







 Author Affiliations
Author Affiliations
Abstract
Background: Proper chest tube management is vital for patient safety in thoracic care, and studies show that nursing professionals express gaps in knowledge acquisition and experience-based confidence. Thirty-five percent of nurses working in low-resource areas face training deficits, which lead to avoidable medical complications. Nursing competencies in chest tube management show insufficient investigation despite their essential clinical role, specifically in general surgical units.
Aim: This study assessed nurses’ knowledge and confidence levels in chest tube management at a tertiary hospital in Swat, Pakistan.
Methods: A cross-sectional investigation included 50 nurses employed at surgical wards who participated via convenience sampling. A self-administered questionnaire with validated instruments gathered the data to measure chest tube knowledge through multiple-choice questions about indications, complications, and maintenance, as well as confidence ratings on a 5-point Likert scale. A combination of descriptive statistics and chi-square tests analyzed knowledge and confidence data alongside their relationship. The researchers conducted their statistical analysis through statistical package for the social sciences (SPSS) version 26.
Results: Research findings showed that nursing staff obtained scores below the competency level for chest tube knowledge while maintaining an average score of 58.2 ± 14.7. An 80% participant majority showed low to moderate levels of confidence according to a Likert scale score average of 2.86 ± 1.12. The study showed that weak understanding of chest tube procedures was linked directly to reduced confidence levels in the measurements (Odds ratio (OR) = 5.67, p = 0.002). Sixty per cent of nurses participated without any prior training, which intensified the identified knowledge deficits.
Conclusion: A deficiency in nursing competency skills reveals an immediate necessity for special training programs that incorporate structured simulation methods for low-resource environments. Emergency preparedness interventions need to strengthen knowledge and confidence through mentorship alongside emergency response training.
Keywords
Chest tube management, Nursing competency, Knowledge gaps, Confidence levels, Low-resource settings.
Introduction
Nurses need to have advanced skills in chest tube management since this technique provides essential care for patients with pneumothorax, hemothorax, and post-operative thoracic drainage.[1] The nursing management of chest tubes requires proper care of the insertion site, together with drainage system monitoring and identification of possible complications. Patient safety outcomes during catheter insertion and management heavily depend on nursing expertise because different levels of nurse knowledge and confidence directly affect treatment results.[2] Healthcare professionals who provide direct patient care must follow evidence-based practices to manage thoracic drainage systems through nursing procedures. Theoretical understanding of practices is demonstrated through knowledge levels, while confidence levels determine nurses’ assurance when performing associated skills.[3]
Studies throughout the world show that nurses hold inadequate chest tube management understanding, ranging from 30% to 45%, while their confidence in dealing with tube complications spans from 25% to 40%. Doctors in low-resource areas demonstrate heightened figures because most nurses have never undergone formal training, after surveys indicated that such cases drive 15-20% of preventable complications, such as infections and delayed pneumothorax detection in thoracic patients. Nurses across all income levels perform better, but statistics indicate that 20-30% of nurses consider their competence insufficient, thus demonstrating universal requirements for standardized educational programs.
Several reports confirm that standardized chest tube management training remains inadequate in nursing care, which results in multiple knowledge deficits and procedural mistakes.[4] A study of tertiary care hospitals found that drainage output assessment competence, along with emergency complication detection skills, exists in 60 to 70 percent of nursing staff.[5] The concerned state of these deficits becomes critical when considering the dangerous nature of thoracic intervention, since delayed problem detection may produce dangerous issues such as tension pneumothorax or infection. Medical complications worsen because structured teaching programs are scarce in places with limited resources and inadequate mentoring opportunities.[6]
Nurses display different levels of confidence regarding chest tube management primarily due to factors such as their seniority in nursing and their practical experiences, and the availability of simulation-based learning opportunities.[7] Chest tube procedures cause distress among new nursing practitioners, even though senior nurses tend to overstate their clinical adeptness through routine procedures instead of following modern evidence-based strategies.[8] Competency assessments should be performed regularly to address the existing gaps, and training programs must be focused on matching them. Simulation-based learning develops benefits in nursing education in high-income nations, yet these resources remain unavailable across vast regions, which intensifies international differences in nursing readiness.[9,10]
The safety of patient care requires acknowledgement that unsatisfactory chest tube management leads to multiple safety risks, which keep patients in the hospital longer and worsen their health outcomes.[11] Respiratory compromise develops when medical personnel do not clamp properly, and they do not detect air leaks effectively. The workload intensifies when nurses operate in intensive care units (ICUs) alongside emergency departments because they must handle several challenging medical cases simultaneously.[12] Healthcare institutions should view this educational effort as both an educational priority and as a specific target for quality improvements within their organizations.[13]
The bulk of available research explores physician approaches toward chest tube placement, yet it barely touches upon how nursing practitioners provide ongoing care for these procedures.[14] The present deficiency ignores how nurses serve as the initial point of contact for detecting sudden clinical conditions alterations.[15] Nurses in Jordan demonstrated through a phenomenological study that training needs were expressed by 78% of the staff, especially regarding drainage system troubleshooting capabilities. The need for nursing education designed to fit medical settings across Southeast Asia and Sub-Saharan Africa persists because these regions show identical educational needs.[16]
The examination seeks to provide a structured assessment of nurses’ knowledge and confidence about chest tube care and determine necessary education targets. The study will apply mixed-methods analysis to measure competence deficiencies and conduct qualitative interviews that will unveil the obstacles related to workload and educational access restrictions.[17] This research will guide developers to create adaptable education programs that enable standardization of care processes in various healthcare institutes to generate better patient results and enhance nursing skill progression.
