






 Author Affiliations
Author Affiliations
Abstract
Background: Critically ill patients are at high risk of pressure ulcer development, with an incidence ranging from 7% to 71.6% across countries.
Broad objective: To determine pressure ulcer incidence and risk factors among critically ill patients at Kenyatta national hospital.
Design: Prospective Cohort study.
Study Method: The Study is a prospective observational single-center study conducted over 3 months at Kenyatta national hospital main critical care unit.
Results: The incidence of pressure ulcers was 15%. Mechanical ventilation (p=0.001), increasing sedation time (odds ratio (OR)=14.0, confidence interval (CI) 2.63 – 74.59, p=0.002), and each unit increase in the length of stay (OR=1.91, p<0.001) were independently associated with pressure ulcer development.
Conclusion: Measuring the incidence of pressure ulcers among critically ill patients is crucial. Mechanical ventilation, length of stay in the unit, and increasing sedation time were identified as independent risk factors for pressure ulcer development.
Keywords
Critical care unit, Pressure ulcer, Incidence, Risk factors, Critically ill, Length of stay.
Introduction
Pressure ulcers represent a major burden but potentially avoidable conditions most often seen in bedridden, elderly, and critically ill patients. A pressure ulcer is an injury to the skin and underlying soft tissues due to prolonged pressure, moisture, friction,n and shear or an association of these, generally over a medical device or a bony prominence. Effective preventive measures may reduce the duration and the severity of pressure and shearing forces. Frequent changes in posture, cushions, and pressure-relieving mattresses have been shown to reduce the effect of pressure on the skin.[1]
Critical care unit (CCU) patients have more than 10-fold higher hospital pressure ulcer incidence rates compared to non-critical care unit patients. The length of stay in the intensive care unit (ICU) and the cost of care for hospitalized patients with pressure ulcers have been found to be higher compared to patients without pressure injuries.[2,3] A study by Lim ML, et al: (2017) found that the median total cost of care is $17,200 in a patient without pressure injuries. In contrast, the median cost of care for patients with pressure ulcers was significantly higher at $36,500.[4] Pressure ulcer incidence rates vary from one country to another. Studies done across countries have shown an incidence rate ranging from 7% to 71.6%.[5] The high incidence rates among critically ill patients are due to multiple risk factors associated with the development of pressure ulcers. Shahin ES et al, have shown that pressure ulcer is a complex phenomenon that involves multiple factors rather than single risk factors in the patient. Tayyib N, et al conceptualized risk factors into intrinsic (inherent factors of critical illness) and extrinsic (related to external forces) factors.[6-10]
Pressure ulcer occurrence is a serious problem in a healthcare facility. However, its incidence and associated risk factors remain unknown in Kenyattanational hospital. This study aims to determine the incidence and risk factors associated with Pressure ulcer development in critically ill patients admitted to KNH-main CCU. Knowledge of potential risk factors will enable critical care providers to prevent the occurrence of pressure ulcers, thus reducing incidence rates in critically ill patients.
Pressure ulcers usually occur in bedridden and critically ill patients. Kenyatta national hospital main CCU is a surgical ICU mainly catering for trauma patients with severe head injuries, being the commonest cause of admission. These patients are bedridden for long periods, thus at high risk of developing pressure ulcers.
No studies have been done locally, as far as this condition is concerned. There is no clear protocol guiding the management of pressure ulcers from admission to discharge in the main critical care unit. This study will shed more light on the condition and will form a basis for the formation of a protocol on the management of pressure ulcers at KNH- main CCU. This study is focused on incidence and risk factors associated with pressure ulcers development among the patients admitted to Kenyatta national hospital-main critical care unit.
Methodology
Design: This is a 3-month prospective cohort study involving patients admitted to the main critical care unit between July 10th and October 9th, 2021.
Study site: The study was conducted in the main critical care unit of the Kenyatta national hospital.
Study Population: All patients admitted to KNH-main CCU during the data collection period are included. Patients admitted to the unit with pre-existing pressure ulcers and patients who declined to sign consent are excluded from the study.
