






 Author Affiliations
Author Affiliations
Abstract
Background: The nursing education produces knowledge and clinical competency as the primary outcomes that guarantee safe and effective patient care. The comparison of government and private nursing students assists in determining the possible differences in education and readiness to work in the field.
Aim: This study aimed to compare the knowledge and clinical competency levels of undergraduate nursing students in government and private institutions in Swat to identify differences in educational outcomes and practical skills.
Methodology: The study was a descriptive comparative cross-sectional study that was carried out on 235 nursing students with clinical experiences (117 government, 118 private). Simple random sampling was used to pick the participants. A structured questionnaire was used to collect data on such variables as demographics, theoretical knowledge, clinical skills, and views on the learning environment.
Results: Most students (61.7) had 10- 20 clinical hours a week, and 76.6% were exposed to a simulation lab. The theoretical knowledge of government students was better (mean 72.4, 10.5) than that of the private students (mean 61.2, 11.2). There were also higher levels of satisfaction with clinical supervision, lab preparation, feedback, and resource availability among government students. Chi-square test has shown that there is a significant relationship between the type of institution and the level of knowledge (23.76, p < 0.001).
Conclusion: The knowledge and clinical competency of the government nursing students were better than those of the students of the private institutions. The differences could be in the form of differences in clinical exposure, faculty support, class size, and availability of resources.
Keywords
Nursing students, Knowledge, Clinical competency, Government institutions, Private institutions, Simulation lab.
Introduction
The concept of nursing knowledge is defined as theoretical knowledge of nursing concepts, principles, and evidence-based practices that facilitate safe and effective care of patients. Clinical competency is the combination of knowledge, psychomotor skills, clinical judgment, communication, and professional behavior in practice in actual healthcare settings.[1] Knowledge and competency are both considered to be the inevitable results of nursing education programs. The nursing standards are shaped in such a way that students develop the necessary theoretical background and practical skills.[2] The lack of balance between these two components can undermine patient safety and care quality. As such, a systematic evaluation of the two areas is needed. The institutional differences can also play a major role in affecting the student learning outcomes.[3]
Nursing education is critical to the creation of a competent nursing workforce that can address healthcare needs. Nursing education is provided in government and privately owned institutions in most countries, which vary in governance, funding, infrastructure, and educational facilities.[4] These differences can lead to disparities in the learning content of academic standards and clinical skills of nursing students. Issues of discrepancies in graduate preparedness have been raised in various kinds of institutions. These disparities can impact the performance of the professionals and patient outcomes. There is a need, therefore, to compare the educational outcomes. The knowledge of such differences facilitates the standardization of nursing education.[5]
A combination of theoretical teaching and practical application is one of the foundations of nursing education. Students in nursing must acquire complicated scientific knowledge and gain practical clinical skills. The nursing institutions usually admit many students in the government, thus constraining conducive individual instruction and supervision. Class sizes are usually smaller in institutions that are privately owned, which might bring about close interaction between faculty and students.[6] Nevertheless, there are still disparities in curriculum delivery and clinical exposure. Competency requires a good integration of theory and practice. The failure to integrate properly may give rise to knowledge-performance gaps.[7]
A major measure of the quality of nursing education is believed to be clinical competency. It comprises technical proficiency, critical thinking, decision making, communication, and ethics. Government facilities also tend to expose a person to large patient volumes, and a range of clinical experiences is provided.[8] Nevertheless, the concentration of people and inadequate supervision can affect the development of skills. Structured supervision may be offered by private institutions, but with a limited variety of patients. Every environment has its own strengths and opportunities in terms of the acquisition of skills. Such differences in context can affect the level of competency of students. Such variations can be identified using comparative assessment.[9]
It is also important that nursing practice requires knowledge acquisition. The solid theoretical base helps the nurses to comprehend the processes of the disease, implement nursing interventions, and make effective clinical choices. Instruction techniques, testing techniques, and faculty skills contribute significantly to the development of knowledge. There could be unequal academic rigor and assessment standards in government and private institutions. Such disparities may affect the learning outcomes and academic results. Differences in the implementation of the curriculum can also have an impact on knowledge retention. It is hence important to measure the level of knowledge across the institutions.[10]
Availability and effectiveness of the faculty also play a significant role in the learning of students. Administrative and financial constraints usually cause a problem of shortages of faculty in government institutions. This could lead to work pressure and less academic supervision. Private institutions can put more funds into faculty training and learning materials. Mentoring, feedback, and academic support are influenced by teacher student ratio. Good faculty involvement increases knowledge and clinical competency. Faculty support could also be a source of differences in the performance of students.[11]