Methodology
The researchers used a cross-sectional research design to measure the knowledge and confidence levels of nurses performing chest tube responsibilities at Saidu Teaching Hospital (SGTH) in Swat. The research dedicated its activities to the surgical wards of this tertiary care facility that served many thoracic patients requiring chest tube insertion alongside care procedures. All registered surgical ward nurses employed at Saidu Teaching Hospital were part of the research target population. The researchers selected 50 nurses by using convenience sampling for data collection because these nurses were readily available and accessible. The study only accepted participants who met both six months of work experience in the ward and direct involvement in chest tube practices. The participants selected for the study included nurses who voluntarily agreed to join. The chosen environment served as an important setting in which to evaluate clinical competencies in practice. The researchers collected immediate information on existing competencies through this approach. The study disclosed useful information about the training needs for future training. Ethical principles received attention in all stages of the research process.
Data collection procedure: The data collection process utilized an adopted validated (CVI 0.86) and reliable (Cronbach’s Alpha 0.82) questionnaire, which participants filled out. This instrument targeted the evaluation of clinical skills and understanding regarding chest tube procedures by nurse practitioners. An assessment of knowledge included twenty multiple-choice questions (MCQS) that focused on core content about indications, potential complications, and maintenance procedures. The twenty multiple-choice questions evaluated the nurse’s theoretical knowledge of chest tube procedures. Participants evaluated their clinical skills performance competence using a 5-point Likert scale, measuring their self-perceived ability. The questionnaire utilized a five-point rating scale that began at “not confident at all” and ended at “very confident.” clinical skills component, participants with a mean score of ≥4.0 on the 5-point Likert scale (where 1 = “not confident at all” and 5 = “very confident”) were considered to have adequate clinical skill competence. The questionnaire was distributed to healthcare professionals working in surgical wards. Anonymity in responding was implemented to obtain truthful answers from participants. The established approach provided uniformity to data collection activities.
Data analysis procedure: The researchers employed SPSS version 26 for statistical computations, incorporating descriptive and inferential methods. The researchers utilized descriptive statistics to condense the data showing nurses’ understanding of chest tube care through mean scores and percentages. The assessment methodology accurately illustrated how the overall performance spread and competency distribution appeared in the sample group. The chi-square test was performed as an inferential analysis to determine relationships between selected variables that included years of experience and knowledge or confidence levels. Analysis of the data revealed important associations between different variables through this method. The study used a p <0.05 significance level to confirm the reliability of its research findings.
