






 Author Affiliations
Author Affiliations
Abstract
Childhood immune thrombocytopenia (ITP) affects approximately 5 in 100,000 children annually, characterized by autoimmune-mediated platelet destruction and impaired platelet production, resulting in low platelet counts. Approximately 20% of cases progress to a chronic course, defined by persistently low platelet counts (< 10 × 10^9/L) for over 12 months, often necessitating long-term immunosuppressive therapy, which increases susceptibility to infectious complications. We present a case of a 14-year-old obese female with chronic immune thrombocytopenic purpura treated with combined dexamethasone, vincristine, and elthrombopag. She presented with a 7-day history of acute fever and left hip pain, diagnosed with septic arthritis caused by Citrobacter freundii in the left hip, concurrent urinary tract infection due to Escherichia coli, and typhoid fever caused by Salmonella typhi. Surgical drainage of the purulent hip and broad-spectrum intravenous antibiotics for 3 weeks led to significant clinical improvement. Children undergoing long-term immunosuppressive therapy for chronic ITP are at heightened risk of serious concurrent infections, particularly in obese pediatric patients. Obesity’s association with osteoarthritis in weight-bearing joints may further exacerbate infection risks, underscoring the need for additional observational studies to better understand this relationship.
Keywords
Chronic ITP, Immunosuppressive therapy, Concurrent infection, Septic arthritis, Typhoid, Urinary Tract Infection.
Introduction
Childhood immune thrombocytopenic purpura (ITP) is an isolated thrombocytopenia that is secondary to increased destruction of platelets by the macrophages in the reticulo-endothelial system (RES), particularly the spleen, consequent to antibodies formed against platelets in response to a viral illness. It is the most common acquired bleeding disorder in children, with a prevalence of 5 in 100,000 [1]. ITP commonly affects children between one and seven years of age. Severe life-threatening bleeding is rare (0.2–0.9%) [2]. Childhood primary ITP usually benign, self-limiting course, with or without treatment. Complete remission occurs within six months from diagnosis, commonly within 6–12 weeks, in the majority of children with the diagnosis of ITP.
Around 20% pursue a chronic course, which is defined as a platelet count that has been < 10 ×109/L for longer than 12 months, with some cases requiring long-term immunosuppressive therapy, which can be prone to bacterial infection complications. In addition, obesity can have a marked impact on hip arthritis and osteoarthritis [3]. Here, we report on an obese adolescent girl who consequently developed severe concurrent infections by several different pathogens, following long-term treatment with combined immunosuppressive drugs for chronic immune thrombocytopenia. The objective of this presentation is to share the risk factors for this case and the success of a quick diagnosis and accurate management.
Case Presentation
A 14-year-old girl presented with a 7-day history of intermittent fever and vomiting several times, accompanied by progressive left hip pain associated with restricted movement. Therefore, the patient was admitted to our Department of Pediatric Hematology – Immunology and Transfusion Medicine, National Pediatric Hospital (NPH).
On physical examination, she had a fever at 38.4oC, tachycardia (120 bpm) associated with painful flexion and extension of the left hip. There was no evidence of organomegaly, distal neurovascular deficit, rashes, or skin lesions except stretch marks on the abdomen (Figure 1) and acanthosis nigricans (Figure 2), and the eye examination was unremarkable.
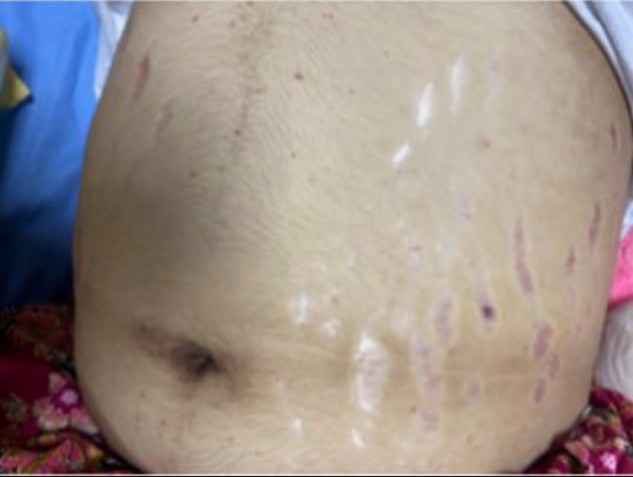
Figure 1: Stretch marks on abdomen

Figure 2: Acanthosis nigricans.
