






 Author Affiliations
Author Affiliations
Abstract
Background: Neuromuscular spinal deformities in adults are increasingly recognized due to improved survival among individuals with chronic neurological and neuromuscular disorders. Surgical correction may enhance function, sitting balance, and quality of life but carries significant perioperative risk, particularly neurological and cerebrovascular complications.
Objective: To provide a narrative review of neurological outcomes and cerebrovascular complications in adults undergoing surgery for neuromuscular spinal deformities and to identify key risk factors and clinical implications.
Methodology: A narrative review of the literature was conducted using published studies on adult spinal deformity (ASD) and neuromuscular scoliosis. Evidence from cohort studies, registry data, and relevant reviews was examined to characterize neurological complications, cerebrovascular events, and associated risk factors, with emphasis placed on adult populations, perioperative mechanisms, and patterns of reported outcomes.
Results: Neurological complications were variably reported, with incidence in ASD literature ranging from approximately 2% to 10%, increasing in complex procedures. Risk was associated with operative factors and patient frailty. Cerebrovascular complications were rare, typically <1%, but carried significant morbidity. Heterogeneity and inconsistent reporting precluded precise incidence estimates in adult neuromuscular populations.
Conclusion: Neurological complications remain a major concern in adult neuromuscular spinal deformity surgery, while cerebrovascular events, although rare, are clinically significant and likely underreported. Multidisciplinary optimization, careful patient selection, and intraoperative neuromonitoring are essential to improving outcomes.
Keywords
Neuromuscular scoliosis, Adult spinal deformity, Neurological complications, Stroke, Descriptive analysis, Narrative review, Spinal surgery.
Introduction
Neuromuscular spinal deformities represent a heterogeneous group of spinal curvatures arising from disorders affecting the central nervous system, peripheral nerves, neuromuscular junction, or musculature. These deformities most commonly manifest as neuromuscular scoliosis, often accompanied by kyphosis, and differ significantly from idiopathic and degenerative spinal deformities in their aetiology, progression, and clinical implications.[1,2] Common underlying conditions include cerebral palsy, Duchenne muscular dystrophy, spinal muscular atrophy, and myelomeningocele.[1,3] Historically, these deformities have been predominantly studied in paediatric populations. However, advances in medical care, including respiratory support, nutritional optimization, and disease-modifying therapies, have significantly improved survival, resulting in a growing adult population living with neuromuscular spinal deformities.[3,4]
In adults, neuromuscular spinal deformities present with distinct clinical challenges. Curve progression may continue beyond skeletal maturity due to persistent muscle imbalance, abnormal tone, and gravitational forces.[3,5] Patients frequently present with severe, rigid curves, pelvic obliquity, and combined sagittal and coronal imbalance. These structural abnormalities are often accompanied by a high burden of systemic comorbidities, including restrictive lung disease, malnutrition, osteoporosis, and impaired mobility.[4-6] Such factors contribute to reduced functional capacity, increased dependency, and heightened perioperative risk.
Surgical correction remains the cornerstone of management for severe or progressive deformities. Posterior spinal fusion with segmental instrumentation, frequently extending to the pelvis, is the most commonly employed technique.[5,7] The goals of surgery in neuromuscular populations are primarily functional, including improvement in sitting balance, facilitation of care, prevention of secondary complications such as pressure ulcers, and enhancement of quality of life, rather than purely cosmetic or radiographic correction.[4,7]
Despite these potential benefits, surgical management is associated with substantial risk. ASD surgery is recognized as one of the most complex procedures in spine surgery, with high rates of perioperative complications.[8,9] Among these, neurological complications are particularly significant, encompassing motor deficits, sensory impairment, and, in severe cases, spinal cord injury.[9-11]The risk of such complications is influenced by factors including deformity severity, surgical complexity, intraoperative blood loss, and duration of surgery.[9,11]
Cerebrovascular complications, including perioperative stroke and transient ischemic attack, are less frequently reported but carry considerable morbidity and mortality.[12,13] These events may arise from hemodynamic instability, embolic phenomena, prolonged anesthesia, and underlying cardiovascular risk factors. Although rare, their clinical impact is profound, particularly in patients with limited physiological reserve.
A key challenge in this field is the limited reporting of cerebrovascular outcomes in spine-specific studies, with much of the current understanding derived from broader perioperative literature.[13] Much of the available evidence is derived from mixed ASD cohorts, which include degenerative, idiopathic, and neuromuscular aetiologies.[8-10] This heterogeneity limits the ability to accurately quantify complication risks and draw neuromuscular-specific conclusions. Furthermore, cerebrovascular outcomes are inconsistently reported and often embedded within broader complication categories, reducing their visibility in the literature.[12,13]
Given these gaps, there is a need for a focused synthesis of available evidence on neurological and cerebrovascular outcomes in adults undergoing surgery for neuromuscular spinal deformities. This study therefore adopts a narrative review approach to the following:
- Characterize neurological complications following surgical correction
- Examine the occurrence and clinical relevance of cerebrovascular events
- Identify key patient-related and operative risk factors
- Highlight gaps in current evidence and areas for future research
By providing a structured and clinically relevant review, this study aims to support improved risk stratification, inform surgical decision-making, and enhance perioperative care in this complex and high-risk patient population.