The clinical learning environment plays a very important role in competency development. Availability of skills laboratories, simulations, and the use of modern equipment increases clinical preparedness. Laboratories and organized skills training are common in private institutions. Hospital-based learning experiences are essential to government institutions. Inadequate exposure to regulated practice settings can be a barrier to the acquisition of skills. Clinical settings have an effect on confidence, decision-making, and performance. Such disparities create the need to compare competency results in a comparative manner.[12]
The method of assessment applied by schools and colleges has a great influence on the learning behavior of students. To measure actual performance, competency-based tests, objective structured clinical exams, and continuous exams are important elements that can be utilized to assess actual performance. Theory-oriented or inconsistent testing cannot necessarily depict real clinical competence. Various assessment methods can be employed by the government and other institutions. The way evaluation is done may have an impact on student preparation and motivation. There is a need to have standardized assessment systems to provide fairness. Comparative analysis offers us an understanding of how well an assessment is effective.[13]
There are also institutional academic support systems that affect student outcomes. The confidence and performance of students are enhanced with the help of academic counseling, mentorship programs, and feedback mechanisms. Academic and psychological support is often organized in private institutions. The government institutions can also be poorly supported because of the lack of resources. Absence of mentoring is detrimental to education and capacity building. Conducive learning conditions lead to academic achievements. The existence of these institutional variations is something to be studied systematically.[14]
The process of becoming a nursing student to a professional nurse requires being well-prepared in terms of knowledge and clinical competency. Unconfident or incompetent graduates can become a burden in clinical practice. Lack of preparation may affect patient safety and care. There is a need to be consistent in the educational results of institutions. Comparative evaluations will be used to identify gaps that need to be addressed. Workforce preparedness is improved through strengthening nursing education. Skilled graduates help to enhance better healthcare results.[15,16]
Comparative evaluation of government and private nurse students in terms of knowledge and clinical competency can be useful evidence to teachers and policy-makers.[17] The recognition of differences facilitates specific curriculum changes and resource distribution. Evidence-based interventions can enhance the quality of teaching, assessment, and clinical training. These assessments assist in the normalization of education in nursing. Finally, the quality of education would result in a competent and self-confident nursing staff. The research focuses on improving the field of nursing education and the provision of healthcare.
Methodology
The descriptive comparative cross-sectional research design was used in this study to examine and juxtapose the scope of knowledge and clinical competency among the undergraduate nursing students in government and private nursing colleges in Swat. A cross-sectional approach was suitable because it was possible to measure the variables simultaneously at one point in time without any manipulations, and the comparative part was used to identify the difference between the two institutional groups. The study setting also comprised the nursing colleges in the selected government and private colleges that were offering the undergraduate nursing programs and were selected based on accessibility, availability of the students, and institutional consent.
The population was those undergraduate nursing students in the final year of their studies who had completed their core theoretical courses and had at least one clinical rotation. Homogeneity was upheld by eliminating students who had worked in other fields of nursing before or those not exposed to clinical nursing comprehensively. There were about 600 eligible students in total. The required sample size was estimated in the Raosoft online sample size calculator with 5% margin of error and 95% level of confidence, which gave the result of 235 participants. The simple random sampling was used to make the sample representative to reduce selection bias.
Data collection procedure: Ethical approval from Zalan College of Nursing, Swat, Ref No ZCN/IRB/2026/02. Written permission was granted by the administration of the chosen government and private nursing colleges. The study purpose and objectives were well explained to the participants, and they gave informed consent before data collection. The process was voluntary and confidential.
The data collection tool was a structured questionnaire, which was used to measure the theoretical knowledge and clinical competency of the participants. A total of 118 students in the private nursing colleges and 117 students in the government nursing colleges were used to gather data. The researcher personally went to the institutions to hand out and collect questionnaires, assuring the clarity of instructions and responding to the questions raised by the participants. The On-site review of completed questionnaires was done to check on completeness and accuracy. The information obtained was coded and inputted in SPSS to be analyzed.
Data analysis procedure: SPSS version 27 was used in the process of data analysis. The demographic characteristics, level of clinical competency, and knowledge scores were summarized using descriptive statistics (frequency, percentages, mean, and standard deviation). The application of inferential statistics was implemented to compare the results between the government and the private nursing students. The relationships among categorical variables were analyzed with chi-square tests, whereas the correlation was employed to study the connection between the level of knowledge and clinical competency. The interpretation of results was made at a 95% confidence level, and the results were displayed in tables and narrative format to enable them to be clear and understood.
