






 Author Affiliations
Author Affiliations
Abstract
Background: Mental health literacy and stigma toward mental illness significantly influence recognition of psychological disorders, help-seeking behavior, and community support. In rural areas of Pakistan, limited awareness and strong sociocultural beliefs may contribute to misconceptions and negative attitudes toward mental illness.
Aim: To assess the level of mental health literacy and the degree of stigma toward mental illness among young adults in rural Swat, and to examine the association between these variables.
Methodology: A quantitative descriptive cross-sectional analytical study was conducted among 93 young adults aged 18–25 years residing in rural villages of Charbagh and Khwazakhela Union Councils, Swat. The sample size was calculated using G*Power software assuming a moderate correlation (r = 0.30), 95% confidence level, and 80% power. Data were collected using a structured questionnaire including socio-demographic variables, the 35-item Mental Health Literacy Scale (MHLS), and the 18-item Depression Stigma Scale (DSS). Descriptive statistics summarized literacy and stigma scores, and Pearson’s correlation coefficient was applied to assess the association (p < 0.05).
Results: Participants demonstrated moderate mental health literacy (mean ± SD: 108.4 ± 14.2) and moderate to high stigma levels (mean ± SD: 56.7 ± 9.8). A statistically significant negative correlation was found between mental health literacy and stigma (r = -0.46, p < 0.001), indicating that higher literacy was associated with lower stigma.
Conclusion: Mental health literacy among young adults in rural Swat was moderate, while stigmatizing attitudes persisted. Strengthening community-based mental health education and stigma-reduction initiatives is essential to promote early help-seeking and improve mental health outcomes.
Keywords
Mental health literacy, Stigma, Young adults, Depression stigma, Help-seeking behavior.
Introduction
The determinants of help-seeking behavior, early identification, and community support of individuals facing psychological disorders are mental health literacy and the stigmatization of mental illness.[1] Mental health literacy is the knowledge and perceptions regarding mental illness that can be used in the identification, treatment, or prevention of mental health issues. Stigma related to mental illness involves negative attitudes, perceptions towards a group of people, prejudice, and discriminatory practices toward mentally ill individuals. [2] Young adulthood is one of the transitional developmental stages that is marked by identity development, adaptation to social roles, and higher susceptibility to stress-related illnesses. Poor awareness and views toward mental illness may also be a factor in rural communities, with a variety of misconceptions. Mental health literacy and stigma are concepts that need to be understood to develop culturally related educational and awareness programs that can support psychological health and minimize the level of discrimination among young adults in rural Swat.[3]
Mental health disorders are a major contributor to the global burden of disease, with almost 13 % of total disability-adjusted life years being attributed worldwide.[4] Research has shown that about one out of every five young adults reports having a mental health issue every year, with anxiety disorders and depression disorders being the most common ones.[5] In most of the low- and middle-income countries, the level of mental health literacy is low despite this high prevalence. It has been found that 40-60 % of young adults are not well informed to be able to identify common mental disorders, more so in rural areas where there is low accessibility to information.[6]
Stigma against mental illness is also a significant obstacle to care. In most traditional societies, the negative beliefs that mental illness is a sign of weakness, spiritual punishment, or a social disgrace still exist.[7] This stigma deters help-seeking, delays diagnosis, and leads to social isolation of the affected individuals. Individuals who have been subjected to stigmatizing attitudes are not prone to seek professional help when in a state of psychological distress.[8]
Mental health literacy has an impact on attitudes and behavior that pertain to mental illness. Increased degrees of knowledge are connected with enhanced awareness of the symptoms, encouraging attitude, and enhanced chances of seeking professional attention [9]. Low literacy levels tend to attract misunderstanding, fear, and dependency on non-medical or informal activities.[10]
Mental illness is heavily subject to cultural beliefs and rural settings. In more conservative and rural societies, such as some of Khyber Pakhtunkhwa, mental illness is often explained by supernatural forces or some kind of moral breakdown.[11] These problems are also augmented by a lack of mental health services and trained professionals.[12]
Psychosocial stressors faced by young adults in the rural context of Swat are distinct; such problems may be economic instability, pressure to study, and job availability. The vulnerability to psychological distress may be augmented by exposure to sociopolitical unrest in the area and natural catastrophes.[13] Lack of awareness and stigmatization may further deteriorate the condition and lower resiliency in this group of people.