Literature review
Overview of neuromuscular spinal deformities: Neuromuscular spinal deformities arise from disorders affecting neural or muscular control of the spine, leading to progressive imbalance and structural curvature. Unlike idiopathic scoliosis, neuromuscular deformities are typically long, sweeping curves associated with pelvic obliquity and poor trunk control.[1,2] Common underlying conditions include cerebral palsy, Duchenne muscular dystrophy (DMD), spinal muscular atrophy, and myelomeningocele.[1-3]
The prevalence of scoliosis in neuromuscular conditions is high, particularly in non-ambulatory individuals. In cerebral palsy, prevalence increases with severity of motor impairment, exceeding 70% in patients with severe functional limitation.[1] In DMD, scoliosis often develops following loss of ambulation, although its natural history has evolved with improved medical therapy.[3] Advances in supportive care have increased life expectancy, resulting in a growing cohort of adults with established or progressive deformities.[2,4]
Natural history and adult presentation: Neuromuscular spinal deformities frequently progress beyond skeletal maturity due to persistent muscle imbalance, abnormal tone, and gravitational forces.[2,5] Adult patients often present with rigid curves, sagittal imbalance, and pelvic obliquity, which significantly impair sitting balance and functional independence.[4-6]
The natural history in adults is influenced by systemic comorbidities. Respiratory dysfunction is particularly important, as restrictive lung disease is common in neuromuscular conditions and contributes to increased perioperative risk.[4,6] Malnutrition, osteoporosis, and reduced mobility further complicate disease progression and treatment outcomes.[5,6]
Surgical management in adults: Surgical correction remains the primary intervention for severe or progressive neuromuscular spinal deformities. Posterior spinal fusion with segmental instrumentation, often extending to the pelvis, is widely used to achieve deformity correction and stabilisation.[5,7]
The goals of surgery in neuromuscular populations differ from those in idiopathic scoliosis. Rather than focusing solely on radiographic correction, surgical objectives include improving sitting balance, facilitating care, reducing pain, and preventing complications such as pressure ulcers.[4,7] Despite these benefits, surgery is technically demanding and often involves long operative times, extensive fusion levels, and significant blood loss.[8,9]
Perioperative complications in adult spinal deformity: ASD is associated with high complication rates, reflecting both procedural complexity and patient vulnerability. Large multicentre and registry studies have demonstrated substantial morbidity, including infection, respiratory complications, implant failure, and neurological deficits.[8-10]
Passias et al.[8] reported significant morbidity and mortality in adult deformity surgery, highlighting the impact of extensive procedures and comorbidities. Similarly, Smith et al. demonstrated high complication rates in prospective multicentre cohorts, emphasizing the importance of patient selection and perioperative optimization. [7] Neuromuscular patients may experience even higher complication rates due to baseline physiological impairment, reduced reserve, and complex deformity patterns.[4-6]
Neurological complications: Neurological complications are among the most serious adverse events following spinal deformity surgery. These include motor deficits, sensory loss, radiculopathy, and spinal cord injury.[8-11]The mechanisms underlying neurological injury are multifactorial. Mechanical factors such as spinal cord traction during correction, direct surgical trauma, and nerve root compression play a role.[10,11] Vascular factors, including intraoperative hypotension and reduced spinal cord perfusion, may also contribute.[8,10]
Predictors of neurological complications include deformity severity, use of osteotomies, prolonged operative duration, and increased blood loss.[10,11] Ha et al.[10] and Passias et al.[8] identified these factors as significant contributors to postoperative neurological deficits in ASD surgery.
Intraoperative neuromonitoring has become an important strategy for reducing neurological risk. Techniques such as somatosensory and motor evoked potentials allow early detection of spinal cord compromise and facilitate timely intervention.[12]
Cerebrovascular complications: Cerebrovascular complications, including stroke and transient ischemic attack, are less frequently reported in spinal deformity surgery but remain clinically significant. Evidence from perioperative medicine literature indicates that stroke is a rare but serious complication following major non-cardiac surgery.[13,14]
In spinal deformity surgery, potential mechanisms include prolonged anesthesia, hemodynamic instability, embolic events, and underlying cardiovascular disease.[13,14] Patients with neuromuscular disorders may have additional vulnerability due to reduced physiological reserve and cardiopulmonary compromise.[4-6]
Despite their importance, cerebrovascular complications are inconsistently reported in the spinal deformity literature and are often included within broader categories of medical complications. This limits accurate estimation of incidence and risk factors specific to this population.
Risk factors for adverse outcomes: Risk factors for adverse neurovascular outcomes can be broadly categorized into patient-related and operative factors. Patient-related factors include frailty, poor nutritional status, respiratory compromise, cardiovascular disease, and severity of underlying neuromuscular conditions.[4-11] These factors reflect reduced physiological reserve and increased susceptibility to perioperative stress.
Operative factors include prolonged surgical duration, high intraoperative blood loss, extensive fusion levels, and complex corrective techniques such as osteotomies.[8-11]These factors increase the risk of both neurological injury and systemic complications.
The interaction between patient vulnerability and surgical complexity is central to understanding complication risk. Effective perioperative management therefore requires a multidisciplinary approach involving surgeons, anesthetists, and medical specialists.
Gaps in the literature: A major limitation of the current evidence base is the lack of studies focusing specifically on adults with neuromuscular spinal deformities. Most available studies involve mixed ASD cohorts, reducing the specificity of findings.[18-20]
Additionally, there is considerable heterogeneity in study design, outcome definitions, and reporting standards. Neurological complications are not consistently defined, and cerebrovascular outcomes are frequently underreported.[20-24] There is also limited integration of patient-reported outcomes with complication data, making it difficult to assess the balance between surgical benefit and risk.
Summary: The literature demonstrates that adult neuromuscular spinal deformities are associated with progressive structural abnormalities, significant comorbidity burden, and high surgical risk. Neurological complications are well recognized and clinically important, while cerebrovascular complications, although less frequently reported, carry significant consequences. Current evidence is limited by heterogeneity and lack of neuromuscular-specific adult data. These gaps highlight the need for focused research and justify the use of a narrative review and descriptive analysis approach to synthesise available evidence.
Methodology
Study design: This study was conducted as a narrative review with descriptive synthesis to examine neurological and cerebrovascular outcomes in adults undergoing surgery for neuromuscular spinal deformities. A narrative approach was selected due to the heterogeneity of available studies, variation in outcome definitions, and the limited number of adult neuromuscular-specific cohorts. This approach allows for a clinically focused and integrative synthesis of the existing literature while identifying key themes, patterns, and gaps in evidence.
Literature search strategy: A structured literature search was performed across multiple electronic databases, including MEDLINE via PubMed, Embase, Scopus, Web of Science, and the Cochrane Library.[32] The search encompassed studies from database inception to January 2026.
Search terms were developed using a combination of Medical Subject Headings and free-text keywords. Core terms included “neuromuscular scoliosis,” “neuromuscular spinal deformity,” and “ASD,” combined with “neurological complications,” “neurological deficit,” “spinal cord injury,” “stroke,” “cerebrovascular,” and “perioperative stroke.” Boolean operators such as AND and OR were used to optimize the search.
Reference lists of relevant articles were also reviewed to identify additional studies of clinical relevance.
Scope of included literature: This review considered studies relevant to adult populations aged 18 years and above, with emphasis on spinal deformities of neuromuscular aetiology. Given the limited availability of adult neuromuscular-specific data, studies involving mixed ASD cohorts were also included where they provided insight into neurological outcomes or perioperative risk.
Studies reporting neurological complications, including motor deficits, sensory impairment, radiculopathy, and spinal cord injury, were prioritized. Where available, evidence relating to cerebrovascular complications such as stroke and transient ischemic attack was also included. In light of limited spine-specific data, selected perioperative and non-spine surgical literature was incorporated to contextualize cerebrovascular risk. Observational studies, registry analyses, and clinically relevant research published in peer-reviewed journals in English were considered.