Results
Demographic data analysis: Table 1 demonstrates demographic and scholarly attributes of 235 nursing students who participated in the research. The research involved most participants (68.1%) who were within the age group of 20 25 years and 27.8% within the age group 26-30 years, with a small proportion of 2.1 years old. The sample consisted of 65.1% of male students and 34.9% of female students. The sample was nearly balanced in terms of the government (49.8) and the private (50.2) nursing institutions. On clinical exposure, 61.7% of students reported 1020 clinical hours/week, 23.4% more than 20 hours, and 14.9% less than 10 hours. The vast majority (76.6) had experience in the simulation laboratory, and 23.4% did not. These features give a base for the analysis of knowledge and clinical competency differences in the government and the private nursing students.
| Variable | Category | Frequency (n) | Percentage (%) |
| Age (years) | <20 | 05 | 2.1 |
| 20–25 | 160 | 68.1 | |
| 26–30 | 70 | 27.8 | |
| Gender | Male | 153 | 65.1 |
| Female | 82 | 34.9 | |
| Institution | Government | 117 | 49.8 |
| Private | 118 | 50.2 | |
| Clinical hours per week | <10 | 35 | 14.9 |
| 10–20 | 145 | 61.7 | |
| >20 | 55 | 23.4 | |
| Simulation lab exposure | Yes | 180 | 76.6 |
| No | 55 | 23.4 |
Table 1: Demographic characteristics of nursing students
The theoretical assessment of the nursing students showed significant variations in government and non-government institutions. Out of the government students, 57 (48.7%) showed good knowledge (>75%), 50 (42.7) moderate (50-75), and 10 (8.5) poor (<50) knowledge. Conversely, the students of private institutions had less knowledge, as only 18 (15.3) students had good knowledge, 70 (59.3) students had moderate knowledge, and 30 (25.4) students had poor knowledge. The total mean of the knowledge score was greater among the government students (72.4, 10.5) than among the private students (61.2, 11.2), and the combined mean score was 66.8, 12.0. These findings show that students of government nursing are usually more knowledgeable in theory, and students of the private sector have a higher percentage of low rankers. These disparities in the level of knowledge may be based on differences in faculty support, the size of the classes, and resources (Figure 1).
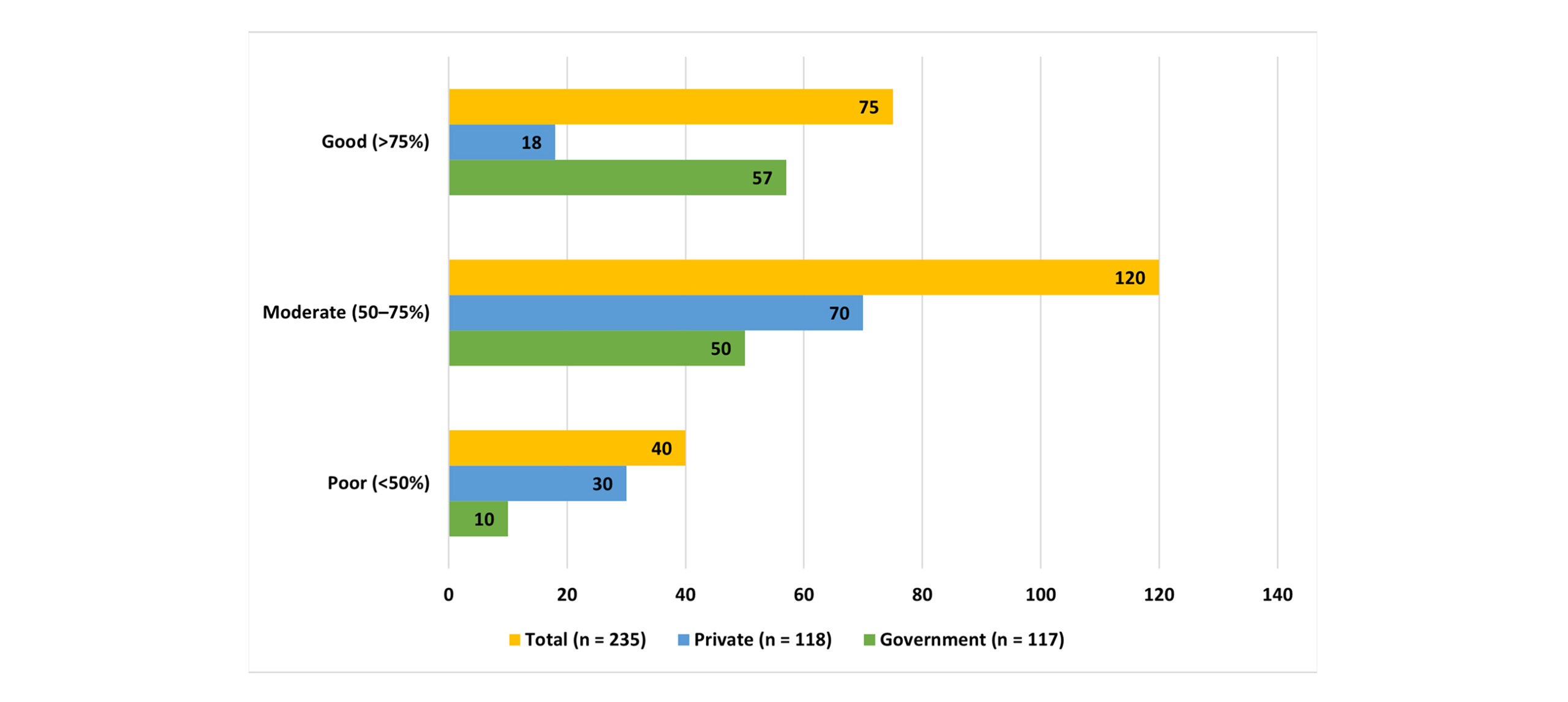
Figure 1: Knowledge test scores of nursing students (n = 235)
