







 Author Affiliations
Author Affiliations
Abstract
Background: Pressure ulcers are a common health problem and are considered a burden on the health care system. They manifest negative impacts on patients, such as creating discomfort, pain, prolonged hospital stays, and sometimes additional treatment such as wound debridement and daily wound dressing.
Aim: Identify the risk and associated factors of pressure ulcer development among hospitalized surgical and medical patients in Civil Hospital and Ziauddin Hospital Karachi, Pakistan.
Methodology: A cross-sectional descriptive study was conducted over one year, involving 454 hospitalized patients from neurosurgery, neuro-medicine, and orthopedic departments. Data were collected using a structured questionnaire covering demographics, special protocols, preventive devices, remedies, and Braden and Norton scales. Statistical Package for the Social Sciences (SPSS) version 22.0 was used for data analysis.
Results: The study found that Improved sensory perception, nutrition, physical, and mental conditions significantly reduced pressure ulcer risk, with sensory perception being most protective in neurosurgery (Odds ratio (OR)=0.213). Moisture, friction, and incontinence were not significantly associated. Males had a 1.41 times higher risk than females. Risk increased with age (OR=1.225), longer hospital stays (OR=1.552), and higher body mass index (BMI, marginally significant, OR=1.042). Special protocols showed a protective trend (OR=0.783) but were not statistically significant.
Conclusion: This study found that key risk factors for pressure ulcer development included impaired sensory perception, mobility, activity, poor nutrition, and compromised physical and mental health. Moisture and incontinence were not significant. Gender, age, BMI, special protocols, and hospital stay length were associated factors.
Keywords
Pressure ulcer, Risk factors, Associated factors, Patient, Nurse, Nursing Care.
Introduction
Pressure ulcers, interchangeably referred to as decubitus ulcers or bedsores, are one of the most serious health concerns occurring in the world.[1] Patients who are hospitalized are vulnerable to it, and even non-hospitalized patients are not free of it. They are caused by long-term pressure on the skin, particularly over bony prominences, which leads to a lack of normal blood flow to tissues, ischemia, tissue necrosis, and ulceration.[2,3] In spite of all the improvements that healthcare and clinical practices have experienced over time, pressure ulcers remain a major source of physical, psychological, and economic pressures on both the patients and healthcare systems. Their development is multi-factorial, with both intrinsic patient conditions and extrinsic environmental factors.[4,5]
The formation of pressure ulcers derives its pathophysiology from unrelieved pressure being greater than the capillary pressure, thus resulting in tissue hypoxia and cell death. Lack of mobility, Sensory impairment, Friction, Shear, and Moisture play a significant role in increasing the risk of ulceration. Patients bedridden or in wheelchairs for a long time are especially susceptible.[5-7] The research also states that even pressure of 150 mm Hg, if exerted over a long period, can cause ulceration, particularly in places such as the sacrum, heels, and trochanters where subcutaneous tissues are minimal.[8]
Clinically, pressure ulcers are staged from Stage I (non-blanchable rash) to Stage IV (full-thickness tissue loss with exposed bone/muscle) and up to unstageable ulcers and deep tissue injury. The classification is useful to guide the treatment and resource allocation. Early identification and management are critical because the progression from early to severe stages costs more, and their treatment is difficult.[9,10]
Pressure ulcers’ development is associated with a spectrum of risk and associated factors. Some risk factors having established relationships with ulcer development are immobility, incontinence, malnutrition, low serum albumin, impaired mental status, and comorbidities including diabetes and cardiovascular disease.[11,12] Factors related to it indirectly enhance the propensity for ulcerations and consist of age, gender, BMI, duration of hospitalization, and operations. Interestingly, the elderly and the long surgical patients are at increased risk as well; patients in units of intensive care or orthopedic and neurosurgical interventions are also at high risk.[13]
Rates for prevalence and incidence of pressure ulcers show great disparity throughout the world, but appear shockingly high in both developed and developing nations. European countries report prevalence rates of 15–20% among hospitalized patients, and in the intensive care unit (ICU), this rate may be up to 42%.[14] In these surgical patients, prevalence may run 8.5% or higher, and spinal cord injury patients may demonstrate 50% or higher in some regions. The incidence rate also brings out the magnitude of the problem, as some research shows up to 39.8% of admitted patients.[15,16] These figures highlight the need for efficient prevention protocols in healthcare settings.[17]
Pressure ulcers put a tremendous financial strain on healthcare systems. The cost of treatment increases with the severity of ulcers, ranging from £1,000 to more than £10,000 per case in the United Kingdom (UK).[18] In the United States, the annual treatment price tag of hospital-acquired pressure ulcers exceeds $11 billion, with over 60,000 deaths occurring year in and year out from complications of pressure ulcers. Economic implications include direct medical expenses apart from indirect loss of time for nurses extending patient stays, lost productivity for patients, and their caregivers.[19-21]