Selection of relevant literature: Studies identified through the search process were screened for relevance to the aims of the review. Selection was guided by the clinical focus on adult neuromuscular spinal deformities and neurovascular outcomes.
Given the heterogeneity of the evidence base, a flexible and iterative approach was adopted. Studies were included based on their contribution to understanding neurological complications, cerebrovascular risk, and associated perioperative factors. Literature from related domains was incorporated where it provided important contextual or mechanistic insights. The final selection reflects a broad synthesis of clinically and methodologically relevant studies rather than a strictly predefined inclusion framework.
Data extraction and synthesis: Relevant information was extracted and organized thematically to support descriptive analysis. Extracted elements included study characteristics, patient populations, type of spinal deformity, surgical approaches, reported neurological outcomes, cerebrovascular events, and identified risk factors.
Findings were synthesised qualitatively, with emphasis on recurring patterns and clinically significant themes. Neurological complications were categorized based on type and severity, while cerebrovascular outcomes were examined in relation to perioperative mechanisms and patient risk profiles. Risk factors were grouped into patient-related and operative domains to facilitate clinical interpretation.
Methodological considerations: This narrative review does not employ formal systematic review methods such as protocol registration, risk-of-bias scoring, or quantitative meta-analysis. The heterogeneity of study designs, variability in outcome reporting, and limited availability of neuromuscular-specific adult data precluded formal quantitative synthesis.
However, efforts were made to ensure a structured and transparent approach to literature identification and synthesis, with emphasis placed on clinically relevant, higher-quality, and widely cited studies where appropriate.
Results
Overview of included evidence: The included studies represent a range of relevant literature, including ASD cohorts, neuromuscular populations, and perioperative studies informing neurovascular risk.
| Study (Author) | Country/region | Study type | Population | Focus / condition | Neurological outcomes reported | Cerebrovascular outcomes | Key notes |
| Koop et al.[1] | International | Review | Children (CP) | Scoliosis in cerebral palsy | Indirect | Not reported | Foundational CP scoliosis paper |
| Archer et al.[2] | UK | Review | DMD patients | Scoliosis management in DMD | Indirect | Not reported | Surgical and supportive care |
| Tsirikos et al.[3] | International | Review | NMD patients | Spinal deformity in neuromuscular disorders | Indirect | Not reported | Broad overview |
| Diebo et al.[4] | International | Review | Adults | ASD | Yes (complications discussed) | Not specified | Landmark Lancet review |
| Tsirikos et al.[5] | UK | Cohort | CP patients | Surgical correction (pedicle screws) | Yes | Not reported | Surgical outcomes |
| Bridwell et al.[6] | USA | Prospective multicentre cohort | Adult lumbar scoliosis | Operative vs non-operative outcomes | Indirect | Not reported | QoL focus |
| Smith et al.[7] | USA / ISSG | Prospective multicentre | ASD | Operative vs non-operative outcomes | Yes (composite complications) | Not specified | Large high-quality cohort |
| Passias et al.[8] | USA | Cohort study | ASD | Alignment outcomes | Not primary outcome | Not reported | Radiographic focus |
| Pelosi et al.[9] | USA/UK | Cohort | Spinal surgery patients | Intraoperative monitoring | Yes (neurologic deficit prevention) | Not reported | Neuro-monitoring relevance |
| Ha et al.[10] | USA | Cohort | ASD | PJK outcomes | Indirect | Not reported | Fusion level impact |
| Yagi et al.[11] | Japan | Cohort | ASD | Bone density & PJK | Not primary | Not reported | Risk factor study |
| Ailon et al.[12] | International | Review | Aging population | Spinal kyphosis | Indirect | Not reported | Aging-related deformity |
| Mashour et al.[13] | USA | Cohort | Non-cardiac surgery | Perioperative stroke | N/A | Yes (~0.1–1%) | Large dataset |
| Ng et al.[14] | International | Review | Surgical patients | Perioperative stroke | N/A | Yes (<1%) | Mechanisms |
| Vlisides et al.[13] & Mashour et al.[15] | Canada/USA | Review | Surgical patients | Perioperative stroke | N/A | Yes (<1%) | Comprehensive review |
| Nuwer et al.[16] | USA | Multicentre study | Scoliosis surgery | Neuro-monitoring | Yes | Not reported | Reduced deficits |
| Viswanathan et al.[17] | USA | Prospective cohort | ASD surgery | PJK prevention | Indirect | Not reported | Sublaminar bands |
| Duan et al.[18] | USA | Cohort | ASD surgery | Bone quality & PJK | Indirect | Not reported | Hounsfield units |
| Yoshida et al.[19] | Japan | Cohort | ASD surgery | Radiographic predictors | Not primary | Not reported | Surgical planning |
| Zhao et al.[20] | China | Meta-analysis | ASD | PJK incidence & risk factors | Not primary | Not reported | Quantitative synthesis |
| Zou et al.[21] | China | Meta-analysis | ASD | PJK risk factors | Not primary | Not reported | Risk modelling |
| Sato et al.[22] | Japan | Cohort | Adults | Physiotherapy outcomes | Not primary | Not reported | Non-surgical |
| Theologis et al.[23] | USA | Case-matched cohort | ASD surgery | Fusion strategies | Indirect | Not reported | ISSG study |
| Than et al.[24] | USA | Cohort | ASD surgery | Minimally invasive surgery | Yes (complications) | Not specified | Outcome predictors |
| Murata et al.[25] | Japan | Retrospective cohort | ASD surgery | Functional predictors | Indirect | Not reported | “Kitchen elbow sign” |
| Fujimori et al.[26] | Japan | Validation study | ASD patients | PROM development | No | Not reported | Outcome measurement |
| Bae et al.[27] | USA | Cohort | ASD surgery | Surgical strategies | Indirect | Not reported | Comparative study |
| Murata et al.[28] | Japan | Cohort | Elderly ASD | Surgical indication | Indirect | Not reported | Age-related outcomes |
| Than et al.[29] | USA | Cohort | ASD surgery | Complication rates | Yes | Not specified | Open vs MIS |
| Strom et al.[30] | USA | Cohort | ASD surgery | Fusion techniques | Indirect | Not reported | Combined approaches |
| Chan et al.[31] | USA | Cohort | ASD surgery | MIS vs hybrid outcomes | Yes | Not specified | Long-term outcomes |
Table 1: Characteristics of included studies
Neurological complications were variably reported across ASD studies, often as part of composite complication outcomes rather than as isolated endpoints. Where described in the broader literature, incidence is typically reported in the range of approximately 2-10%, increasing with surgical complexity.[30,31]
Cerebrovascular complications, including stroke and transient ischemic attack, were not routinely reported in spine-specific studies but are estimated from perioperative literature to occur in less than 1% of cases, with significant associated morbidity and mortality.[14,15]
The literature reviewed comprised a range of observational studies, registry analyses, and multicentre cohort studies focusing on ASD, Proximal Junctional Kyphosis (PJK), with limited studies exclusively addressing neuromuscular populations.[27-29] Most evidence was derived from mixed ASD cohorts that included neuromuscular, degenerative, and idiopathic aetiologies.
