mission of OO is to empower children with visual impairment and their families through medical student interaction and education. Given the underrepresentation of pediatric visual impairment in medical training, OO provides students with early engagement and educational opportunities with these populations, fostering a deeper understanding of the lived experiences faced inside and outside the clinical setting.
A key objective of OO is to raise medical students’ awareness of health equity in visual impairment through community engagement initiatives, such as patient-centered panels. These initiatives provide a mutually beneficial experience for patients who advocate for visual impairment awareness, and medical students support community programs. This allows interaction and valuable learning opportunities with visually impaired populations. Through these experiences, students strengthen their connections with local organizations, deepen their understanding of health equity, and explore potential career paths in pediatric ophthalmology.
This study assesses the impact of a patient-centered panel, “Resilience and Living with Vision Loss,” on medical students’ early awareness, engagement, and support for children with visual impairment. It also assesses whether this early educational panel affects student motivation or the likelihood of future engagement with community visual impairment programs.
Methodology
Study design and participants: This study utilized a pre- and post-panel survey tool to assess the impact of the “Resilience and Living with Vision Loss” panel on medical students’ awareness, engagement, and support for visually impaired individuals. The panel was hosted by OO at the ULSOM with guests from the Kentucky Visually Impaired Preschool Services (VIPS). The event was open to all medical students. Participants were recruited through email announcements, flyers, student organizations, and word-of-mouth. Participation was voluntary. Before the panel began, electronic informed consent was offered.
Inclusion criteria included (1) currently enrolled ULSOM medical student and (2) in-person attendance throughout the OO “Resilience and Living with Vision Loss” panel. All non-current medical students in attendance were excluded from the survey analysis.
Panel structure and content: The “Resilience and Living with Vision Loss” panel featured a diverse group of nine speakers, including a legally blind second-year medical student and his mother, a pediatric ophthalmologist, a vision rehabilitation specialist, and parents of children with visual impairments. The 90-minute discussion covered topics such as the lived experiences of children with vision loss, challenges in medical education and clinical practice, and strategies to improve accessibility in healthcare specific to the unique needs of visually impaired individuals. The event also included a question-and-answer session to foster interactive learning.
The multiple perspectives portrayed at the panel highlight the multifaceted and unique experiences of living with visual impairment and sensory disabilities. The parents of children with visual impairment provided significant insight into the societal and healthcare disparities they have faced regarding their child, including difficulties supporting the child’s growth and independence, the child’s everyday experiences navigating the world and varied healthcare settings, and the lack of support from healthcare systems.
Survey instrument: A literature review using PubMed was conducted to identify previously validated survey instruments regarding medical student education and awareness of visual impairment. Keywords included “medical student,” “visual impairment,” “awareness,” “education,” and “survey.” This search identified a few international surveys observing parental or public knowledge of visual impairment and its causes, but nothing specific to medical students or ophthalmology medical education in the United States.[11,12] This dearth of tools spurred the creation of a novel survey instrument utilizing the expertise of the Department of Ophthalmology and Visual Sciences and including Undergraduate Medical Education at the University of Louisville School of Medicine. The questions within the new survey tool underwent expert review by board-certified academic ophthalmologists to assess clarity, relevance, and appropriateness, supporting face validity. No formal psychometric testing, such as statistical assessment of internal consistency, was performed. The Institutional Review Board reviewed and approved the survey instrument as appropriate for the study.