Pressure ulcers are an increasing yet under-researched health problem in Pakistan. Studies are also limited in number, and the available data are region or patient-group-specific, such as spinal cord injury patients.[22] An example of one such study, where you find a 33% prevalence rate, was found in earthquake-affected spinal injury patients.[23] This lower rate was attributed to improved protocols, including physiotherapy. However, the limited national data and lack of standardized practices suggest that urgent action is needed in terms of greater surveillance, education, and policy interventions to minimize and prevent pressure ulcers in the health care system of Pakistan.[24]
To summarize, pressure ulcers are an important issue in health care because of their high prevalence rate, preventable character, and strong effects upon patient outcomes and health care expenditures.[25] Although risk and related factors are extensively documented, this leads to standardized prevention and care practices that continue to vary, especially in low/middle-income countries. Solving this problem would require a multidisciplinary approach, such as early detection and identification, patient education with staff training, as well as changes in health care policies that will make pressure ulcer prevention and management a priority in all levels of care.
Methodology
This research used a descriptive cross-sectional quantitative research design to determine the risk and associated factors of pressure ulcer development in hospitalized patients who have had cerebrovascular accidents (CVA), neurosurgical conditions, and orthopedic issues. Cross-sectional designs are often utilized in nursing research to evaluate a variable at a single time point, and it was suitable for the purpose of describing the status of risk for pressure ulcers in the selected population of patients. The study population included patients admitted to two tertiary care hospitals in Karachi with neurosurgery, neuro-medicine, and orthopedic illness. Civil Hospital Karachi (public hospital) and Ziauddin Hospital (private hospital campuses in Kamari and North Nazimabad). These hospitals have many patients and more than 1700 beds and 30 departments, making them the right place to get a diverse and representative sample. From these hospitals, participant patients were selected by a probability-based simple random sampling technique of the lottery method, which gave all the eligible participants an equal probability of selection. The selected sampling approach improves the reliability and generalizability of results. This stratum of patients was identified primarily because of high vulnerability to pressure ulceration due to immobility, prolonged bed rest, and nutritional deficit. Scientific adequacy was maintained by calculating the size of the sample based on a regular scheme by considering precision, reliability, and feasibility. The final sample incorporated patients from the public and private sectors to reflect on variations in care practice and patient profile. Such a methodological approach assured that the collected data reflected precisely the risk factors predisposing to the development of pressure ulcers in the Karachi tertiary care hospital setting.
Data collection procedure: Ethical approval was obtained from the institutional review board (IRB) Ziauddin Hospital Ref No IRB/ZH/ 23/12. In this study, primary and secondary data were collected to study the risk and associated factors in pressure ulcer development. Primary data was obtained using a structured questionnaire completed by the researcher during visits in selected hospitals. The questionnaire had two parts: Underutilization of skin assessments using demographic information and hospital protocols, and the Braden and Norton scales to evaluate patient risk factors. These scales used a 3- to 4-point scoring system to measure such things as sensory perception, mobility, nutrition, moisture, activity, and incontinence. Lower scores indicated greater risk for the development of pressure ulcers. The consistency of the scale was proven with an overall Cronbach’s α of 0.73 and individual scale items between 0.68 and 0.82. The data input was using SPSS version 22, whereby each response entered had a numerical code for checking purposes. Coding and tabulation were subsequently undertaken to obtain the descriptive and inferential statistical analysis. Descriptive data using frequencies, percentages, and means were summarized, and analytical interpretation using logistic regression was carried out.
Data analysis procedure: The data analysis process started with the review of the collected questionnaires with the aim of cleaning them up to ensure accuracy and completeness. All data were entered using a pre-defined coding system into SPSS version 22. A summary of the demographic and clinical characteristics was done using descriptive statistics such as frequency, percentage, and mean. Data on Braden and Norton scale scores were analyzed to determine risk levels for the development of pressure ulcers. The inferential statistics were used to test associations between variables. Correlation analysis was used to explore relations between risk and associated factors. Binary logistic regression was carried out to identify major predictors of pressure ulcer development. The p-value of 0.01 was used as an indicator of statistical significance. The strength of associations was identified using odds ratios. The results were carefully analyzed to guarantee valid conclusions in accordance with the objectives of the study.