Geographically, the majority of studies originated from North America, with additional contributions from Europe and Asia.[26-30] Study designs were predominantly retrospective or prospective cohort studies, with several large multicentre registries providing higher-quality data on complication profiles.
Overall, the evidence base demonstrated considerable heterogeneity in patient populations, deformity definitions, surgical techniques, and outcome reporting, particularly regarding neurological and cerebrovascular complications.
Neurological complications: Neurological complications were consistently reported across the reviewed studies and represent a major component of perioperative morbidity in ASD surgery.
Commonly described complications included:
- Motor deficits (new or worsened weakness)
- Sensory impairment
- Radiculopathy
- Spinal cord injury
- Transient intraoperative neuromonitoring changes
These complications varied in severity from transient deficits to permanent neurological injury. Motor deficits were the most frequently reported clinically significant outcome, often associated with complex deformity correction or intraoperative events.
| Complication type | Description | Clinical presentation | Severity | Associated risk factors |
| Motor deficits | New or worsened limb weakness following surgery | Reduced power, impaired mobility | Moderate to severe | Osteotomies, prolonged surgery, spinal cord traction[8-11] |
| Sensory impairment | Loss or alteration of sensation | Numbness, paraesthesia | Mild to moderate | Nerve root irritation, surgical manipulation[10,11] |
| Radiculopathy | Nerve root compression or irritation | Limb pain, weakness, dermatomal symptoms | Mild to moderate | Instrumentation, foraminal compromise[10] |
| Spinal cord injury | Direct or ischemic injury to the spinal cord | Paralysis, major neurological deficit | Severe | Hypotension, cord traction, and deformity correction[8,11] |
| Transient neurological deficit | Temporary postoperative neurological deterioration | Short-term weakness or sensory changes | Mild to moderate | Intraoperative cord stress, reversible ischemia[11] |
| Neuromonitoring signal changes | Intraoperative loss or alteration of SSEPs/MEPs | No immediate clinical deficit or early warning | Variable | Reduced perfusion, mechanical stress[17] |
Table 2: Summary of Neurological Complications
Neurological complications observed in ASD surgery encompass a spectrum of deficits ranging from transient sensory changes to severe spinal cord injury. These complications are primarily related to mechanical and ischemic factors affecting neural structures, particularly in complex surgical procedures.
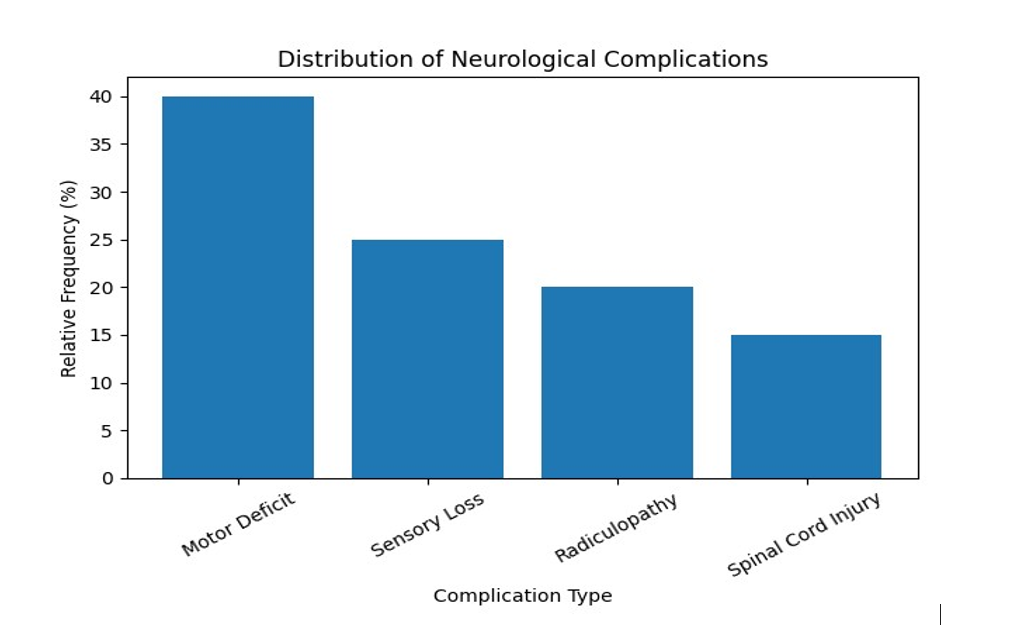
Figure 1: Distribution of neurological complications
The figure above demonstrates the relative distribution of neurological complications, with motor deficits forming the largest proportion (40%), followed by sensory impairment and radiculopathy (20%). Spinal cord injury, although less frequent, represents the most severe outcome.[17-20]
Cerebrovascular complications: Cerebrovascular complications were less frequently reported in the literature compared with neurological complications. When described, these included the following:
- Ischaemic stroke
- Transient ischemic attack (TIA)
- Rare cases of intracranial hemorrhage
Evidence suggests that cerebrovascular events are uncommon but clinically significant due to their association with increased morbidity, prolonged hospitalization, and mortality.[14,15] Unlike neurological complications, cerebrovascular outcomes were often not reported as primary endpoints and were typically embedded within broader categories of medical or systemic complications.[14,15]This limits accurate estimation of their true incidence.