Her past medical history revealed the diagnosis of chronic immune thrombocytopenic purpura, currently being treated with combined dexamethasone, vincristine, and elthrombopag. Her medical history was also notable for obesity (weight 90 Kg, BMI 34.29). There was no history of trauma.
Case Management
Laboratory and imaging findings
The initial laboratory findings: white blood cells (WBC) were 13.6×109/L (neutrophils: 11.83×109/L, lymphocyte count: 1.22×109/L), hemoglobin: 9 g/dL, normal glycated hemoglobin (HbA1c): 5.4%, platelet count: 81 ×109/L, erythrocyte sedimentation rate (ESR): 80 mm/hour and C-reactive protein (CRP): 12 mg/dL. Serum urea and creatinine were increased to 62 mg/dL and 1.8 mg/dL, respectively. Thyroid Stimulating Hormone was increased (TSH) at 6.6 mIU/mL (range: 0.35-5.1), normal free T4: 1.19 ng/dL (range: 0.5-1.4), normal free T3: 3.42 pg/ml (range: 1.8-4.2). The electrolytes and liver function tests were within normal range. The urinalysis showed bacteria 1+, red blood cells (RBC) > 100/HPF, WBC 38/HPF. In addition, the X-Ray of the left hip showed no bone/joint abnormality (Figure 3), whereas the ultrasound indicated an intra-articular collection around 16 mm (Figure 4).
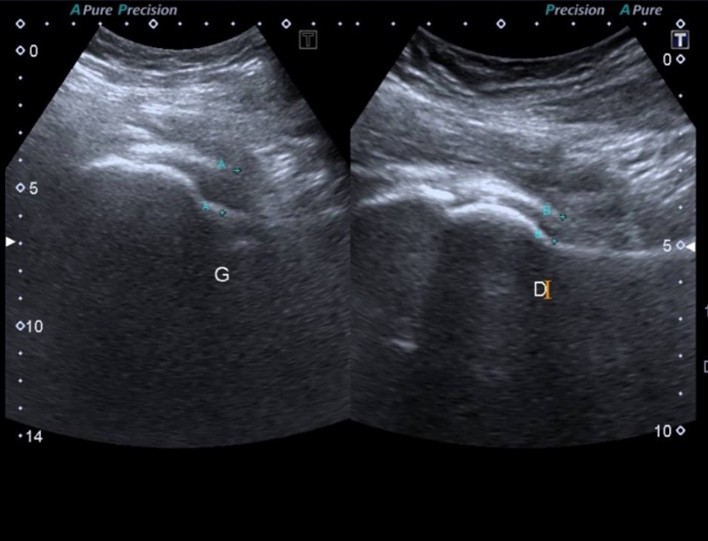
Figure 3: Intra-articular collection of left hip joint

Figure 4: X-ray of left hip joint
The restricted movement of left hip, pain, fever, elevated ESR, CRP and increasing leucocyte count suggested a diagnosis of septic arthritis. Initially, she was referred to the surgery department for surgical intervention after collecting urine and blood for microbiological culture.
Treatment
An urgent decision was taken for surgical arthrotomy and debridement by a team of pediatric surgeons on 03 February 2024. The hip was aspirated with a 16 G needle, confirmed with bloody-purulent fluid (Figure 5). An incision of the posterior and lateral tip of the greater trochanter and about 5cm up to the proximal femur was done. The articular capsule was carefully irrigated with normal saline mixed with diluted betadine. Post operated limb was given skin traction to prevent flexion and internal rotation. Antibiotic tri-therapy was intravenously indicated – ceftriaxone, gentamycin, and ciprofloxacin.

Figure 5: Bloody-purulent fluid of left hip joint
The result of the culture on the purulent fluid showed a facultative anaerobic gram-negative bacillus (Citrobacter freundii) susceptible to the current treatment.
The patient’s clinical condition remained stable after surgery, but the fever continued. The blood culture showed Salmonella typhi, and the urine culture showed Escherichia coli (Table 1)
| Specimens | Pus culture | Urine culture | Blood culture |
| Pathogens | Citrobacter freundii | Escherichia coli | Salmonella typhi |
| Susceptibility | |||
| Ceftriaxone | S | S | S |
| Gentamicin | S | S | ─ |
| Ciprofloxacin | S | S | S |
| Ceftazidime | S | S | ─ |
| Trimeth/sulfa | S | S | S |
| Amoxi/clav | S | ─ | ─ |
Table 1: Pathogens and susceptibility
Drainage of the purulent discharge from the left hip joint was continued along with broad-spectrum intravenous antibiotic therapy. Three weeks later, the patient’s condition significantly improved, and the traction was removed. The patient was discharged and instructed to continue oral ciprofloxacin and cloxacillin for three more weeks. The subclinical hypothyroid was initially treated with levothyroxine.
