






 Author Affiliations
Author Affiliations
Abstract
Background: Autosomal dominant hyper-IgE syndrome (AD-HIES), caused by signal transducer and activator of transcription 3 (STAT3) mutations, is a rare primary immunodeficiency disorder characterized by recurrent eczema-like rashes, skin and pulmonary abscesses, and significantly elevated serum IgE levels. The purpose of this article is to highlight the distinct clinical presentation, the importance of genetic studies in diagnosing AD-HIES, and the role of bronchoscopy lavage in managing pulmonary complications.
Case report: Herein, we report a 9-year-11-month-old girl of Chinese origin who presented with recurrent eczema-like rashes, fingertip abscesses, and recurrent pulmonary infections. In her past medical history, she experienced severe allergies to seafood and peanuts, and frequent infections such as congenital pneumonia, recurrent bacterial and viral pneumonia, and cutaneous abscesses. The immunological workup revealed normal T cells, B cells, and natural killer cells (TBNK) panel, normal general immunology results, and an increase in IgE level > 5000 IU/mL. The genetic testing confirmed a heterozygous STAT3 mutation (autosomal dominant) while the National Institutes of Health (NIH) AD-HIES score was 45 (>40, highly suggestive of Job Syndrome). She underwent extensive immunological and genetic workups, including STAT3 expression testing via flow cytometry, which showed normal expression despite the detected pathogenic variant. Bronchoscopy lavage was performed as part of her pulmonary infection management, which was preferred over surgical intervention.
Conclusion: Further studies on STAT3 mutations are required to better understand genotype-phenotype correlations in HIES. Bronchoscopy lavage should be considered over invasive procedures for managing pulmonary infections in pediatric patients with HIES.
Keywords
Hyper-IgE syndrome, STAT3 mutation, Pulmonary infection, Lung lavage, Immunodeficiency.
Introduction
Autosomal dominant hyper-IgE syndrome (AD-HIES), also known as Job syndrome, is caused by mutations in the STAT3 gene, which impairs the immune system’s ability to mount effective responses to infections.[1] The clinical features include recurrent eczema-like rashes, pulmonary infections, skin abscesses, and significantly elevated IgE levels. While numerous STAT3 mutations have been identified, the exact genotype-phenotype correlation remains poorly understood. This case report details a novel STAT3 mutation in a child with a unique clinical presentation of recurrent pulmonary infections, which underscores the importance of genetic testing and bronchoscopy lavage in managing these complex patients.
Case Presentation & Management
Patient Background: A 9-year-11-month-old Chinese girl, presenting complaints with recurrent eczema, severe allergies, and multiple infections since infancy. Notable history includes congenital pneumonia, recurrent respiratory infections, cutaneous abscesses, and multiple fungal and bacterial infections. Physical Examination revealed eczema-like rashes across her body, finger-tip abscesses, and recurrent pulmonary infections.

Figure 1: Scars following the recurrent cutaneous infection
Key laboratory findings: The patient’s serum IgE level was markedly elevated at over 5000 IU/mL, which is highly suggestive of an atopic phenotype. The NIH AD-HIES score was 45, exceeding the threshold of 40 and strongly indicating Job Syndrome (Autosomal Dominant Hyper-IgE Syndrome). The lymphocyte proliferation test (LPT) showed reduced T-cell proliferation compared to controls, pointing to impaired cellular immune function. Despite this, the patient demonstrated a normal specific antibody response to both tetanus toxoid and pneumococcal vaccines, indicating intact humoral immunity. Genetic analysis confirmed the presence of a pathogenic heterozygous mutation in the STAT3 gene, establishing the diagnosis of Job Syndrome.