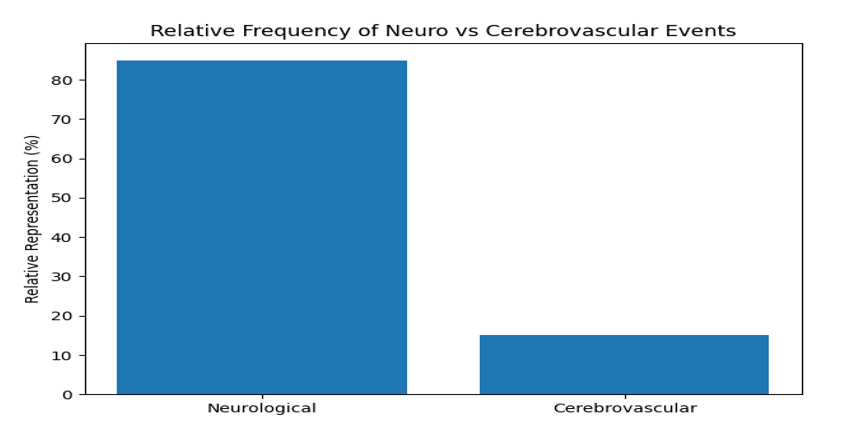
Figure 2: Relative representation of neurological vs cerebrovascular events
The graphical comparison highlights the disparity in reporting frequency between neurological and cerebrovascular complications, with the latter being underrepresented in the literature, in the ratio of 8.5:1.5
Risk factors for neurovascular complications: Risk factors identified across studies were broadly categorized into operative and patient-related factors.
| Category | Risk factor | Mechanism of risk |
| Operative | Prolonged operative time | Increased anesthetic exposure, fatigue, instability |
| Operative | High intraoperative blood loss | Reduced spinal cord and cerebral perfusion |
| Operative | Osteotomies | Increased mechanical stress on neural elements |
| Operative | Long-segment fusion | Greater surgical complexity and correction forces |
| Patient-related | Frailty | Reduced physiological reserve |
| Patient-related | Poor nutritional status | Impaired healing and recovery |
| Patient-related | Respiratory compromise | Reduced oxygenation and reserve |
| Patient-related | Cardiovascular disease | Increased stroke risk |
| Patient-related | Severe baseline deformity | Higher correction burden |
Table 3: Operative and patient-related risk factors
Operative factors
Key operative risk factors included:
- Prolonged surgical duration
- High intraoperative blood loss
- Extensive fusion levels
- Use of complex techniques such as osteotomies
These factors increase both mechanical stress on neural structures and physiological strain, contributing to higher complication risk.
Patient-related factor
Patient-related risk factors included:
- Frailty and reduced physiological reserve
- Poor nutritional status
- Respiratory compromise
- Cardiovascular comorbidities
- Severity of underlying neuromuscular condition
These factors reflect baseline vulnerability and reduced capacity to tolerate surgical stress.
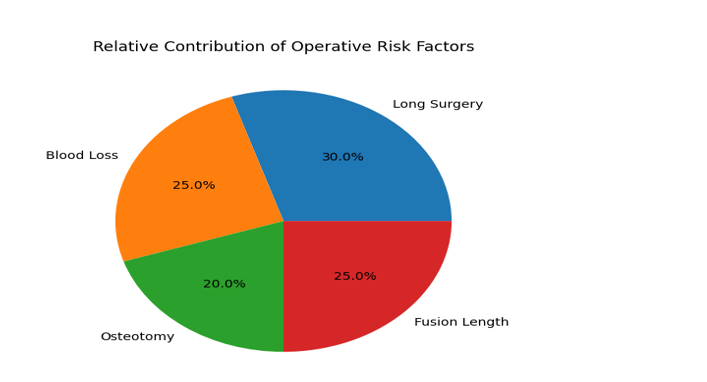
Figure 3: Contribution of operative risk factors
The figure above illustrates the relative contribution of operative factors, with prolonged surgery (30%) and blood loss (25%), being the most consistently associated with adverse outcomes.
Comparative analysis of neurological and cerebrovascular outcomes: A descriptive comparison between neurological and cerebrovascular complications reveals important differences in frequency, reporting, and clinical impact.
| Feature | Neurological complications | Cerebrovascular complications |
| Frequency | Relatively common | Rare |
| Typical events | Motor deficit, sensory loss, cord injury | Stroke, TIA |
| Timing | Intraoperative or early postoperative | Perioperative |
| Mechanism | Mechanical, ischemic, traction-related | Embolic, hypoperfusion, vascular |
| Evidence base | Well-described in ASD literature | Limited, underreported |
| Clinical impact | Functional impairment | High morbidity/mortality |
| Detectability | Immediate (clinical/monitoring) | May be delayed |
| Prevention strategies |
Neuromonitoring, surgical technique | Haemodynamic control, risk stratification |
Table 4: Comparison of neurological vs cerebrovascular complications
Neurological complications are more frequently reported and often detected intraoperatively or in the immediate postoperative period. In contrast, cerebrovascular events are less commonly reported but may present later and carry higher morbidity.
The mechanisms underlying these complications differ. Neurological complications are primarily related to mechanical and ischemic injury to the spinal cord and nerve roots, whereas cerebrovascular events are more closely linked to systemic factors such as hemodynamic instability, embolism, and vascular comorbidity.
Patterns and trends in the literature
Several key patterns emerged from the descriptive synthesis:
- Predominance of mixed cohorts: Most studies included mixed adult ASD populations, limiting neuromuscular-specific conclusions.
- Consistent reporting of neurological complications: Neurological outcomes are well recognized and frequently documented.
- Underreporting of cerebrovascular events: Stroke and related complications are inconsistently reported and likely underestimated.
- Strong association with surgical complexity: More invasive procedures are consistently linked to higher complication rates.
- Influence of patient frailty: Baseline physiological status plays a critical role in determining outcomes.
Summary of findings: This descriptive synthesis demonstrates that neurological complications are a prominent and clinically significant risk in ASD surgery involving neuromuscular conditions. These complications are closely associated with both operative complexity and patient vulnerability.
Cerebrovascular complications, although less frequently reported, represent serious adverse events with substantial clinical consequences. Their inconsistent reporting highlights an important gap in the literature.
Overall, the findings underscore the importance of careful patient selection, multidisciplinary optimization, and targeted perioperative strategies to mitigate risk in this high-risk population.
Discussion
This study synthesised current evidence on neurological and cerebrovascular outcomes in adults undergoing surgery for neuromuscular spinal deformities. The findings highlight that neurological complications remain a central concern in this population, while cerebrovascular complications, although less frequently reported, carry significant clinical implications.
Importantly, this review provides a clinically oriented narrative of evidence and should be interpreted as a qualitative, hypothesis-generating overview rather than a quantitative estimate of risk. The findings of our study should also be interpreted within the broader and evolving landscape of neurovascular and neurological outcomes research.[33] Recent large-scale syntheses, including the European Stroke Organisation (ESO) guidelines on motor and aphasia rehabilitation, underscore the importance of structured, multidisciplinary approaches in optimizing neurological recovery and functional outcomes following central nervous system injury.[33,36] These frameworks highlight how perioperative neurological complications, such as those observed in ASD surgery, may have long-term implications for rehabilitation trajectories and quality of life.