Sampling procedure/ Selection of study participants: All Patients included in the study were actively monitored for pressure ulcers. Consecutive sampling method was used to select study participants until the desired sample size was achieved. Patients were followed from admission to discharge or death. The average length of stay in the unit (20 days) was used as the end of follow-up for patients who were not discharged or died within the study period.
Recruitment and consenting: All patients admitted to the KNH main critical care unit who met the inclusion criteria were enrolled in the study after the consent had been signed by their next of kin. The principal investigator recruited study participants every 48 hours.
Data collection procedures: Study participants were recruited by the principal investigator. Voluntary participants were enrolled based on informed consent obtained from their next of Kin after the nature of the study was explained to them. Prior to data collection, the principal investigator trained research assistants on data collection tools.
Research assistants: Four critical care nurses were trained as research assistants. An educational session on US NPUAP and the Braden scale was given to research assistants prior to data collection. The research assistants were inspecting the study participants from head to toe at the time of nursing care in the early morning. Information was collected by means of the research assistant-administered questionnaire. Additional Data were collected from patients’ clinical records, clinical examination, and interaction with primary nurses; laboratory and radiologic investigations requested by the CCU team using a research assistant-administered questionnaire. Data was taken every 48 hours by the principal investigator and research assistants.
Data analysis: Data was coded and entered into Epi data version 3.1 and exported to statistical package for the social sciences (SPSS) version 23 statistical software for analysis. Demographic and clinical characteristics of patients are presented as frequencies and percentages for categorical data and as means with standard deviations (SD) for continuous data. The incidence of pressure ulcers was calculated as a proportion of those patients who developed pressure ulcers over the total sample size and presented as a percentage. The risk factors associated with pressure ulcer development among critically ill patients were assessed with the use of Chi-square tests, and those found to be significant were subjected to multivariate analysis with the use of logistic regression. Odds ratios as well as 95% confidence intervals were calculated and reported where appropriate. All statistical tests were considered significant where the p-value was < 0.05.
Variables: The studied variables are age, gender, admitting diagnosis, date of occurrence, location of pressure ulcers, progression to the most severe stage, mechanical ventilation, sedation, and length of stay in the unit, which constitute