Results
Demographic characteristics of patients: There were 454 patients participating in the study, with a nearly equal distribution of both genders: half of them male, 50.7%, and half of them female, 49.3%. Distributions of most patients were between 41 and 70 years old, and the highest proportion (23.1%) was in the group 41-50 years. Diagnosis was fairly distributed to various disciplines, neuro-medicine 32.4%, orthopedic surgery 37.2%, and neurosurgery 30.4%. Only 1.1% required repeat admission. Half of the patients had a normal BMI, and 44.5% of the patients had hospital stays between 6 and 10 days (Table 1).
| Variable | Category | Frequency (n) | Percentage (%) |
| Gender | Male | 230 | 50.7 |
| Female | 224 | 49.3 | |
| Age group | Up to 20 years | 17 | 3.7 |
| 21–30 | 42 | 9.3 | |
| 31–40 | 61 | 13.4 | |
| 41–50 | 105 | 23.1 | |
| 51–60 | 89 | 19.6 | |
| 61–70 | 102 | 22.5 | |
| 71 and above | 38 | 8.4 | |
| Diagnosis | Neuro-Medicine (CVA) | 147 | 32.4 |
| Orthopedic surgery | 169 | 37.2 | |
| Neurosurgery | 138 | 30.4 | |
| Repeat admission | Yes | 5 | 1.1 |
| No | 449 | 98.9 | |
| BMI category | Underweight | 21 | 4.6 |
| Normal weight | 227 | 50.0 | |
| Pre-Obesity | 140 | 30.8 | |
| Obesity class I | 58 | 12.8 | |
| Obesity class II | 8 | 1.8 | |
| Length of hospital stay | Less than 5 days | 180 | 39.6 |
| 6–10 days | 202 | 44.5 | |
| 11–15 days | 60 | 13.2 | |
| 16–20 days | 2 | 0.4 | |
| 21–25 days | 9 | 2.0 | |
| 26 days and above | 1 | 0.2 |
Table 1: Demographic characteristics of patients
The majority of participants were between the ages of 41 and 70 years, with the highest number (105) in the 41–50 age group. Fewer participants were in the youngest (17) and oldest (38) age categories (Figure 1).
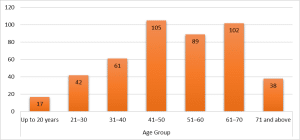
Figure 1: Age of participants
Risk categories based on Braden scale and Norton scale: The distribution of patients’ risk levels as reflected by the use of the Braden and Norton scales. The Braden scale indicates that a larger number of patients are at risk in a mild stage, while the Norton scale categorizes most of them as being of medium risk. Both scales bring to the fore the different levels of risk, with a couple of patients emerging as having severe or very high risk (Table 2).
| Risk category | Braden scale frequency | Braden scale percentage | Braden scale cumulative percentage | Norton scale frequency | Norton scale percentage | Norton scale cumulative percentage |
| Severe risk | 5 | 1.1% | 1.1% | 10 | 2.2% | 2.2% |
| High risk | 46 | 10.1% | 11.2% | 55 | 12.1% | 14.3% |
| Moderate risk | 91 | 20.0% | 31.3% | 274 | 60.4% | 74.7% |
| Mild risk | 312 | 68.7% | 100% | 115 | 25.3% | 100% |
| Total | 454 | 100% | 454 | 100% |
Table 2: Risk categories based on the Braden scale and Norton scale
Binary logistic regression analysis: The odds ratios of various risk factors associated with the development of pressure ulcers were analyzed. Sensory perception, mobility, activity, nutrition, friction, shear, physical condition, and mental condition all showed statistically significant associations with pressure ulcer risk (p < 0.05), indicating strong correlations. In contrast, moisture and incontinence did not have a statistically significant effect (p > 0.05).
