







 Author Affiliations
Author Affiliations
Abstract
Background: Esophageal carcinoma is one of the painful and excruciating sufferings among patients that affects around 5.3% of all global cancer deaths. Most of the patients undergo a percutaneous endoscopic gastrostomy (PEG) tube procedure, which makes them prone to nutritional discrepancies. A PEG tube can result in severe problems when sufficient and proper care is not provided.
Aim: The study aimed to assess the effect of demonstration on the caregivers’ practices regarding percutaneous endoscopic gastrostomy tube feeding of patients diagnosed with esophageal carcinoma.
Methods: A quasi-experimental design was used to evaluate the caregivers’ practices regarding percutaneous endoscopic gastrostomy tube feeding among their patients. The study was conducted in the Institute of radiotherapy and nuclear medicine (IRNUM) Hospital, Peshawar. A total of 60 caregivers of esophageal carcinoma patients were taken as a sample size. A validated 12-item checklist was used to evaluate the practices of caregivers regarding gastrostomy tube feeding of their patients diagnosed with esophageal carcinoma.
Results: There was an increase in the number of patients with good practices from 20% to 40% and a decrease in configuration in poor practices from 45 % to 22 % after the skill demonstration. The patient’s practices were significantly improved (0.000), indicating the positive effect of the nursing intervention. Moreover, the demographic variables showed no significant correlation with the participants’ practices.
Conclusion: The study concluded that the demonstration regarding percutaneous endoscopic gastrostomy tube feeding was helpful and had a positive impact on improving the practices of caregivers to feed their patients living with esophageal carcinoma. Therefore, health care professionals need to be well-equipped to train caregivers to feed their patients with percutaneous endoscopic gastrostomy at home.
Keywords
Esophageal carcinoma, Caregivers, Practices, Gastrostomy tube, Feeding.
Introduction
PEG tube feeding has a vital role in managing those patients who do not take oral nutrition properly. The main aim of the PEG insertion is to provide a route to the stomach for feeding. The patient must have a normal gastrointestinal function before inserting the PEG tube. The beneficial effect of the PEG tube feeding on patients is to increase the survival of patients.[1] Proper nutrition is vital for carcinoma patients prior to, during, and following treatment.[2] Nutritional therapy is essential for cancer patients, if the patient does not receive enough and proper nutrition it can cause severe ailments and sufferings during and after treating cancer patients.[3]
Malnutrition occurs in 79% of patients with esophageal carcinoma. At the time of diagnosis, the patient presented with body loss and difficulty swallowing. Improper management of dysphagia leads the patients to further complications.[4] Approximately 21.3% of patients developed aspiration pneumonia with eating dysfunction caused by esophageal carcinoma. The treatment of localized cancer of the esophagus has been the subject of controversy in recent decades.[5] Neoadjuvant therapy was used empirically, but the evidence was limited due to a lack of high-quality confirmation.[6] For quality care and minimizing complications, family caregivers must receive thorough education and training about tube feeding before discharge from the hospital.[7]
The PEG can lead to many problems if enough postoperative care is not provided. These contain mechanical complications such as blockage of the tube and tube loss associated with hyperstoma granulation and buried bumper syndrome.[8] Gastrointestinal tract (GIT) complications include nausea, vomiting, increased residual gastric volume, diarrhea, and abdominal distension or metabolic irregularities due to under or overfeeding and infection of the stoma.[9]
PEG is an easy-to-perform, low-risk, and greatly trusted long-term enteral feeding modality in patients with head and neck cancer.[10] PEG tube insertion is a commonly used method in clinical practices among patients with esophageal carcinoma. PEG tube feeding is a safe and successful technique for feeding patients with swallowing impairment.[11] Most of the patients diagnosed with esophageal cancer are usually dependent on their family caregivers. The British artificial nutrition survey result shows that 59% of recently registered elderly need partial or complete support. It means that if this help and support is not available, they cannot perform activities of daily living independently, and their health may worsen.[12]
The responsibilities of the family caregivers are to take care of hygiene, dressing changes, administer medicine, and provide nutrition to their patients. Due to advancements in the medical discipline, percutaneous endoscopic gastrostomy procedures are performed via endoscope around the globe, and approximately 100,000 to 125,000 procedures are done yearly in the USA alone. [13,14]
Methodology
Quantitative experimental design (pretest and posttest research design) was used for the current study. The study was conducted at the IRNUM. Data was collected from the caregivers (family members who provide regular care to their patient) of esophageal carcinoma patients at the IRNUM Peshawar. The sample size was 60 caregivers of esophageal carcinoma patients who were on percutaneous endoscopic gastrostomy tube feeding.
