






 Author Affiliations
Author Affiliations
Abstract
Introduction: Clubfoot is a congenital anomaly of the foot requiring correction. Different methods are used to correct.
Objective: To evaluate the outcomes of the Ponseti method in the treatment of idiopathic congenital club-foot deformity.
Study design: Descriptive study.
Setting: Department of Orthopedics, MTI-Khyber teaching hospital, Peshawar.
Duration: May 19, 2022, till November 18, 2022.
Subject: Patients for 1 week to 12 months of both genders having congenital clubfoot were enrolled using non-probability consecutive sampling techniques.
Methodology: Study was conducted after approval of the hospital ethical committee and written informed consent of parents. Demographic data was noted. Baseline X-rays were done, and the pre-operative Pirani score was recorded. Ponseti method was used to correct clubfoot. After 6 weeks, X-rays were done, and the post-procedure Pirani score was noted. Outcomes were recorded on a designed Performa. Data was entered and analyzed using statistical package for the social sciences (SPSS) 23.
Results: In our study, 88 cases were enrolled with a mean age of 5.23±2.57 months. There were 36.4% male and 63.6% female patients. In 55.7%, the left foot was involved, and in 44.3%, the right foot was involved. Pre-operative Pirani score was 4.9±0.6. Post-operative Pirani score was 0.16±0.3. Complete recovery was seen in 73.9% of patients, partial recovery was seen in 19.3%, and no recovery was seen in 6.8% of patients.
Conclusion: Ponseti method is effective in the treatment of congenital clubfoot.
Keywords
Clubfoot, Ponseti method, Pirani score, Descriptive study, X-rays.
Introduction
Idiopathic congenital clubfoot deformity is one of the most common congenital orthopedic deformities that occur almost in every 1000 live births.[1] It is a congenital dysplasia of all musculoskeletal structures (muscles, tendons, ligaments, osteo-articular and neurovascular structures) distal to the knee. It is clinically characterized by the equine and varus of the hind-foot, mid-foot caves, and fore-foot adduction.[2] Congenital clubfoot (CCF) etiology may be associated with myelodysplasia, arthrogryposis, or multiple congenital abnormalities, but the most common presentation is the isolated deformity, which is considered to be idiopathic.[3] Untreated clubfoot is a major disability due to congenital bone and joint deformities and may affect both patients’ quality of life and the economic burden on health care systems.[4]
The traditional treatment modality has been a surgical release procedure that has some long-term disadvantages, including deformity recurrence, joint stiffness, and knee and/or thigh deformity or pain. Nowadays, the non-surgical Ponseti casting method is considered the choice treatment for clubfoot deformity among most orthopedic surgeons.[5] In a study by Tracey and colleagues on the management of idiopathic clubfoot deformity by the Ponseti method, 85% of patients had successful correction of the deformity.[6] In another study by Filho et al, the efficacy of Ponseti method in the correction of congenital clubfoot deformity was found to be 87.5%.[3]
Rationale: In a resource-limited setting like ours, a better knowledge of cost-effective and less skill-demanding interventions could be helpful in overcoming the financial challenges. Ponseti method is a relatively cheaper and comparatively less skill-demanding technique for the correction of idiopathic congenital clubfoot deformity. Through a literature search, it was revealed that no study has been done on this subject in our local population in the last five years. Therefore, I planned to evaluate the outcomes of Ponseti method in the treatment of idiopathic congenital clubfoot deformity. Results of my study will help in better counselling of such patients and can be potentially helpful for studies on this subject in the future.
Literature review: Clubfoot (talipes) can be categorized as
- Postural or positional – Technically, these are not true clubfeet.
- Fixed or rigid – These are either flexible (i.e., correctable without surgery) or resistant (i.e., requiring surgical release, though this is not entirely true according to the Ponseti experience)
The Pirani, Goldner, DiMeglio’s, hospital for joint diseases (HJD), and Walker classes have been announced, but no classification system is universally used.[7] The objectives of nonoperative therapy for clubfoot are to correct the deformity early and fully and to retain the correction until growth stops. Conventionally, surgery for clubfoot has been suggested when a plateau has been achieved in nonoperative treatment. With greater acceptance of the Ponseti conservative technique, surgery has come to be seen as a contentious issue. Surgery is not the only standard of care for clubfeet.
Earlier, clubfoot surgery was performed in a way that did not distinguish severity. The same procedure was executed for all patients. Bensahel offered a more individualized approach (ie, adopting only the structures that require release), in which the surgery is tailored to deformity. For example, if the forefoot is well adjusted and externally rotated, and there is no cavus but there is still significant equinus, a posterior approach alone should suffice.[8]
Anatomy of foot: Factors related to bone anatomy include the following
- Tibia – Slight shortening is possible.
- Fibula – Shortening is common.
- Talus – In equinus in the ankle mortise, with the body of the talus being in external rotation, the body of the talus is extruded anterolaterally and is uncovered and can be palpated; the neck of the talus is medially deviated and plantarflexed; all relations of the talus to the surrounding bones are abnormal.
- Os calcis – Medial rotation and an equinus and adduction deformity are present.
- Navicular – The navicular is medially subluxated over the talar head.
- Cuboid – The cuboid is medially subluxated over the calcaneal head.
- Forefoot – The forefoot is adducted and supinated; severe cases also have caves with a dropped first metatarsal.
Factors related to muscle anatomy include the following:
- Atrophy of the leg muscles, especially in the peroneal group, is seen in clubfeet.
- The number of fibers in the muscles is normal, but the fibers are smaller.
- The triceps surau, tibialis posterior, flexor digitorum longus (FDL), and flexor hallucis longus (FHL) are contracted.
- The calf is smaller and remains so throughout life, even after successful long-lasting correction of the feet.
Thickening of the tendon sheaths is repeatedly present, specifically of the tibialis posterior and peroneal sheaths. Contractures of the posterior ankle capsule, subtalar capsule, and talonavicular and calcaneocuboid joint capsules are commonly seen. Contractures are seen in the calcaneofibular, talofibular, (ankle) deltoid, long and short plantar, spring, and bifurcate ligaments. The plantar fascial contracture influences the caves, as does contracture of fascial planes in the
foot.[9]
Pathophysiology of clubfoot: Several theories of the pathogenesis of clubfeet have been developed, containing the following:
- Arrest of fetal development in the fibular stage
- Defective cartilaginous anlage of the talus
- Neurogenic factors
- Retracting fibrosis
- Anomalous tendon insertions
- Seasonal variations
With respect to neurogenic factors, histochemical abnormalities have been observed in the posteromedial and peroneal muscle groups of patients with clubfeet. This is suggested to be due to innervation alterations in intrauterine life secondary to a neurologic event, such as a stroke, leading to mild hemiparesis or paraparesis. This is further confirmed by a 35% occurrence of varus and equinovarus deformity in spina bifida.
Retracting fibrosis (or myofibrosis) may follow secondary to the growth of fibrous tissue in muscles and ligaments. In fetal and cadaveric studies, Ponseti also observed the collagen in all the ligamentous and tendinous structures (except the Achilles (calcaneal) tendon), and it was very loosely crimped and could be stretched.[2] The Achilles tendon, on the other hand, was made up of tightly crimped collagen and was resistant to stretching. Zimny et al found myoblasts in medial fascia on electron microscopy and postulated that they initiate medial contracture.[9] Inclan proposed that anomalous tendon insertions result in clubfeet.[10] However, other studies have not supported this proposal. It is more likely that the distorted clubfoot anatomy can make it seem that tendon insertions are anomalous.
Robertson noted seasonal variations to be a factor in his epidemiological studies in growing countries.[11] This coincided with a similar variation in the incidence of poliomyelitis in the children in the community. Clubfoot was therefore suggested to be a sequela of an antenatal polio-like condition. This theory was further proven by motor neuron changes in the anterior horn of the spinal cord of these babies.
Etiology: The real etiology of congenital clubfoot is unidentified. Most infants who have clubfoot have no identifiable genetic, syndromal, or extrinsic cause.[12] Extrinsic associations involve teratogenic agents (e.g., sodium aminopterin), oligohydramnios, and congenital constriction rings. Genetic associations comprise mendelian inheritance (e.g., diastrophic dwarfism; autosomal recessive pattern of clubfoot inheritance). Cytogenetic abnormalities (e.g., congenital talipes equinovarus (CTEV)) can be seen in syndromes containing chromosomal deletion. It has been recommended that idiopathic CTEV in otherwise healthy infants is the result of a multifactorial system of inheritance.[13] Evidence for this is as follows:
- Incidence in the general population is 1 per 1000 live births.
- Incidence in first-degree relations is approximately 2%
- Incidence in second-degree relations is approximately 0.6%
- If one monozygotic twin has CTEV, the second twin has only a 32% chance of having CTEV.