Education facilities and community educational measures are also essential in enhancing mental health literacy. There is evidence that organized mental health education can greatly decrease stigma and positively change attitudes of youth.[14] The early interventions that are aimed at young adults can be used to create a helpful peer environment and normalize the behavior of seeking help.
There is limited empirical evidence on mental health literacy and stigma among young adult people living in rural Swat. Most of the literature is based on cities or healthcare workers. The context-related evidence will have to be used to find out the gaps in knowledge, existing misconceptions, and sociocultural factors that may influence attitudes in this area. Mental health literacy and stigma among the young adults in rural Swat will be assessed to give baseline information in directing public health activities, educational efforts, and policy formulation to limit the stigma and enhance mental health.[15]
Methodology
The quantitative descriptive cross-sectional analytic design was chosen to assess mental health literacy and stigma against mental illness among the young adults living in rural settings in District Swat, Khyber Pakhtunkhwa, Pakistan. The search was done in the rural union councils of Charbagh and Khwazakhela, which symbolize the typical agrarian rural communities that are marred by limited access to mental health services and are replete with strong sociocultural values. The research population comprised youthful adults between the ages of 18 and 25 who had a minimum of 6 months of stay in these areas. The participants are both male and female; they have a range of educational and socioeconomic statuses.
Based on Fisher’s Z transformation, a priori power analysis using G*Power 3.1 was carried out to test the relationship between two continuous variables. The calculated minimum sample size was 84 participants with an expectation of a moderate effect size (r 0.30), 0.05 significance level, and power of 80 %. To offset non-response, 10 per cent was tentatively included, and this resulted in a target population of 93 people. The study participants were identified through convenience sampling, and participants with severe psychiatric conditions or cognitive deficiencies were excluded.
Data collection procedure: The institutional review board gave ethical approval before the beginning of the data collection. Local community leaders were also contacted to obtain their permission to recruit participants. Villages and small towns were visited, and informed consent was obtained before the participation of eligible young adults.
The data collection method was a structured, self-administered questionnaire with socio-demographic questions, MHLS, and DSS. The instrument was translated into Urdu and Pashto to make it culturally relevant. MHLS examined the knowledge in terms of mental disorders and help procedures, and the DSS measured personal and perceived stigmatization. Where the respondents had lower levels of literacy, the investigator read the questions aloud, ensuring neutrality of response. The questionnaire took about 15-20 minutes to complete, and confidentiality was ensured through coded responses.
Data analysis procedure: Data collected were coded, entered, and then analyzed statistically using the Statistical Package for the Social Sciences (SPSS) 27. Socio-demographic variables were summarized with descriptive statistics that included frequencies and percentages. Mean scores and standard deviations were determined between MHLS and DSS, as continuous variables. The correlation coefficient between mental health literacy and stigma was used by Pearson to evaluate the relationship between the two variables; a p-value of less than 0.05 was a statistically significant relationship.
Results
Demographic characteristics of participants: The socio-demographic make-up of the ninety-three young adults who participated in the study is outlined in Table 1. A marginally higher number of the cohort was male (51.6%), with females (48.4%), which means that there was a relatively equal gender distribution. The majority of respondents aged between 21 and 23 years were 39.8%, then 18 and 20 years were 31.2%, and 24 and 25 years were 29.0%. At the educational level, most of them were undergraduate (34.4%), followed by those at intermediate level (32.3%), secondary education (22.6%), and postgraduate status (10.7%). In regard to occupation, students had the highest percentage (58.1%), 22.6% were employed, and 19.3% were unemployed. Specifically, over fifty percent of the participants (57.0) reported that they had not, in the past, received formal mental-health information, which highlights potential gaps in mental-health literacy among the rural residents.