Table 3 summarizes the comparative analysis of clinical competency between the government and the private nursing students. Government students always score higher in terms of means compared to the private students across all skill areas. In vital signs and basic assessment, the government students scored 4.2 0.5 versus 3.7 0.6, whereas in aseptic wound dressing, the government students scored 4.1 0.5 versus 3.6 0.7. Government students (mean scores of 4.0-4.2) also exhibited higher competency in skills like IV-line insertion and care, safe medication administration, and response to deterioration of patients when compared to their counterparts who are students in private schools (3.5-3.7 scores). The same was true in competencies in communication, pain assessment, documentation, patient/family teaching, and CPR performance. All in all, the overall mean scores demonstrate that government nursing students have higher clinical skills, so the variations in clinical exposure, patient load, and supervision can be one of the factors that bring these differences in the levels of competencies.
| Skill Area | Government (n = 117) | Private (n = 118) | Total (n = 235) |
| Vital signs & basic assessment | 4.2 ± 0.5 | 3.7 ± 0.6 | 3.95 ± 0.6 |
| Aseptic wound dressing | 4.1 ± 0.5 | 3.6 ± 0.7 | 3.85 ± 0.65 |
| IV-line insertion & care | 4.0 ± 0.6 | 3.5 ± 0.7 | 3.75 ± 0.65 |
| Safe medication administration | 4.1 ± 0.5 | 3.6 ± 0.6 | 3.85 ± 0.6 |
| Effective nurse-patient communication | 4.2 ± 0.5 | 3.7 ± 0.6 | 3.95 ± 0.55 |
| Responding to patient deterioration | 4.0 ± 0.6 | 3.5 ± 0.7 | 3.75 ± 0.65 |
| Pain assessment & management | 4.1 ± 0.5 | 3.6 ± 0.6 | 3.85 ± 0.6 |
| Documentation accuracy | 4.2 ± 0.5 | 3.7 ± 0.6 | 3.95 ± 0.55 |
| Patient/family teaching | 4.1 ± 0.5 | 3.6 ± 0.6 | 3.85 ± 0.6 |
| CPR performance | 4.0 ± 0.6 | 3.5 ± 0.7 | 3.75 ± 0.65 |
Table 2: Self-reported clinical competency (Mean scores, 1–5 scale)
The evaluation of the perception of the students on their clinical training shows that there is a significant difference between the government and the private nursing training institutions. Government students always recorded higher satisfaction with all statements than their counterparts, the private students. In the case of clinical supervision, government students scored 4.1 ± 0.5, compared to 3.6 ± 0.6 in private students. On the same note, government students gave lab preparation a mean score of 4.2 ± 0.5, and private students scored 3.7 ± 0.6. Government students rated the timeliness of feedback on clinical performance 4.0, regardless of whether it was provided or not, whereas the private students rated it 3.5, regardless of whether the feedback was provided. Government students also rated access to adequate equipment and supplies as better (4.1 ± 0.5) than that of the private students (3.6 ± 0.6). Government students overall had a higher perception of being prepared to engage in safe and effective nursing practice (4.2 ± 0.5) in comparison to their colleagues in the private institution (3.7 ± 0.5). These results indicate that variations in supervision, exposure to skills laboratories, feedback system, and availability of resources can be causative factors of both clinical competency and student confidence.