| Risk Factors | Coefficient | Odds ratio | 95% Confidence interval (CI) | p-value | |
| Lower | Upper | ||||
| Sensory perception | -1.029 | 0.357 | 0.258 | 0.495 | 0.000 |
| Moisture | -0.400 | 0.671 | 0.412 | 1.092 | 0.108 |
| Mobility | -0.936 | 0.392 | 0.284 | 0.542 | 0.000 |
| Activity | -1.344 | 0.261 | 0.186 | 0.365 | 0.000 |
| Nutrition | -1.384 | 0.251 | 0.163 | 0.385 | 0.000 |
| Fractions and shear | -1.247 | 0.287 | 0.199 | 0.415 | 0.000 |
| Physical condition | -1.474 | 0.229 | 0.143 | 0.368 | 0.000 |
| Mental condition | -1.766 | 0.171 | 0.101 | 0.289 | 0.000 |
| Incontinence | -0.269 | 0.764 | 0.489 | 1.195 | 0.238 |
Table 3: Binary logistic regression analysis
Discussion
This study was intended to determine the risk and related factors for pressure ulcer development in hospitalized neuro-medicine, neurosurgery, and orthopedic patients. The outcomes of the research demonstrated that there were some risk factors which were statistically associated with the development of pressure ulcers (sensory perception, mobility, activity, nutrition, physical condition, mental condition), with some others being statistically not significant (moisture, incontinence). A study confirmed that sensory perception, the ability to move, and physical condition are among the main risk factors.[26]
Sensory perception became an important risk factor in this study; a reduction of sensory perception led to an increased risk of pressure ulcers in all three patient categories. An odds ratio of 0.357 for sensory perception was used to show that better sensory perception greatly reduces the risk of pressure ulcers. The association was also strongest among neurosurgery and orthopedic patients, in line with results from earlier research.[27] This underscores the need for routine sensory assessment to prevent pressure ulcers for these high-risk patient categories.
Mobility was also another significant risk factor, as evidenced in this research. The increased immobility raised the likelihood of pressure ulcers, which correlates with the results of other recent literature, where immobility is reported to be a key predictor of hospital-acquired pressure ulcers.[28] It was observed that increased mobility greatly decreased the chance of developing pressure ulcers. Orthopedic patients had most of the results (odds ratio = 0.321, p-value = 0.000). These findings justify the requirement for mobilization strategies in hospitalized patients to reduce the risk of pressure sores.[29]
The activity level was considered another protective factor in preventing pressure ulcer development. The study showed that patients who are more active are less likely to develop pressure ulcers (Odds ratio = 0.261, p-value = 0.000). This finding agrees with other research, which indicates that physical activity aids pressure redistribution, minimizing prolonged contact with bony prominences.[30] The findings have highlighted the need to promote as much activity as possible while patients are in the hospital, especially for neurosurgery and orthopedic departments.
Nutrition was also another essential factor linked to the pressure ulcer development issue. The better the nutritional status, the less likely pressure ulcer formation was to occur significantly (Odds ratio = 0.251, p-value = 0.000). This finding is consistent with previously published findings that indicated the importance of nutrition in the process of healing wounds and the prevention of pressure ulcers.[31] Nutritional interventions such as adequate protein intake should be given priority in managing patients who are highly at risk of pressure ulcers, which include neurology, neurosurgery, and orthopedics settings.[32]
Physical and mental conditions of the patients were also of great importance in preventing pressure ulcer development. Patients with superior physical (Odds ratio = 0.299, p-value = 0.000) and mental conditions (Odds ratio = 0.171, p-value = 0.000), according to the study, had a significantly reduced risk of getting pressure ulcers. Previous literature has continuously determined that physical and mental health are important components of patient care, influencing pressure ulcer outcomes.[33] These outcomes underline the effectiveness of a holistic approach to care that focuses not only on the physical but also on the psychological well-being of patients at risk for pressure ulcers.
Apart from clinical risk factors, demographic and hospital-related factors were also investigated in this study. The independent variables age, gender, BMI, special protocol, and length of hospital stay were associated with pressure ulcer development. The study found that male patients, advanced age, and high BMI were all associated with the development of signs, which agrees with previous studies that have identified gender, age, and BMI as important risk factors for pressure ulcers.[31] In addition, it was observed that the duration of hospital stays increased the probabilities of developing pressure ulcers, something that highlights the need for careful monitoring and pressure ulcer prevention measures among those patients who spend a long time in the hospital.[32]
Interestingly, moisture, friction, shear, and incontinence were identified in this study as not having statistically significant associations with pressure ulcer development. These results are consistent with some of the past research, indicating that moisture and friction do not always predict pressure ulcers.[31] Even though these factors have been indicated in some investigators as probable risk factors for pressure ulcers, the insignificant findings in this case imply that the relationship between these factors and pressure ulcer occurrence may vary from clinical setting to clinical setting and patient population to patient population.