A novel structured questionnaire was designed to evaluate medical students’ perspectives before and after attending the “Resilience and Living with Vision Loss” panel (Table 1).
| Survey question | Response options |
| What is your gender? | Male, Female, Non-binary, prefer not to say |
| What year of medical school are you in? | M1, M2, M3, M4, I am not a medical student |
| If applicable, please mark all of the student interest groups you are a member of: | OptiKids Outreach, Ophthalmology Interest Group, Pediatric Interest Group, Family Medicine Interest Group, Neurology Interest Group, Ear, Nose, and Throat (ENT) Interest Group, Other |
| Have you ever interacted with children with visual impairment or blindness? | Yes, No, No Opinion |
| Which of the following experiences have you had with a person with visual impairment? (Mark all that apply) | Medical setting, Education setting, As a family member, As a friend, As a community volunteer, None of the above, Other… |
| Visual impairment involves vision that cannot be corrected to a normal level. | True, False, No Opinion |
| Premature birth can cause visual impairment. | True, False, No Opinion |
| What is Cortical Visual Impairment (CVI)? | Damage to the optic nerve, Damage to the retina caused by premature birth, Damage to the visual processing areas of the brain, No Opinion |
| Cataracts can lead to permanent blindness in children | True, False, No Opinion |
| What is the best corrected visual acuity in the better-seeing eye for a person to be considered legally blind? | 20/20, 20/100, 20/200, 20/400, No Opinion |
| What does treating amblyopia try to prevent? | Decreased sun exposure to eyes, Decreased vision in one or both eyes, Degeneration of the optic nerve, Decreased night vision, No Opinion |
| I am able to identify a child with visual impairment | 1 Strongly Disagree, 2 Disagree, 3 No Opinion, 4 Agree, 5 Strongly Agree |
| I can engage with people with visual impairment to address their health needs | 1 Strongly Disagree, 2 Disagree, 3 No Opinion, 4 Agree, 5 Strongly Agree |
| I can engage with people with visual impairment to address their social needs | 1 Strongly Disagree, 2 Disagree, 3 No Opinion, 4 Agree, 5 Strongly Agree |
| I can engage with the families of individuals with visual impairment to assess their general needs | 1 Strongly Disagree, 2 Disagree, 3 No Opinion, 4 Agree, 5 Strongly Agree |
| I understand the health needs of individuals with visual impairment | 1 Strongly Disagree, 2 Disagree, 3 No Opinion, 4 Agree, 5 Strongly Agree |
| I understand the social needs of individuals with visual impairment | 1 Strongly Disagree, 2 Disagree, 3 No Opinion, 4 Agree, 5 Strongly Agree |
| I feel comfortable providing support for a person with visual impairment | 1 Strongly Disagree, 2 Disagree, 3 No Opinion, 4 Agree, 5 Strongly Agree |
| I feel comfortable providing care for a person with visual impairment | 1 Strongly Disagree, 2 Disagree, 3 No Opinion, 4 Agree, 5 Strongly Agree |
Table 1: OO Educational survey of vision loss and resilience questions and their corresponding response options. Identical questions were asked in both the pre-panel survey and the post-panel survey, and survey responses were linked anonymously.
It was structured into three sections:
- Awareness: Understanding participants’ knowledge of visual impairment and its impact on child development.
- Engagement: Estimating participants’ willingness to interact with and advocate for visually impaired individuals and their unique needs.
- Support: Identifying participants’ comfort level in providing care and assistance to individuals with vision loss.
The final 20-question survey tool consisted of a combination of multiple-choice, true/false, and 5-point Likert-scale items. The multiple-choice and true/false questions were limited to the awareness section and had correct answers. The awareness section had six items. Likert scale items (1 = strongly disagree, 5 = strongly agree) comprised the remaining engagement and support sections to allow the participant to gauge their self-confidence and skills working with individuals with visual impairment. The engagement and support each had four Likert-scale items.
The survey’s design philosophy was to competently compare improvements in knowledge and self-confidence regarding working with visually impaired individuals as a result of a pediatric ophthalmology-related medical education event. As the survey was targeted for medical students, it was designed to be brief to maximize participation. To compare pre- and post-event scores while maintaining confidentiality, de-identified numbers consisting of the last five digits of the student’s school ID number were obtained in the demographics section. This allowed for the matching of pre- and post-event surveys with a unique number to identify improvements in score, maintaining the privacy of the student. No other personal identifiable information was gathered.