| Statement | Government (n = 117) | Private (n = 118) | Total (n = 235) |
| My college provides enough clinical supervision. | 4.1 ± 0.5 | 3.6 ± 0.6 | 3.85 ± 0.55 |
| Skills lab sessions prepared me well for clinical practice. | 4.2 ± 0.5 | 3.7 ± 0.6 | 3.95 ± 0.55 |
| I get timely feedback on clinical performance. | 4.0 ± 0.6 | 3.5 ± 0.7 | 3.75 ± 0.65 |
| I have access to adequate equipment/supplies during training. | 4.1 ± 0.5 | 3.6 ± 0.6 | 3.85 ± 0.55 |
| Overall, my training prepares me for safe and effective nursing practice. | 4.2 ± 0.5 | 3.7 ± 0.6 | 3.95 ± 0.55 |
Table 3: Perceptions of learning environment (Mean scores, 1–5 scale)
The comparison of theoretical knowledge among the government and the private engineering students in nursing revealed a statistically significant difference. Out of the government students, 57 (48.7%) showed good knowledge (>75%), 50 (42.7) moderate (50-75), and 10 (8.5) poor (<50) knowledge. Conversely, there were 18 (15.3) good, 70 (59.3) moderate, and 30 (25.4) poor in the private students. The chi-square test revealed that there was a significant relationship between institution type and level of knowledge (23.76, p < 0.001), which indicated that government nursing students tend to have better theoretical knowledge than their counterparts who are in the private sector. This disparity can be explained by such factors as the size of the classes, faculty support, and access to learning resources.
| Knowledge level | Government (n = 117) | Private (n = 118) | Total (n = 235) | χ² (p-value) |
| Poor (<50%) | 10 | 30 | 40 | |
| Moderate (50–75%) | 50 | 70 | 120 | |
| Good (>75%) | 57 | 18 | 75 | 23.76 (p < 0.001) |
Table 4: Association between knowledge level and institution type
Discussion
The current research was a survey of clinical exposure and simulation laboratories of undergraduate nursing students. The results showed that most students (61.7) spent 10 to 20 hours in clinical work in a week, with only 14.9 spending less than 10 hours and 23.4 spending more than 20 hours. These findings show that the majority of students are practicing to a moderate extent in clinical practice, which is critical in gaining competency and confidence in dealing with patients. Similar results were achieved by Al-Hussami et al., as nursing students spent an average of 1218 clinical hours per week, and this proved that structured clinical hours are a significant reason behind acquiring and developing skills in the profession.[18,19] In comparison, a study by Chiu et al. established that a significant number of students worked more than 20 hours in a clinical setting per week and indicated that there is a difference in the exposure to a clinical setting in various institutions, and there is a possibility that fatigue or burnout may occur when the clinical experience exceeds 20 hours a week. They can be institutional differences, access to clinical placement sites, and student-to-preceptor ratios, which determine the amount and quality of direct learning.[20]
Exposure to the simulation lab was noted among 76.6% of all students, meaning that the majority of the respondents were exposed to the structured practical training in a controlled setting. This is in line with other researchers, Foronda et al., who highlighted that simulation-based learning improves clinical judgment, procedural skills, and self-efficacy in nursing students. The prevalence of exposure to simulation lab experienced by the current study is high and is indicative of a positive institutional focus on a combination of theoretical knowledge and practical skills.[21] Nonetheless, only 23.4% of the students were exposed to simulation labs, and this may hinder their preparedness for clinical situations in the real world. Equally, Cant and Cooper have found that students who do not have simulation experience frequently experience difficulties with critical thinking and independent procedure performance, which proves the necessity to ensure equal access to simulation resources. The difference in exposure can be explained by the lack of laboratories or conflicts in lectures within the curriculum.[22]
The relationship between the number of hours of clinical exposure and simulation exposure is important to maximize the effect of learning. Although clinical practice is the only one that will enable students to interact with real patients, simulation labs will enable safe practice for the students. Research conducted by Shin et al. pointed out that both techniques are more effective than either in skill retention or confidence. In this respect, simulation exposure in the current research is high, with moderate clinical hours to facilitate holistic nursing education.[23] It is also interesting to note that students with less than 10 hours of clinical time per week might experience fewer chances of interacting with patients, and thus, this might impact competence. The observation is similar to the study by Omer and Alotaibi, who observed that a lack of clinical exposure relates to a lack of self-reported confidence in carrying out the core nursing procedures. On the contrary, clinical hours were too many, and as is witnessed in a smaller group of participants, it might cause fatigue and less efficient learning, as is confirmed by one study.[24]
The demographics of the participants, though not described in this paper, might have an impact on clinical engagement, too. Research has shown that younger students and those who are still under training tend to need more supervision as they train, and senior students tend to be more advantageous in independent clinical practice. The question of the ratio of clinical hours to exposure to simulation, as witnessed in this study, would seem to offer a suitable scaffold to the development of skills at various levels of student experience.[25] When these findings are compared to the situations in other countries, it is obvious that there is a vast range of clinical hour allocations. In certain countries, students might be given less formal time but more simulation laboratory incorporation, whereas other countries have much clinical exposure, which is heavily based in hospitals. As an example, research carried out in the United States indicated that learners with less access to simulation laboratories relied mainly on clinical placements, but in Australia, simulation laboratories were more likely to be used as an addition to clinical hours, and this factor increased competency outcomes.[26,27]
The results also highlight the importance of the design of curricula in nursing education. Those institutions that combine moderate clinical hours with simulation laboratories are certain that the students will not only attain the required standards of evaluation but also attain a certain level of confidence in both technical and non-technical skills. The findings of this study are in keeping with the suggestions by Jeffries who proposed a blended learning method where simulation is supplemented with real-life clinical experience to achieve the best skills.[28] Besides, the findings demonstrate the necessity of constant review of clinical hour allocation. The existing balance appears to be efficient, but regular evaluation is required so that the balance can be adjusted to meet the evolving healthcare needs, student requirements, and educational technological innovations. The works by Liaw et al identified how the dynamic change of the clinical and simulation hours is more effective in improving student satisfaction and learning outcomes, which further supports the need to plan the curriculum flexibly.[29,30]
Although the findings of the study are encouraging, the study has limitations in using self-reported data on clinical hours and exposure to the simulation lab, which could have resulted in reporting bias. It was observed to have similar constraints in the works of Johnson et al., where objective assessment of clinical participation and simulation involvement would make such research more reliable. Nevertheless, the research also offers some important contributions to the existing nursing education practices and areas of improvement.