the focus of this article. Laboratory variables (Hemoglobin, blood sugar, creatinine, albumin, white blood cells (WBC)), history of co-morbid medical conditions (diabetes mellitus (DM), cardiovascular disease, kidney failure, prognostic variables (Braden scale for pressure ulcer risk and APACHE II score), treatment with steroids, variables related to pressure relief area, nutritional status (body adiposity index (BAI)) will be looked at in the next article.
Results
113 patients were recruited and followed during the study period in the Kenyatta national hospital- main critical care unit.
Demographic characteristics: Demographically, the present study recruited 77 (68.1%) males and 36 (31.9%) females. Most patients were aged between 21 and 40 years, with a mean age of 37.0 (SD 20.8), and the minimum and maximum ages being 5 months and 88.0 years.
| Pressure ulcer | ||||
| Yes (n=12) | No(n=72) | OR (95% CI) | p-value | |
| Age, mean±SD | 40.0±23 | 1.00 | 0.509 | |
| 2 | (0.98– 1.03) | |||
| Gender, n | 13 | 64 | 1.63 | 0.427 |
| (%)Male/ | (76.5) | (66.7) | (0.49– 5.39) | |
| Female | 4 (23.5) | 32 (33.3) | Reference | |
Table 1: Demographic characteristics
There was a difference in the odds and no statistical differences (p=0.509) for age and development of pressure ulcer, and on gender, the odds of developing pressure ulcer were 1.63 times more for males than for females, but there was no statistical association (p=0.427).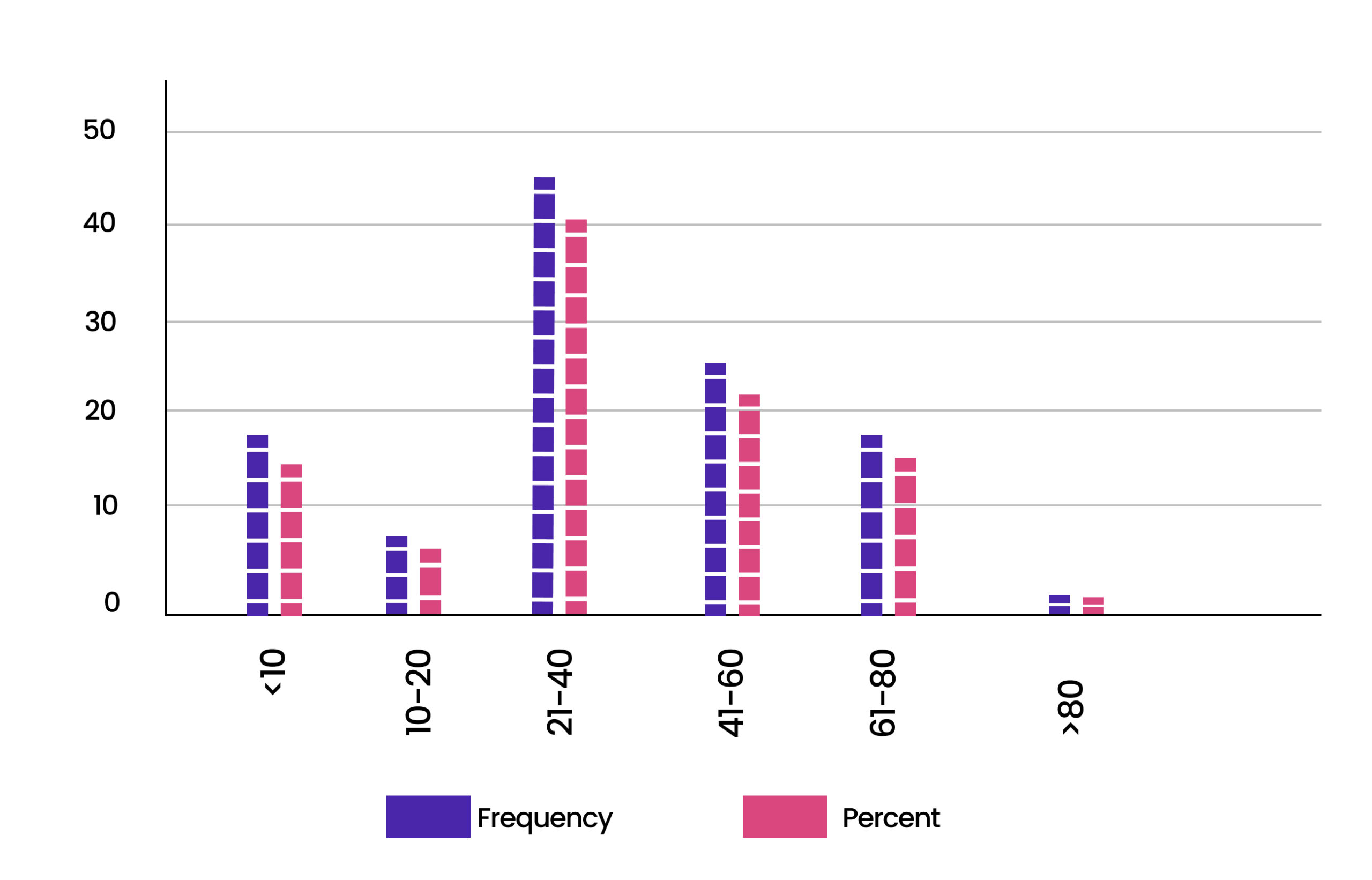
Figure 1: Distribution by age