Data collection and analysis: Surveys were hosted using Qualtrics and distributed electronically before and immediately after the “Resilience and Living with Vision Loss” panel discussion. Both pre- and post-event surveys used identical questions to identify the improvement of participants’ awareness, engagement, and support scores after the panel. Students were given about five to ten minutes to fill out each survey. Qualitative feedback was recorded based on informal comments made by participants during and after the panel.
Descriptive statistics were used to summarize demographic data. Two-tailed paired t-tests were conducted to analyze pre- and post-event awareness, engagement, and support scores and identify statistical improvement after the panel. Pre- and post-event survey scores were graded by the number of correct answers for the awareness section, ranging from 0 to 6, and the summation of the 5-point Likert scale items for the engagement and support sections, ranging from 4 to 20 for each section. Statistical significance was set at p < 0.05. Data was analyzed using SPSS software (version 27.0, IBM Corp).
Ethics declaration: The study protocol was reviewed and approved by the Institutional Review Board (IRB) at the University of Louisville (IRB # 24.0789). All participation was voluntary, and responses were deidentified to maintain participant privacy. De-identified, partial student ID numbers were used to match the participants’ responses in the pre-panel and post-panel surveys for analysis.
Results
Overall, student body attendance was limited, with about one-fifth of the first-year medical student class (n = 31 of 162 first-year students, 19%) attending the panel. The majority of student participants were first (n = 31, 52%) and second year (n = 20, 33%) pre-clinical medical students, with relatively little representation among the clinical third (n = 7, 12%) and fourth year (n = 2, 3%) classes. In total, 65 medical students attended the panel, with 63 completing the surveys. Among the 63 completing the surveys, two participants’ pre- and post-event surveys were unable to be matched due to a mismatch in identification numbers. Additionally, one participant did not complete any post-event survey questions. These three participants’ entries were omitted from the analysis, leaving 60 participants in the final analysis (Figure 1).
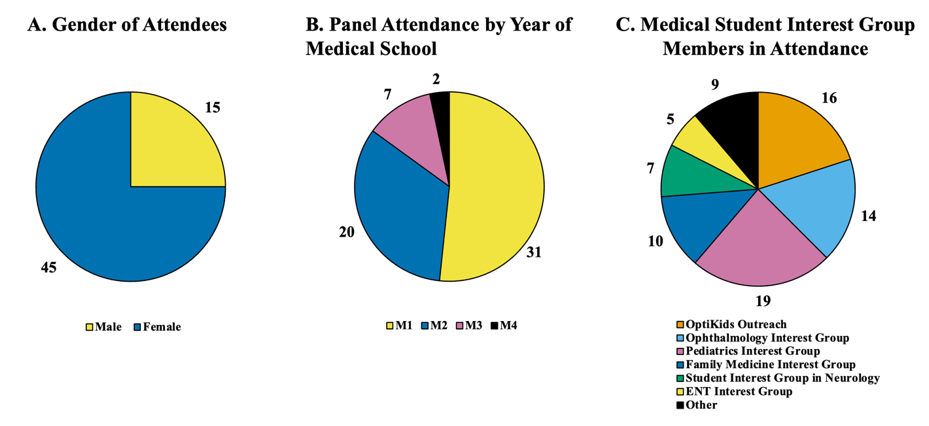
Figure 1: Demographics of attendees at the “Resilience and Living with Vision Loss” panel
A) Distribution of attendees by year in medical school. B) Medical student interest group affiliations; participants could select multiple groups. C) Gender distribution of attendees
The participants were predominantly female (n = 45, 75%). Participants represented a wide range of interest groups, with the Pediatrics interest group being the most predominant at 32% (n = 19), followed by OO at 27% (n = 16), Ophthalmology interest group at 23% (n = 14), Family Medicine at 17% (n = 10), and Neurology at 12% (n = 7). About 23% of participants (n = 14) also noted participation in other interest groups, including the ENT interest group, Emergency Medicine, Internal Medicine, and more.