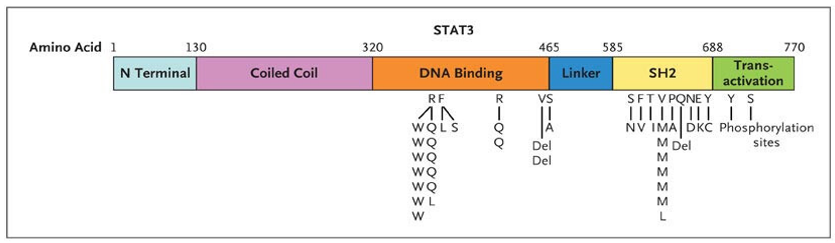
Figure 2: Genomic deoxyribonucleic acid (DNA) analysis, STAT3 Mutations
Infection history: During the neonatal period, the patient developed congenital pneumonia requiring continuous positive airway pressure (CPAP) support. Throughout childhood, they experienced multiple episodes of pneumonia, including infections caused by respiratory syncytial virus (RSV) and Mycoplasma pneumoniae. The patient also had recurrent abscesses, notably methicillin-sensitive Staphylococcus aureus (MSSA)-positive shoulder and cervical lymphadenitis. Fungal infections were documented, including onychomycosis, oral candidiasis, and detection of Aspergillus niger. At the age of five, high-resolution computed tomography (HRCT) of the thorax confirmed the presence of right middle lobe bronchiectasis.
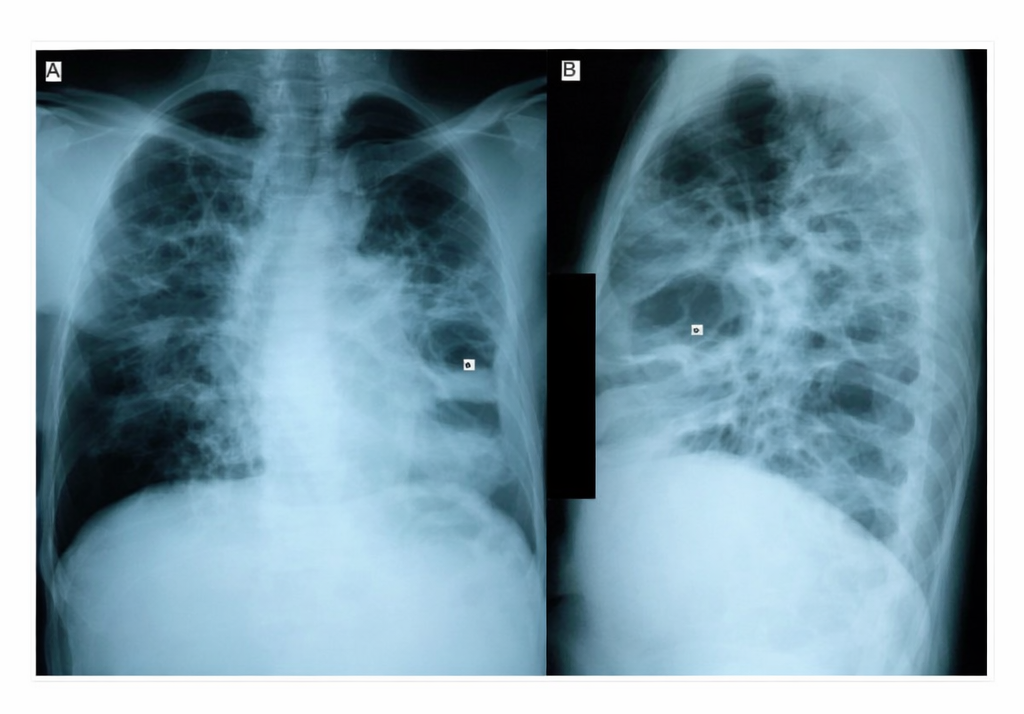