Finally, the research indicates that most nursing students possess sufficient clinical experience and have substantial access to simulation labs, and facilitate in achieving the achievement of competencies and the development of practical skills. The findings, as compared to the rest of the literature, comply with the global trends of blended learning modalities that incorporate simulation and clinical practice. The institutions must go on providing equal opportunities to the use of simulation resources, maintaining an optimal ratio of clinical hours to gain maximum learning results and prepare students to work in the real world.
Recommendations for the study:
- Ensure that all nursing students receive adequate clinical hours, ideally within the 10–20 hours per week range, to balance skill acquisition and prevent fatigue.
- Increase access to simulation lab experiences for students who currently lack exposure, ensuring equitable learning opportunities across all cohorts.
- Integrate simulation-based training with clinical placements to reinforce practical skills, critical thinking, and clinical judgment.
- Provide structured debriefing sessions following simulation scenarios to enhance reflection, problem-solving, and knowledge retention.
- Periodically review and adjust clinical hour allocation to match evolving educational needs, student feedback, and healthcare practice demands.
- Standardize simulation lab scenarios and ensure high-fidelity training to maintain consistency and quality of learning outcomes.
- Train faculty and clinical instructors in effective supervision and mentorship to optimize the learning experience during both clinical rotations and simulation exercises.
- Conduct further research to evaluate the long-term impact of combined clinical and simulation exposure on nursing competence and professional readiness.
Conclusion
The research found that most nursing students were well exposed to clinical practice, with 10-20 hours per week being the most prevalent and extensive exposure to simulation laboratory training. Clinical practice combined with this simulation experience enables the acquisition of real-world skills, clinical rationale, and confidence in students. In comparison with a smaller percentage of students with less clinical experience or none, the general trend shows that the existing curriculum manages to balance the amount of practical patient care with the amount of simulated learning experience rather well. Fair access to clinical placements and simulation labs ensures maximum competency and preparedness for professional practice.
References
- Prendi E, Stievano A, Caruso R, et al. Measuring professional competencies of registered nurses and nursing students. A cross-sectional comparative study. Acta Biomed. 2022;93(4):e2022282. doi:10.23750/abm.v93i4.13332
PubMed | Crossref | Google Scholar - Farsi Z, Nasiri M, Sajadi SA, Khavasi M. Comparison of Iran’s nursing education with developed and developing countries: a review on descriptive-comparative studies. BMC Nurs. 2022;21(1):105. doi:10.1186/s12912-022-00861-x
PubMed | Crossref | Google Scholar - Grande RAN, Berdida DJE, Susanto T, Khan A, Waelveerakup W, Saad Z. Nursing competency inventory and professional competence of graduating students in six Asian countries: A cross-sectional study. Nurse Educ Today. 2022;116:105470. doi:10.1016/j.nedt.2022.105470
PubMed | Crossref | Google Scholar - Sharma SK, Arora D, Belsiyal X. Self-reported clinical practice readiness of nurses graduating from India: A cross-sectional survey in Uttarakhand. J Educ Health Promot. 2020;9:125. doi:10.4103/jehp.jehp_55_20
PubMed | Crossref | Google Scholar - Hussain S, Khan A, Arshad L, Rubab E. Trapped in the Screen: Clinical Insights into Digital Addiction and Mental Health Among Young Adults. medtigo J Neurol Psychiatr. 2025;2(3):e3084234. doi:10.63096/medtigo3084234