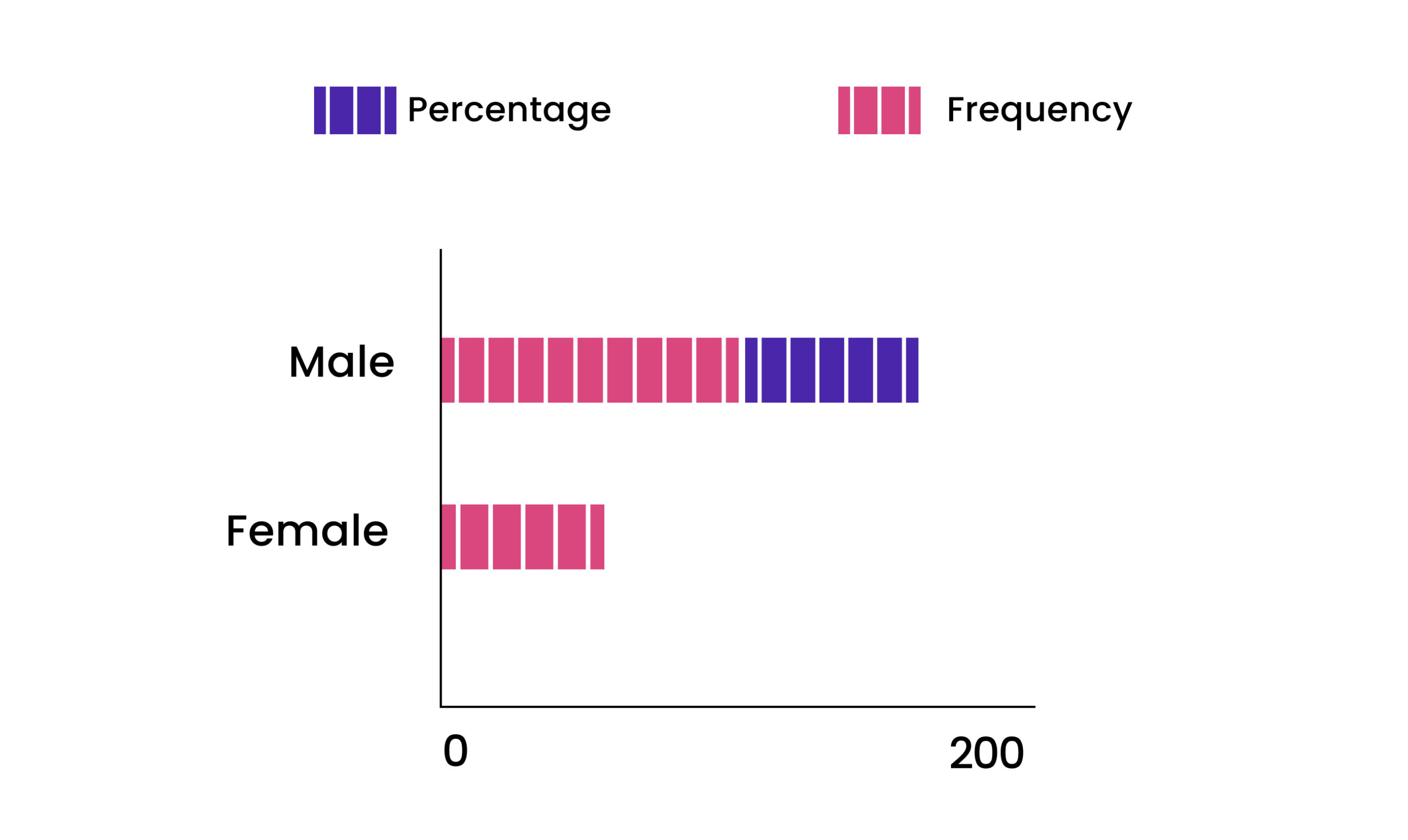
Figure 2: Distribution by gender
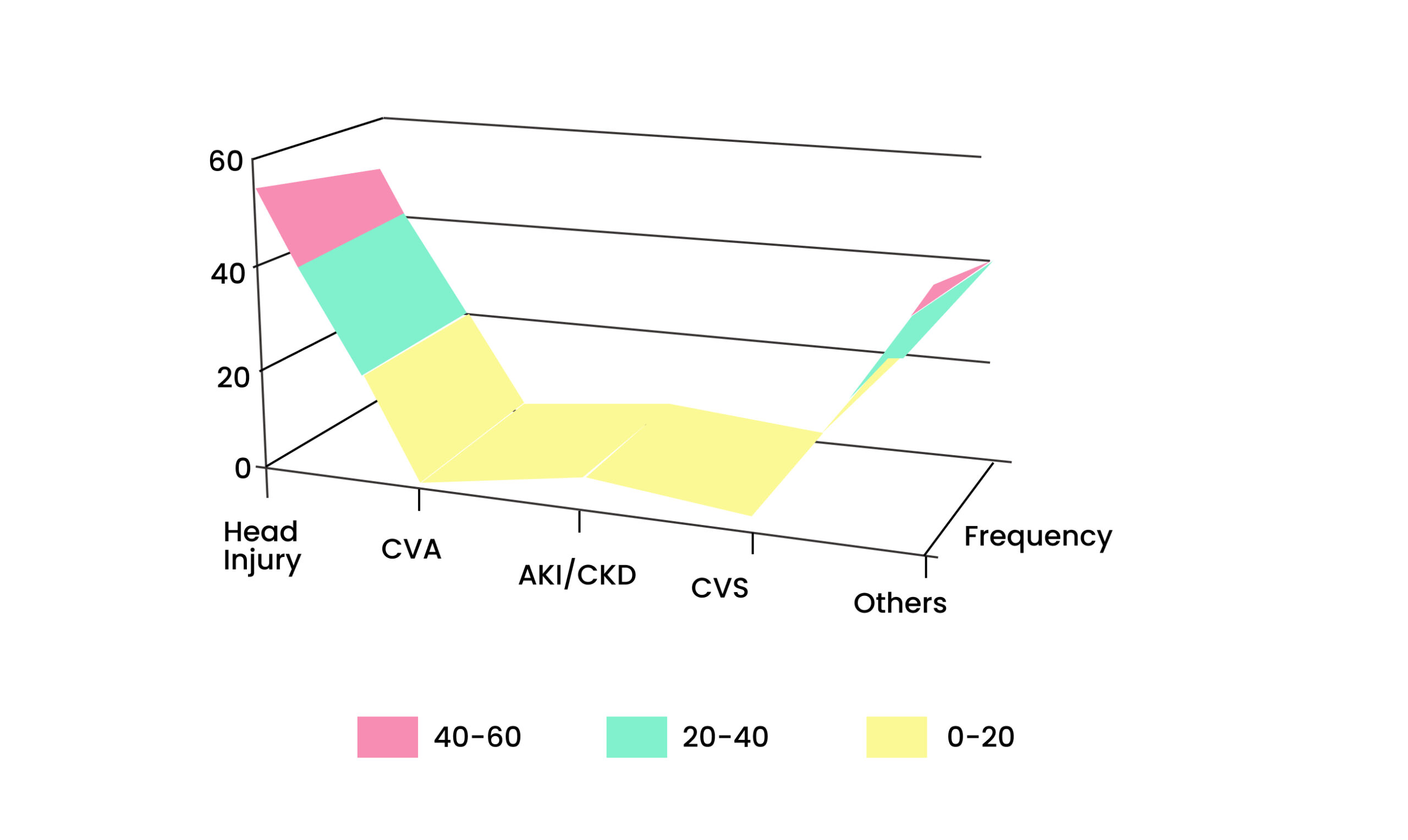
Figure 3: Distribution by admitting diagnosis
Traumatic brain injury was the commonest admitting diagnosis (48.7%). 17 patients out of 113 patients recruited developed pressure ulcers.
Incidence: 113 patients were recruited and followed up between July 10th and October 9th, 2021. Of these patients, 17 patients developed pressure ulcers, giving an incidence of 15%.
| Frequency(n=113) | Percent | |
| Yes | 17 | 15.0 |
| No | 96 | 85.0 |
Table 2: Incidence of Pressure ulcers
Date of occurrence: The onset of pressure ulcer development occurred within a mean±SD of 8.8±3.3 days after admission to the critical care unit. The minimum was 3 days, and the maximum was 16 days.
| Date of Occurance | Frequency(n=17) | Percentage(100%) |
| ≤5 days | 2 | 11.8 |
| 6 – 10 days | 10 | 58.8 |
| >10 days | 5 | 29.4 |
Table 3: Patient distribution according to the date of occurrence
Location of pressure ulcers: Most pressure ulcers developed in the gluteal region (70.6%), followed by the back of the thigh (17.6%).
| Site | Frequency(n=17) | Percent |
| Hip | 1 | 5.9 |
| Gluteal region | 12 | 70.6 |
| Back of the tigh | 3 | 17.6 |
| Occipital | 1 | 5.9 |
Table 4: Distribution by anatomical sites
Progression of pressure ulcers to the most severe stage: Of the 17 patients who had pressure ulcers (Stage I), 4 patients (23.5%) progressed to a Stage II ulcer during their stay in the unit.