| Variable | Category | Frequency (n) | Percentage (%) |
| Gender | Male | 48 | 51.6 |
| Female | 45 | 48.4 | |
| Age (Years) | 18–20 | 29 | 31.2 |
| 21–23 | 37 | 39.8 | |
| 24–25 | 27 | 29.0 | |
| Education level | Secondary | 21 | 22.6 |
| Intermediate | 30 | 32.3 | |
| Undergraduate | 32 | 34.4 | |
| Postgraduate | 10 | 10.7 | |
| Occupation | Student | 54 | 58.1 |
| Employed | 21 | 22.6 | |
| Unemployed | 18 | 19.3 | |
| Received mental health information | Yes | 40 | 43.0 |
| No | 53 | 57.0 |
Table 4.1: Socio-demographic characteristics of participants
The mean of the Mental Health Literacy Scale (MHLS) was 104.36 with a standard deviation of 18.42 across the cohort. The range was between 62 and 145, thus showing a moderate, and in certain instances, strong level of mental health knowledge in the participants. Conversely, the Depression Stigma Scale (DSS) had a mean of 55.27 and a standard deviation of 12.15, and the lowest and highest scores were 29 and 82, respectively, indicating that there was a moderate level of stigma against mental illness in the sample.
| Variable | Mean ± SD | Minimum | Maximum |
| MHLS | 104.36 ± 18.42 | 62 | 145 |
| DSS | 55.27 ± 12.15 | 29 | 82 |
Table 2: Descriptive statistics of MHLS and DSS scores
Figure 1 shows the stratified levels of mental-health literacy of the surveyed cohort. The data shows that a significant percentage of 55.9 0.00 of the participants had moderate literacy levels, and 24.7 0.00 of the participants had high literacy levels. On the other hand, 19.4 %t of the respondents were categorized as having low mental-health literacy.
Such findings suggest that, despite most young adults showing an average level of knowledge regarding mental-health concepts, a significant proportion of them is still poorly informed about the related problems. Such a gap highlights the necessity of further educational interventions and specific awareness programs.
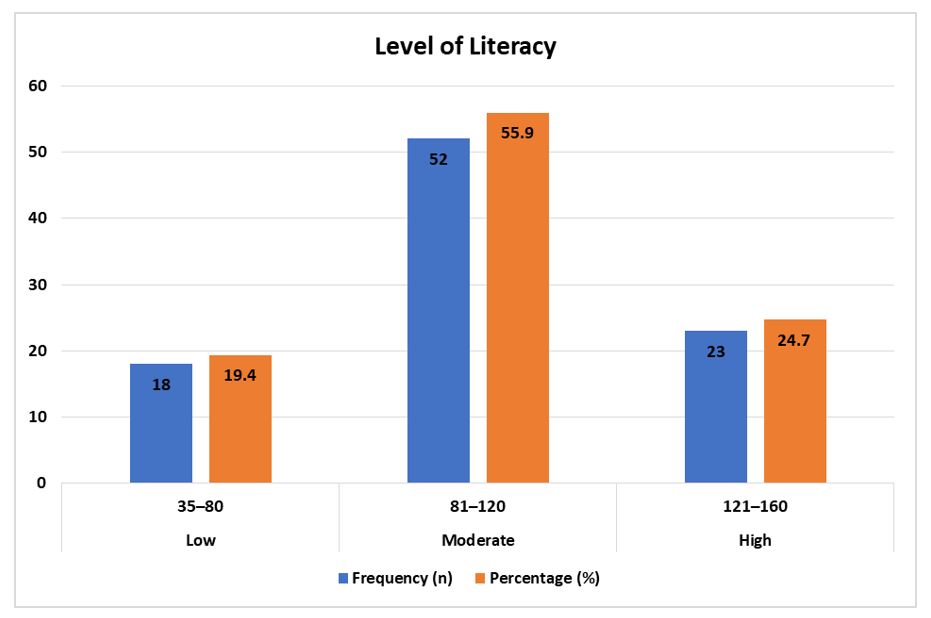
Figure 1: Level of mental health literacy (Categorized)
Figure 2 presents the distribution of stigma levels among participants. The majority (54.8%) exhibited moderate stigma toward mental illness. Low stigma levels were observed in 21.5% of participants, while 23.7% demonstrated high stigma. These results indicate that stigmatizing attitudes remain prevalent among young adults in rural Swat, despite varying levels of mental health literacy.