Recommendations: It is recommended that nurses use assessment scales at the time of patient admission to identify individuals at high, moderate, or low risk of developing pressure ulcers. This information should serve as a baseline for implementing preventive interventions. Nutritional screening should be conducted for elderly patients to guide appropriate nutritional planning. Nurses should also assess mobility, physical, and mental conditions—particularly in neuro-medicine, neurosurgery, and orthopedic patients—to encourage movement and support overall well-being. Additionally, the availability of preventive devices should be increased for high-risk patients.
Management and policymakers are advised to perform pressure ulcer risk assessments within 24 hours of admission and to conduct regular surveillance of elderly, immobile, and malnourished patients. Postnatal care (PNC) services should introduce specialized training for primary care providers (PCP) handling, review caretaker-to-patient ratios, and advocate for increased staffing of nurses and nurse assistants to enhance preventive care. Further research should aim to replicate these findings in other settings and populations, particularly regarding preventive devices, remedies, and special protocols, and explore interventional approaches in ethnically diverse groups.
Conclusion
These findings indicate the critical role of sensory perception, mobility, activity, nutrition, physical condition, and mental condition in developing pressure ulcers in hospitalized neuro-medicine, neurosurgery, and orthopedic patients. It underscores the necessity of prevention measures targeted at individual benefits, such as repeated sensory assessments, improved mobility programs, and nutritional balance. Although moisture, friction, shear, and incontinence were not found to be significant in this study, it is also important to note that demographic factors (such as age, gender, and BMI) are also significantly important in pressure ulcer development. Future research should have a specific goal of investigating the intricate relationships between these factors and their effects on pressure ulcer prevention.
References
- Kottner J, Cuddigan J, Carville K, et al. Pressure ulcer/injury classification today: An international perspective. J Tissue Viability. 2020;29(3):197-203. doi:10.1016/j.jtv.2020.04.003 PubMed | Crossref | Google Scholar
- Zhang X, Zhu N, Li Z, Xie X, Liu T, Ouyang G. The global burden of decubitus ulcers from 1990 to 2019. Sci Rep. 2021;11(1):21750. doi:10.1038/s41598-021-01188-4 PubMed | Crossref | Google Scholar
- Gefen A, Brienza DM, Cuddigan J, Haesler E, Kottner J. Our contemporary understanding of the aetiology of pressure ulcers/pressure injuries. Int Wound J. 2022;19(3):692-704. doi:10.1111/iwj.13667 PubMed | Crossref | Google Scholar
- McEvoy N, Avsar P, Patton D, Curley G, Kearney CJ, Moore Z. The economic impact of pressure ulcers among patients in intensive care units. A systematic review. J Tissue Viability. 2021;30(2):168-177. doi:10.1016/j.jtv.2020.12.004 PubMed | Crossref | Google Scholar
- Crawford A, Harris H. Caring for adults with impaired physical mobility. Nursing. 2016;46(12):36-41. doi:10.1097/01.NURSE.0000504674.19099.1d PubMed | Crossref | Google Scholar
- Prakash AC, Prakash A. Prevention and management of pressure ulcer in neurosurgical wards at RIMS: A single centre experience. IOSR J Dent Med Sci. 2019;18:59-66. doi:10.9790/0853-1802075966 Crossref | Google Scholar
- Kinoro H. Prevention of Pressure Ulcers among the Elderly: Systematic Literature Review. Degree thesis. Yrkeshögskolan Novia; 2023. Prevention of Pressure Ulcers Among the Elderly: Systematic Literature Review
- Nguvulu FN. Incidence and Risk Factors of Pressure Ulcer Among Critically Ill Patients at Kenyatta National Hospital. Master’s thesis. University of Nairobi; 2022. Incidence and Risk Factors of Pressure Ulcer Among Critically Ill Patients at Kenyatta National Hospital