Results
Demographic characteristics of participants: Research data collected from 50 participants showed that young nurses formed 80% of the total, while males made up 60% of the sample. The nursing professionals in this study had between one and five years of experience (56%), yet a notable percentage (34%) had over five years of experience. A significant percentage of 60% among participants lacked formal education or training for managing chest tubes, which demonstrates a critical need for ongoing nursing education. The study results identify a compelling training need because young nurses with minimal experience need specialized instruction (Table 1).
| Variable | Category | Frequency (n) | Percentage (%) |
| Age (years) | 20–30 | 22 | 44.0 |
| 31–40 | 18 | 36.0 | |
| 41–50 | 8 | 16.0 | |
| >50 | 2 | 4.0 | |
| Gender | Male | 30 | 60.0 |
| Female | 20 | 40.0 | |
| Experience (years) | <1 | 5 | 10.0 |
| 1–5 | 28 | 56.0 | |
| >5 | 17 | 34.0 | |
| Previous training | Yes | 20 | 40.0 |
| No | 30 | 60.0 |
Table 1: Demographic characteristics of nurses (N = 50)
Knowledge levels of nurses in chest tube management: The evaluation showed wide knowledge deficits because 74% of nurses achieved less than 70% competency marking (24% poor and 50% fair). Chest tube management knowledge levels among nurses were inadequate because only 26% scored in the adequate range (6% excellent and 20% good), while 74% exhibited inadequate understanding (50% fair plus 24% poor). Systemic training deficits exist across the healthcare profession according to the positively skewed distribution (mean = 58.2 ± 14.7), particularly because 60% of participants did not receive formal instruction. The research demonstrates an immediate requirement to develop standardized educational initiatives for enhancing clinical proficiency.
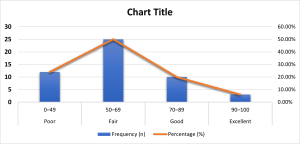
Figure 1: Knowledge levels of nurses in chest tube management (MCQ Scores, N = 50)
Confidence levels of nurses in chest tube management: The assessment showed worrisome results because nurses reported low confidence levels in chest tube management, as only 20% expressed high confidence (mean = 4.2). Eighty percent of nurses showed limited confidence in chest tube management, among which 36 percent demonstrated particularly low confidence (mean = 1.8) and 44 percent had moderate levels of confidence (mean = 3.0). Significant performance anxiety is demonstrated in the overall confidence distribution (mean = 2.86 ± 1.12) among nurses, even though 60% received no official training. The discovered results demonstrate strongly that healthcare facilities require ongoing practical simulation training and experienced mentorship to build nursing practitioners’ confidence in handling this significant intervention.
| Confidence level | Mean score (1–5) | Frequency (n) | Percentage (%) |
| Not confident (1–2) | 1.8 | 18 | 36.0% |
| Moderately confident (3) | 3.0 | 22 | 44.0% |
| Very confident (4–5) | 4.2 | 10 | 20.0% |
Table 2: Confidence levels of nurses in chest tube management (Likert scale, N = 50)
Association between knowledge and confidence levels: The study results showed that knowledge positively correlated with confident practice of chest tube management because the obtained result had statistical significance (χ² = 9.72, p = 0.002). The study showed that well-informed nurses showed 5.7 times higher rates of confidence reporting (85% opposed to 15%, OR = 5.67, 95% confidence interval (CI): 1.42-22.6). Research data shows that 75% of nurses with low clinical confidence displayed weak knowledge levels, indicating a cyclic pattern of knowledge deficiencies destroying their confidence in chest tube care. The outcome shows that education must teach both conceptual knowledge and practical competencies to enhance clinical competency in nursing practice.
| Variable | Poor knowledge | Good knowledge | p-value |
| Low confidence | 15 (75%) | 3 (15%) | 0.002 |
| High confidence | 5 (25%) | 17 (85%) | – |
Table 3: Association between knowledge and confidence levels (Chi-Square test, N = 50)
Discussion
The study demonstrates genuine knowledge and confidence deficiencies among nursing professionals when it comes to chest tube management during clinical practice and builds upon earlier research results. The nursing workforce of this study consists mainly of junior staff with little experience, since 80% were between 20 and 40 years old, and 56% possessed 1 to 5 years of nursing practice. Results indicate that young nurses who have limited experience constitute most of the workforce, since 60% of practitioners have not received formal training.[18] This figure nearly matches the double percentage reported by better-funded healthcare systems.