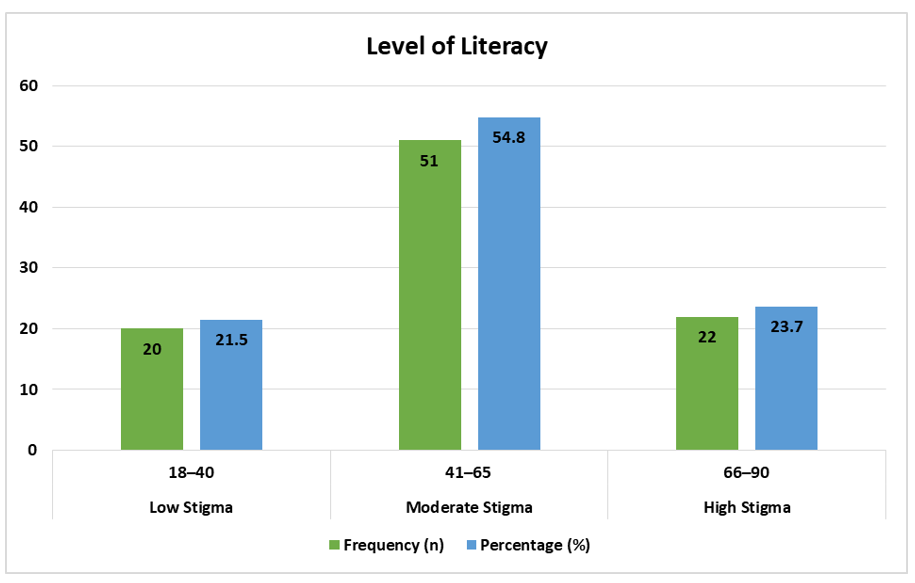
Figure 2: Level of stigma toward mental illness (Categorized)
The findings showed that there was a moderate negative relationship between the scores of MHLS and DSS, with r = -0.46. This correlation was statistically significant (p=0.001), which means that the higher the mental health literacy was, the lower the degree of stigma towards mental illness. These results indicate that the improvement of mental health knowledge may be a key factor in the minimization of stigma among young adults in rural Swat.
| Variables | Pearson’s r | p-value |
| MHLS & DSS | -0.46 | 0.001* |
Table 2: Correlation between mental health literacy and stigma (N = 93)
Discussion
The current research has determined the mental health literacy and stigma of mental illness in young adults in rural Swat and found moderate levels of literacy and moderate levels of stigma. The demographic results indicated an almost equal gender distribution and high representation of the age groups 21-23 years, which can also be associated with the studies carried out in the rural South Asian contexts, where young adults are considered an extremely important group to study in the context of mental health awareness (as well). [16] The student profile, with most of them being undergraduate and intermediate students, indicates that there is an uprising literate youth in rural areas, although formal education did not always result in the best mental health literacy.
The results showed that a significant percentage of the participants had not been informed about mental health before. This is in tandem with the past findings of low and middle-income countries that have indicated a lack of organized mental health education in rural societies. [17] Conversely, previous research outcomes in urban Pakistani and international settings have found that they were more exposed to mental awareness programs, which have enhanced the rate of literacy among the youth.[18] The reduced level of information exposure in the present study could indicate the deficits in the community-based awareness of rural swat.
The general mean mental health literacy scores implied a medium level of awareness about the awareness of the common disorders and a means of seeking help. Similar results were explained in rural Indian and Bangladeshi communities, where young people showed incomplete knowledge of depression and anxiety, but were not very clear about the ways of treatment.[19] There were, however, higher literacy scores in studies conducted in high-income countries, which may be because of systematic mental health education campaigns and the incorporation of mental health issues in school curricula.[20] This opposition signifies inequality in the distribution of resources and health communication.
The scores of stigmas in this research indicated that there were still negative attitudes towards mental illness, especially around personal stigma. The same cases were seen in Middle Eastern and South Asian studies that were conducted in rural areas, in which cultural beliefs linked mental illness to weakness or spiritual reasons.[22] Comparatively, the anti-stigmatization campaigns and open discussion have gradually reduced stigmatization observed in Western populations in the last few years.[23] The increased stigma levels in rural Swat could hence be affected by the sociocultural beliefs and lack of access to proper mental health information.
The mental health literacy and stigma were found to be significantly negatively correlated, which means that the greater the knowledge, the lower the stigmatizing attitude. The finding is in agreement with previous findings that show better literacy leads to fewer misconceptions and less discriminatory beliefs.[24] Similar correlations were also found between the students at the university in Malaysia and Turkey, which confirmed the hypothesis’s theoretical assumption that awareness is a protective factor against stigma.[25] There have, however, been some studies that have shown lesser associations, which argues that deeply held cultural beliefs might remain despite better knowledge.[26]
In this study, gender disparities with regard to literacy and stigma were low in comparison to some of the international results, where females generally show greater mental health literacy and reduced stigma.[27] There would be no significant gender disparities in rural Swat, which could be attributed to the fact that both genders were exposed to sociocultural factors and educational opportunities in the chosen communities to some extent. Homogeneity of cultures can decrease the differences among demographic subgroups.