Figure 3: Chest radiograph on admission (A: posteroanterior and B: lateral view) showing multiple thin‐walled cysts (pneumatoceles) with air‐fluid level
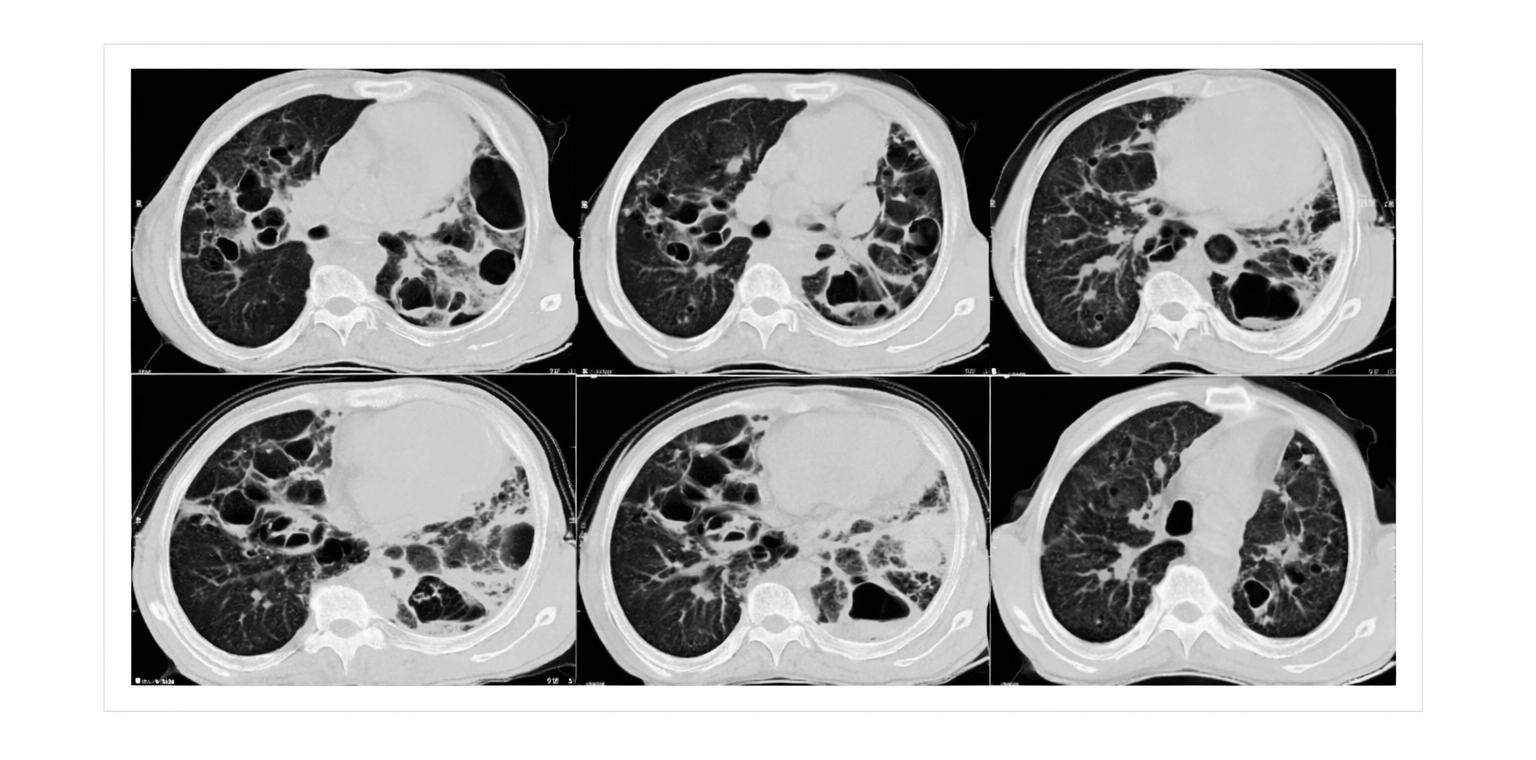
Figure 4: Chest computer tomography (CT) scan on admission showed multiple and large pneumatoceles, some with air‐fluid level consistent with superinfection mainly at middle and lower lung fields, mild consolidation, bronchiectasis, and left pleural thickening
Immunological & functional Studies: STAT3 expression was found to be normal despite the presence of a pathogenic mutation, which is a common feature observed in Job Syndrome. The neutrophil oxidative burst assay using dihydrorhodamine (DHR) was normal, indicating intact neutrophil function. However, LPT demonstrated a reduced response to mitogens, suggesting impaired T-cell proliferation. Additionally, isohemagglutinin titers were elevated, further supporting the presence of immune dysregulation.