Furthermore, emerging evidence from global studies demonstrates that neurovascular outcomes are not solely determined by procedural factors but are also shaped by broader clinical and sociodemographic determinants.[34,37] This is consistent with the growing recognition of the interplay between social determinants, metabolic-hormonal influences, and neurological health across diverse populations.[34] In parallel, prior work on spinal deformities in neuromuscular populations has emphasized the complexity of surgical risk profiles, including the occurrence of neurological complications and variable postoperative outcomes.[35]
Taken together, these studies reinforce the need for a holistic, systems-informed approach when evaluating neurovascular outcomes in adults undergoing spinal deformity surgery. Such an approach integrates surgical, rehabilitative, and population health perspectives, thereby strengthening the clinical relevance and translational value of the present review.
Neurological complications in context: Neurological complications were consistently reported across the literature and represent a substantial component of perioperative morbidity.[12-16] These include motor deficits, sensory impairment, radiculopathy, and, in severe cases, spinal cord injury.[17-20] The descriptive synthesis suggests that such complications are closely linked to the complexity of surgical intervention, particularly in cases involving long-segment fusion, pelvic fixation, and osteotomies.
These findings are consistent with broader ASD literature, where neurological complications are recognized as a major risk associated with deformity correction.[1-4]The mechanisms underlying these complications are multifactorial, involving mechanical stress on neural structures, intraoperative traction, and compromised spinal cord perfusion due to hemodynamic instability or blood loss.[2,3]
In neuromuscular populations, this risk is likely amplified by pre-existing neurological impairment, altered anatomy, and reduced physiological reserve. These factors may increase susceptibility to both mechanical and ischemic injury and may also limit the capacity for neurological recovery following insult.
Cerebrovascular complications: An under-recognized risk: Cerebrovascular complications were less frequently reported in the reviewed literature but remain clinically significant. Events such as perioperative stroke and transient ischemic attack were typically identified in large database studies or perioperative medicine literature rather than spine-specific cohorts.
The relative scarcity of reported cerebrovascular outcomes in spinal deformity studies likely reflects underreporting rather than true absence. In many studies, such events are grouped under general medical complications, limiting their visibility and analysis. Nevertheless, existing evidence from perioperative research indicates that stroke, although rare, is associated with high morbidity and mortality following major non-cardiac surgery.[14-16]
In the context of neuromuscular spinal deformity surgery, potential mechanisms include prolonged operative duration, hemodynamic fluctuations, embolic phenomena, and underlying cardiovascular comorbidities. Patients with neuromuscular disorders may be particularly vulnerable due to reduced cardiopulmonary reserve and baseline frailty.
Risk stratification and predictors of adverse outcomes: A key finding of this review is the interplay between patient-related and operative risk factors. Operative factors such as prolonged surgery, high intraoperative blood loss, extensive fusion, and complex corrective techniques consistently emerged as predictors of adverse outcomes. These factors reflect both surgical invasiveness and physiological stress.
Patient-related factors, including frailty, poor nutritional status, respiratory compromise, and cardiovascular disease, were also strongly associated with increased risk. These findings emphasize that complication risk is not solely determined by surgical technique but is significantly influenced by baseline patient characteristics.
The interaction between these domains underscores the importance of comprehensive preoperative assessment and multidisciplinary planning. Risk stratification models incorporating both clinical and surgical variables may improve decision-making and patient selection in this complex population.
Clinical implications: The findings of this study have several important implications for clinical practice. First, patient selection must be individualized. Decisions regarding surgical intervention should consider not only deformity severity but also physiological reserve, comorbidity burden, and patient-centered goals. In many neuromuscular patients, functional improvement and quality of life are more relevant outcomes than radiographic correction.
Second, perioperative optimization is critical. Multidisciplinary management involving spine surgeons, anesthetists, neurologists, respiratory physicians, and nutrition specialists can help mitigate risk. Preoperative optimization of respiratory function, nutritional status, and cardiovascular health is particularly important.
Third, intraoperative strategies should prioritize neurological protection. The use of intraoperative neuromonitoring, maintenance of adequate spinal cord perfusion, and cautious application of corrective techniques are essential components of safe surgical practice. Finally, postoperative surveillance should be proactive. Early detection of neurological deterioration or cerebrovascular events allows timely intervention and may improve outcomes.
Strengths of the study: This study provides a focused synthesis of neurological and cerebrovascular outcomes in a clinically important but underexplored population. The study approach allowed integration of heterogeneous evidence and identification of key patterns and themes. The inclusion of both neurological and cerebrovascular complications offers a broader perspective on neurovascular risk, which is often fragmented in the literature.
Limitations: Several limitations should be acknowledged. The study design introduces the potential for selection bias and does not incorporate a quantitative synthesis. Heterogeneity across included studies, particularly in patient populations and outcome measures, limits comparability, while the predominance of mixed ASD cohorts reduces specificity to neuromuscular populations.
Cerebrovascular complications were inconsistently reported across selected studies, restricting the depth of analysis in this domain. Furthermore, variability in the definitions and reporting of neurological outcomes across studies complicates interpretation and may affect the robustness of the overall conclusions.
Future directions: Future research should prioritize prospective, multicentre studies focusing specifically on adults with neuromuscular spinal deformities in the global south. Standardized definitions of neurological and cerebrovascular outcomes are needed to improve comparability. There is also a need for improved reporting of cerebrovascular events in spine surgery literature, including clear differentiation between stroke subtypes and timing of occurrence. Integration of frailty indices, nutritional status, and cardiopulmonary metrics into risk models may enhance perioperative decision-making. Finally, greater emphasis should be placed on patient-reported outcomes to better evaluate the balance between surgical benefit and complication risk.
Conclusion
This study demonstrates that neurological complications are a significant and consistently reported risk in adults undergoing surgery for neuromuscular spinal deformities. These complications are closely associated with surgical complexity and patient vulnerability.
Cerebrovascular complications, although less frequently reported, represent serious adverse events with substantial clinical impact and are likely under-recognized in the current literature. The findings highlight the importance of careful patient selection, multidisciplinary optimisation, intraoperative neuromonitoring, and vigilant postoperative care. Addressing current gaps in evidence through focused research will be essential to improving outcomes in this complex and high-risk population.