- Elam R, Doan J, Weaver F, et al. “Pathological” fractures in spinal cord injuries and disorders: Insight into International classification of diseases, ninth revision coding. J Spinal Cord Med. 2023;46(2):317-325. doi:10.1080/10790268.2022.2042658 PubMed | Crossref | Google Scholar
- Stefanopoulos S, Qiu Q, Alshaibani K, et al. Evaluation of Current Pressure Ulcer Staging. Am Surg. 2023;89(4):665-670. doi:10.1177/00031348211038574 PubMed | Crossref | Google Scholar
- Idris M, Smiley A, Patel S, Latifi R. Risk Factors for Mortality in Emergently Admitted Patients with Acute Gastric Ulcer: An Analysis of 15,538 Patients in National Inpatient Sample, 2005-2014. Int J Environ Res Public Health. 2022;19(23):16263. doi:10.3390/ijerph192316263 PubMed | Crossref | Google Scholar
- Avishai E, Yeghiazaryan K, Golubnitschaja O. Impaired wound healing: facts and hypotheses for multi-professional considerations in predictive, preventive and personalised medicine. EPMA J. 2017;8(1):23-33. doi:10.1007/s13167-017-0081-y PubMed | Crossref | Google Scholar
- Markwart R, Saito H, Harder T, et al. Epidemiology and burden of sepsis acquired in hospitals and intensive care units: a systematic review and meta-analysis. Intensive Care Med. 2020;46(8):1536-1551. doi:10.1007/s00134-020-06106-2 PubMed | Crossref | Google Scholar
- World Health Organization. Global Report on the epidemiology and burden on sepsis: current evidence, identifying gaps and future directions. 2020. Global report on the epidemiology and burden of sepsis
- Rabee H, Tanbour R, Nazzal Z, et al. Epidemiology of sepsis syndrome among intensive care unit patients at a tertiary university hospital in Palestine in 2019. Indian J Crit Care Med. 2020;24(7):551-556. doi:10.5005/jp-journals-10071-23474 PubMed | Crossref | Google Scholar
- Guest JF, Vowden K, Vowden P. The health economic burden that acute and chronic wounds impose on an average clinical commissioning group/health board in the UK. J Wound Care. 2017;26(6):292-303. doi:10.12968/jowc.2017.26.6.292 PubMed | Crossref | Google Scholar
- Phillips CJ, Humphreys I, Thayer D, et al. Cost of managing patients with venous leg ulcers. Int Wound J. 2020;17(4):1074-1082. doi:10.1111/iwj.13366 PubMed | Crossref | Google Scholar
- Mearns ES, Liang M, Limone BL, et al. Economic analysis and budget impact of clostridial collagenase ointment compared with medicinal honey for treatment of pressure ulcers in the US. Clinicoecon Outcomes Res. 2017;9:485-494. doi:10.2147/CEOR.S133847 PubMed | Crossref | Google Scholar
- Oozageer Gunowa N, Hutchinson M, Brooke J, Jackson D. Pressure injuries in people with darker skin tones: A literature review. J Clin Nurs. 2018;27(17-18):3266-3275. doi:10.1111/jocn.14062 PubMed | Crossref | Google Scholar
- Chauhan A, Walton M, Manias E, et al. The safety of health care for ethnic minority patients: a systematic review. Int J Equity Health. 2020;19(1):118. doi:10.1186/s12939-020-01223-2 PubMed | Crossref | Google Scholar
- Togo C, Zidorio AP, Gonçalves V, Botelho P, de Carvalho K, Dutra E. Does Probiotic Consumption Enhance Wound Healing? A Systematic Review. Nutrients. 2021;14(1):111. doi:10.3390/nu14010111 PubMed | Crossref | Google Scholar
- Muhammad D. Knowledge, attitude and practices of nurses regarding pressure ulcers prevention at a tertiary care hospital of Peshawar, Khyber Pakhtunkhwa. J Khyber Coll Dent. 2017;7(2):42–47. knowledge, attitude and practices of nurses regarding pressure ulcers prevention at a tertiary care hospital of Peshawar, Khyber Pakhtunkhwa
- Zafar M, Kashif M, Bunyad S, et al. Effectiveness of educational campaign in promoting knowledge and attitude of pressure ulcer among physical therapists working in tertiary care hospitals. J Liaquat Univ Med Health Sci. 2023;22(1):68-74. Effectiveness of educational campaign in promoting knowledge and attitude of pressure ulcer among physical therapists working in tertiary care hospitals