Duration of mechanical ventilation (MV), length of stay in the unit, and sedation: Each unit increase in duration of mechanical ventilation increased the odds of developing pressure ulcers by 3 times, and this was statistically significant (p=0.001). We observed that each unit increase in the length of stay in the unit increased the odds of developing a pressure ulcer by 1.9 times, and this was statistically significant. We also found that the odds of developing pressure ulcer increased with increasing sedation time, and the results revealed a statistically significant difference between those not sedated, who were the reference point, and those patients who had sedation time greater than 72 hours (OR=14.0, CI 2.63 – 74.59, p=0.002).
| Pressure ulcer | ||||
| Yes(n=17) | No(n=9 6) | OR (95% CI) | p- value | |
| MV, Days mean±SD |
10.2±2.9 | 3.8±2.0 | 3.06 (1.54 – 6.10) | 0.001 |
| LOS, Days mean±SD |
14.7±5.6 | 4.5±2.4 | 1.91 (1.38–2.65) | <0.001 |
| Sedation | ||||
| Not | 3 (17.6) | 35 (36.5) | ||
| Sedated | 1 (5.9) | 19 (19.8) | 0.61 (0.06-6.32) | 0.682 |
| <48 hours | 7 (41.2) | 37 (38.5) | 2.21 (0.53-9.22) | 0.278 |
| 48 – 72 hours | 6 (35.3) | 5 (5.2) | 14.00 (2.63-74.59) | 0.002 |
Table 5: Duration of MV, length of stay in the unit, and sedation
Discussion
This study aimed at identifying the incidence rate and potential risk factors of pressure ulcers among critical patients at Kenyatta national hospital. The present study exhibits that the incidence of pressure ulcers at Kenyatta national hospital was 15%, and the gluteal region was found to be the commonest location. This is in keeping with the study done by Mutabazi G. et al, which revealed that the incidence of pressure ulcer in the large critical care unit at the referral hospital of Kigali was 15%. They also found that the commonest location for pressure ulcers was the buttocks, and Stage 2 was the most common severity for pressure ulcers.[11] However, other studies quoted a higher incidence rate with Tayyib N et al, who demonstrated that up to 40 % of patients develop pressure ulcers during their admission to the intensive care unit.[7]
There was no significant association between age and the development of pressure ulcers (p-value=0.509). This contrasts with the study carried out by Tayyib N et al that revealed that increased age independently predicted the development of pressure ulcers. Males are more prone to develop pressure ulcers than females. However, this was not statistically significant. Our findings are supported by other studies that showed a higher incidence of pressure ulcers in men admitted to the critical care unit.[12-19]. This study contrasts with findings by Lindgren M., et al, that demonstrated that more women than men developed pressure ulcers, and female gender was one of those risk factors identified in multiple stepwise regression analyses.[20] There was a significant association between each unit of increase in the duration of mechanical ventilation and the development of pressure ulcers. This study is similar to the study done in Saudi Arabia by Tayyib N et al. that found that prolonged mechanical ventilation was an independent risk factor for pressure ulcer development.[7,21,23] Our findings were also similar to the study by Celia et al, which revealed that the presence of organ failure and the duration of mechanical ventilation were significantly associated with the development of pressure ulcers.
The length of stay in the unit was significantly associated with pressure ulcer development. Each unit increase in the length of stay in the unit increases the odds of developing pressure ulcers by 1.9 times. This finding is supported by the study conducted in Sweden by L. Gunningberg, et al, which revealed that more days of hospitalization were significantly associated with pressure ulcers. These findings can be explained by suggesting that most critical care unit patients stay for long periods in the hospital, and little attention is given to their turning schedule and nutrition, thus increasing pressure on the small points and decreasing perfusion to these sites.[24,25]
Conclusion
The incidence of pressure ulcers was 15%, and all of them were stage I. The most common location of ulcers was the gluteal region. Mechanical ventilation, Length Of stay in the unit, and increasing sedation time were found to be independent risk factors for pressure ulcer development.