A study by Weymouth et al demonstrated that associated promoter variants in Homeobox A9 (HOXA9),
α-tropoomyosin (TPM1), and β-tropomyosin (TPM2) alter promoter expression, which suggested that they may have a functional role in gene regulation in clubfoot. A major candidate gene has not yet been identified.[14,15]
Epidemiology: The prevalence of clubfoot is approximately 1 case per 1000 live births in the United States. An analysis utilizing information from the European surveillance of congenital anomalies (EUROCAT) network reported that the total prevalence of congenital clubfoot in Europe was 1.13 per 1000 births.[16] The incidence differs between ethnicities. For example, there are close to 75 cases per 1000 live births in the Polynesian islands, particularly in Tonga. The male-to-female ratio has been stated to be 2:1. Bilateral involvement is found in 30-50% of cases. A 2017 study by Zionts et al discovered that severity did not differ extensively by either sex or bilaterality, however patients with bilateral clubfoot had a wider range of severity.[17] There is a 10% chance of a subsequent child being affected if the parents already have a child with a clubfoot.
Parker et al pooled data from several birth defects surveillance programs (6139 cases of clubfoot) to better estimate the prevalence of clubfoot and examine its risk factors.[12] The overall occurrence of clubfoot was 1.29 per 1000 live births, with figures of 1.38 among non-hispanic whites, 1.30 among hispanics, and 1.14 among non-hispanic blacks or African Americans. Maternal age, equality, education, and marital status were significantly correlated with clubfoot, along with maternal smoking and diabetes.
Prognosis: About 50% of clubfeet in newborns can be improved nonoperatively. Ponseti reported an 89% success rate operating his technique (including an Achilles tenotomy); others reported success rates of 10-35%. One study examined the correction progression of patients with idiopathic clubfeet after the Ponseti technique.[18] The data showed that successive castings lead to decreased cavus and medial crease with a gradual correction of midfoot rotation, adduction, and heel varus. Interestingly, heel equinus increased concurrently with midfoot variables and with final casting. Most series have reported 75-90% satisfactory results of operative treatment (appearance and function of the foot). The amount of motion in the joints of the foot and ankle correlates with the degree of patient satisfaction.[19-21]
Satisfactory results were found in 81% of cases, and the range of ankle movement was a key factor in determining the functional result, which again was influenced by the degree of talar dome flattening (suggesting that the primary bone deformity present at birth dictates the eventual result of treatment). In all, 44% of patients had no dorsiflexion beyond neutral, and 38% of patients needed further surgery (nearly two-thirds of these were bony procedures). Recurrence rates of deformity were stated at around 25%, with a range of 10-50%. Menelaus reported a 38% recurrence rate.[22,23] The best results were acquired with children older than 3-4 months with a foot large enough to allow the procedure to be operated without compromise (>8 cm, as specified by Simons).[24,25] The age at operation is directly linked to the result. Less-than-satisfactory results may be correlated with overcorrection, which appears in nearly 15% of cases.
Some studies have recommended that earlier surgery seems to have a detrimental effect on the result. However, a study of 73 symptomatic children with idiopathic clubfoot previously treated by means of either the Ponseti method or surgery found that these patients had comparable degrees of gait deviation and perceived disability, regardless of which treatment they had received.[26] Steinman et al evaluated the Ponseti and French functional techniques for idiopathic clubfeet (265 feet (176 patients) by the Ponseti method; 119 feet (80 patients) by the French functional method).[27] The study disclosed that although there was a trend toward improved results with the Ponseti method, the difference was not significant. Parents chose the Ponseti method twice as often as the French functional method. Initial correction rates were 94.4% for the Ponseti method and 95% for the French functional method.
Relapses occurred in 37% of the Ponseti-method feet, and in a third of these cases, further nonoperative treatment was successful; however, surgical treatment was necessary for the other two-thirds.[27] Relapses occurred in 29% of the feet treated by the French functional method; surgical intervention was necessary in all those cases. At the latest follow-up, outcomes with the Ponseti method were good in 72% of cases, fair in 12%, and poor in 16%. For the French functional method, outcomes were good in 67%, fair in 17%, and poor in 16%.
In a controlled study of 164 patients (238 feet), Jeans et al compared the Ponseti method (n = 122) with the French physiotherapy (PT) method (n = 116) in terms of pedobarographic findings at age 5 years.[28] The only significant difference documented between the two groups was that the PT group had significantly less medial movement of the center of pressure (COP) line. Plantar pressures in the hindfoot and first metatarsal regions were reduced in both groups, as associated with control subjects, and increased in the midfoot and lateral forefoot regions. Mild residual deformity remained even though clinically successful outcomes were achieved.
Parada et al investigated the safety of general anesthesia in infants who underwent percutaneous tendoachilles tenotomy. The procedure was performed in 137 patients (182 tenotomies). Of the tenotomies, 92 were unilateral and 45 bilateral. No complications related to anesthesia were acknowledged, and nearly all patients were discharged on the day of surgery.[29] Pavone et al succeeded in good/excellent outcomes in 96% of the 82 patients with 114 congenital clubfeet treated with the Ponseti method from 2004 through 2010, with follow-up through 2011.[30]
A two-institution review by Miller et al found that strict adherence to the Ponseti method in nonoperative treatment of isolated clubfoot, as opposed to more flexible adherence, was associated with enhanced outcome in the form of a reduced risk of subsequent unplanned surgical intervention.[31] In a cross-sectional study of postcorrection brace wear over a 3-month period in 48 patients in four age-based groups (6-12 months, >1 to 2 years, >2 to 3 years, and >3 to 4 years) who were treated for idiopathic clubfoot, Sangiorgio et al found that patients who wore the brace for a mean of 8 hours daily had significantly lower relapse rates than those who wore the brace for a mean of 5 hours daily.[32]
Jeans et al evaluated functional outcomes at age 10 years in 175 children (263 feet) initially treated nonoperatively for clubfoot with either the Ponseti or the French PT method and compared outcomes in feet that had undergone only nonoperative treatment with those that required subsequent surgery.[33] They found that clubfeet treated without surgery had better ankle power and isokinetic strength than those that underwent intra-articular surgery for residual deformity or recurrence. Compared with controls, both nonoperatively and surgically treated clubfeet had significant limitations in ankle plantarflexion, resulting in decreased range of motion, moment, and power.
Clubfoot clinical presentation: Seek a detailed family history of clubfoot or neuromuscular disorders and perform a general examination to identify any other abnormalities. Examine the feet with the child prone, with the plantar aspect of the feet visualized, and supine to evaluate internal rotation and varus. If the child can stand, determine whether the foot is plantigrade, whether the heel is bearing weight, and whether it is in varus, valgus, or neutral. Similar deformities are seen with myelomeningocele and arthrogryposis. Therefore, always examine these associated conditions. The ankle is in equinus, and the foot is supinated (varus) and adducted (a normal infant foot usually can be dorsiflexed and everted, so that the foot touches the anterior tibia). Dorsiflexion beyond 90° is not possible.
The navicular is displaced medially, as is the cuboid. Contractures of the medial plantar soft tissues are present. Not only is the calcaneus in a position of equinus, but the anterior aspect is also rotated medially and the posterior aspect laterally. The heels are small and empty. The heel feels soft to the touch (akin to the feel of the cheeks). As the treatment progresses, it fills in and develops a firmer feel (akin to the feel of the nose or of the chin).
The talar neck is easily palpable in the sinus tarsi as it is uncovered laterally. Generally, this is covered by the navicular, and the talar body is in the mortise. The medial malleolus is difficult to palpate and is often in contact with the navicular. The normal navicular-malleolar interval is diminished. The hindfoot is supinated, but the foot is often in a position of pronation relative to the hindfoot. The first ray often drops to create a position of cavus.
The Ponseti method of closed management of clubfeet through manipulations and casting defines the elevation of the first metatarsal as a first step, even if it means seemingly exacerbating the supination of the foot. The tibia often has internal torsion. This assumes special importance in the casting management of clubfeet, where care should be taken to rotate the feet into abduction, avoiding spurious tibial rotation through the knee. (See the images below). Even after correction, the foot often remains short, and the calf thin.

Figure 1: Idiopathic congenital talipes equinovarus (ICTEV): A) Anterior view; B) Posterior view (bilateral)
Clubfoot (Talipes) workup: While imaging studies generally are not essential to know the nature or the severity of the deformity, radiography provides a useful baseline before and after surgical correction of the feet, closed Achilles tenotomy, or a limited posterior release. Radiographs show the true gain in foot (ankle) dorsiflexion and confirm the appearance of an iatrogenic rocker-bottom foot should one result. Occasionally, radiographs are necessary to diagnose clubfeet associated with tibial hemimelia.
Talocalcaneal parallelism is the radiographic feature of clubfoot (talipes). Simulated weight-bearing X-rays are used for infants who have not commenced walking. Positioning for foot x-rays is very important. The anteroposterior (AP) view is taken with the foot in 30° of plantarflexion and the tube at 30° from vertical. The lateral view is taken with the foot in 30° of plantarflexion. AP and lateral views can also be taken in full dorsiflexion and plantarflexion. This is especially essential in determining the total amount of dorsiflexion completed at the end of treatment, as well as the relative positions of the talus and calcaneum.
Measure the talocalcaneal angle in the AP and lateral films. AP lines are drawn through the center of the long axis of the talus (parallel to the medial border) and through the long axis of the calcaneum (parallel to the lateral border), and they usually subtend an angle of 25-40°. Any angle less than 20° is considered abnormal. The AP talocalcaneal lines are almost parallel in clubfeet. As the feet are correct with casting or surgery, the calcaneus rotates externally, and the talus reciprocally also derotates to a lesser degree to give a convergent talocalcaneal angle. Lateral lines are drawn through the midpoint of the head and body of the talus and along the bottom of the calcaneum, usually 35-50°. Clubfoot ranges between 35° and –10°.