The majority of the student participants, 55% (n = 33), never interacted with a child with visual impairment or blindness, compared to 43% (n = 26) with prior interactions. 67% of participants (n = 40) had prior interaction with a person with visual impairment or blindness, citing the medical setting as the most common exposure at 42% of participants (n = 25) followed by friend/acquaintance (n = 14, 23%), community volunteer (n = 13, 22%), educational setting (n = 12, 20%), family member (n = 8, 13%), and other (n = 5, 8%). The majority of students were pre-clinical students, particularly first-year students (52%), with twelve (38.7%) having prior interactions, compared to eighteen (58%) without prior interactions. However, there was no statistical difference between first-year medical students and all other participants. In addition, there was no statistical difference in scores between students who had interactions with children with visual impairments versus those who had no interactions.
The “Resilience and Living with Vision Loss” panel increased medical students’ early awareness, engagement, and support for visually impaired individuals and their families. Pre- and post-panel survey data analysis demonstrated statistically significant improvements across all domains (Figure 2).
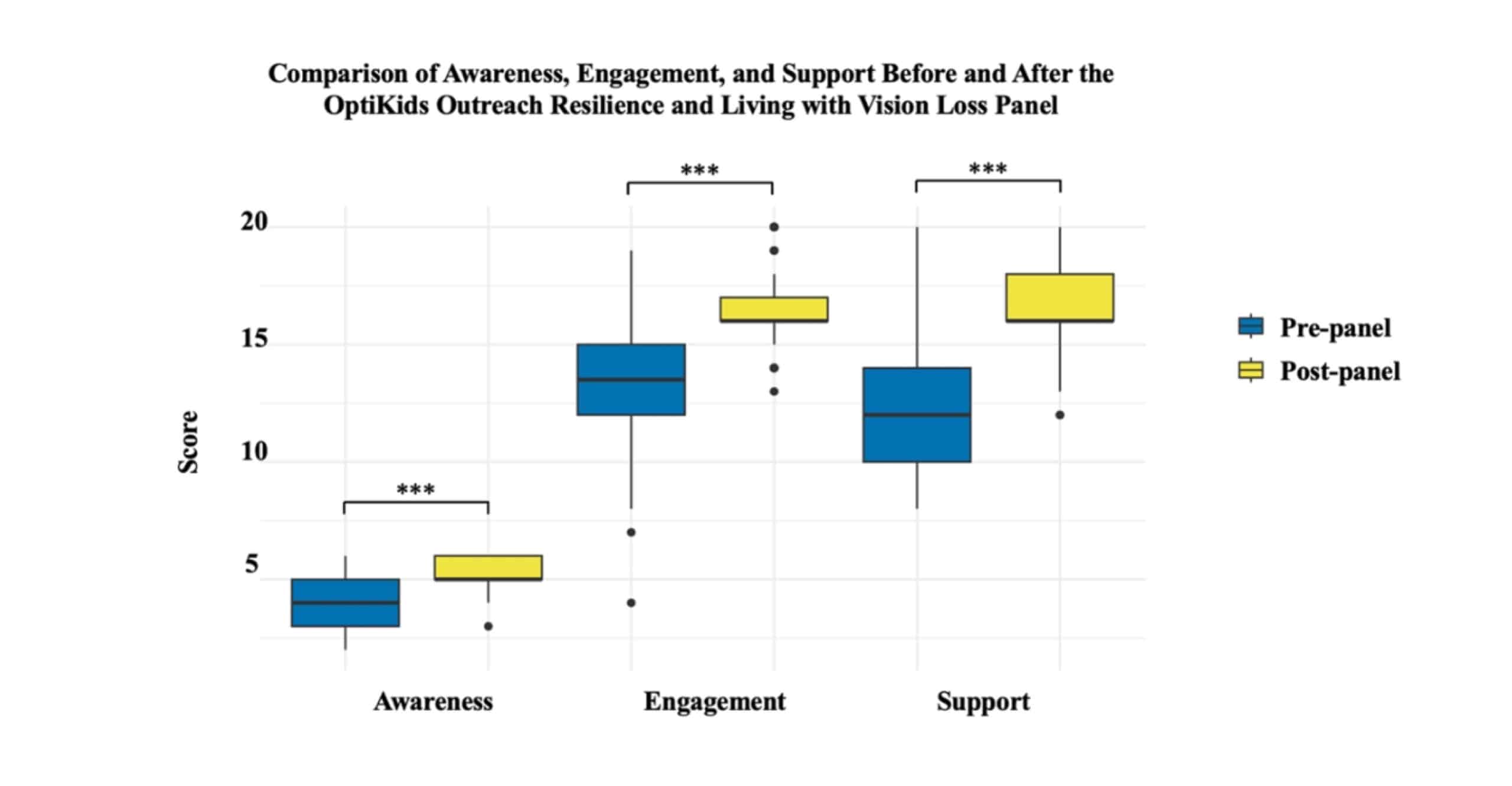
Figure 2: The statistically significant difference in medical students’ (n = 60) perceived awareness, engagement, and support for visually impaired children and their families before the “Resilience and Living with Vision Loss” panel and after the “Resilience and Living with Vision Loss” panel; *** = p < 0.001
Awareness scores increased from 4.17 ± 1.11 to 5.20 ± 0.68 (p < 0.001), engagement scores rose from 13.02 ± 9.19 to 16.58 ± 3.52 (p < 0.001), and support scores improved from 12.42 ± 10.59 to 16.51 ± 4.60 (p < 0.001). Average awareness scores increased from 4.17 (standard deviation [SD] = 1.05) to 5.20 (SD = 0.82) (p < 0.001). Similarly, average engagement scores rose from 13.02 (SD = 3.03) to 16.58 (SD = 1.87) (p < 0.001). Support scores showed the largest improvement, increasing from 12.42 (SD = 3.25) to 16.51 (SD = 2.14) (p < 0.001). These findings are illustrated in Figure 2.