Management and treatment: The patient is on prophylactic antibiotic therapy with trimethoprim-sulfamethoxazole (Bactrim) at a dose of 130 mg every other day. For antifungal prophylaxis, itraconazole is administered at 100 mg once daily. Bronchodilator therapy includes the use of a salbutamol metered dose inhaler (MDI) as needed. A corticosteroid inhaler, fluticasone, was previously used but was discontinued in November 2021. The patient is followed by immunology specialists every two months. For pulmonary management, bronchoscopy with lavage is employed during pulmonary infections to aid in diagnosis and treatment.
Discussion and diagnosis: This patient presents clinical and laboratory features highly suggestive of Hyper-IgE Syndrome (Job Syndrome), which is characterized by severe eczema, recurrent skin abscesses, elevated IgE levels, recurrent respiratory infections, and STAT3 mutation (autosomal dominant). The presence of these hallmark findings confirms the diagnosis.[2]
The elevated serum IgE (>5000 IU/mL), reduced T-cell proliferation (LPT), and the NIH AD-HIES score (45) are all critical in leading to the diagnosis. The patient has a history of recurrent bacterial, viral, and fungal infections, which are typical in Job Syndrome due to impaired immunity, specifically related to T-cell dysfunction.[3]
Management and prognosis: While there is no definitive cure for Job Syndrome, management focuses on prophylactic antibiotics and antifungal treatments to reduce infection risk—pulmonary care to manage recurrent respiratory infections and bronchiectasis. Regular immunology follow-ups are necessary to monitor immune function and prevent infections. The prognosis varies depending on the severity of the condition and the presence of complications. Early interventions and preventive treatments significantly improve outcomes and quality of life.
Differential diagnosis: Given the complexity of the patient’s clinical presentation, the differential diagnosis for her symptoms may include severe combined immunodeficiency (SCID). SCID can present with recurrent infections and eczema, but the reduced LPT and the genetic confirmation of STAT3 mutation steer the diagnosis toward Job Syndrome rather than SCID. The differential diagnosis also includes Wiskott-Aldrich Syndrome (WAS), which can present with eczema, recurrent infections, and immune dysregulation. However, thrombocytopenia was not observed in this patient, which is a key distinguishing feature of WAS. Chronic granulomatous disease (CGD), another consideration due to recurrent infections, is characterized by neutrophil dysfunction; however, a normal DHR assay in this patient effectively rules out CGD. While the presence of eczema could suggest atopic dermatitis, the combination of recurrent infections, markedly elevated IgE levels, and a confirmed pathogenic STAT3 mutation makes Hyper-IgE Syndrome (Job Syndrome) the most consistent diagnosis.
Genetics of Job syndrome: The STAT3 mutation is crucial in diagnosing Autosomal Dominant Hyper-IgE Syndrome (AD-HIES), also known as Job Syndrome. STAT3 plays a central role in regulating immune responses, and mutations in this gene lead to the characteristic immune dysregulation seen in Job Syndrome, including defects in T-helper cell function and increased susceptibility to infections. The patient has a heterozygous mutation in STAT3, indicating an autosomal dominant inheritance pattern. This suggests that one affected parent could potentially pass on the mutation; however, genetic testing of the parents was negative, implying the mutation may be de novo or undetected in the parents.