The lateral talocalcaneal lines are almost parallel in clubfeet. As the feet are correct with casting or surgery, the calcaneum dorsiflexes relative to the talus to give a convergent talocalcaneal angle. These two angles, AP and lateral, are added to derive the talocalcaneal index, which in a corrected foot should be more than 40°. The AP and lateral talar lines normally pass through the center of the navicular and the first metatarsal.
In older children, a flat-top talus can be demonstrated radiologically if the talus is adequately calcified, but care is required for positioning of the foot. A lateral film with the foot held in maximal dorsiflexion is the most consistent method of diagnosing an uncorrected clubfoot; the absence of calcaneal dorsiflexion is evidence that the calcaneus is still locked in varus angulation under the talus. A study by Sri Harsha et al found that in infants with idiopathic clubfeet, the Pirani and DiMeglio’s clinical scores correlated well with radiologic parameters, suggesting that routine use of radiography in evaluation and follow-up could be avoided and exposure to radiation thereby prevented.[34]

Figure 2: Lateral view in talipes equinovarus demonstrates an abnormally elevated tibiocalcaneal angle (Normal angle is 60-90°)

Figure 3: Dorsoplantar views obtained in a patient with unilateral clubfoot show that the talus and calcaneus are more overlapped than in the normal condition (Talocalcaneal angle is <15°)
Clubfoot (Talipes) treatment & management: Although it is sometimes recommended that idiopathic clubfoot (talipes) be treated as soon as possible, this condition does not constitute an orthopedic emergency.[35]
Traditionally, surgery for clubfoot has been suggested when a plateau has been achieved in nonoperative treatment. It is usually performed when the child is of sufficient size to allow for the recognition of the anatomy. No specific contraindications for surgery exist, though the child’s size dictates that surgery is best performed at approximately age 6 months. With greater acceptance of the Ponseti conservative technique, surgery has come to be seen as a contentious issue. Surgery for clubfeet is not the only standard of care.[36]
Nonoperative therapy: The aims of nonoperative therapy for clubfoot are to correct the deformity early and fully and to maintain the correction until growth stops.
Traditionally, two categories of clubfeet are identified, as follows:
- Easy or correctable clubfeet – These are readily corrected with manipulation, casting, and splintage alone.
- Resistant clubfeet – These respond poorly to splinting and relapse quickly after seemingly successful manipulative treatment; they require early operative management and are said to be associated with a thin calf and a small, high heel.
The Pirani scoring system, devised by Shafiq Pirani, MD, of Vancouver, BC, consists of six categories, three in the hindfoot and three in the midfoot, as follows:
- Curvature of the lateral border (CLB) of the foot
- Medial crease (MC)
- Uncovering of the lateral head of the talus (LHT)
- Posterior crease (PC)
- Emptiness of the heel (EH)
- Degree of dorsiflexion (DF)
The first three (CLB, MC, and LHT) constitute the midfoot score, and the last three (PC, EH, and DF) constitute the hindfoot score.[4,37] Each category is scored as 0, 0.5, or 1. The lowest possible (best) total score for all categories combined is 0, and the highest possible (worst) total score is 6. The Pirani scoring system can be used to identify the severity of the clubfoot and to monitor the correction. It is necessary to provide counsel and advice to parents. They should be reassured that they are in no way responsible for the deformity and that it is unlikely to be reproduced in subsequent pregnancies.
With traditional nonoperative treatment, splintage begins 2-3 days after birth. The order of correction is as follows:
- Forefoot adduction
- Forefoot supination
- Equinus
Attempts to correct equinus first may break the foot, producing a rocker-bottom foot (see the image below). Force must never be used. Merely bring the foot to the best position obtainable and maintain this position either by strapping every few days or by changing the casting weekly until either full correction is obtained or correction is halted by some irresistible force.
The corrected position is maintained for several months. Surgery should be used as soon as it is obvious that conservative treatment is failing (persisting deformity, rocker-bottom deformity, or rapid relapse after correction has stopped). By 6 weeks, it is usually apparent whether the foot is easy or resistant; this is confirmed on x-ray due to the orientation of the bones. Reported success rates for these traditional casting methods are 11-58%.
Ponseti method: This method was developed by Ignacio Ponseti, MD, of the University of Iowa. Its premise is based on Ponseti’s cadaveric and clinical observations.[1,3,27,38] An accelerated Ponseti method has been proposed in which manipulations, five castings, and Achilles tenotomy are implemented within a week. A preliminary study found this approach to be safe and effective for the initial correction of severe idiopathic clubfoot in children younger than 3
months.[39]
The standard Ponseti method may be divided into seven steps, as follows.
Step 1: The calcaneal internal rotation (adduction) coupled with plantarflexion is the key deformity. The foot is adducted and plantarflexed at the subtalar joint, and the goal is to abduct the foot and dorsiflex it. To achieve correction of the clubfoot, the calcaneum should be allowed to rotate freely under the talus, which is also free to rotate in the ankle mortise. The correction takes place through the normal arc of the subtalar joint. This is achieved by placing the index finger of the operator on the medial malleolus to stabilize the leg and levering on the thumb placed on the lateral aspect of the head of the talus while abducting the forefoot in supination. Forcible attempts to correct the heel varus by abducting the forefoot while applying counterpressure at the calcaneocuboid joint prevent the calcaneum from abducting and therefore everting.
Step 2: Foot cavus increases when the forefoot is pronounced. If cavus is present, the first step in the manipulation process is to supinate the forefoot by gently lifting the dropped first metatarsal to correct the cavus. Once the cavus is corrected, the forefoot can be abducted as outlined in step 1.
Step 3: Pronation of the foot also causes the calcaneum to jam under the talus. The calcaneum cannot rotate and stays in varus. The cavus increases as outlined in step 2. This results in a bean-shaped foot. At the end of step 1, the foot is maximally abducted but never pronated.
Step 4: The manipulation is carried out in the cast room, with the baby having been fed just before, or even during, the treatment. After the foot is manipulated, a long leg cast is applied to hold the correction.
Initially, the short leg component is applied. The cast should be snug with minimal but adequate padding. The authors paint or spray the limb with tincture of benzoin to allow adherence of the padding to the limb. The authors prefer to apply additional padding strips along the medial and lateral borders to facilitate safe removal of the cast with a cast saw. The cast must incorporate the toes right up to the tips, but not squeeze the toes or obliterate the transverse arch. The cast is molded to contour around the heel while abducting the forefoot against counter pressure on the lateral aspect of the head of the talus.
The knee is flexed to 90° for the long leg component of the cast. The parents can soak these casts for 30-45 minutes before removal with a plaster knife. The author’s preferred method is to use the oscillating plaster saw for cast removal. The cast is bivalved and removed. The cast is then reconstituted by coating the two halves. This allows for monitoring of the progress of the forefoot abduction and, in the later stages, the amount of dorsiflexion or equinus correction.
Step 5: Forcible correction of the equinus (and cavus) by dorsiflexion against a tight Achilles tendon results in a spurious correction through a break in the midfoot, resulting in a rocker-bottom foot. The cavus should be separately treated as outlined in step 2, and the equinus should be corrected without causing a midfoot break. It generally takes as many as four to seven casts to achieve maximum foot abduction. The cast changes weekly. The foot abduction (correction) can be considered adequate when the thigh-foot axis is 60°.
After maximal foot abduction is obtained, most cases require a percutaneous Achilles tenotomy. This is performed in the cast room under aseptic conditions. The local area is anesthetized with a combination of a topical lidocaine preparation (EMLA Cream; AstraZeneca, Wilmington) and minimal local infiltration of lidocaine. The tenotomy is performed through a stab incision with a round-tip (6400) beaver blade. The wound is closed with a single absorbable suture or with adhesive strips. The final cast is applied with the foot in maximum dorsiflexion, and the foot is held in the cast for 2-3 weeks.
Step 6: After the manipulation and casting phase, the feet are fitted with open-toed strait-laced shoes attached to a Dennis Brown bar. The affected foot is abducted (Externally rotated) to 70° with the unaffected foot set at 45° of abduction. The shoes also have a heel counter bumper to prevent the heel from slipping out of the shoe. The shoes are worn for 23 hours a day for 3 months and are worn at night and during naps for up to 3 years.
Step 7: In 10-30% of cases, a tibialis anterior tendon move to the lateral cuneiform is performed when the child is approximately 3 years of age. This gives lasting correction of the forefoot, preventing metatarsus adducts and foot inversion. This technique is indicated in a child aged 2-2.5 years with dynamic supination of the foot. Before surgery, cast the foot in a long leg cast for a few weeks to regain the correction.
Reported results: The range of outcomes described in this setting is diverse. A systematic review of 124 trials by Golfer et al identified 20 isolated outcomes and 16 outcome tools used as outcome measures for Ponseti correction of idiopathic clubfoot.[40] The most reported isolated outcomes were qualitative and subjective; the most reported quantitative outcomes were ankle range of motion, standing foot position, and muscle function. A 2014 Cochrane review found the Ponseti approach to yield significantly better results than either the Kite method or a traditional approach, though the quality of the evidence was not high.[41]
A study by Dragoni et al recommended that this approach may be efficient for the treatment of rigid residual deformity of congenital clubfoot after walking age.[42] A study of 90 children by Liu et al suggested that starting Ponseti treatment between the ages of 28 days and 3 months was associated with fewer casts essential, a lower relapse rate, and a lower final international clubfoot study group score (ICFSG) score than starting either earlier or later.[43]
A systematic review of 124 trials by Muzzammil et al identified a considerable correlation between patient nutritional status and the outcome of Ponseti treatment.[44] Malnourished patients needed more casts and were more likely to require Achilles tenotomy.