General surgical nurses participated in this study instead of specialized teams, thus possibly explaining why knowledge deficits reached 74% below the competency threshold. An alarming deficit was found when participants answered questions about emergency complications, so it appears that such settings face challenges in evaluating critical conditions, including tension pneumothorax.[18,19] Results indicated that structured training programs increase educational attainment since the observed mean knowledge score (58.2%) stood much lower than those measured in programs.[20]
The survey indicates low confidence among medical students because just one-fifth had high confidence, compared to better performance observed in studies from settings with better resources. Healthcare professionals may have different amounts of clinical contact and less access to simulation training, as explained in this gap. The direct relationship between nurses’ knowledge levels and confidence stood out stronger than in other studies, probably since this research site did not provide supportive structures for building confidence despite low knowledge.[21]
Male nurses exhibited higher confidence levels than their female counterparts, who showed identical knowledge test results in this study, although other studies failed to detect such a gender discrepancy.[22] Experienced nurses in this context-maintained competence without formal training recently, while studies from other contexts showed skill degradation following a lack of education refreshers. It appears that informal mentorship practices maintain proficiency in these nurses.
The results obtained are significant for both nursing education and clinical practice. The findings establish an immediate requirement for specific training opportunities in scarcity-related healthcare facilities that must prioritize emergency preparedness curriculum.[23] Simulation-based practical education should complement didactic methods because the obtained confidence gap data indicates this combination leads to better results in nursing education. Further investigation of the gender gap in confidence should be conducted to create equal development opportunities for both genders.[24]
Several boundaries existed in this research because it concentrated its data collection at one facility while using subjective confidence reporting from participants. The research would gain strength by conducting studies across multiple facilities while observing healthcare workers demonstrate their competencies.[25] The research outcomes validate the necessity of delivering systematic training approaches that address distinct service requirements in healthcare facilities. These initiatives need to focus on both completing knowledge acquisition and developing practitioner confidence, specifically in emergency response readiness as well as risk identification.
Contextual factors shown in the study strongly affect competency growth because they affect staff demographics and training opportunities, as well as clinical encounter frequency. The findings indicate nurses should adapt evidence-based interventions to their local healthcare environment since one-size solutions do not always translate directly to other healthcare facilities.[26]
Recommendations
The recommended solution involves both classroom instruction and hands-on training for nurses requiring instruction about chest tube procedures through affordable simulation models while concentrating on emergency response actions that address tension pneumothorax complications. Nurse competency assessments need to be built into systems that combine biannual skills tests with professional assessments to certify competent patient care before independent nursing practice begins. The thoracic care team structure should receive full-time commitment, while bedside tools and continuous consultation from expert personnel need installation. Educational programs should implement confidence-building endeavors by providing psychological preparedness training together with peer support groups and recognition programs. Public policies need to secure institutional financial support, dedicated time for educational development, and relevant training content that fits the specific needs of understaffed medical sites. Additional studies need to examine intervention effectiveness on patient recovery results, together with gender patterns of confidence growth, and establish economic simulation techniques for hospitals with minimal resources to create enduring progress in nursing expertise and healthcare quality.
Conclusion
A research investigation discloses major deficiencies in both competency levels and skill confidence of nurses who care for chest tubes, specifically among less skilled beginner staff at understaffed facilities. Research results demonstrate that insufficient formal training causes substandard skill competence because most nursing professionals score below the necessary requirements for safe clinical practices. Extensive training programs should be implemented because knowledge deficits strongly relate to poor confidence levels among nursing staff. The serious nature of chest tube treatment creates additional difficulties because any mistakes could produce fatal outcomes. The analysis demonstrates that enhancing nurses’ abilities to care for chest tubes is an essential patient safety matter, and, above all else, it is an educational need.