Treatment rationale:
- Prophylactic antibiotics (Bactrim): Regular use of Bactrim is recommended to prevent bacterial infections, particularly pneumonia, which is a common complication in patients with Job Syndrome due to impaired immune function.
- Antifungal prophylaxis (Itraconazole): Patients with Job Syndrome are at increased risk for fungal infections such as Candidiasis and Aspergillus. Itraconazole is used prophylactically to reduce the incidence of these infections.
- Bronchodilator therapy: Bronchodilators are employed to manage recurrent respiratory infections and alleviate bronchospasm, which may occur, especially in cases of bronchiectasis, which is often seen in these patients.
- Inhaled corticosteroids (Fluticasone): Fluticasone was part of the treatment regimen but was discontinued in November 2021. This decision may have been due to concerns about potential side effects or a lack of effectiveness in the setting of the patient’s underlying immune dysregulation.
- Immunology follow-ups: Regular follow-ups with immunology are crucial for monitoring infection development and adjusting treatment protocols. This ensures timely and appropriate management of the patient’s immune deficiencies.
- Bronchoscopy lavage: This procedure is used to manage pulmonary infections in a less invasive manner. It serves as a diagnostic and therapeutic tool that can help avoid the need for more aggressive interventions, such as surgery.
Complications and prognosis infections: Recurrent infections, including respiratory issues, skin abscesses, and fungal infections, are a major concern in this patient and highlight the need for early prophylactic treatment to improve outcomes. Bronchiectasis, already present in this patient, could progressively worsen if infections are not adequately managed. Children with Job Syndrome may also experience growth delays or developmental issues due to the persistent nature of recurrent infections and immune dysregulation. This case underscores the importance of recognizing the signs of Hyper-IgE Syndrome (Job Syndrome) early, particularly when recurrent infections, eczema, and immune dysregulation are present. The genetic confirmation of a STAT3 mutation solidifies the diagnosis, which guides management decisions, such as the use of prophylactic antibiotics, antifungal treatments, and regular immunology follow-ups. Early intervention and ongoing care are essential to improving quality of life and preventing severe complications, including recurrent infections and progressive bronchiectasis.
Discussion
This patient presented classical features of AD-HIES, including recurrent pneumonias, eczema, and elevated IgE levels. The identified STAT3 mutation was not inherited from the parents, suggesting a de novo mutation. Despite normal STAT3 expression, the pathogenic variant supports a diagnosis of AD-HIES. The presence of bronchiectasis at a young age emphasizes the importance of early pulmonary interventions to prevent long-term complications.[6] Compared to previous reports, this case demonstrates an unusual persistence of respiratory symptoms despite standard prophylaxis, suggesting possible differences in disease progression among STAT3 mutations. The successful use of bronchoscopy lavage instead of surgery highlights a less invasive but effective management approach for pulmonary abscesses.
Recent literature suggests that AD-HIES patients with STAT3 mutations have a wide spectrum of clinical severity, making early genetic screening critical for timely interventions.[7] Additionally, the observed immune dysregulation, including impaired lymphocyte proliferation and elevated isohemagglutinin titers, supports the role of close immunological monitoring.[8] Infection control remains a major challenge in AD-HIES, as recurrent bacterial and fungal infections are common despite antimicrobial prophylaxis. This case emphasizes the need for individualized prophylactic regimens based on infection patterns. Furthermore, emerging therapies targeting STAT3-related immune dysregulation, including JAK inhibitors, warrant further investigation.
Conclusion
STAT3-related hyper-IgE syndrome requires comprehensive immunological and genetic assessment. In managing pulmonary complications, bronchoscopy lavage should be considered to avoid surgical interventions in pediatric patients. Early recognition and treatment of secondary infections and immune dysregulation are crucial for optimizing outcomes.
Further research is needed to correlate specific STAT3 mutations with clinical outcomes and optimize treatment strategies. Multicenter studies on genotype-phenotype relationships in AD-HIES could provide valuable insights into personalized management approaches. Investigating novel treatment options, including targeted immunomodulatory therapies, may improve the long-term prognosis for affected patients.