References
- Bauer K, Rock K, Nazzal M, Jones O, Qu W. Pressure ulcers in the United States’ inpatient population from 2008 to 2012: results of a retrospective nationwide study. Ostomy Wound Manage. 2016;62(11):30-38.
Pressure ulcers in the United States’ inpatient population from 2008 to 2012: results of a retrospective nationwide study - Coyer F, Miles S, Gosley S, et al. Pressure injury prevalence in intensive care versus non-intensive care patients: a state-wide comparison. Aust Crit Care. 2017;30(5):244-250. doi:10.1016/j.aucc.2016.12.003
PubMed | Crossref | Google Scholar - Afzali Borojeny L, Albatineh AN, Hasanpour Dehkordi A, Ghanei Gheshlagh R. The incidence of pressure ulcers and its associations in different wards of the hospital: a systematic review and meta-analysis. Int J Prev Med. 2020;11:171. doi:10.4103/ijpvm.IJPVM_182_19 PubMed | Crossref | Google Scholar
- Lim ML, Yuh A. Impact of hospital-acquired pressure injuries on hospital costs – experience of a tertiary hospital in Singapore. Wound Pract Res. 2017;25(1):42-47.
Impact of hospital-acquired pressure injuries on hospital costs – experience of a tertiary hospital in Singapore - Skerritt L, Moore Z. The prevalence, aetiology and management of wounds in a community care area in Ireland. Br J Community Nurs. 2014;Suppl:S11-S17. doi:10.12968/bjcn.2014.19.sup6.s11 PubMed | Crossref | Google Scholar
- Shahin ESM, Dassen T, Halfens RJG. Incidence, prevention and treatment of pressure ulcers in intensive care patients: a longitudinal study. Int J Nurs Stud. 2009;46(4):413-421. doi:10.1016/j.ijnurstu.2008.02.011
PubMed | Crossref | Google Scholar - Tayyib N, Coyer F, Lewis P. Saudi Arabian adult intensive care unit pressure ulcer incidence and risk factors: a prospective cohort study. Int Wound J. 2016;13(5):912-919. doi:10.1111/iwj.12406 PubMed | Crossref | Google Scholar
- Terekeci H, Kucukardali Y, Top C, et al. Risk assessment study of the pressure ulcers in intensive care unit patients. Eur J Intern Med. 2009;20(4):394-397. doi:10.1016/j.ejim.2008.11.001 PubMed | Crossref | Google Scholar
- Hortig A, et al. Pressure ulcer predictors in ICU patients: nursing skin assessment versus objective parameters. J Wound Care. 2008;17(10):417-424. doi:10.12968/jowc.2008.17.10.31304 PubMed | Crossref | Google Scholar
- Nijs N, Toppets A, Defloor T, Bernaerts K, Milisen K, Van Den Berghe G. Incidence and risk factors for pressure ulcers in the intensive care unit. J Clin Nurs. 2009;18(9):1258-1266. doi:10.1111/j.1365-2702.2008.02554.x
PubMed | Crossref | Google Scholar - Mutabazi G, Silver J. Notes from the field: establishing baseline data for pressure ulcers in a Rwandan intensive care unit. Rwanda J Ser F Med Health Sci. 2015;2(2). doi:10.4314/rj.v2i2.50F Crossref | Google Scholar
- He M, Tang A, Ge X, Zheng J. Pressure ulcers in the intensive care unit: an analysis of skin barrier risk factors. Adv Skin Wound Care. 2016;29(11):493-498. doi:10.1097/01.ASW.0000494779.66288.c9 PubMed | Crossref | Google Scholar
- Labeau SO, Afonso E, Benbenishty J, et al. Prevalence, associated factors and outcomes of pressure injuries in adult intensive care unit patients: the DecubICUs study. Intensive Care Med. 2021;47(2):160-169. doi:10.1007/s00134-020-06234-9 PubMed | Crossref
- Afzali Borojeny L, Albatineh AN, Hasanpour Dehkordi A, Ghanei Gheshlagh R. The incidence of pressure ulcers and its associations in different wards of the hospital: a systematic review and meta-analysis. Int J Prev Med. 2020;11:171. doi:10.4103/ijpvm.IJPVM_182_19 PubMed | Crossref | Google Scholar