References
- Silva EG da, Araujo BR, Borges R de M, Vieira TW, Paula CC de, Caregnato RCA. Nursing care for adult patients with chest drainage: a scoping review. Rev Esc Enferm USP. 2024;58:e20240017. doi:10.1590/1980-220X-REEUSP-2024-0017en PubMed | Crossref | Google Scholar
- Mahmoud SF, Mourad AH, Senosy AMK. Effect of educational guidelines on nurses’ performance for caring of critically ill patients with digital chest drainage system. Egypt J Health Care. 2023;14(4):864-873. doi:10.21608/ejhc.2023.334880 Crossref | Google Scholar
- Salime RAA, Abd El-Aziz WW, Al-Metyazidy HA, Weheida SM. Effectiveness of implementation of evidence-based educational intervention regarding chest tube on clinical patient’s outcomes in cardiothoracic care unit. Egypt J Health Care. 2021;12(1):171-192. doi:10.21608/ejhc.2021.138613 Crossref | Google Scholar
- Finn JK. Physiotherapy treatment modalities and the effects thereof on clinical outcomes when addressing intra-pleural abnormalities in trauma patients: A systematic review. Master’s thesis. University of the Witwatersrand; 2023. Physiotherapy treatment modalities and the effects thereof on clinical outcomes when addressing intra-pleural abnormalities in trauma patients: A systematic review
- Qalawa SA. Nurse’s performance regarding caring of patient with chest drain according to their demographic variables. Int J Health Sci. 2022;6(S5):10367-10382. Nurse’s performance regarding caring of patient with chest drain according to their demographic Variables
- Kayser SA, Williamson R, Siefert G, Roberts D, Murray A. Respiratory rate monitoring and early detection of deterioration practices. Br J Nurs. 2023;32(13):620-627. doi:10.12968/bjon.2023.32.13.620 PubMed | Crossref | Google Scholar
- Kever A. Enhancing nurse confidence and efficiency in chest tube management: implementation of a structured troubleshooting checklist. Abstract presented at: 2024 Parkview Health Nursing Research Symposium; November 7, 2024; Fort Wayne, Indiana, United States. Accessed April 25, 2025. Enhancing Nurse Confidence and Efficiency in Chest Tube Management: Implementation of a structured troubleshooting checklist
- Matlhola TP. Nurses’ role in mechanical ventilation management in neonatal intensive care units in academic tertiary care. Dissertation. University of the Witwatersrand, Johannesburg; 2020. Nurses’ role in mechanical ventilation management in neonatal intensive care units in academic tertiary care
- Hippe DS, Umoren RA, McGee A, Bucher SL, Bresnahan BW. A targeted systematic review of cost analyses for implementation of simulation-based education in healthcare. SAGE Open Med. 2020;8:2050312120913451. doi:10.1177/2050312120913451 PubMed | Crossref | Google Scholar
- Bajwa M, Najeeb F, Alnazzawi H, et al. A scoping review of Pakistani healthcare simulation: insights for lower-middle-income countries. Cureus. 2024;16(12):e76485. doi:10.7759/cureus.76485 PubMed | Crossref | Google Scholar
- Gan KL, Tan M. Evidence-based management of patients with chest tube drainage system to reduce complications in cardiothoracic vascular surgery wards. Int J Evid Based Healthc. 2015;13(2):58-65. doi:10.1097/XEB.0000000000000041 PubMed | Crossref | Google Scholar
- Anderson D, Chen SA, Godoy LA, Brown LM, Cooke DT. Comprehensive Review of Chest Tube Management: A Review. JAMA Surg. 2022;157(3):269-274. doi:10.1001/jamasurg.2021.7050 PubMed | Crossref | Google Scholar
- Aloufi O, Alharbi N. Awareness and practice of nine life-saving patient safety solutions among healthcare workers. Int J Health Sci. 2023;7:3640-3654. doi:10.53730/ijhs.v7nS1.15287 Crossref | Google Scholar
- Visser LS, CPEN F, Montejano AS. Rapid access guide for triage and emergency nurses: chief complaints with high-risk presentations. eBook. 2nd edition. Springer Publishing Company; 2023. Rapid Access Guide for Triage and Emergency Nurses
- Guo X, Li H, Zou Q, Cao Y, Lin T, Zhang M. How Do Nurses Decide on Missed Nursing Care? A Grounded Theory Study of Grassroots Arrangement of Nursing Care. J Clin Nurs. 2025. doi:10.1111/jocn.17648 PubMed | Crossref | Google Scholar
- Abdelhadi N, Drach-Zahavy A, Srulovici E. The nurse’s experience of decision-making processes in missed nursing care: A qualitative study. J Adv Nurs. 2020;76(8):2161-2170. doi:10.1111/jan.14387 PubMed | Crossref | Google Scholar
- Zeyrek Kurtoglu S, Yildirim Cetinkaya M, Erbas A. Nurses’ knowledge levels about the care of the patients with chest tube. Int J Caring Sci. 2021;14(2):1334-1342. Nurses’ Knowledge Levels About the Care of the Patients with Chest Tube