Qualitative feedback reinforced the impact of the panel, with students highlighting the value of firsthand storytelling and interactive discussions. Beyond limited exposure to visual impairment in the pediatric population, medical students also have minimal exposure to their peers with early childhood disabilities, especially of the sensory type.[8] We were fortunate to have the University of Louisville School of Medicine’s first legally blind medical student on the panel, along with his mother, to help provide a peer’s firsthand perspective of growing up with visual impairment. Despite his disability, the student highlighted how early pediatric treatment and interventions like magnified text shaped his confidence at an early age. Moreover, his family’s persistent support to help both his brother and him adapt early to their visual impairments further shaped his educational goals at a young age. Attendees reported that hearing from a legally blind peer who emphasized the role of family and medical support in childhood impacted their views on early intervention and support for those with visual impairment. Finally, his inclusion facilitated early discussions about possible student-led interventions for this population, such as neon signs, sensory rooms, and one-on-one tutors, compared to the limited resources previously available when he was in preschool.
Discussion
Examining the statistically significant changes in awareness, engagement, and support scores offers insight into the educational value of the panel. The improved awareness score may reflect a greater understanding of pediatric visual impairment and its impact on child development. Similarly, improvement in engagement scores may suggest an increased motivation among students to interact with and advocate for visually impaired families. Support scores in an observational one-panel survey may oversimplify students’ confidence in their ability to engage without direct engagement with this patient population. However, structured patient-centered educational interventions can help bridge gaps in medical education, and with more application, could enhance limited educational exposure, such as pediatric ophthalmology and disability advocacy.