- Goodall R, Armstrong A, Hughes W, et al. Trends in decubitus ulcer disease burden in European Union 15+ countries, from 1990 to 2017. Plast Reconstr Surg Glob Open. 2020;8(11):e3252. doi:10.1097/GOX.0000000000003252
PubMed | Crossref | Google Scholar - Karimkhani C, Dellavalle RP, Coffeng LE, et al. Global skin disease morbidity and mortality: an update from the Global Burden of Disease Study 2013. JAMA Dermatol. 2017;153(5):406-412. doi:10.1001/jamadermatol.2016.5538
PubMed | Crossref | Google Scholar - Global Burden of Disease Study 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386(9995):743-800. doi:10.1016/S0140-6736(15)60692-4 PubMed | Crossref
- Lichterfeld-Kottner A, Lahmann N, Kottner J. Sex-specific differences in prevention and treatment of institutional-acquired pressure ulcers in hospitals and nursing homes. J Tissue Viability. 2020;29(3):204-210. doi:10.1016/j.jtv.2020.05.001 PubMed | Crossref | Google Scholar
- Raeder K, Jachan DE, Müller-Werdan U, Lahmann NA. Prevalence and risk factors of chronic wounds in nursing homes in Germany: a cross-sectional study. Int Wound J. 2020;17(5):1128-1134. doi:10.1111/iwj.13486
PubMed | Crossref | Google Scholar - Lindgren M, Unosson M, Krantz A-M, Ek A-C. Pressure ulcer risk factors in patients undergoing surgery. Nurs Stand. 2005;50(6):605-612. doi:10.1111/j.1365-2648.2005.03441.x PubMed | Crossref | Google Scholar
- Loudet CI, Marchena MC, Maradeo MR, et al. Reducing pressure ulcers in patients with prolonged acute mechanical ventilation: a quasi-experimental study. Rev Bras Ter Intensiva. 2017;29(1):39-46. doi:10.5935/0103-507X.20170007 PubMed | Crossref | Google Scholar
- Manzano F, Navarro MJ, Roldán D, et al. Pressure ulcer incidence and risk factors in ventilated intensive care patients. J Crit Care. 2010;25(3):469-476. doi:10.1016/j.jcrc.2009.09.002 PubMed | Crossref | Google Scholar
- Nijs N, Toppets A, Defloor T, Bernaerts K, Milisen K, Van Den Berghe G. Incidence and risk factors for pressure ulcers in the intensive care unit. J Clin Nurs. 2009;18(9):1258-1266. doi:10.1111/j.1365-2702.2008.02554.x
PubMed | Crossref | Google Scholar - Bergstrom N, Braden B. A prospective study of pressure sore risk among institutionalized elderly. J Am Geriatr Soc. 1992;40(8):747-758. doi:10.1111/j.1532-5415.1992.tb01845.x PubMed | Crossref | Google Scholar
- Digesa LE, Baru A, Shanko A, et al. Incidence and predictors of pressure ulcers among adult patients in intensive care units at Arba Minch and Jinka hospitals, Southern Ethiopia. Biomed Res Int. 2023;2023:9361075. doi:10.1155/2023/9361075 PubMed | Crossref | Google Scholar
Acknowledgments
Not reported
Funding
Financial support by Kenyatta National Hospital, Hospital in Nairobi, Kenya.
Author Information
Franck N. Nguvulu
Department of Anesthesia
University of Nairobi, University President Joseph Kasa Vubu, Democratic Republic of the Congo
Email: [email protected]
Author Contribution
The author contributed to the conceptualization, investigation, and data curation by acquiring and critically reviewing the selected articles and was involved in the writing – original draft preparation and writing – review & editing to refine the manuscript.
Ethical Approval
This study has been approved by the Kenyatta National Hospital, University of Nairobi ethics and research committee (P27/04/2021).
Conflict of Interest Statement
The authors declare no conflict of interest.
Guarantor
None
DOI
Cite this Article
Franck NN. Incidence and Risk Factors of Pressure Ulcer Among Critically Ill Patients at Kenyatta National Hospital- Main Critical Care Unit. medtigo J Anesth Pain Med. 2025;1(1):e3067111. doi:10.63096/medtigo3067111 Crossref