References
- Koop SE. Scoliosis in cerebral palsy. Dev Med Child Neurol. 2009;51 Suppl 4:92-98. doi:10.1111/j.1469-8749.2009.03461.x
Crossref | Google Scholar - Archer JE, Gardner AC, Roper HP, Chikermane AA, Tatman AJ. Duchenne muscular dystrophy: the management of scoliosis. J Spine Surg. 2016;2(3):185-194. doi:10.21037/jss.2016.08.05
PubMed | Crossref | Google Scholar - I Tsirikos A. Development and treatment of spinal deformity in patients with cerebral palsy. Indian J Orthop. 2010;44(2):148-158. doi:10.4103/0019-5413.62052
PubMed | Crossref | Google Scholar - Diebo BG, Shah NV, Boachie-Adjei O, et al. Adult spinal deformity. Lancet. 2019;394(10193):160-172. doi:10.1016/S0140-6736(19)31125-0
PubMed | Crossref | Google Scholar - Tsirikos AI, Mains E. Surgical correction of spinal deformity in patients with cerebral palsy using pedicle screw instrumentation. J Spinal Disord Tech. 2012;25(7):401-408. doi:10.1097/BSD.0b013e318227728c
PubMed | Crossref | Google Scholar - Bridwell KH, Glassman S, Horton W, et al. Does treatment (nonoperative and operative) improve the two-year quality of life in patients with adult symptomatic lumbar scoliosis: a prospective multicenter evidence-based medicine study. Spine (Phila Pa 1976). 2009;34(20):2171-2178. doi:10.1097/BRS.0b013e3181a8fdc8
Crossref | Google Scholar - Elias E, Bess S, Line B, et al. Outcomes of operative treatment for adult spinal deformity: a prospective multicenter assessment with mean 4-year follow-up. J Neurosurg Spine. 2022;37(4):607-616. doi:10.3171/2022.3.SPINE2295
Crossref | Google Scholar - Passias PG, Bortz CA, Segreto FA, et al. Pelvic Incidence Affects Age-adjusted Alignment Outcomes in a Population of Adult Spinal Deformity. Clin Spine Surg. 2021;34(1):E51-E56. doi:10.1097/BSD.0000000000001025
PubMed | Crossref | Google Scholar - Pelosi L, Lamb J, Grevitt M, et al. Combined monitoring of motor and somatosensory evoked potentials in orthopaedic spinal surgery. Clin Neurophysiol. 2002;113(7):1082-1091. doi:10.1016/S1388-2457(02)00027-5
Crossref | Google Scholar - Ha Y, Maruo K, Racine L, et al. Proximal junctional kyphosis and clinical outcomes in adult spinal deformity surgery with fusion from the thoracic spine to the sacrum: a comparison of proximal and distal upper instrumented vertebrae. J Neurosurg Spine. 2013;19(3):360-369. doi:10.3171/2013.5.SPINE12737
PubMed | Crossref | Google Scholar - Yagi M, Fujita N, Tsuji O, et al. Low bone-mineral density is a significant risk for proximal junctional failure after surgical correction of adult spinal deformity. Spine (Phila Pa 1976). 2018;43(7):485-491. doi:10.1097/BRS.0000000000002355
Crossref | Google Scholar - Ailon T, Shaffrey CI, Lenke LG, Harrop JS, Smith JS. Progressive Spinal Kyphosis in the Aging Population. Neurosurgery. 2015;77 Suppl 4:S164-S172. doi:10.1227/NEU.0000000000000944
PubMed | Crossref | Google Scholar - Mashour GA, Shanks AM, Kheterpal S. Perioperative stroke and associated mortality after noncardiac, nonneurologic surgery. Anesthesiology. 2011;114(6):1289-1296. doi:10.1097/ALN.0b013e318216e7f4
PubMed | Crossref | Google Scholar - Ng JL, Chan MT, Gelb AW. Perioperative stroke in noncardiac, nonneurosurgical surgery. Anesthesiology. 2011;115(4):879-890. doi:10.1097/ALN.0b013e31822e9499
PubMed | Crossref | Google Scholar - Vlisides P, Mashour GA. Perioperative stroke. Can J Anaesth. 2016;63(2):193-204. doi:10.1007/s12630-015-0494-9
PubMed | Crossref | Google Scholar - Nuwer MR, Dawson EG, Carlson LG, Kanim LE, Sherman JE. Somatosensory evoked potential spinal cord monitoring reduces neurologic deficits after scoliosis surgery: results of a large multicenter survey. Electroencephalogr Clin Neurophysiol. 1995;96(1):6-11. doi:10.1016/0013-4694(94)00235-d
PubMed | Crossref | Google Scholar - Viswanathan VK, Kukreja S, Minnema AJ, Farhadi HF. Prospective assessment of the safety and early outcomes of sublaminar band placement for the prevention of proximal junctional kyphosis. J Neurosurg Spine. 2018;28(5):520-531. doi:10.3171/2017.8.SPINE17672
Crossref | Google Scholar - Yoshie N, Maruo K, Arizumi F, Kishima K, Kusukawa T, Tachibana T. The Relationship between the Hounsfield Units Value of the Upper Instrumented Vertebra and the Severity of Proximal Junctional Fracture after Adult Spinal Deformity Surgery. Medicina (Kaunas). 2023;59(6):1086. doi:10.3390/medicina59061086
PubMed | Crossref | Google Scholar - Yoshida G, Ushirozako H, Hasegawa T, et al. Preoperative and Postoperative Sitting Radiographs for Adult Spinal Deformity Surgery: Upper Instrumented Vertebra Selection Using Sitting C2 Plumb Line Distance to Prevent Proximal Junctional Kyphosis. Spine (Phila Pa 1976). 2020;45(15):E950-E958. doi:10.1097/BRS.0000000000003452
PubMed | Crossref | Google Scholar - Zhao J, Chen K, Zhai X, Chen K, Li M, Lu Y. Incidence and risk factors of proximal junctional kyphosis after internal fixation for adult spinal deformity: a systematic evaluation and meta-analysis. Neurosurg Rev. 2021;44(2):855-866. doi:10.1007/s10143-020-01309-z
Crossref | Google Scholar - Zou L, Liu J, Lu H. Characteristics and risk factors for proximal junctional kyphosis in adult spinal deformity after correction surgery: a systematic review and meta-analysis. Neurosurg Rev. 2019;42(3):671-682. doi:10.1007/s10143-018-1004-7
PubMed | Crossref | Google Scholar - Sato K, Ito T, Endo T, Miura T, Iwabuchi M, Shirado O. Novel assessment of physiotherapy outcomes in adults with structural spinal disorders. Eur Spine J. 2023;32(6):1887-1894. doi:10.1007/s00586-023-07696-3
PubMed | Crossref | Google Scholar - Iyer S, Klineberg EO, Zebala LP, et al. Dural Tears in Adult Deformity Surgery: Incidence, Risk Factors, and Outcomes. Global Spine J. 2018;8(1):25-31. doi:10.1177/2192568217717973