Figure 4: Casting with plaster of paris
Surgical therapy
Preparation for surgery: The operating room is kept warm, and a general anesthetic is used. The usual position is supine with the foot resting over the contralateral leg in a figure-four position. Some surgeons prefer the lateral decubitus position or even a prone position. A tourniquet is generally used, and the surgical technique is performed with the help of optical loupe magnification.
Incision: Options for incisions include the following:
- Cincinnati incision
- Turco curvilinear medial or posteromedial incision
The Cincinnati incision is a transverse incision that extends from the anteromedial (region of navicular-cuneiform joint) to the anterolateral (just distal and medial to the sinus tarsi) aspect of the foot and over the back of the ankle at the level of the tibiotalar joint.[45] The Turco incision can lead to wound breakdowns, especially at the corner of the vertical and medial limbs.[46] To avoid this problem, some surgeons prefer to use either three separate incisions (posterior vertical, medial, and lateral) or two separate incisions (curvilinear medial and posterolateral).
Any approach should be able to address the release in all quadrants, as follows:
- Plantar: Plantar fascia, abductor hallucis, flexor digitorum brevis (FDB), long and short plantar ligaments.
- Medial: Medial structures, tendon sheaths, talonavicular and subtalar release, tibialis posterior, flexor hallucis longus (FHL), and flexor digitorum longus (FDL) lengthening.
- Posterior: Ankle and subtalar capsulotomy, especially releasing talofibular and tibiofibular ligaments and calcaneofibular ligaments.
- Lateral: Lateral structures, peroneal sheath, calcaneocuboid joint, and completion of talonavicular and subtalar release.
Surgical clubfoot release: In the past, clubfoot surgery was implemented in a way that did not separate severity. The same procedure was performed for all patients. Bensahel aimed for a more individualized approach (i.e., addressing only the structures that require release). The surgery is tailored to the deformity. For example, if the forefoot is well corrected and externally rotated, if there is no caves, but if there is still a significant equinus, a posterior advance alone should suffice.[47,48]
Any approach should afford adequate exposure. Structures to be released or lengthened are the following:
- Achilles (calcaneal) tendon
- Tendon sheaths of the muscles crossing the subtalar joint
- Posterior ankle capsule and deltoid ligament
- Inferior tibiofibular ligament
- Calcaneofibular ligament
- Capsules of the talonavicular and subtalar joints
- Division of associated ligaments around the subtalar joint
- Plantar fascia and intrinsic muscles
The longitudinal axis of the talus and calcaneum should be separated by about 20° in the lateral projection, and the calcaneal angle should be a right angle to the shaft of the tibia.
The correction is held with wires at the talocalcaneal joint, the talonavicular joint, or both, possibly with a plaster cast. The wound should never be forcibly closed. It can be left open to granulate and heal by secondary intention or even grafted with split-thick skin grafts.
Surgical treatment should consider the age of the patient, as follows:
- In children younger than 5 years, correction can be achieved with soft tissue techniques
- Children older than 5 require bony reshaping (e.g., dorsolateral wedge excision of the calcaneocuboid joint (Dillwyn Evans procedure) or osteotomy of the calcaneum to correct varus)
- If the child is older than 10 years, lateral wedge tarsectomy or triple fusion (arthrodesis) is required (salvage procedures)
Posterior release steps, in brief, are as follows:
- Longitudinal incision
- Z-lengthened tendocalcaneus
- Identify the neurovascular (NV) bundle
- Tendon sheaths of FHL, FDL, and tibialis posterior released; tendons not elongated.
- Ankle joint capsule opened; talofibular, calcaneofibular, and deep portion of deltoid ligaments released (blunt dissection)
- Release of distal tibial and fibula ligaments
- Posterior release of the subtalar joint
- With the foot held just above neutral, the tendocalcaneum is repaired, and the skin is closed
- Plaster-of-Paris cast in corrected position for 4 weeks, followed by splints until maturity.[45,46]
A posteromedial release (Turco procedure) is performed as follows.
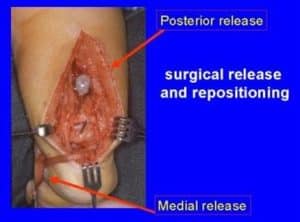
Figure 5: Posteromedial release for clubfoot
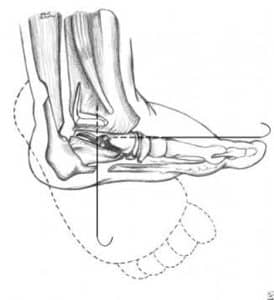
Figure 6: Schematic representation of posteromedial release
Make a medial incision 8-9 cm long from the base of the first metatarsal to the tendocalcaneum, curving it just inferior to the medial malleolus without undermining skin. Mobilize and expose the tendons of the tibialis posterior, FDL, FHL, Achilles tendon, and posterior NV bundle.
Continuing the incision in the sheaths of FDL and FHL, divide Henry’s master knot beneath the navicular. Divide the spring ligament, detaching it from the sustentaculum tali and the origin of the abductor hallucis. Release the remaining contractures, starting posteriorly. Lengthen the Achilles tendon (Z-plasty), detaching the medial half of the tendon insertion.
Retract the NV bundle and FHL anteriorly to expose the posterior aspect of the ankle and subtalar joints. Then, incise the posterior capsule of the ankle joint under direct visualization, as well as the posterior talofibular ligament (if necessary, currently). Divide the subtalar capsule and calcaneofibular ligament.
Retract the NV bundle posteriorly and divide the tibiocalcaneal part of the deltoid ligament. Lengthen the tibialis posterior if it is contracted. Open the talonavicular joint and divide its capsule, but avoid damaging the articular surface. Then, the subtalar ligaments are released, and the navicular structure is reduced onto the head of the talus, which should properly align with the other tarsal bones.
Ensure that the relation of the talus to the calcaneus and navicular is correct and stabilize the foot with Kirschner wires (K-wires). The first K-wire is passed from the dorsum of the foot across the first metatarsal shaft, the medial cuneiform, the navicular, and into the talus. A second wire fixes the subtalar joint, and this should maintain the foot in the corrected position.
Apply an above-the-knee plaster-of-Paris cast, which is changed to 3 weeks and maintained to 6 weeks. The foot is initially held in slight equinus if there is tension on the skin closure, which is corrected at the time of cast change. Splintage is continued for at least 4 months after surgery, and night splints are used for several years.
The Ilizarov correction is used for recurrent clubfeet, specifically in conditions such as arthrogryposis.[49-52] The calcaneum is held with two opposing olive-tipped wires. The distractor force, in the form of heel-pushing distractors, must be posteriorly directed to prevent anterior subluxation of the talus in the ankle mortise. Joshi’s external stabilization system (JESS), an external fixator–based method that makes use of differential distraction, has been employed to treat neglected, neurogenic, or relapsed clubfeet. A study of 31 such clubfeet in 24 patients (16 males, 8 females; age range, 2-10 years) by Altaf et al found that JESS led to correction of all clubfoot components in all patients, though one patient did require tibialis anterior transfer for dynamic forefoot adduction at the end of treatment.[53]

Figure 7: Ilizarov distraction for arthrogrypotic clubfoot
Postoperative care: Pay meticulous attention to the wound after surgery. If the skin closure is difficult, it is better to leave the wound open and allow it to granulate for a delayed primary or secondary closure or allow it to heal by granulation tissue. Skin grafts can also be used to cover the defect. The plaster splint should be only lightly applied, and the wound should be inspected regularly. The transfixion pins usually are removed in 3-6 weeks. The foot requires splintage in appropriate footwear for 6-12 months.
Complications: Complications of the treatment of clubfoot include the following:
- Infection (rare).
- Wound breakdown: Release skin retractors every 30 minutes and release the tourniquet before closing the wound and applying a cast.
- Stiffness and restricted range of motion: Early stiffness correlates with a poor result.
- Avascular necrosis(AVN) of the talus: A 40% incidence of avascular necrosis of the talus occurs with combined simultaneous medial and lateral release.
- Persistent in toeing: This is quite common; it is due not to tibial intorsion but, rather, to insufficient external rotation correction of the subtalar joint.
Overcorrection is associated with the following:
- Release of the interosseous ligament of the subtalar joint.
- Excess lateral displacement of the navicular on the talus.
- Overlengthening of tendon units.
For residual deformity following the initial surgery, rule out neurologic causes of recurrence (e.g., tethered cord). A residual deformity may be either of the following:
- Dynamic: With residual adducts and supination that are fully correctable passively, treat with split anterior tibial tendon transfer.
- Fixed: If scarring is not excessive and the patient is younger than 5 years, repeat the release; if the patient is older than 5 years, a bony procedure to straighten the lateral border of the foot is required.