Follow-up
The patient underwent routine monitoring for both hematological and clinical parameters. During the antibiotic treatment and surgical intervention, the immunosuppressive drugs were stopped. This was due to the platelet count gradually increasing during the infection from 81 ×109/L to 861 ×109/L, then declining to 250 ×109/L four months later (Table 2). The patient is doing great so far.
| Date | Platelet count ×109/L | HbA1c (%) |
| 31/01/2024 | 171 | – |
| 02/02/2024 | 105 | – |
| 03/02/2024 | 81 – Surgical intervention | |
| 09/02/2024 | 592 | – |
| 14/02/2024 | 861 | 5.40 |
| 22/02/2024 | 713 | – |
| 03/03/2024 | 766 | – |
| 10/05/2024 | 564 | – |
| 17/06/2024 | 250 | 3.21 |
Table 2: Variation of platelet count and HbA1C before and after surgical intervention
Discussion
Septic arthritis in the pediatric hip joint is relatively rare, with an incidence of 1-10 in 100,000 individuals, and is considered an orthopedic emergency. It has 3 sources: hematogenic spread, direct inoculation, and spread from adjacent tissue [4]. This condition can lead to permanent damage to the joint if not treated promptly and effectively. Early diagnosis and treatment are crucial to avoiding long-term complications. The case reported two interesting aspects of this uncommon condition.
Firstly, septic arthritis is often secondary to the hematogenic spread of bacteria from other locations, but in our case, there was no apparent primary source. The pathogen isolated from the aspirated pus of the affected hip was different from that isolated in the blood and urine cultures.
Secondly, septic arthritis is more prevalent among individuals with weakened immune systems, joint problems, or certain medical conditions [5]. Additionally, weight load due to obesity is another risk that puts an excess load on the hip joints and leads to hip osteoarthritis [6].
Corticosteroids are known as the main immunosuppressants associated with severe infections in patients with ITP who were exposed to long-term treatment [7]. Our case was an obese child with chronic ITP who was under long-term use of immunosuppressive therapy such as Dexamethasone and Vincristine, which seemed to be the risk factors that caused serious concurrent infections by three different pathogens.
To date, the recommended treatment for septic arthritis, including antibiotics and surgical debridement of the inflammatory tissue, is to administer culture-specific intravenous antibiotics for seven days, then switch to oral antibiotics for two to three weeks [8]. To treat typhoid fever due to Salmonella typhi and urinary tract infection due to Escherichia coli, the choice of antibiotics is generally based on susceptibility. In our case, those 3 pathogens were susceptible to similar antibiotics.
Being overweight is known as an independent risk predictor for type 2 diabetes mellitus [9]. In addition to weight load, the presence of acanthosis nigricans, potentially caused by insulin resistance, is a warning signal to alert potential pre-diabetic states that make it more likely to develop type 2 diabetes mellitus. However, these two indications in our obese patient were not consistent with her normal levels of HbA1c during the two successive follow-ups over the past 1.5 years.
The latest report by Mukul Aggarwal et al from prospective study of 128 Indians aged more than 12 years old, diagnosed as persistent and chronic ITP demonstrated that thyroid dysfunction was common in ITP patients, present in around 25.7% of patients in which overt hypothyroidism was seen in 16.4% (21/128) of patients, subclinical hypothyroidism in 7.0% (9/128) [10] as we found the increased TSH with normal free T4 in the case. Role of glucocorticoids, estrogens, and systemic illness (acute/chronic) can probably alter thyroid hormones, including T4 and TSH [10].
The unexpected thrombocytosis, which declined to normal levels after antibiotic therapy, was probably due to the infectious event. It may also have been a response to the combined course of high-dose dexamethasone and vincristine.
Conclusion
Long-term treatment of combined immunosuppressive drugs for chronic ITP in obese patients is prone to serious concurrent infections such as typhoid fever, urinary tract infection, and septic arthritis of the hip joint. Being vigilant with patients showing these risk factors can lead to a correct diagnosis and timely management. The key success of treatment for our patient is the collaboration between orthopedic surgeons and hematologists.