PubMed | Crossref | Google Scholar - Than KD, Park P, Fu KM, et al. Clinical and radiographic parameters associated with best versus worst clinical outcomes in minimally invasive spinal deformity surgery. J Neurosurg Spine. 2016;25(1):21-25. doi:10.3171/2015.12.SPINE15999
PubMed | Crossref | Google Scholar - Murata S, Nagata K, Iwasaki H, et al. Long-Term Outcomes after Selective Microendoscopic Laminotomy for Multilevel Lumbar Spinal Stenosis with and without Remaining Radiographic Stenosis: A 10-Year Follow-Up Study. Spine Surg Relat Res. 2022;6(5):488-496. 2022. doi:10.22603/ssrr.2021-0200
PubMed | Crossref | Google Scholar - Fujimori T, Nagamoto Y, Takenaka S, et al. Development of patient-reported outcome for adult spinal deformity: validation study. Sci Rep. 2024;14(1):1286. doi:10.1038/s41598-024-51783-4
Crossref | Google Scholar - Bae J, Theologis AA, Strom R, et al. Comparative analysis of 3 surgical strategies for adult spinal deformity with mild to moderate sagittal imbalance. J Neurosurg Spine. 2018;28(1):40-49. doi:10.3171/2017.5.SPINE161370
PubMed | Crossref | Google Scholar - Murata S, Tsutsui S, Hashizume H, et al. Importance of physiological age in determining indications for adult spinal deformity surgery in patients over 75 years of age: a propensity score matching analysis. Eur Spine J. 2022;31(11):3060-3068. doi:10.1007/s00586-022-07379-5
PubMed | Crossref | Google Scholar - Than KD, Mummaneni PV, Bridges KJ, et al. Complication rates associated with open versus percutaneous pedicle screw instrumentation among patients undergoing minimally invasive interbody fusion for adult spinal deformity. Neurosurg Focus. 2017;43(6):E7. doi:10.3171/2017.8.FOCUS17479
Crossref | Google Scholar - Strom RG, Bae J, Mizutani J, Valone F 3rd, Ames CP, Deviren V. Lateral interbody fusion combined with open posterior surgery for adult spinal deformity. J Neurosurg Spine. 2016;25(6):697-705. doi:10.3171/2016.4.SPINE16157
PubMed | Crossref | Google Scholar - Wewel JT, Ozpinar A, Walker CT, Okonkwo DO, Kanter AS, Uribe JS. Safety of lateral access to the concave side for adult spinal deformity. J Neurosurg Spine. 2021;35(1):100-104. doi:10.3171/2020.10.SPINE191270
PubMed | Crossref | Google Scholar - Haddaway NR, Page MJ, Pritchard CC, McGuinness LA. PRISMA2020: An R package and Shiny app for producing PRISMA 2020-compliant flow diagrams, with interactivity for optimised digital transparency and Open Synthesis. Campbell Syst Rev. 2022;18(2):e1230 doi:10.1002/cl2.1230
PubMed | Crossref | Google Scholar - Alt Murphy M, Munoz-Novoa M, Heremans C, et al. European Stroke Organisation (ESO) guideline on motor rehabilitation. Eur Stroke J. 2025;10(4):1160-1188. doi:10.1177/23969873251338142
PubMed | Crossref | Google Scholar - Maredza M, Bertram MY, Gómez-Olivé XF, Tollman SM. Burden of stroke attributable to selected lifestyle risk factors in rural South Africa. BMC Public Health. 2016;16:143. doi:10.1186/s12889-016-2805-7
PubMed | Crossref | Google Scholar - Onyebuchi CW, Anyahara NH, Gbadamosi FO et al. Spinal Deformities in Paediatric Neuromuscular Disorders: A systematic review and Meta-Analysis of Prevalence, Predictors, and Surgical Outcomes. medtigo J Neurol Psychiatr. 2026;3(1):e3084314. doi:10.63096/medtigo3084314
Crossref - Brady MC, Mills C, Prag Øra H, et al. European Stroke Organisation (ESO) guideline on aphasia rehabilitation. Eur Stroke J. 2025;10(4):1189-1220. doi:10.1177/23969873241311025
PubMed | Crossref | Google Scholar - Getie A, Gedfew M, Kitaw TA, Yilak G, Bimerew M. Mortality rate of stroke and its determinants in Africa: An umbrella review of systematic review and meta-analysis. Glob Epidemiol. 2025;10:100225. doi:10.1016/j.gloepi.2025.100225
PubMed | Crossref | Google Scholar
Acknowledgments
The authors acknowledge that the data for this study were derived from peer-reviewed articles indexed in major biomedical databases, which formed the foundation of this work. We also thank the European Stroke Organisation and European Board of Neurology for their role in advancing clinical training and professional development in neurology.
Funding
None
Author Information
Corresponding Author:
Chinua Onyebuchi
Department of Neurology
Neurology Section, European Union of Medical Specialists, Brussels, Belgium
Email: [email protected]
Co-Authors:
Ali Mohammed Ramat, James Kefas Wida
Department of Orthopedic Surgery
National Orthopedic Hospital Azare – Hawul, Borno State, Nigeria
Sani Abdullahi Amoto
Department of Medicine
Madonna University Elele, Rivers State, Nigeria
Ikechukwu Eric Samuel Onwubuya
Department of Public Health
Torrens University, Australia
Chidinma Emmanuella Okobah
Department of Medicine
Delta State University College of Health Sciences, Nigeria
Authors Contributions
All authors contributed to conceptualization, data curation, drafting, review, and supervision, ensuring accuracy; all approved the final manuscript prior to submission.
Ethical Approval
This study used only publicly available data, adhering to GDPR principles and best practices for ethical, responsible, and transparent research conduct.
Conflict of Interest Statement
The authors declare no conflict of interest.
Guarantor
Chinua Onyebuchi is the guarantor of this study and takes full responsibility for the integrity of the data and the accuracy of data analysis.
DOI
Cite this Article
Ramat AM, Wida JK, Onyebuchi CW, Amoto SA, Onwubuya IES, Okobah CE. Neurovascular Outcomes in Adults Undergoing Surgery for Spinal Deformities: A Narrative Review. medtigo J Neurol Psychiatr. 2026;3(2):e3084324. doi:10.63096/medtigo3084324 Crossref