Options to correct conduct are as follows:
- Metatarsal osteotomy: This operation creates a secondary deformity to compensate for a primary deformity in the tarsus; it is rarely indicated.
- Cuboid decancellation.
- Calcaneocuboid fusion: The Dillwyn Evans procedure consists of a medial and posterior release together with excision and fusion of the calcaneocuboid joint55; it should be reserved for patients older than 4 years; these two procedures aim to shorten the lateral side of the foot.
- Lengthening the medial side of the foot (e.g., talar osteotomy): This is not widely performed; avascular necrosis (AVN) is a risk.
Options to correct residual hindfoot deformity are the following:
- Heel varus: Open the medial wedge or close the lateral wedge; lateral displacement os calcis osteotomy is preferred.
- Residual cavus and adductus: Perform a wedge tarsectomy.
- Failed feet: Perform a triple arthrodesis.
Long-term monitoring: As small infants with operated clubfeet have grown into heavy adults, they have been prone to painful stiff feet, despite good correction.[56] Deitz and Cooper published a 30-year follow-up study of patients treated with the Ponseti method.[57] These cases had comparatively pain-free supple feet. The Ponseti method is gaining mainstream acceptance, as evidenced by the emergence of Ponseti clubfeet centers at major teaching hospitals across the United States. Of the patients who have been monitored over the long term, those who are heavy and those who have jobs involving long periods on their feet (especially performing manual labor) were found to be more likely to have painful feet.[58] This correlated with the trend seen in the general population at large.
Richards et al evaluated the value of standing lateral radiographs of successfully treated idiopathic clubfeet made at 18-24 months of age for predicting late recurrence (211 patients, 312 clubfeet).[59] Patients were younger than 3 months at presentation, had a clinically plantigrade foot at 2 years of age, and were followed for a minimum of 4 years. Radiographs were assessed for talocalcaneal angle and tibiocalcaneal angles by two trained practitioners. These measurements were not found to be helpful in predicting future relapse.
Little et al studied 104 children (172 feet) with the aim of determining whether poor evertor muscle activity on clinical examination could predict recurrence of idiopathic clubfoot at 5-year follow-up (mean, 62 months; range, 41-71) after Ponseti treatment.[60] Of the 104 patients, 76 had good evertor activity and 28 had poor activity; 19 (18.3%) had recurrence that was treated with repeat casting, and 14 (13.5%) required additional surgery after recasting. Recurrence was highly associated with poor evertor activity. The authors suggested that semiquantitative evertor muscle activity assessment could predict recurrence and should be added to routine clinical assessment to facilitate individualization of treatment.
Objective: To evaluate the outcomes of Ponseti method in the treatment of idiopathic congenital club-foot deformity.
Congenital club-foot deformity: It was confirmed when.
- Clinical examination: Newborn having foot that is rotated internally at the ankle, heels deviated upwards with foot pointing down and inwards, and the soles of the feet facing each other.
- Imaging: X-ray the foot revealing talo-calcaneal angleless than 35o on lateral view, talo-calcaneal angle less than 20o on antero-posterior view, talus to first metatarsal angle greater than 15o on AP view and medial subluxation of the navicular on the talus.
Ponseti method: It is a non-surgical intervention for correction of congenital club-foot deformity that involves manipulations and plaster exchanges with weekly inguino-podal immobilization for a period of six weeks.
Outcomes of ponseti method were assessed using Pirani Score Sheet (annexure 1). Outcomes were in terms of
- Pirani score of 0 after completion of 6 weeks of treatment was labelled as complete recovery.
- Pirani’s score of 0.5 after the completion of 6 weeks of treatment was labelled as partial recovery.
- Pirani score of 1 after completion of 6 weeks of treatment was labelled as treatment failure.
Methodology
Study design: Descriptive study.
Settings: Department of orthopedics, MTI-Khyber teaching hospital, Peshawar.
Study duration: May 19, 2022, till November 18, 2022.
Sampling technique: Non-probability Consecutive Sampling Technique.
Sample size: Sample size is calculated using the WHO sample size. Taking the expected frequency of complete recovery, p = 85%, margin of error= 7.5%, confidence level= 95%, and n = 88 (one foot was considered as one case).
Inclusion criteria:
- Patient age: 1 week to 12 months.
- Both genders.
- Patients presenting with congenital clubfoot deformity as per the operational definition.
Exclusion criteria:
- Patients with a previous history of manipulation or intervention for clubfoot deformity.
- Patients with a history of myelodysplasia or arthrogryposis.
- Patients with a history of multiple congenital abnormalities
- Patients with active infections cannot be subjected to casting.
- Patients with iatrogenic birth injuries.
Data collection: After approval from the ethical and research department, patients with congenital club-foot deformity were enrolled from the outdoor department of orthopedics of the hospital. Informed written consent was taken from all study participants. Baseline information was noted on arrival, including age, gender, and laterality of the foot (right, left, or bilateral).
At our institution, a baseline X-ray of the clubfoot is performed on initial arrival for future comparison and calculation of the Pirani score. All study participants were subjected to correction of clubfoot deformity through the Ponseti method, which involved correction of cavus by stretching the plantar structures and maintaining them in supination through casting for one week, followed by correction of varus, adduction, and equinus through weekly casting for the next five weeks. Achilles tenotomy was performed on patients who failed to achieve equine correction after 5 weeks of casting. All the casting and surgical procedures (Achilles tenotomy) were performed by a consultant orthopedic surgeon with five years of post-fellowship experience. After completion of the casting period for 6 weeks, an X-ray of the foot was performed, and the Pirani score was calculated. The outcome of the Ponseti method was assessed by calculating the post-casting Pirani score. Outcomes were recorded in terms of frequency of complete recovery (Pirani score=0), partial recovery (Pirani score=0.5), and treatment failure (Pirani score=1) as per operational definition. All the data was recorded by the researcher himself on a specially designed proforma (annexure-II).
Data analysis: Data was analyzed using the statistical analysis program IBM SPSS version 23. Frequencies and percentages were calculated for qualitative variables including gender, laterality of the foot (right, left, or bilateral), and outcomes (complete recovery, partial recovery, treatment failure). Mean ± standard deviation was calculated for quantitative variables, including age, baseline Pirani score, and post-casting Pirani score. Effect modifiers like age, gender, and foot laterality were controlled through stratification. Post-stratification chi-square test was applied, and a p-value ≤ 0.05 was considered statistically significant.
Results
In our study, 88 cases were enrolled with a mean age of 5.23±2.57 months (Table 1).
| N | Minimum | Maximum | Mean | Standard deviation (SD) | |
| Age (months) | 88 | 1 | 12 | 5.23 | 2.57 |
Table 1: Age of the sampled population
There were 36.4% male and 63.6% female patients (Table 2).
| Frequency | Percent | ||
| Gender | Male | 32 | 36.4 |
| Female | 56 | 63.6 | |
| Total | 88 | 100.0 | |
Table 2: Gender distribution
In 55.7%, the left foot was involved, and in 44.3%, the right foot was involved (Table 3).
| Frequency | Percent | ||
| Laterality | Right | 39 | 44.3 |
| Left | 49 | 55.7 | |
| Total | 88 | 100.0 | |
Table 3: Laterality of foot
Pre-operative Pirani score was 4.9±0.6 (Table 4).
| N | Minimum | Maximum | Mean | SD | |
| Pre-operative Pirani score | 88 | 4.00 | 6.00 | 4.931 | 0.621 |
Table 4: Pre-operative Pirani score
Post-operative Pirani score was 0.16±0.3 (Table 5).
| N | Minimum | Maximum | Mean | SD | |
| Post-operative Pirani score | 88 | 0.00 | 1.00 | 0.1648 | 0.30059 |
Table 5: Post-operative Pirani score
Complete recovery was seen in 73.9% of patients, partial recovery was seen in 19.3%, and no recovery was seen in 6.8% of patients (Table 6).
| Frequency | Percent | ||
| Outcome | Complete recovery | 65 | 73.9 |
| Partial recovery | 17 | 19.3 | |
| No recovery | 6 | 6.8 | |
| Total | 88 | 100.0 | |
Table 6: Frequency of treatment outcomes
Data stratification was done in age groups, gender, and foot laterality (Tables 7, 8, 9).