- Ramjan LM, Maneze D, Krstevska E, Pathrose SP, Lewis P. Educational programs to improve nurses’ knowledge, attitude, and practice in adolescent and young adult health: An integrative review. Nurse Educ Today. 2022;118:105510. doi:10.1016/j.nedt.2022.105510 PubMed | Crossref | Google Scholar
- Carney PA, Valenzuela S, Ericson A, et al. The association between length of training and family medicine residents’ clinical knowledge: a report from the Length of Training Pilot Study. Fam Med. 2023. doi:10.22454/FamMed.2023.427621 PubMed | Crossref | Google Scholar
- Daibes MA, Iblasi AS, Demir Korkmaz F, Oden TN, Elagoz I. Assessing pressure injury knowledge among Jordanian and Turkish nursing students: A cross-cultural comparison. J Tissue Viability. 2024;33(4):706-711. doi:10.1016/j.jtv.2024.07.007 PubMed | Crossref | Google Scholar
- Foronda CL, Fernandez-Burgos M, Nadeau C, Kelley CN, Henry MN. Virtual Simulation in Nursing Education: A Systematic Review Spanning 1996 to 2018. Simul Healthc. 2020;15(1):46-54. doi:10.1097/SIH.0000000000000411 PubMed | Crossref | Google Scholar
- Shayan Z, Khoddami N, Jafari P, Askarian M, Borazjani R. Gender differences in nurses’ knowledge, practice, and attitudes towards contact isolation precautions: a measurement invariance study. Shiraz E-Med J. 2024;26(3):e148167. doi:10.5812/semj-148167 Crossref | Google Scholar
- Reierson IÅ, Ravik M, Blomberg K, et al. Comparing didactic approaches for practical skills learning in Scandinavian nursing simulation centres: A qualitative comparative study. J Adv Nurs. 2024;80(12):5003-5017. doi:10.1111/jan.16150 PubMed | Crossref | Google Scholar
- Bø B, Madangi BP, Ralaitafika H, Ersdal HL, Tjoflåt I. Nursing students’ experiences with simulation-based education as a pedagogic method in low-resource settings: A mixed-method study. J Clin Nurs. 2022;31(9-10):1362-1376. doi:10.1111/jocn.15996 PubMed | Crossref | Google Scholar
- Usak M, Kubiatko M, Shabbir MS, Dudnik OV, Jermsittiparsert K, Rajabion L. Health care service delivery based on the Internet of Things: a systematic and comprehensive study. Int J Commun Syst. 2020;33:e4179. doi:10.1002/dac.4179 Crossref | Google Scholar
- Nifakos S, Chandramouli K, Nikolaou CK, et al. Influence of Human Factors on Cyber Security within Healthcare Organisations: A Systematic Review. Sensors (Basel). 2021;21(15):5119. doi:10.3390/s21155119 PubMed | Crossref | Google Scholar
Acknowledgments
The authors would like to express their sincere gratitude to Dr. Shah Hussain, Principal/Assistant Professor, Zalan College of Nursing, Swat, for his invaluable supervision, guidance, and support throughout the course of this study.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author Information
Corresponding Author:
Sabiha RGN
Department of Nursing
Magdalene Nursing Care Home, UK
Email: [email protected]
Co-Authors:
Naheed Akhtar
Department of Nursing
Sina Institute of Nursing & Allied Health Science, Quetta, Balochistan
Zar Tasha
Department of Nursing
Mirpur Institute of Medical Sciences, AJK
Najma Naz
Department of Nursing
Institute of Nursing Science, KMU, Peshawar
Shah Hussain
Department of Nursing
Zalan College of Nursing, Swat, Pakistan
Authors Contributions
Sabiha was responsible for data collection and data analysis. Naheed Akhtar and Zar Tasha contributed to data collection and literature review. Shah Hussain and Najma Naz were involved in data analysis.
Ethical Approval
All ethical considerations were addressed throughout every phase of the study. Institutional approval was obtained from SGTH (Ref No: SGTH/IRB/25/16). Prior to data collection, the research adhered to all ethical requirements. Written informed consent was obtained from each participant after they were informed about the study’s purpose, procedures, and their rights, including voluntary participation and the freedom to withdraw at any time without penalty. To ensure confidentiality, personal identifiers were replaced with questionnaire codes, and all data were securely stored with access limited to the research team.
Conflict of Interest Statement
The authors declare no conflict of interest.
Guarantor
Sabiha is the guarantor of this study and takes full responsibility for the integrity of the data and the accuracy of the data analysis.
DOI
Cite this Article
Sabiha RGN, Naheed A, Zar T, Najma N, Shah H. Knowledge and Confidence Levels of Nurses in Chest Tube Management. medtigo J Med. 2025;3(2):e30623210. doi:10.63096/medtigo30623210 Crossref