The educational level did not show much impact on literacy scores, as the higher the participant’s academic level, the more likely they are to demonstrate higher comprehension of mental health concepts. This observation is consistent with a study that found formal education to be more effective at creating awareness and critical thinking about health matters.[26] However, education was not the ultimate predictor of reducing stigma, and this is a positive indication that knowledge is not solely a determinant of attitudes; rather, cultural discourses and beliefs in the community condition attitudes.[28]
The large percentage of students among the participants might have led to a relatively mediocre level of literacy since the educational settings expose students to some information about health. The same literacy trends were reported in studies of college students in Pakistan and other developing nations, although stigma was still predominant even with students enrolled in schools.[29] This indicates that schools in rural settings might need to have systematic mental health programs to aid in the elimination of attitudinal obstacles.
Conclusion
The current study evaluated the standard of mental health literacy and the extent of stigma towards mental illness among the rural Swat young adults. The results indicated that subjects portrayed satisfactory mental health literacy rates, although the stigmatization of mental illness was still quite elevated. There was a high inverse correlation between mental health literacy and stigma, which showed that the higher the literacy, the lower the negative attitude. Although most of the participants have a reasonable educational background, a low exposure to organized mental health information has led to continued misconceptions and discriminatory perspectives. The rural perception of mental illness seemed to be influenced by cultural factors, insufficient mental health services, and the absence of community-based awareness programs. The study indicates a dire need to implement specific educational programs to enhance awareness, stigma, and positive help-seeking behavior in the rural communities among young adults.
Recommendations: Based on the findings, the following recommendations are proposed: Mental health awareness programs should be provided in the rural Swat community to enhance knowledge and reduce stigma. Schools ought to incorporate systematic mental health education in the curriculum to promote literacy levels among young adults. Local language (Pashto and Urdu) based public health campaigns on mental illness cultural misconceptions must be created. Health care providers, religious leaders, and community elders should collaborate to enhance positive attitudes towards mental health. More extensive and longitudinal research needs to be done to understand more determinants of mental health literacy and stigma among the rural population.
References
- Verma S, Pandey B. Mental Health Literacy and Barriers to Care among Rural Women: A Systematic Review. J Behav Sci. 2025;20(3):120-130. doi:10.69523/tjbs.2025.287148
Crossref | Google Scholar - Goda AMI, Elhamid SAA, Wassif GO. Mental health literacy: a comparative study on stigmatizing attitude and help-seeking behavior towards mental disorders between adolescents and adults. J Egypt Public Health Assoc. 2025;100(1):7. doi:10.1186/s42506-025-00184-0
PubMed | Crossref | Google Scholar - Koutra K, Pantelaiou V, Mavroeides G. Breaking Barriers: Unraveling the Connection between Mental Health Literacy, Attitudes towards Mental Illness, and Self-Stigma of Psychological Help-Seeking in University Students. Psychology International. 2024; 6(2):590-602. doi:10.3390/psycholint6020035
Crossref | Google Scholar - Raghavan V, Chandrasekaran S, Paul V, et al. Effectiveness of a mental health literacy module on stigma related mental health knowledge and behaviour among youth in two educational settings in Chennai, South India: A quasi-experimental study. Asian J Psychiatr. 2024;98:104074. doi:10.1016/j.ajp.2024.104074
PubMed | Crossref | Google Scholar - Vasim KA, Ashokbhai PK, Biswas B, Soham S, Patel D, Gurha S. Mental Health Awareness and Stigma in the General Population: A Mixed-Methods Approach in Semi-Urban Areas. Cureus. 2025;17(12):e100401. doi:10.7759/cureus.100401
PubMed | Crossref | Google Scholar - Setia Lesmana MH, Chung MH. Mediating roles of perceived stigma and mental health literacy in the relationship between school climate and help-seeking behavior in Indonesian adolescents. PLoS One. 2024;19(5):e0298017. doi:10.1371/journal.pone.0298017
PubMed | Crossref | Google Scholar - Sayed M, Sinha A. Mental Health Literacy and Depression Literacy Among Young Adults. In: Sustainable Digital Technology and Ethics in an Ever-Changing Environment. Springer Cham; 2025.