| Outcome | Total | |||||
| Complete recovery | Partial recovery | No recovery | ||||
| Age groups | 1-6 months | Count | 52 | 13 | 0 | 65 |
| % within Age groups | 80.0% | 20.0% | 0.0% | 100.0% | ||
| 7-12 months | Count | 13 | 4 | 6 | 23 | |
| % within Age groups | 56.5% | 17.4% | 26.1% | 100.0% | ||
| p-value = 0.001 | ||||||
Table 7: Data stratification for frequency of treatment outcomes and age groups
| Outcome | Total | |||||
| Complete recovery | Partial recovery | No recovery | ||||
| Gender | Male | Count | 20 | 9 | 3 | 32 |
| % within Gender | 62.5% | 28.1% | 9.4% | 100.0% | ||
| Female | Count | 45 | 8 | 3 | 56 | |
| % within Gender | 80.4% | 14.3% | 5.4% | 100.0% | ||
| p-value = 0.185 | ||||||
Table 8: Data stratification for frequency of treatment outcomes and gender
| Outcome | Total | |||||
| Complete recovery | Partial recovery | No recovery | ||||
| Laterality | Right | Count | 33 | 4 | 2 | 39 |
| % within Laterality | 84.6% | 10.3% | 5.1% | 100.0% | ||
| Left | Count | 32 | 13 | 4 | 49 | |
| % within Laterality | 65.3% | 26.5% | 8.2% | 100.0% | ||
| Total | Count | 65 | 17 | 6 | 88 | |
| % within Laterality | 73.9% | 19.3% | 6.8% | 100.0% | ||
Table 9: Data stratification for frequency of treatment outcomes and foot laterality
Discussion
Worldwide, 150,000-200,000 babies with idiopathic congenital talipes equino varus (ICTEV) are born each year, and approximately 80% of them are born in the developing world with limited access to appropriate medical care. Untreated or incorrectly treated clubfoot soon becomes “neglected clubfoot” as the child grows older and learns to walk.[61] ICTEV is a common complex congenital anomaly in 0.39-7 children per 1000 births worldwide.[62] The affected children have abnormal foot anatomy and biomechanics, with the affected feet being fixed in an extended, adducted position.[63] The burden of untreated or incorrectly treated ICTEV negatively impacts society and should be viewed as a public health issue to reduce its prevalence through early diagnosis andthe institution of appropriate treatment.[64] The goal of treatment is to achieve early and full correction of all four deformities of the foot, ensure that the patient has a functional, pain-free, plantigrade foot, with good mobility, without calluses, and does not need to wear modified shoes.[65] The treatment modalities for ICTEV have evolved through a series of trials to include conservative and surgical methods since the 18th century.
Ponseti, in the 1950s, developed a non-operative technique of management of ICTEV and published his findings in 1963, registering excellent outcomes in terms of function. The early treatment outcomes have kept improving since the time many surgeons began embracing the technique about 35 years ago. Ponseti technique in the past 13 years has been embraced as the standard treatment for patients with ICTEV.[66] This study was done to determine the outcomes of the Ponseti method in our population. In our study, 88 cases were enrolled with a mean age of 5.23±2.57 months. There were 36.4% male and 63.6% female patients. In 55.7%, the left foot was involved, and in 44.3%, the right foot was involved. Pre-operative Pirani score was 4.9±0.6. Post-operative Pirani score was 0.16±0.3. Complete recovery was seen in 73.9% of patients, partial recovery was seen in 19.3%, and no recovery was seen in 6.8% of patients.
Our results were like other studies. In a study by Tracey and colleagues on the management of idiopathic club-foot deformity by Ponseti method, 85% of patients had successful correction of the deformity. [6] In another study by Filho et al, the efficacy of Ponseti method in the correction of congenital clubfoot deformity was found to be 87.5%.[3] A study conducted in Pakistan there were 43 males (69.4%) and 19 females (30.6%). Mean age was 11.16±5.52 months. Frequency of outcome results was excellent in 30 patients (48.4%), good in 20 patients (32.3%), fair in 08 patients (12.9%), and poor in 04 (6.5%). A statistically significant difference was found between the ages of children and hind foot varus (p<0.05) and between the ages of children and ankle dorsiflexion.[67]
In another study, 86 patients were enrolled, 53(68%) were boys and 33(32%) were girls. There was a total of 111 feet in the study. Of the total, 13(12%) patients had a family history of TEV, and 24(23%) had bilateral deformity. The age range of the sample was from one week to 10 years. Children aged up to 4 years need 5-6 casts while the rest need 8-10 casts. An excellent/good functional outcome was reported in 85% of cases.[68] In a multicenter study a total of fifty (50) patients coming to the Outpatient department of either gender from one to three years of age with Idiopathic clubfoot of moderate to severe deformity according to pirani score (i.e. 3 to 6). The outcome was recorded at the time of removal of the final cast after 3 weeks, and the final Pirani score was documented to assess the success of treatment. The results of the study reveal that most of the patients i.e. 48%(n=24) had 2 years of age, mean and SD was calculated as 1.64+0.76 years, 58%(n=29) male and 42%(n=21) females, mean and of Pirani Score was 1.31+0.43 years, frequency of efficacy of Ponseti method for treatment of idiopathic clubfoot by correction of all deformities in toddlers in terms of percentage of excellent Pirani score reveals in 68%(n=34) while 32%(n=16) had no findings of efficacy.[69]
In a study conducted in Turkey included 44 feet of 31 patients (25 boys, 6 girls; mean age 3 months; range 4 days to 8 months) with idiopathic clubfoot deformities of grade II, III, or IV. Twenty-seven feet (19 patients) had not received any treatment before. Twelve patients (17 feet) had had unsuccessful prior conservative treatment elsewhere. All patients had manipulation casting in accordance with the Ponseti technique, and percutaneous Achilles tenotomy was performed in the presence of persistent equinus. Maintenance of correction was obtained with the use of a foot abduction brace. The mean follow-up period was 18 months (range 6.5 to 40 months). Forty-two feet (95%, 29 patients) were treated successfully using the Ponseti method.[70]. All these studies validate our results.
Conclusion
We concluded that Ponseti treatment technique in children with ICTEV under the care of predominantly orthopedic surgeons had excellent to good outcomes even in low-resource settings like Pakistan.
References
- Baghdadi T, Bagheri N, Najafi A, Mansouri P, Farzan M. Ponseti Casting Method in Idiopathic Congenital Clubfoot and Its Correlation with Radiographic Features Abstract. Arch Bone Jt Surg. 2017;5(3):168-173 Ponseti Casting Method in Idiopathic Congenital Clubfoot and Its Correlation with Radiographic Features Abstract
- Chueire AJ, Carvalho Filho G, Kobayashi OY, Carrenho L. Treatment of congenital clubfoot using Ponseti method. Rev Bras Ortop. 2016;51(3):313-318. doi:10.1016/j.rboe.2015.06.020 PubMed | Crossref | Google Scholar
- Fcg F, Wgc N, Lu R, Lc G, et al. Treatment of congenital idiopathic clubfoot by the ponseti method. Experience children’s hospital martagao gesteira. Preliminary assessment. Rheumatol Orthop Med. 2018;3(2):1-4. doi:10.15761/ROM.1000148 Crossref | Google Scholar
- Fan H, Liu Y, Zhao L, et al. The Correlation of Pirani and Dimeglio Scoring Systems for Ponseti Management at Different Levels of Deformity Severity. Sci Rep. 2017;7(1):14578. doi:10.1038/s41598-017-14977-7
PubMed | Crossref | Google Scholar - Walter C, Sachsenmaier S, Wünschel M, Teufel M, Götze M. Clubfoot treatment with Ponseti method-parental distress during plaster casting. J Orthop Surg Res. 2020;15(1):271. doi:10.1186/s13018-020-01782-8
PubMed | Crossref | Google Scholar - Smythe T, Chandramohan D, Bruce J, Kuper H, Lavy C, Foster A. Results of clubfoot treatment after manipulation and casting using the Ponseti method: experience in Harare, Zimbabwe. Trop Med Int Health. 2016;21(10):1311-1318. doi:10.1111/tmi.12750 PubMed | Crossref | Google Scholar
- Kaewpornsawan K, Khuntisuk S, Jatunarapit R. Comparison of modified posteromedial release and complete subtalar release in resistant congenital clubfoot: a randomized controlled trial. J Med Assoc Thai. 2007;90(5):936-941 Comparison of modified posteromedial release and complete subtalar release in resistant congenital clubfoot: a randomized controlled trial
- Celebi L, Muratli HH, Aksahin E, Yagmurlu MF, Bicimoglu A. Bensahel et al. and International Clubfoot Study Group evaluation of treated clubfoot: assessment of interobserver and intraobserver reliability. J Pediatr Orthop B. 2006;15(1):34-36. doi:10.1097/01202412-200601000-00007 PubMed | Crossref | Google Scholar
- Zimny ML, Willig SJ, Roberts JM, D’Ambrosia RD. An electron microscopic study of the fascia from the medial and lateral sides of clubfoot. J Pediatr Orthop. 1985;5(5):577-581. doi:10.1097/01241398-198509000-00014
PubMed | Crossref | Google Scholar - Inclan A. Clubfoot (Talipes). Medscape. 2023 Clubfoot (Talipes)
- Robertson WW Jr, Corbett D. Congenital clubfoot. Month of conception. Clin Orthop Relat Res. 1997;(338):14-18. doi:10.1097/00003086-199705000-00004 PubMed | Crossref | Google Scholar
- Parker SE, Mai CT, Strickland MJ, et al. Multistate study of the epidemiology of clubfoot. Birth Defects Res A Clin Mol Teratol. 2009;85(11):897-904. doi:10.1002/bdra.20625 PubMed | Crossref | Google Scholar
- Paton RW, Freemont AJ. A clinicopathological study of idiopathic CTEV. J R Coll Surg Edinb. 1993;38(2):108-109 A clinicopathological study of idiopathic CTEV
- Weymouth KS, Blanton SH, Powell T, Patel CV, Savill SA, Hecht JT. Functional Assessment of Clubfoot Associated HOXA9, TPM1, and TPM2 Variants Suggests a Potential Gene Regulation Mechanism. Clin Orthop Relat Res. 2016;474(7):1726-1735. doi:10.1007/s11999-016-4788-1 PubMed | Crossref | Google Scholar
- Pavone V, Chisari E, Vescio A, Lucenti L, Sessa G, Testa G. The etiology of idiopathic congenital talipes equinovarus: a systematic review. J Orthop Surg Res. 2018;13(1):206. doi:10.1186/s13018-018-0913-z PubMed | Crossref | Google Scholar
- Wang H, Barisic I, Loane M, et al. Congenital clubfoot in Europe: A population-based study.