Demonstration intervention and protocol: The patient who was diagnosed with esophageal carcinoma was approached within the first 24 hours of admission. First, the patient was assessed for inclusion criteria, then the aim and objectives of the study were explained to each patient, and after agreement and signing the informed consent, the patient was included in this study. The pre-test data from each caregiver was collected using the validated checklist.
The intervention was the checklist that proposed twelve steps with correct/incorrect responses for feeding the patient with a percutaneous endoscopic gastrostomy tube. After the pre-test data, the intervention was demonstrated using the twelve-step checklist step by step to the caregiver for their patient, which took 15 minutes of time. After two weeks, the caregiver was approached to demonstrate the steps of intervention, so for the correct step, the caregiver was scored “1”, while for the incorrect step, the caregiver was scored “0”.
The intervention was validated by three experts working in the gastro-oncology unit. While a pilot study was conducted that revealed the KR-20 score of 0.81, which represents good reliability.
Data collection procedure: Data was collected from all participants of the study through a questionnaire. The study instrument had two parts. The first part had demographic information, including age, gender, qualification, Relationship with Patient, Employment Status, etc. While 2nd part was consisted of 12 items having correct / incorrect answers. This study was conducted in three phases: assessment, pre-intervention phase, implementation phase, and evaluation post-intervention phase. Data was collected pre/post demonstration.
Data analysis procedure: The data was analyzed using statistical package for the social sciences (SPSS) software Version-22. Frequencies and percentages were calculated for categorical variables, while the mean and standard deviation of continuous variables. Paired t-test was applied to identify the difference between pre-test score and post-test score, while chi-square test was applied to identify the association of knowledge with demographic variables. The scoring rate for this checklist was scored above 80%. = Good Practices, score between 60-79% = Average Practices and score Less than 59% = Poor Practices.
Ethical consideration: First the subject of the review was endorsed by the institute of nursing sciences (INS), Khyber Clinical College. Furthermore, the study was approved by the advance studies and research board (ASRB) and ethical review board (ERB). Participants were made aware of the study’s goals and objectives in detail.
Before the data was collected, consent forms were signed by the participants. A separate room was used for data collection to protect privacy. The participants were made aware that the study would never harm or benefit any of them. Only the primary author can evaluate the data, which was password protected.
Results
Demographic characteristic of study participants: The total participant of the study was 60, where the number of male participants was high compared to female participants (Table 1).
| Variable | Categories | Frequency(n-60) | Percentage |
| Age | 20 – 29 30 – 39 40 -49 50 and above |
18 12 15 15 |
30 % 20 % 25 % 25 % |
| Gender | Male Female |
44 16 |
73 % 27 % |
| Marital status | Single Married |
18 42 |
30% 70% |
| Education
|
Illiterate Primary Secondary Higher school University |
20 06 02 19 13 |
33 % 10 % 03 % 31 % 21 % |
| Relationship
|
Wife Husband Parent Sibling In-laws |
07 06 23 15 09 |
12 % 10 % 38 % 25 % 15 % |
| Employment status | Employed Unemployed Retired |
29 31 00 |
48 % 52 % 00 % |
| Previous training | Yes No |
48 12 |
80 % 20 % |
| Training received from
|
Doctors Nursing staff Technical staff Others |
02 42 04 00 |
04 % 88 % 08 % 00 % |
| Duration of PEG | Less than one month 2 months 3 months More than 3 months |
17 08 08 27 |
29 % 13 % 13 % 45 % |
Table 1: Demographic data of the participants
Comparison of the pre-test and post-test practices: Table 2 illustrates that the post-test mean score of the patients was increased (77.2 ± 13.3) compared to the pre-test score (67.7 ± 12.2). Therefore, the intervention was significant (0.000) (Table 2). Table 2: Pre- and post-test analysis with cutoff valuesFigure 1 reveals that the number of good practices in post-patients increased to (n-24) from the pre-test number (n-12), while the number of poor practices in patients in the pre-test (n-27) decreased to (n-13) in the post-test. That shows the effectiveness of nursing intervention (Figure 1).