Mental Health Literacy and Depression Literacy Among Young Adults - He XY, Tan WY, Guo LL, Ji YY, Jia FJ, Wang SB. Mental Health Literacy Among Urban and Rural Residents of Guangdong Province, China. Risk Manag Healthc Policy. 2024;17:2305-2318. doi:10.2147/RMHP.S479868
PubMed | Crossref| Google Scholar - Poudel DB, Sharif LS, Acharya S, Mahsoon A, Sharif K, Wright R. Mental Health Literacy and Attitudes Towards Mental Health Problems Among College Students, Nepal. Behav Sci (Basel). 2024;14(12):1189. doi:10.3390/bs14121189
PubMed | Crossref | Google Scholar - Renwick L, Pedley R, Johnson I, et al. Mental health literacy in children and adolescents in low- and middle-income countries: a mixed studies systematic review and narrative synthesis. Eur Child Adolesc Psychiatry. 2024;33(4):961-985. doi:10.1007/s00787-022-01997-6
PubMed | Crossref | Google Scholar - Afreen R, Surya SL, Jara T, et al. Enhancing mental health literacy and care through community-driven solutions in rural Bangladesh. Front Glob Womens Health. 2024;5:1478817. doi:10.3389/fgwh.2024.1478817
PubMed | Crossref | Google Scholar - Shah H, Atta U, Arif U. Nurses’ experiences with ethical dilemmas in critical care settings: A mixed-method study at Saidu Teaching Hospital. medtigo J Med. 2025;3(1):e30623135. doi:10.63096/medtigo30623135
Crossref | Google Scholar - Nyali J, Chirwa G, Chitalah BC, Jumbe S. Culturally adapting a mental health literacy intervention with youth (stakeholders) for implementation in Malawi universities. Mental Health Sci. 2025;3(1):e70007. doi:10.1002/mhs2.70007
Crossref | Google Scholar - Kwegyir Tsiboe A, Raghuraman S, Marshall TC. Caught between two worlds: mental health literacy and stigma among bicultural youth. Int J Qual Stud Health Well-being. 2024;19(1):2321644. doi:10.1080/17482631.2024.2321644
PubMed | Crossref | Google Scholar - Kumar P, Tiwari DS, Kanabar BR, Patel VK, Chanpa NB, Vasavada DA. Knowledge, stigma, and attitude toward mental illness among rural school students. Ann Indian Psychiatry. 2020;4(2):202-207. doi:10.4103/aip.aip_73_20.
Crossref | Google Scholar - Simões de Almeida R, Trigueiro MJ, Portugal P, et al. Mental Health Literacy and Stigma in a Municipality in the North of Portugal: A Cross-Sectional Study. Int J Environ Res Public Health. 2023;20(4):3318. 2023. doi:10.3390/ijerph20043318
PubMed | Crossref | Google Scholar - Schroeder S, Tan CM, Urlacher B, Heitkamp T. The Role of Rural and Urban Geography and Gender in Community Stigma Around Mental Illness. Health Educ Behav. 2021;48(1):63-73. doi:10.1177/1090198120974963
PubMed | Crossref | Google Scholar - Nazari A, Garmaroudi G, Foroushani AR, Hosseinnia M. The effect of web-based educational interventions on mental health literacy, stigma and help-seeking intentions/attitudes in young people: systematic review and meta-analysis. BMC Psychiatry. 2023;23(1):647. 2023. doi:10.1186/s12888-023-05143-7
PubMed | Crossref | Google Scholar - Ma KKY, Anderson JK, Burn AM. Review: School-based interventions to improve mental health literacy and reduce mental health stigma – a systematic review. Child Adolesc Ment Health. 2023;28(2):230-240. doi:10.1111/camh.12543
PubMed | Crossref | Google Scholar - Fleary SA, Joseph PL, Gonçalves C, Somogie J, Angeles J. The Relationship Between Health Literacy and Mental Health Attitudes and Beliefs. Health Lit Res Pract. 2022;6(4):e270-279. doi:10.3928/24748307-20221018-01
PubMed | Crossref | Google Scholar - Green B, Jones K, Lyerla R, Dyar W, Skidmore M. Stigma and behavioral health literacy among individuals with proximity to mental health or substance use conditions. J Ment Health. 2021;30(4):481-487. doi:10.1080/09638237.2020.1713998
PubMed | Crossref | Google Scholar - Murthy MKS, Dasgupta M, Chaturvedi SK. Mental Health Literacy in Rural India. In: Chaturvedi SK, ed. Mental Health and Illness in the Rural World. Springer; 2020.