References
- Kamat DM, et al. Immune thrombocytopenic purpura. In: Quick reference guide to pediatric care. 2nd ed. American Academy of Pediatrics; 2017:554-559. doi:10.1542/9781610021128-immune Crossref
- Bolton-Maggas PHB. Severe bleeding in idiopathic thrombocytopenic purpura. J Pediatr Hematol Oncol. 2003;25(Suppl 1):S47-S52. doi:10.1097/00043426-200312001-00011 PubMed | Crossref | Google Scholar
- Ackerman IN, Osborne RH. Obesity and increased burden of hip and knee joint disease in Australia: Results from a national survey. BMC Musculoskelet Disord. 2012;13(1):254. doi:10.1186/1471-2474-13-254
PubMed | Crossref | Google Scholar - Tretiakov M, Cautela FS, Walker SE, et al. Septic arthritis of the hip and knee treated surgically in pediatric patients: Analysis of the Kid’s Inpatient Database. J Orthop. 2019;16(1):97-100. doi:10.1016/j.jor.2018.12.017 PubMed | Crossref | Google Scholar
- Chalil AM, Kurup KK, Eapen F, Hashim S, Prince G. Case of left hip acute pediatric septic arthritis – polymicrobial etiology. Int J Res Orthop. 2023;9:1286-1288. doi:10.18203/issn.2455-4510.IntJResOrthop20233280 Crossref
- Kulkarni K, Karssiens T, Kumar V, Pandit H. Obesity and osteoarthritis. Maturitas. 2016;89:22-28. doi:10.1016/j.maturitas.2016.04.006 PubMed | Crossref | Google Scholar
- Moulis G, Palmaro A, Sailler L, Lapeyre-Mestre M. Corticosteroid risk function of severe infection in primary immune thrombocytopenia adults: A nationwide nested case-control study. PLoS One. 2015;10(11):e0142217. doi:10.1371/journal.pone.0142217 PubMed | Crossref | Google Scholar
- Earwood JS, Walker TR, Sue GJC. Septic arthritis: Diagnosis and treatment. Am Fam Physician. 2021;104(6):589-597. Septic arthritis: Diagnosis and treatment PubMed | Google Scholar
- Regmi D, AlShamsi S, Govender RD, et al. Incidence and risk factors of type 2 diabetes mellitus in an overweight and obese population: A long-term retrospective cohort study from a Gulf state. BMJ Open. 2020;10:e035813. doi:10.1136/bmjopen-2019-035813 PubMed | Crossref | Google Scholar
- Aggarwal M, Mahapatra M, Seth T, Tyagi S, Tandon N, Saxena R. Thyroid dysfunction in patients with immune thrombocytopenia: Prevalence and its impact on outcome. Indian J Hematol Blood Transfus. 2022;38(1):173-177. doi:10.1007/s12288-021-01460-7 PubMed | Crossref | Google Scholar
Acknowledgments
The authors thank Assoc. Prof. Ou Cheng Ngiep, Dr. Sok Youlay and a team of pediatric surgeons for their contribution to the interventional arthrotomy, debridement, and further care post-surgery.
Funding
Not applicable
Author Information
Corresponding Author:
Try Lytheang
Department of Pediatric Hematology and Immunology
National Pediatric Hospital, Phnom Penh, Cambodia
Email: trylytheang@gmail.com
Co-Authors:
Long Laiya
Department of Pediatric Hematology and Immunology
National Pediatric Hospital, Phnom Penh, Cambodia
Chean Sophâl
Department of Pediatric Hematology and Immunology
National Pediatric Hospital, Phnom Penh, Cambodia
Lam Pechkethia
Department of Pediatric Hematology and Immunology
National Pediatric Hospital, Phnom Penh, Cambodia
Robyn Devenish
Department of Laboratory
National Pediatric Hospital, Phnom Penh, Cambodia
Authors Contributions
All authors contributed to the conceptualization, investigation, and data curation by acquiring and critically reviewing the selected articles. They were collectively involved in the writing – original draft preparation, and writing – review & editing to refine the manuscript. Additionally, all authors participated in the supervision of the work, ensuring accuracy and completeness. The final manuscript was approved by all named authors for submission to the journal.
Informed Consent
Informed consent was provided to a child’s parents as they agreed to the case publication.
Conflict of Interest Statement
The authors declare that they have no competing interests.
Guarantor
Not reported
DOI
Cite this Article
Lytheang T, Laiya L, Pechkethia L, Sophâl C, Devenish R. Concurrent Infections in an Obese Adolescent Female with Chronic Immune Thrombocytopenia. medtigo J Med. 2024;2(3):e3062238. doi:10.63096/medtigo3062238 Crossref