Am J Med Genet A. 2019;179(4):595-601. doi:10.1002/ajmg.a.61067 PubMed | Crossref | Google Scholar - Zionts LE, Jew MH, Ebramzadeh E, Sangiorgio SN. The Influence of Sex and Laterality on Clubfoot Severity. J Pediatr Orthop. 2017;37(2):e129-133. doi:10.1097/BPO.0000000000000603 PubMed | Crossref | Google Scholar
- Chaudhry S, Chu A, Labar AS, Sala DA, van Bosse HJ, Lehman WB. Progression of idiopathic clubfoot correction using the Ponseti method. J Pediatr Orthop B. 2012;21(1):73-78. doi:10.1097/BPB.0b013e328346c03b
PubMed | Crossref | Google Scholar - Morcuende JA, Abbasi D, Dolan LA, Ponseti IV. Results of an accelerated Ponseti protocol for clubfoot. J Pediatr Orthop. 2005;25(5):623-626. doi:10.1097/01.bpo.0000162015.44865.5e PubMed | Crossref | Google Scholar
- Ponseti IV. Relapsing clubfoot: causes, prevention, and treatment. Iowa Orthop J. 2002;22:55-56 Relapsing clubfoot: causes, prevention, and treatment
- Ponseti IV. Clubfoot management. J Pediatr Orthop. 2000;20(6):699-700. doi:10.1097/00004694-200011000-00001 PubMed | Crossref | Google Scholar
- Haft GF, Walker CG, Crawford HA. Early clubfoot recurrence after use of the Ponseti method in a New Zealand population. J Bone Joint Surg Am. 2007;89(3):487-493. doi:10.2106/JBJS.F.00169 PubMed | Crossref | Google Scholar
- Dobbs MB, Corley CL, Morcuende JA, Ponseti IV. Late recurrence of clubfoot deformity: a 45-year followup. Clin Orthop Relat Res. 2003;(411):188-192. doi:10.1097/01.blo.0000065837.77325.19 PubMed | Crossref | Google Scholar
- Simons GW. Calcaneocuboid joint deformity in talipes equinovarus: an overview and update.
J Pediatr Orthop B. 1995;4(1):25-35. doi:10.1097/01202412-199504010-00004 PubMed | Crossref | Google Scholar - Simons GW. A standardized method for the radiographic evaluation of clubfeet. Clin Orthop Relat Res. 1978;(135):107-118 PubMed | Crossref | Google Scholar
- McCahill JL, Stebbins J, Harlaar J, Prescott R, Theologis T, Lavy C. Foot function during gait and parental perceived outcome in older children with symptomatic club foot deformity. Bone Jt Open. 2020;1(7):384-391. doi:10.1302/2633-1462.17.BJO-2020-0046.R1 PubMed | Crossref | Google Scholar
- Richards BS, Faulks S, Rathjen KE, Karol LA, Johnston CE, Jones SA. A comparison of two nonoperative methods of idiopathic clubfoot correction: the Ponseti method and the French functional (physiotherapy) method. J Bone Joint Surg Am. 2008;90(11):2313-2321. doi:10.2106/JBJS.G.01621 PubMed | Crossref | Google Scholar
- Jeans KA, Erdman AL, Karol LA. Plantar Pressures After Nonoperative Treatment for Clubfoot: Intermediate Follow-up at Age 5 Years. J Pediatr Orthop. 2017;37(1):53-58. doi:10.1097/BPO.0000000000000589
PubMed | Crossref | Google Scholar - Parada SA, Baird GO, Auffant RA, Tompkins BJ, Caskey PM. Safety of percutaneous tendoachilles tenotomy performed under general anesthesia on infants with idiopathic clubfoot. J Pediatr Orthop. 2009;29(8):916-919. doi:10.1097/BPO.0b013e3181c18ab5 PubMed | Crossref | Google Scholar
- Pavone V, Testa G, Costarella L, Pavone P, Sessa G. Congenital idiopathic talipes equinovarus: an evaluation in infants treated by the Ponseti method. Eur Rev Med Pharmacol Sci. 2013;17(19):2675-2679 Congenital idiopathic talipes equinovarus: an evaluation in infants treated by the Ponseti method
- Miller NH, Carry PM, Mark BJ, et al. Does Strict Adherence to the Ponseti Method Improve Isolated Clubfoot Treatment Outcomes? A Two-institution Review. Clin Orthop Relat Res. 2016;474(1):237-243. doi:10.1007/s11999-015-4559-4 PubMed | Crossref | Google Scholar
- Sangiorgio SN, Ho NC, Morgan RD, Ebramzadeh E, Zionts LE. The Objective Measurement of Brace-Use Adherence in the Treatment of Idiopathic Clubfoot. J Bone Joint Surg Am. 2016;98(19):1598-1605. doi:10.2106/JBJS.16.00170
PubMed | Crossref | Google Scholar - Jeans KA, Karol LA, Erdman AL, Stevens WR Jr. Functional outcomes following treatment for clubfoot: Ten-year follow-up. J Bone Joint Surg Am.2018;100(23):2015-2023. doi:10.2106/JBJS.18.00317 PubMed | Crossref | Google Scholar
- Sriharsha Y, Balaji G, Bharathi D, Patro DK. Do the clinical scores (Pirani and Dimeglio scores) correlate with the radiological parameters in idiopathic club foot in infants? A cross-sectional study. J Pediatr Orthop B. 2021;30(5):471-477. doi:10.1097/BPB.0000000000000835 Crossref
- Zionts LE, Sangiorgio SN, Cooper SD, Ebramzadeh E. Does Clubfoot Treatment Need to Begin As Soon As Possible?. J Pediatr Orthop. 2016;36(6):558-564. doi:10.1097/BPO.0000000000000514 Crossref | Google Scholar
- Jeans KA, Erdman AL, Jo CH, Karol LA. A Longitudinal Review of Gait Following Treatment for Idiopathic Clubfoot: Gait Analysis at 2 and 5 Years of Age. J Pediatr Orthop. 2016;36(6):565-571. doi:10.1097/BPO.0000000000000515
PubMed | Crossref - Dyer PJ, Davis N. The role of the Pirani scoring system in the management of club foot by the Ponseti method. J Bone Joint Surg Br. 2006;88(8):1082-1084. doi:10.1302/0301-620X.88B8.17482 PubMed | Crossref | Google Scholar
- Cummings RJ. The effectiveness of botulinum A toxin as an adjunct to the treatment of clubfeet by the Ponseti method: a randomized, double blind, placebo controlled study. J Pediatr Orthop. 2009;29(6):564-569. doi:10.1097/BPO.0b013e3181b2f21d PubMed | Crossref | Google Scholar
- Ahmad AA, Aker L. Accelerated Ponseti method: First experiences in a more convenient technique for patients with severe idiopathic club feet. Foot Ankle Surg. 2020;26(3):254-257. doi:10.1016/j.fas.2019.03.003
PubMed | Crossref | Google Scholar - Gelfer Y, Hughes KP, Fontalis A, Wientroub S, Eastwood DM. A systematic review of reported outcomes following Ponseti correction of idiopathic club foot. Bone Jt Open. 2020;1(8):457-464. doi:10.1302/2633-1462.18.BJO-2020-0109.R1 PubMed | Crossref | Google Scholar
- Gray K, Pacey V, Gibbons P, Little D, Burns J. Interventions for congenital talipes equinovarus (clubfoot). Cochrane Database Syst Rev. 2014;2014(8):CD008602. doi:10.1002/14651858.CD008602.pub3 PubMed | Crossref | Google Scholar
- Dragoni M, Farsetti P, Vena G, Bellini D, Maglione P, Ippolito E. Ponseti Treatment of Rigid Residual Deformity in Congenital Clubfoot After Walking Age. J Bone Joint Surg Am. 2016;98(20):1706-1712. doi:10.2106/JBJS.16.00053 PubMed | Crossref | Google Scholar
- Liu YB, Li SJ, Zhao L, Yu B, Zhao DH. Timing for Ponseti clubfoot management: does the age matter? 90 children (131 feet) with a mean follow-up of 5 years. Acta Orthop. 2018;89(6):662-667. doi:10.1080/17453674.2018.1526534
PubMed | Crossref | Google Scholar - Muzzammil M, Mughal A, Qadir A, et al. Does malnutrition in clubfoot patients affect Ponseti technique and its outcome?. Int J Clin Pract. 2021;75(5):e13957. doi:10.1111/ijcp.13957 PubMed | Crossref | Google Scholar
- Hsu WK, Bhatia NN, Raskin A, Otsuka NY. Wound complications from idiopathic clubfoot surgery: a comparison of the modified Turco and the Cincinnati treatment methods. J Pediatr Orthop. 2007;27(3):329-332. doi:10.1097/BPO.0b013e3180340d86 PubMed | Crossref | Google Scholar
- Singh BI, Vaishnavi AJ. Modified Turco procedure for treatment of idiopathic clubfoot.