References
- Minegishi Y, Saito M, Tsuchiya S, et al. Dominant-negative mutations in the DNA-binding domain of STAT3 cause hyper-IgE syndrome. Nature. 2007;448(7157):1058-1062. doi:10.1038/nature06096 PubMed | Crossref | Google Scholar
- Grimbacher B, Holland SM, Gallin JI, et al. Hyper-IgE syndrome with recurrent infections–an autosomal dominant multisystem disorder. N Engl J Med. 1999;340(9):692-702. doi:10.1056/NEJM199903043400904 PubMed| Crossref | Google Scholar
- Yong PF, Freeman AF, Engelhardt KR, Holland S, Puck JM, Grimbacher B. An update on the hyper-IgE syndromes. Arthritis Res Ther. 2012;14(6):228. doi:10.1186/ar4069 PubMed | Crossref | Google Scholar
- Holland SM, DeLeo FR, Elloumi HZ, et al. STAT3 mutations in the hyper-IgE syndrome. N Engl J Med. 2007;357(16):1608-1619. doi:10.1056/NEJMoa073687 PubMed | Crossref | Google Scholar
- Pelham SJ, Lenthall HC, Deenick EK, Tangye SG. Elucidating the effects of disease-causing mutations on STAT3 function in autosomal-dominant hyper-IgE syndrome. J Allergy Clin Immunol. 2016;138(4):1210-1213.e5. doi:10.1016/j.jaci.2016.04.020 PubMed | Crossref | Google Scholar
- Grimbacher B, Holland SM, Gallin JI, et al. Hyper-IgE syndrome with recurrent infections–an autosomal dominant multisystem disorder. N Engl J Med. 1999;340(9):692-702. doi:10.1056/NEJM199903043400904 PubMed | Crossref | Google Scholar
- Schimke LF, Sawalle-Belohradsky J, Roesler J, et al. Diagnostic approach to the hyper-IgE syndromes: immunologic and clinical key findings to differentiate hyper-IgE syndromes from atopic dermatitis. J Allergy Clin Immunol. 2010;126(3):611-7.e1. doi:10.1016/j.jaci.2010.06.029 PubMed | Crossref | Google Scholar
- Béziat V, Tavernier SJ, Chen YH, et al. Dominant-negative mutations in human IL6ST underlie hyper-IgE syndrome. J Exp Med. 2020;217(6):e20191804. doi:10.1084/jem.20191804 PubMed | Crossref | Google Scholar
Acknowledgments
The authors would like to express their gratitude to the patient and parents who kindly consented to this case presented in this paper.
Funding
No funding sources.
Author Information
Corresponding Author:
Chin Soey
Department of Pediatric Hematology and Immunology
National Pediatric Hospital, Federation of Russia Blvd, Phnom Penh, Cambodia
Email: [email protected]
Co-Authors:
Chean Sophâl
Department of Pediatric Hematology and Immunology
National Pediatric Hospital, Phnom Penh, Cambodia
Adli Bin Ali
Department of Pediatrics
UKM Specialist Children’s Hospital, The National University of Malaysia, Kuala Lumpur, Malaysia
Authors Contributions
The manuscript was written by Chin Soey and revised by Adli Bin Ali and Chean Sophâl. All the authors have read and approved the final manuscript.
Informed Consent
Informed consent was obtained from the child’s parents for publication of the case.
Conflict of Interest Statement
The authors declare no conflict of interest.
Guarantor
None
DOI
Cite this Article
Chin S, Chean S, Adli BA. Novel STAT3 Mutation in a Patient with Hyper-IgE Syndrome Presenting with Recurrent Pulmonary Infections (Job Syndrome). medtigo J Med. 2025;3(2):e30623211. doi:10.63096/medtigo30623211 Crossref