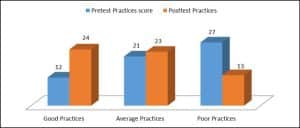
Figure 1: Pre-test and post-test comparison of the practices
Association of pre-practice scores with demographics: The demographic variables show no association with the feeding practices of patients, except previous training (Table 3).Table 3: Association of the pre-practice score with demographics of the participants
| Variable | Categories | Frequency(n-60) | Percentage |
|
Age |
20 – 29 30 – 39 40 -49 50 and above |
18 12 15 15 |
30 % 20 % 25 % 25 % |
| Gender | Male Female |
44 16 |
73 % 27 % |
| Marital status | Single Married |
18 42 |
30% 70% |
| Education
|
Illiterate Primary Secondary Higher school University |
20 06 02 19 13 |
33 % 10 % 03 % 31 % 21 % |
| Relationship
|
Wife Husband Parent Sibling In-laws |
07 06 23 15 09 |
12 % 10 % 38 % 25 % 15 % |
| Employment status | Employed Unemployed Retired |
29 31 00 |
48 % 52 % 00 % |
| Previous training | Yes No |
48 12 |
80 % 20 % |
| Training received from
|
Doctors Nursing staff Technical staff Others |
02 42 04 00 |
04 % 88 % 08 % 00 % |
| Duration of PEG | Less than one month 2 months 3 months More than 3 months |
17 08 08 27 |
29 % 13 % 13 % 45 % |
| Mean |
Standard deviation (SD) | Standard error mean | t-test (T) | degrees of freedom (df) | Sig (2 Tail) | |
| Pre-test | 67.7000 | 12.24036 | 2.2347 | -11.977 | 59 | 0.000 |
| Post-test | 77.2000 | 13.35906 | 2.43902 | |||
| Pre & post | -9.50000 | 6.14376 | 0.79316 |
| Association of practices with age | |||||||
| Age | Category | Poor | Average | Good | df | Chi square | P value |
| 20-29 | 7 | 6 | 5 | 6
|
0.355
|
0.113 | |
| 30-39 | 6 | 4 | 4 | ||||
| 40-49 | 4 | 7 | 2 | ||||
| Above 50 | 10 | 4 | 1 | ||||
| Association of pre-practice scores with the qualification | |||||||
| Qualification | Category | Poor | Average | Good | df | Chi square | P value |
| Illiterate | 12 | 7 | 2 |
8 |
8.840 |
0.356 |
|
| Primary | 4 | 2 | |||||
| Secondary | 1 | 1 | |||||
| High School | 7 | 6 | 5 | ||||
| University | 3 | 5 | 5 | ||||
| Association of pre-practice score with gender | |||||||
| Gender | Category | Poor | Average | Good | df | Chi square | P value |
| Male | 19 | 15 | 10 |
2 |
0.774 |
0.679 |
|
| Female | 8 | 6 | 2 | ||||
| Association of pre-practice score with previous training | |||||||
| Previous training |
Category | Poor | Average | Good | df | Chi square | P value |
| Received | 17 | 20 | 11 |
2 |
8.967 |
0.011 |
|
| Not Received | 10 | 1 | 1 | ||||
| Association of pre-practice score with previous training received from | |||||||
| Training received from | Category | Poor | Average | Good | df | Chi square | P value |
| Nurse | 13 | 19 | 10 |
4 |
4.926 |
0.295 |
|
| Doctor | 1 | 0 | 1 | ||||
| Technical staff | 3 | 1 | 0 | ||||
Discussion
The current study shows that more than two-thirds of the studied participants were male. This result followed the investigations.[15] This document states that approximately 60 percent of the surveyed participants were male in their study. According to the literature, approximately 60 percent of the surveyed participants were male in their study. [16] The result of the study findings showed that most of the participants were from the age of 20-29 (30%), followed by 30-39 (20%), 40-49 (25%), and above 50 (25%) While the result is contradictory to a study, in which 40 % of the participants were below the age of 30 years.[17] The study findings showed that one-third of the participants were illiterate and had no formal education. These findings were found parallel in their nature with one of the studies conducted previously, which documented that less than half of the studied participants were illiterate and untrained.[18]