Both the parents and the vision rehabilitation specialist representing VIPS provided significant insight into practices that can be implemented at the hospital. This included (1) utilizing color-guided floor lines, (2) protecting sharp corners with special highlighting, and (3) implementing touch and sound-based methods for personal interaction. Also, hearing from a visually impaired medical student peer about his early childhood experience left a profound impact on the relatability and strength of the panel’s message. Finally, the pediatric ophthalmologist engaged students in a brief discussion on how he works with visually impaired populations from the physician’s perspective. Overall, the discussion seemed to provide students with a more holistic perspective on families caring for those living with visual impairment.
The initial success of this single educational panel supports the expansion of similar interactive programs to equip future physicians with the knowledge and confidence to provide inclusive, patient-centered care. Our findings demonstrate that interactive panel discussions may enhance medical students’ understanding, knowledge, and empathy for pediatric patients with visual impairments beyond traditional lectures and textbooks. Patient-centered educational panels may add value to medical curricula by addressing gaps in disability education across all four years of medical school, as we found limited exposure to pediatric visual impairment among students at every level.
Limitations of the study included the creation of a novel survey tool due to the lack of previously validated pediatric visual impairment survey tools in the current literature. The survey design lacked prior validity testing to estimate medical students’ early awareness, engagement, and support for visually impaired populations. Expert opinion from the Department of Ophthalmology was obtained in the creation of the survey tool; however, a pilot test among medical students would have maximized validity. Another limitation is selection bias. Students selected to attend this panel may have greater motivation and show greater improvement in scores compared to a session that the entire class attends. In addition, the majority in attendance were first- and second-year pre-clinical students, which may account for differences observed in the survey results. However, the curriculum provides very limited exposure to clinical experiences beyond the one-week introduction to non-clinical basic ophthalmology during the second year. The small sample size of clinical-level students lacked sufficient power to provide significant insight into this population.
This one-time survey is further limited by the inability to capture whether improvements in awareness, engagement, and support for visually impaired children were sustained over time. Future comparative research should examine the long-term impact of integrating similar panels for medical education. Surveying the pre-clinical medical students who attended the original panel and even those not in attendance after completing the core clinical clerkships may reveal increased awareness, engagement, and support for pediatric visual disabilities. Additionally, this study is limited by a small sample size, without inclusion of the majority of the student body, and lacks a representative exposure group. Sampling a wider student population will allow for broader assessment of student awareness, engagement, and support. This, in turn, can help broaden medical educational tools for those impacted by severe pediatric vision loss. Finally, panel facilitation during the daytime school hours, or virtually, may increase medical student attendance. To overcome after-hours, less attended educational events, it may be beneficial to incorporate similar panels during ongoing current humanitarian pre-clinical courses or other daytime activities.
References
- Chadha RK, Subramanian A. The effect of visual impairment on quality of life of children aged 3-16 years. Br J Ophthalmol. 2011;95(5):642-645. doi:10.1136/bjo.2010.182386
PubMed | Crossref | Google Scholar - Keeffe J. Childhood vision impairment. Br J Ophthalmol. 2004;88(6):728-729. doi:10.1136/bjo.2003.040006