- Qazi M, Khattak AF, Barki MT. Pressure Ulcers in Admitted Patients at a Tertiary Care Hospital. Cureus. 2022;14(4):e24298. doi:10.7759/cureus.24298 PubMed | Crossref | Google Scholar
- Moda Vitoriano Budri A, Moore Z, Patton D, et al. Impaired mobility and pressure ulcer development in older adults: Excess movement and too little movement-Two sides of the one coin?. J Clin Nurs. 2020;29(15-16):2927-2944. doi:10.1111/jocn.15316 PubMed | Crossref | Google Scholar
- Ledger LJ, Worsley PR, Hope J, Schoonhoven L. Patient perceptions and understanding of pressure ulcer risk in the community: Empirical Research Qualitative. J Adv Nurs. 2023;79(9):3312-3323. doi:10.1111/jan.15637 PubMed | Crossref | Google Scholar
- Le Fort M, Espagnacq M, Perrouin-Verbe B, Ravaud JF. Risk Analyses of Pressure Ulcer in Tetraplegic Spinal Cord-Injured Persons: A French Long-Term Survey. Arch Phys Med Rehabil. 2017;98(9):1782-1791. doi:10.1016/j.apmr.2016.12.017 PubMed | Crossref | Google Scholar
- Yang D, Feng R, Liu L. Effect of comprehensive nursing based on evidence-based nursing on reducing the incidence of pressure ulcers in patients undergoing posterior orthopedic surgery. Medicine (Baltimore). 2023;102(38):e35100. doi:10.1097/MD.0000000000035100 PubMed | Crossref | Google Scholar
- Techanivate A, Athibai N, Siripongsaporn S, Singhatanadgige W. Risk Factors for Facial Pressure Ulcers in Patients Who Underwent Prolonged Prone Orthopedic Spine Surgery. Spine (Phila Pa 1976). 2021;46(11):744-750. doi:10.1097/BRS.0000000000003892 PubMed | Crossref | Google Scholar
- Chen B, Yang Y, Cai F, et al. Nutritional status as a predictor of the incidence of pressure injury in adults: A systematic review and meta-analysis. J Tissue Viability. 2023;32(3):339-348. doi:10.1016/j.jtv.2023.04.005 PubMed | Crossref | Google Scholar
- Workum JD, van Olffen A, Vaes PJ, van Gestel A, Vos P, Ramnarain D. The association between obesity and pressure ulcer development in critically ill patients: A prospective cohort study. Obes Res Clin Pract. 2022;16(1):56-62. doi:10.1016/j.orcp.2022.01.003 PubMed | Crossref | Google Scholar
- Beder FS, Mansour HE, Goada T, Kandeel NA. Risk factors for pressure ulcer development in medical intensive care units: an observational study. Mansoura Nurs J. 2023;10(1):309-317. doi:10.21608/mnj.2023.321870 Crossref | Google Scholar
Acknowledgments
The authors would like to express their sincere gratitude to Alia Nasir, Associate Professor and Principal, Rufayda Hamdard College of Nursing, Hamdard University Karachi, Pakistan, for his invaluable supervision, guidance, and support throughout this study.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author Information
Corresponding Author:
Aziz Ullah Shah
Department of Nursing
Bab-e-Khyber College of Nursing, Bandai, Swat, Pakistan
Email: [email protected]
Co-Authors:
Alia Nasir
Department of Nursing
Rufayda Hamdard College of Nursing, Hamdard University, Karachi, Pakistan
Anwar Ali
Department of Nursing
T&H Academy of Nursing & Allied Health Sciences, Swat, Pakistan
Shah Hussain
Department of Nursing
Zalan College of Nursing, Swat, Pakistan
Authors Contributions
Aziz Ullah Shah contributed to data collection and data analysis. Alia Nasir was involved in data analysis and interpretation. Anwar Ali assisted with data collection. Shah Hussain contributed to data analysis and was responsible for the manuscript write-up.
Ethical Approval
Ethical approval was obtained from the IRB of Ziauddin Hospital with Ref No: IRB/ZH/23/12.
Conflict of Interest Statement
The authors declare no conflict of interest.
Guarantor
Aziz Ullah Shah is the guarantor of this study and takes full responsibility for the integrity of the data and the accuracy of the data analysis.
DOI
Cite this Article
Aziz US, Alia N, Anwar A, Shah H. Identification of Risk and Associated Factors of Pressure Ulcer among Hospitalized Patients in Karachi. medtigo J Med. 2025;3(2):e30623216. doi:10.63096/medtigo30623216 Crossref