Crossref | Google Scholar - Beil-Hildebrand MB, Smith HB. Comparative Analysis of Advanced Practice Nursing: Contextual and Historical Influences in North American and German-Speaking European Countries. Policy Polit Nurs Pract. 2022;23(3):162-174. doi:10.1177/15271544221105032
PubMed | Crossref | Google Scholar - Jeffery N, Donald F, Martin-Misener R, et al. A Comparative Analysis of Teaching and Evaluation Methods in Nurse Practitioner Education Programs in Australia, Canada, Finland, Norway, the Netherlands and USA. Int J Nurs Educ Scholarsh. 2020;17(1):/j/ijnes.2020.17.issue-1/ijnes-2019-0047/ijnes-2019-0047.xml. doi:10.1515/ijnes-2019-0047
PubMed | Crossref | Google Scholar - Gunawan J, Aungsuroch Y, Fisher ML, McDaniel AM, Marzilli C. Perceived Managerial Competence of First-Line Nurse Managers: A Comparative Analysis Among Public Hospitals. Policy Polit Nurs Pract. 2020;21(3):151-163. doi:10.1177/1527154420926616
PubMed | Crossref | Google Scholar - Almondes K, Bizarro L, Miyazaki C, et al. Comparative analysis of psychology responding to the COVID-19 pandemic in BRICS nations. Front Psychol. 2021;12:567585. doi:10.3389/fpsyg.2021.567585
Crossref | Google Scholar - Tesfaye TS, Alemu W, Mekonen T. Perceived Clinical Practice Competency and Associated Factors Among Undergraduate Students of Medicine and Health Science Collage in Dilla University, SNNPR, Ethiopia. Adv Med Educ Pract. 2020;11:131-137. doi:10.2147/AMEP.S235823
PubMed | Crossref | Google Scholar - Cannistrà M, Agasisti T, Amagir A, et al. A comparative analysis of financial literacy levels and initiatives among students in five European countries. Res Comp Int Educ. 2022;17(2):246-280. doi:10.1177/17454999211066183
Crossref | Google Scholar - Kaur J, Sharma A. What do I know about social-emotional learning: a comparative analysis between public and private preschool teachers in Punjab. SAGE Open. 2022;12(2). doi:10.1177/21582440221091254
Crossref | Google Scholar - Ahmer Z, Fatima R, Sohaira R, Fatima M. How important is medical ethics? Descriptive cross-sectional survey among medical students of Karachi. Eur J Environ Public Health. 2021. doi:10.21601/ejeph/11058
Crossref | Google Scholar - Pavlic D, Burns HH, Wong A, Lehmer J. Comparative health systems immersion in South Korea: A constructivist competency-based approach to educating master’s nursing students. J Prof Nurs. 2020;36(1):92-97. doi:10.1016/j.profnurs.2019.07.001
PubMed | Crossref | Google Scholar - McFarlan S. An Experiential Educational Intervention to Improve Nurse Managers’ Knowledge and Self-Assessed Competence With Health Care Financial Management. J Contin Educ Nurs. 2020;51(4):181-188. doi:10.3928/00220124-20200317-08
PubMed | Crossref | Google Scholar - Guerrero JG, Tungpalan-Castro GM, Pingue-Raguini M. Impact of simulation debriefing structure on knowledge and skill acquisition for postgraduate critical care nursing students: three-phase vs. multiphase. BMC Nurs. 2022;21(1):318. doi:10.1186/s12912-022-01100-z
PubMed | Crossref | Google Scholar - Yi QF, Yan J, Zhang CJ, Yang GL, Huang H, Yang Y. The experience of anxiety among Chinese undergraduate nursing students in the later period of their internships: findings from a qualitative study. BMC Nurs. 2022;21(1):70. doi:10.1186/s12912-022-00847-9
PubMed | Crossref | Google Scholar - Aldhafeeri F, Alosaimi D. Perception of satisfaction and self-confidence with high-fidelity simulation among nursing students in government universities. J Educ Pract. 2019;11:137. doi:10.7176/JEP/11-12-16
Crossref | Google Scholar - Ankita B, Ipsa M. First year medical students’ and standard precautions: The need for change. Clin Epidemiol Glob Health. 2021;9:221-226. doi:10.1016/j.cegh.2020.09.002
PubMed | Crossref | Google Scholar - Chaisuwan C. The Influence of Cultural Values on Critical Thinking Dispositions among Baccalaureate Nursing Students: A Comparative Analysis between Thailand and the United States. Dissertation. Sage School of Health Sciences; 2020.