Clin Orthop Relat Res. 2005;438:209-214. doi:10.1097/01.blo.0000173251.77826.05 PubMed | Crossref | Google Scholar - Bensahel H, Csukonyi Z, Desgrippes Y, Chaumien JP. Surgery in residual clubfoot: one-stage medioposterior release “à la carte”. J Pediatr Orthop. 1987;7(2):145-148. doi:10.1097/01241398-198703000-00005
PubMed | Crossref | Google Scholar - Bensahel H, Jehanno P, Delaby JP, Themar-Noël C. Carpik ayağin konservatif tedavisi: Fonksiyonel Yöntem ve uzun dönemli izlem (Conservative treatment of clubfoot: the Functional Method and its long-term follow-up). Acta Orthop Traumatol Turc. 2006;40(2):181-186 Carpik ayağin konservatif tedavisi: Fonksiyonel Yöntem ve uzun dönemli izlem (Conservative treatment of clubfoot: the Functional Method and its long-term follow-up)
- Ferreira RC, Costa MT, Frizzo GG, Santin RA. Correction of severe recurrent clubfoot using a simplified setting of the Ilizarov device. Foot Ankle Int. 2007;28(5):557-568. doi:10.3113/FAI.2007.0557 PubMed | Crossref | Google Scholar
- Freedman JA, Watts H, Otsuka NY. The Ilizarov method for the treatment of resistant clubfoot: is it an effective solution?. J Pediatr Orthop. 2006;26(4):432-437. doi:10.1097/01.bpo.0000226276.70706.0e
PubMed | Crossref | Google Scholar - López-Carrero E, Castillo-López JM, Medina-Alcantara M, Domínguez-Maldonado G, Garcia-Paya I, Jiménez-Cebrián AM. Effectiveness of the Ponseti Method in the Treatment of Clubfoot: A Systematic Review. Int J Environ Res Public Health. 2023;20(4):3714. doi:10.3390/ijerph20043714 PubMed | Crossref | Google Scholar
- Gupta P, Bither N. Ilizarov in relapsed clubfoot: a necessary evil?. J Pediatr Orthop B. 2013;22(6):589-594. doi:10.1097/BPB.0b013e32836486de PubMed | Crossref | Google Scholar
- Altaf KA, Shah SBS, Ahmad S, Mumtaz U, Mantoo SA. Results of JESS (Joshi’s External Stabilizing System) in Relapsed, Neglected and Neurogenic Clubfoot in an Age Group of 2-10 Years. Ortop Traumatol Rehabil. 2020;22(2):121-129. doi:10.5604/01.3001.0014.1170 PubMed | Google Scholar
- Gray K, Burns J, Little D, Bellemore M, Gibbons P. Is tibialis anterior tendon transfer effective for recurrent clubfoot?. Clin Orthop Relat Res. 2014;472(2):750-758. doi:10.1007/s11999-013-3287-x
PubMed | Crossref | Google Scholar - Graham GP, Dent CM. Dillwyn Evans operation for relapsed club foot. Long-term results. J Bone Joint Surg Br. 1992;74(3):445-448. doi:10.1302/0301-620X.74B3.1587899 Crossref | Google Scholar
- Schlegel UJ, Batal A, Pritsch M, et al. Functional midterm outcome in 131 consecutive cases of surgical clubfoot treatment. Arch Orthop Trauma Surg. 2010;130(9):1077-1081. doi:10.1007/s00402-009-0948-z
PubMed | Crossref | Google Scholar - Cooper DM, Dietz FR. Treatment of idiopathic clubfoot. A thirty-year follow-up note. J Bone Joint Surg Am. 1995;77(10):1477-1489. doi:10.2106/00004623-199510000-00002 PubMed | Crossref | Google Scholar
- Wallander H, Larsson S, Bjönness T, Hansson G. Patient-reported outcome at 62 to 67 years of age in 83 patients treated for congenital clubfoot. J Bone Joint Surg Br. 2009;91(10):1316-1321. doi:10.1302/0301-620X.91B10.22796
PubMed | Crossref | Google Scholar - Richards BS, Faulks S, Razi O, Moualeu A, Jo CH. Nonoperatively Corrected Clubfoot at Age 2 Years: Radiographs Are Not Helpful in Predicting Future Relapse. J Bone Joint Surg Am. 2017;99(2):155-160. doi:10.2106/JBJS.16.00693
PubMed | Crossref | Google Scholar - Little Z, Yeo A, Gelfer Y. Poor Evertor Muscle Activity Is a Predictor of Recurrence in Idiopathic Clubfoot Treated by the Ponseti Method: A Prospective Longitudinal Study With a 5-Year Follow-up. J Pediatr Orthop. 2019;39(6):e467-471. doi:10.1097/BPO.0000000000001357 PubMed | Crossref
- Penny JN. The neglected clubfoot. Tech Orthop. 2005;20(2):153–166 The Neglected Clubfoot
- Cartlidge I. Observations on the epidemiology of club foot in Polynesian and Caucasian populations. J Med Genet. 1984;21(4):290-292. doi:10.1136/jmg.21.4.290 PubMed | Crossref | Google Scholar
- Chung CS, Nemechek RW, Larsen IJ, Ching GH. Genetic and epidemiological studies of clubfoot in Hawaii. General and medical considerations. Hum Hered. 1969;19(4):321-342. doi:10.1159/000152236
PubMed | Crossref | Google Scholar - Owen RM, Penny JN, Mayo A, Morcuende J, Lavy CB. A collaborative public health approach to clubfoot intervention in 10 low-income and middle-income countries: 2-year outcomes and lessons learnt. J Pediatr Orthop B. 2012;21(4):361-365. doi:10.1097/BPB.0b013e3283504006 PubMed | Crossref | Google Scholar
- Giesberts RB, Hekman EEG, Maathuis PGM, Verkerke GJ. Quantifying the Ponseti method.
J Mech Behav Biomed Mater. 2017;66:45-49. doi:10.1016/j.jmbbm.2016.10.021 PubMed | Crossref | Google Scholar - Staheli L, Ponseti I, et al. Clubfoot: Ponseti Management. eBook. GHO Publications; 2009 Clubfoot: Ponseti Management
- Abbas M, Qureshi OA, Jeelani LZ, Azam Q, Khan AQ, Sabir AB. Management of congenital talipes equinovarus by Ponseti technique: a clinical study. J Foot Ankle Surg. 2008;47(6):541-545. doi:10.1053/j.jfas.2008.07.002
PubMed | Crossref | Google Scholar - Sahito B, Rasheed N, Kumar D, Tariq SM, Soomro ZE, Ali M. Experience of treating the Talipes equinovarus deformity with Ponsetti technique at district level. J Pak Med Assoc.
2019;69(Suppl 1):S25-28 Experience of treating the Talipes equinovarus deformity with Ponsetti technique at district level - Verma A, Mehtani A, Sural S, et al. Management of idiopathic clubfoot in toddlers by Ponseti’s method. J Pediatr Orthop B. 2012;21(1):79-84. doi:10.1097/BPB.0b013e328347a329 PubMed | Crossref | Google Scholar
- Göksan SB. Doğuştan çarpik ayağin Ponseti yöntemi ile tedavisi (Treatment of congenital clubfoot with the Ponseti method). Acta Orthop Traumatol Turc. 2002;36(4):281-287 Treatment of congenital clubfoot with the Ponseti method
Acknowledgments
I offer humble thanks for conducting a study of this magnitude, which would not have been possible without the constant help and guidance of my Supervisor, Prof. Dr. Muhammad Ayaz Khan. I also thank my colleagues for their help in literature review writing and data analysis.
Funding
The authors declared no funding was received for the study.
Author Information
Corresponding Author:
Sohail Rehman
Department of Orthopedic Surgery
Registrar, Global Medics Ireland
Email: sann090909@gmail.com
Co-Authors:
Zia Ullah Jan, Talha Anwar, Muhammad Ayaz Khan
Department of Orthopaedic
Khyber Teaching Hospital Peshawar, Pakistan
Asif Nawaz
Department of Orthopaedic & Trauma
Khyber Teaching Hospital Peshawar, Pakistan
Musawer Iqbal
Department of Orthopaedic
University Hospital Waterford, Ireland
Authors Contributions
All authors contributed to the conceptualization, investigation, and data curation by acquiring and critically reviewing the selected articles. They were collectively involved in the writing – original draft preparation, and writing – review & editing to refine the manuscript. Additionally, all authors participated in the supervision of the work, ensuring accuracy and completeness. The final manuscript was approved by all named authors for submission to the journal.
Ethical Approval
Study was conducted after approval (262/DME/KMC) of the institutional research ethical board of Khyber medical college/Khyber teaching hospital, Pakistan.
Conflict of Interest Statement
The authors declare no conflict of interest.
Guarantor
None
DOI
Cite this Article
Sohail R, Zia UJ, Asif N, Musawer I, Talha A, Muhammad AK. Evaluation of the Outcomes of Ponseti Method in the Treatment of Idiopathic Congenital Clubfoot Deformity in Tertiary Care Hospital of Pakistan: A Descriptive Study. medtigo J Med. 2025;3(1):e3062318. doi:10.63096/medtigo3062318 Crossref