Mental Health Literacy in Rural India - Hussain S, Khan A, Arshad L, Rubab E. Trapped in the Screen: Clinical Insights into Digital Addiction and Mental Health Among Young Adults. medtigo J Neurol Psychiatr. 2025;2(3):e3084234. doi:10.63096/medtigo3084234
Crossref | Google Scholar - Singh S, Zaki RA, Farid NDN, Kaur K. The Determinants of Mental Health Literacy among Young Adolescents in Malaysia. Int J Environ Res Public Health. 2022;19(6):3242. doi:10.3390/ijerph19063242
PubMed | Crossref | Google Scholar - Nishio A, Marutani T. Mental health literacy survey among Cambodia’s urban and rural populations: Results from a vignette-based population survey. PLoS One. 2022;17(4):e0265120. doi:10.1371/journal.pone.0265120
PubMed | Crossref | Google Scholar - Shivani KM, Judge J. Exploration of mental health awareness and stigma associated with mental illness among college students. Int J Health Sci. 2022;6(S2):80688076. doi:10.53730/ijhs.v6nS2.7014
Crossref | Google Scholar - Tully LA, Hawes DJ, Doyle FL, Sawyer MG, Dadds MR. A national child mental health literacy initiative is needed to reduce childhood mental health disorders. Aust N Z J Psychiatry. 2019;53(4):286-290. doi:10.1177/0004867418821440
PubMed | Crossref | Google Scholar - Ratnayake P, Hyde C. Mental health literacy, help-seeking behaviour and wellbeing in young people: implications for practice. The Educational and Developmental Psychologist. 2019;36(01):1-6. doi:10.1017/edp.2019.1
Crossref | Google Scholar - Bjørnsen HN, Espnes GA, Eilertsen MB, Ringdal R, Moksnes UK. The Relationship Between Positive Mental Health Literacy and Mental Well-Being Among Adolescents: Implications for School Health Services. J Sch Nurs. 2019;35(2):107-116. doi:10.1177/1059840517732125
PubMed | Crossref | Google Scholar
Acknowledgments
The authors would like to express their sincere gratitude to Dr. Shah Hussain, Principal/Associate Professor, Janbar College of Nursing, Swat, for his invaluable supervision, guidance, and support throughout the course of this study.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author Information
Corresponding Author:
Nasar Mian
Department of Nursing
National College of Nursing, Swat, Pakistan
Email: nasarmian819@gmail.com
Co-Authors:
Atta Ullah Khan, Muhammad Rayyan, Atta Ur Rahman, Anwar Sayed, Adam Khan, Saifullah Khan, Syed Shahzad Khalid, Salman Khan
Department of Nursing
National College of Nursing, Swat, Pakistan
Authors Contributions
Nasar Mian, Atta Ullah Khan, and Muhammad Rayyan contributed to data collection and data analysis. Atta Ur Rahman, Anwar Sayed, and Adam Khan were responsible for data collection and conducting the literature review. Saifullah Khan, Syed Shahzad Khalid, and Salman Khan contributed to data collection and data organization.
Ethical Approval
Ethical Approval was obtained from the National College of Nursing, Swat, Ref No NCN/IRB/2026/06.
Conflict of Interest Statement
The authors declare that there is no conflict of interest regarding the publication of this paper.
Guarantor
Nasar Mian is the guarantor of this study and takes full responsibility for the integrity of the data and the accuracy of the data analysis.
DOI
Cite this Article
Mian N, Khan AU, Rayyan M, et al. Mental Health Literacy and Stigma Towards Mental Illness Among Young Adults in Rural Swat. Medtigo J Neurol Psychiatr. 2026;3(2):e3084321. doi:10.63096/medtigo3084321 Crossref