PubMed | Crossref | Google Scholar - Abdolalizadeh P, Chaibakhsh S, Falavarjani KG. Global burden of paediatric vision impairment: a trend analysis from 1990 to 2017. Eye (Lond). 2021;35(8):2136-2145. doi:10.1038/s41433-021-01598-8
PubMed | Crossref | Google Scholar - Stein JD, Andrews C, Musch DC, Green C, Lee PP. Sight-Threatening Ocular Diseases Remain Underdiagnosed Among Children of Less Affluent Families. Health Aff (Millwood). 2016;35(8):1359-1366. doi:10.1377/hlthaff.2015.1007
PubMed | Crossref | Google Scholar - Shoshany TN, Chinn RN, Staffa SJ, Bishop K, Michalak S, Hunter DG. Identifying Characteristics Predictive of Lost-to-Follow-Up Status in Amblyopia. Am J Ophthalmol. 2021;230:200-206. doi:10.1016/j.ajo.2021.05.002
PubMed | Crossref | Google Scholar - Esparaz ES, Binder SB, Borges NJ. How prepared are medical students to diagnose and manage common ocular conditions. J Educ Eval Health Prof. 2014;11:29. doi:10.3352/jeehp.2014.11.29
PubMed | Crossref | Google Scholar - Antonio-Aguirre B, Ambrosino CM, Dai X, Collins ME. Addressing Health Disparities in Pediatric Eye Care for School-Age Children: A Call to Action. Transl Vis Sci Technol. 2023;12(11):17. doi:10.1167/tvst.12.11.17
PubMed | Crossref | Google Scholar - Liao J, Wright RR, Vora GK. The Decline of Basic Ophthalmology in General Medical Education: A Scoping Review and Recommended Potential Solutions. J Med Educ Curric Dev. 2024;11:23821205241245635. doi:10.1177/23821205241245635
PubMed | Crossref | Google Scholar - Moxon NR, Goyal A, Giaconi JA, et al. The State of Ophthalmology Medical Student Education in the United States: An Update. Ophthalmology. 2020;127(11):1451-1453. doi:10.1016/j.ophtha.2020.05.001
PubMed | Crossref | Google Scholar - Antonio-Aguirre B, Ambrosino CM, Dai X, Collins ME. Addressing Health Disparities in Pediatric Eye Care for School-Age Children: A Call to Action. Transl Vis Sci Technol. 2023;12(11):17. doi:10.1167/tvst.12.11.17
PubMed | Crossref | Google Scholar - Alshammari LK, Alaradi LA, Alanazi AM, et al. Levels of awareness regarding pediatric eye diseases among Saudi parents from the Hail and Al-Qassim regions, Saudi Arabia. Cureus. 2024;16(4):e57871. doi:10.7759/cureus.57871
Crossref | Google Scholar - Lupón M, Cardona G, Armayones M. Public knowledge of low vision and blindness, and readability of on-topic online information. J Optom. 2021;14(3):240-246. doi:10.1016/j.optom.2020.06.005
PubMed | Crossref | Google Scholar
Acknowledgments
The authors wish to thank the volunteer members of OptiKids Outreach, the Department of Ophthalmology & Visual Sciences, and the Undergraduate Medical Education Faculty at the University of Louisville School of Medicine for their overall support.
Funding
None
Author Information
Corresponding Author:
Shorye Durrett
Department of Ophthalmology & Visual Sciences
University of Louisville School of Medicine, Louisville, KY, USA
Email: shorye.durrett@louisville.edu
Co-Authors:
George Nemeth, Caroline G. Ploeger, Tanya Gupta, Shelby Lands, Cole Wyatt, Shreya Pandya
University of Louisville School of Medicine, Louisville, KY, USA
Joern Soltau
Department of Ophthalmology & Visual Sciences
University of Louisville School of Medicine, Louisville, KY, USA
Authors Contribution
Shorye Durrett and George Nemeth contributed to the conceptualization of the study. All the authors were involved in the investigation and data curation of the study. George Nemeth and Caroline Ploeger contributed to the organization of the manuscript. All authors collectively were involved in the writing (original draft preparation and writing) of the manuscript. All authors contributed to reviewing, editing, and refining the manuscript.
Ethical Approval
The study protocol was reviewed and approved on 11/06/2024 by the IRB at the University of Louisville (IRB # 24.0789). Electronically informed consent was offered before participants filled out the pre- and post-survey tool in this study.
Conflict of Interest Statement
The authors declare no conflict of interest.
Guarantor
None
DOI
Cite this Article
Nemeth G, Ploeger CG, Gupta T, et al. OptiKids Outreach: Enhancing Medical Student Awareness, Engagement, and Support for Pediatric Visual Impairment Through a Patient-Centered Panel. medtigo J Med. 2026;4(1):e3062418. doi:10.63096/medtigo3062418 Crossref