The Influence of Cultural Values on Critical Thinking Dispositions among Baccalaureate Nursing Stud… - Tseng LP, Hou TH, Huang LP, Ou YK. Effectiveness of applying clinical simulation scenarios and integrating information technology in medical-surgical nursing and critical nursing courses. BMC Nurs. 2021;20(1):229. doi:10.1186/s12912-021-00744-7
PubMed | Crossref | Google Scholar - Berhe S, Gebreyohannis T. Nursing students’ challenges toward the clinical learning environment at the School of Nursing and Midwifery, Addis Ababa University: a qualitative study. Int J Afr Nurs Sci. 2021;15:100378. doi:10.1016/j.ijans.2021.100378
Crossref | Google Scholar - Burau V, Falkenbach M, Neri S, Peckham S, Wallenburg I, Kuhlmann E. Health system resilience and health workforce capacities: Comparing health system responses during the COVID-19 pandemic in six European countries. Int J Health Plann Manage. 2022;37(4):2032-2048. doi:10.1002/hpm.3446
PubMed | Crossref | Google Scholar - Aboubakr RM, Bayoumy HMM. Evaluating educational service quality among dentistry and nursing students with the SERVQUAL model: A cross-sectional study. J Taibah Univ Med Sci. 2022;17(4):648-657. doi:10.1016/j.jtumed.2022.01.009
PubMed | Crossref | Google Scholar - Agrawal N, Kumar S, Bhargava S, Mahajan S, Usmanova G, Gautam A, Srivastava A, Shah H, Sinha P, Kumar AV, Bairagi A. Evaluating the effect of strengthening nurse midwifery pre-service education in two Indian states: a single group pre- and post-intervention study. Nurse Educ Today. 2020;104640. doi:10.1016/j.nedt.2020.104640
Crossref | Google Scholar - Mayra K, Padmadas SS, Matthews Z. Challenges and needed reforms in midwifery and nursing regulatory systems in India: Implications for education and practice. PLoS One. 2021;16(5):e0251331. doi:10.1371/journal.pone.0251331
PubMed | Crossref | Google Scholar - Purabdollah M, Zamanzadeh V, Ghahramanian A, Valizadeh L, Ghasempour M, Mousavi S. Determining and comparing the achieved competencies of graduating nursing students of public and private universities in Iran. BMC Med Educ. 2025;25(1):25. doi:10.1186/s12909-024-06622-5
PubMed | Crossref | Google Scholar - Terefe TF, Geletie HA, GebreEyesus FA, et al. Clinical competency and associated factors among undergraduate nursing students studying in universities of Southern regional state of Ethiopia, 2021. Heliyon. 2023;9(8):e18677. doi:10.1016/j.heliyon.2023.e18677
PubMed | Crossref | Google Scholar - Upashe S, Shil R, Shetty S. Self-reported clinical practice skill readiness of final-year nursing students studying in Bengaluru, Karnataka: an institutional-based cross-sectional study. J Health Allied Sci NU. 2022;13. doi:10.1055/s-0042-1744554
Crossref | Google Scholar - Srivastava S, Pandurangan H, Kumar A. Development and validation of a comprehensive nursing competence assessment questionnaire (CNCAQ) to determine the perceived clinical competence of nursing graduates. Nurs Midwifery Res J. 2024;20:96-111. doi:10.1177/0974150X241247986
Crossref | Google Scholar
Acknowledgments
The authors would like to express their sincere gratitude to Dr. Shah Hussain, Principal/Assistant Professor, Janbar College of Nursing, Swat, for his invaluable supervision, guidance, and support throughout the course of this study.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author Information
Corresponding Author:
Shah Hussain
Department of Nursing
Janbar College of Nursing, Swat, Pakistan
Email: shahrnpeads@gmail.com
Co-Authors:
Talha Ahmad, Sohail Wahab, Izhar Fazal, Saad Saeed, Asif Iqbal, Ubaid Zia, Abdur Rahman Khan
Department of Nursing
Saidu Teaching Hospital, Swat, Pakistan
Rizwan Ullah
Department of Nursing
Zalan College of Nursing, Swat, Pakistan
Authors Contributions
Talha Ahmad, Sohail Wahab, Izhar Fazal, Saad Saeed, Asif Iqbal, Ubaid Zia, and Abdur Rahman contributed to data collection and literature review. Shah Hussain Rizwan Ullah contributed to data analysis and interpretation.
Ethical Approval
Ethical Approval was obtained from Zalan College of Nursing, Swat, Ref No ZCN/IRB/2026/02.
Conflict of Interest Statement
The authors declare that there is no conflict of interest.
Guarantor
Talha Ahmad is the guarantor of this study and takes full responsibility for the integrity of the data and the accuracy of the data analysis.
DOI
Cite this Article
Ahmad T, Ullah R, Wahab S, et al. Comparative Assessment of Knowledge and Clinical Competency Level among Government and Private Nursing Students. medtigo J Med. 2026;4(1):e3062420. doi:10.63096/medtigo3062420 Crossref