The study showed that the primary caregivers (38%) for PEG tube patients at home were parents. One of the previous studies has shown contrasting results in association with the current study findings, which reported that the primary caregivers were their own offspring in the majority of the cases, other than their other relative members.[19] Literature shows none of the specified reasons for the discrepancy, explaining why the other caregivers were involved in care other than parents. The present study shows that half of the studied participants had a PEG tube insertion duration of more than three months, according to another study.[20] which claimed that the mean treatment time of esophageal cancer was longer than one year. The result shows statistically significant differences in the practice scores of caregivers before and after attending the demonstration regarding percutaneous endoscopic gastrostomy tube feeding. In comparing pre- and post-test practice scores via paired t-test, there was a highly significant difference with a p-value of 0.000. These findings were like the result of a study in which there was a highly significant difference with a p-value of 0.000.[21] Similarly, another study’s results revealed a highly significant association with a p-value of 0.000 among pre- and post-test score comparisons.[22]
The results show an improvement in the caregivers’ practices regarding PEG tube feeding. This result was not in agreement with another study. This shows no significant differences between physicians and nurses after practical training.[23] The present study shows that 45% of the participants in the pre-test scored poorly, 35% obtained an average practice score, and only 20% obtained a good practice score. The results of the current study are comparable to the findings of a study in which 40% of the participants in the pre-test scored poorly, 50% obtained an average score, and 10% obtained a good score. Similarly, another study revealed that 46.7% scored poorly, while 43.3% obtained an average score.[24,25]
The present study shows that 22% of the participants in the post-test scored poorly, 38% obtained an average practice score, and 40% got good practice. Achieve the results of the current study are comparable to the finding of a study in which 10 % of the participants in the post-test scored poorly, 47% obtained an average score, and 43% got a good score The demonstration was highly productive for the participants and showed a significant improvement in the post-practices scores.[26] It is the opinion of the investigator that the important responsibility of nurses concerning client and family caregivers is to train them through educational sessions to improve the quality of client care, particularly cancer patients. Further research is needed to carefully guide caregivers during percutaneous gastrostomy tube feeding. Nurses play an important part in the early identification of risks and complications in patients. The educational program is essential to ensure the regular provision of the best nursing care.[27]
Limitation of the study: The study was conducted carefully and comprehensively in the required research setting. However, it was limited to only a single entity of the health care settings; therefore, the study may be conducted in more settings to have added findings to the pool of information.
Conclusion
The current study findings reflect that the caregivers of esophageal carcinoma patients in Pakistan had a poor level of practice, as reported in the pre-demonstration phase of percutaneous endoscopic gastrostomy tube feeding techniques. Thus, there is a significant need to educate caregivers. After the administration of a proper demonstration of PEG feeding protocols, the mean post-test practice score increased, as the majority of the study participants scored well; it seems that the demonstration was highly effective in improving the practices of caregivers. The demonstration regarding PEG tube feeding was helpful in improving the caregivers’ practice.
Hospital administration needs to play a role in patient-caregiver education and skills improvement programs at clinical settings. Healthcare providers and nurses need to give frequent demonstrations of PEG tube feeding to patients’ caregivers. Policy makers and regulatory bodies should take proper steps to devise policies and procedures for caregivers’ awareness of PEG feeding practices to fulfill the nutritional and medicinal needs of patients. The regulators should be involved in adding appropriate interventions and study materials regarding PEG feeding in the nursing curricula for the betterment of such patients.
References
- Pars H, Çavuşoğlu H. A literature review of percutaneous endoscopic gastrostomy: dealing with complications. Gastroenterol Nurs. 2019;42(4):351-359. doi:10.1097/SGA.0000000000000320 PubMed | Crossref | Google Scholar
- de Las Peñas R, Majem M, Perez-Altozano J, et al. SEOM clinical guidelines on nutrition in cancer patients (2018). Clin Transl Oncol. 2019;21(1):87-93. doi:10.1007/s12094-018-02009-3. PubMed | Crossref | Google Scholar
- Ravasco P. Nutrition in cancer patients. J Clin Med. 2019;8(8):1211. doi:10.3390/jcm8081211
PubMed | Crossref | Google Scholar - Montoro-Huguet MA. Dietary and nutritional support in gastrointestinal diseases of the upper gastrointestinal tract (I): esophagus. Nutrients. 2022;14(22):4819. doi:10.3390/nu14224819 PubMed | Crossref | Google Scholar
- Lambert A, Schwarz L, Ducreux M, Conroy T. Neoadjuvant treatment strategies in resectable pancreatic cancer. Cancers (Basel). 2021;13(18):4724. doi:10.3390/cancers13184724 PubMed | Crossref | Google Scholar
- Kawata S, Hiramatsu Y, Shirai Y, et al. Multidisciplinary team management for prevention of pneumonia and long-term weight loss after esophagectomy: a single-center retrospective study. Esophagus. 2020;17(3):270-278. doi:10.1007/s10388-020-00721-0. PubMed | Crossref | Google Scholar
- Mahran GS, Mohammed MA. Effect of high gastric residual volume on critically ill patients’ outcomes. Assiut Sci Nurs J. 2021;9(26):95-102. doi:10.21608/asnj.2021.90425.1219 Crossref | Google Scholar
- Pars H, Çavuşoğlu H. A literature review of percutaneous endoscopic gastrostomy: dealing with complications. Gastroenterol Nurs. 2019;42(4):351-359. doi:10.1097/SGA.0000000000000320 PubMed | Crossref | Google Scholar
- Swinson BD, Witherow H, Amin M, Kalavrezos N, Newman L. Principles of management in oral cancer. Hosp Med. 2003;64(7):404-410. doi:10.12968/hosp.2003.64.7.2277 PubMed | Crossref | Google Scholar
- Anderson NJ. Improving dysphagia quality of life outcomes in patients receiving head and neck radiotherapy. Monash University; 2021. Improving dysphagia quality of life outcomes in patients receiving head and neck radiotherapy
- Liang J, Jiang Y, Abboud Y, Gaddam S. Role of endoscopy in management of upper gastrointestinal cancers. Diseases. 2022;11(1):3. doi:10.3390/diseases11010003 PubMed | Crossref | Google Scholar
- Abdi S, Spann A, Borilovic J, de Witte L, Hawley M. Understanding the care and support needs of older people: a scoping review and categorisation using the WHO international classification of functioning, disability and health framework (ICF). BMC Geriatr. 2019;19(1):195. doi:10.1186/s12877-019-1189-9 PubMed | Crossref | Google Scholar
- Teixeira MJC, Abreu W, Costa N, Maddocks M. Understanding family caregivers’ needs to support relatives with advanced progressive disease at home: an ethnographic study in rural Portugal. BMC Palliat Care. 2020;19(1):73. doi:10.1186/s12904-020-00583-4. PubMed | Crossref | Google Scholar
- Elsaid Hussein ES, Mohamed Abu Negm LM. Nursing-based guidelines for caregivers regarding adult patients with percutaneous endoscopic gastrostomy. Open Nurs J. 2020;14(1):1-9. doi:10.2174/1874434602014010148
Crossref | Google Scholar - Ryan J, Lopian L, Le B, et al. It’s not raining men: a mixed-methods study investigating methods of improving male recruitment to health behaviour research. BMC Public Health. 2019;19(1):814. doi:10.1186/s12889-019-7087-4
PubMed | Crossref | Google Scholar - Islam MS, Siddique AB, Akter R, et al. Knowledge, attitudes and perceptions towards COVID-19 vaccinations: a cross-sectional community survey in Bangladesh. BMC Public Health. 2021;21(1):1851. doi:10.1186/s12889-021-11880-9
PubMed | Crossref | Google Scholar - Yu B, Chen X, Chen X, Yan H. Marijuana legalization and historical trends in marijuana use among US residents aged 12-25: results from the 1979-2016 National Survey on Drug Use and Health. BMC Public Health. 2020;20(1):156. doi:10.1186/s12889-020-8253-4 PubMed | Crossref | Google Scholar
- Kinyua AH. When the trainer is untrained: Stakeholder incapacitation in implementation and utilization of open educational resources in Kenya. J Learn Dev. 2021;8:171-181. doi:10.56059/jl4d.v8i1.396 Crossref | Google Scholar
- Homan M, Hauser B, Romano C, et al. Percutaneous endoscopic gastrostomy in children: an update to the ESPGHAN position paper. J Pediatr Gastroenterol Nutr. 2021;73(3):415-426. doi:10.1097/MPG.0000000000003207
PubMed | Crossref | Google Scholar - Hazzard E, Gulliver S, Walton K, McMahon AT, Milosavljevic M, Tapsell L. The patient experience of having a feeding tube during treatment for head and neck cancer: a systematic literature review. Clin Nutr ESPEN. 2019;33:66-85. doi:10.1016/j.clnesp.2019.07.005 PubMed | Crossref | Google Scholar
- McGuinness MJ, Hsee L. Impact of the COVID-19 national lockdown on emergency general surgery: Auckland City Hospital’s experience. ANZ J Surg. 2020;90(11):2254-2258. doi:10.1111/ans.16336 PubMed | Crossref | Google Scholar
- Gunasegaran P, Tahmina S, Daniel M, Nanda SK. Role of vitamin D-calcium supplementation on metabolic profile and oxidative stress in gestational diabetes mellitus: a randomized controlled trial. J Obstet Gynaecol Res. 2021;47(3):1016-1022. doi:10.1111/jog.14629 PubMed | Crossref | Google Scholar
- Kahveci G, Akin S. Knowledge levels and practices about the enteral nutritional practices of informal caregivers caring for patients fed through a percutaneous endoscopic gastrostomy tube: a descriptive observational study. Gastroenterol Nurs. 2021;44(5):E80-90. doi:10.1097/SGA.0000000000000623 PubMed | Crossref | Google Scholar
- Janelli M, Lipnevich A. Effects of pre-tests and feedback on performance outcomes and persistence in massive open online courses. Comput Educ. 2021;161:104076. doi:10.1016/j.compedu.2020.104076 Crossref | Google Scholar
- Wardani S. Improving student vocabulary mastery using word mapping strategy. OKARA J Bahasa Sastra. 2015;9(1):131-144. doi:10.19105/ojbs.v9i1.585 Crossref | Google Scholar
- Permatasari TAE, Rizqiya F, Kusumaningati W, Suryaalamsah II, Hermiwahyoeni Z. The effect of nutrition and reproductive health education of pregnant women in Indonesia using quasi-experimental study. BMC Pregnancy Childbirth. 2021;21(1):180. doi:10.1186/s12884-021-03676-x PubMed | Crossref | Google Scholar
- Burgdorf JG, Arbaje AI, Chase JA, Wolff JL. Current practices of family caregiver training during home health care: a qualitative study. J Am Geriatr Soc. 2022;70(1):218-227. doi:10.1111/jgs.17492 PubMed | Crossref | Google Scholar
Acknowledgments
Not reported
Funding
Not reported
Author Information
Corresponding Author:
Shah Hussain
Department of Nursing
Zalan College of Nursing, Swat, Pakistan
Email: [email protected]
Co-Authors:
Sardar Ali and Dildar Muhammad
Department of Nursing
Khyber Medical University Peshawar, Pakistan
Ejaz Hassan Khan
Department of Pathology
Gandhara University-Peshawar, Pakistan
Muhammad Anwar
Department of Nursing
Medtach College of Nursing Dir, Pakistan
Authors Contributions
All authors contributed to the conceptualization, investigation, and data curation by acquiring and critically reviewing the selected articles. They were collectively involved in the writing – original draft preparation, and writing – review & editing to refine the manuscript. Additionally, all authors participated in the supervision of the work, ensuring accuracy and completeness. The final manuscript was approved by all named authors for submission to the journal.
Informed Consent
Not applicable
Conflict of Interest Statement
The authors declare no conflict of interest.
Ethical Approval
This study was approved by the ethical board of Khyber Medical University, Peshawar.
Guarantor
None
DOI
Cite this Article
Shah H, Sardar A, Dildar M, Ejaz HK, Muhammad A. Effect of Demonstration Regarding Percutaneous Endoscopic Gastrostomy Tube Feeding among Caregivers of Patients Diagnosed with Esophageal Carcinoma. medtigo J Med. 2024;2(4):e30622465. doi:10.63096/medtigo30622465 Crossref













