







 Author Affiliations
Author Affiliations
Abstract
Background: Metabolic syndrome (MetS), which involves insulin resistance, high blood pressure, dyslipidemia, and central obesity, is a well-known risk factor for type 2 diabetes and heart disease. Growing research on natural products led to the discovery that berberine, a compound isolated from the genus Berberis, influences the regulation of metabolism.
Objective: This narrative review attempts to give an in-depth perspective on the pharmacology, therapeutic value, and application of berberine in MetS.
Methodology: A thorough search of relevant scientific databases has been performed, and only those articles that address the mechanism of action and therapeutic efficacy of berberine in MetS have been considered.
Results: The mechanism of action of berberine is multifaceted, mainly via stimulation of adenosine monophosphate-activated protein kinase (AMPK), which results in better glucose utilization, increased insulin resistance, and lipid regulation. Based on clinical evidence, there have been observed changes in lowering fasting plasma glucose levels, favorable effects on lipid parameters, and a reduction in body mass index (BMI). In some instances, the drug is as effective as established drugs like metformin and statins. However, its use in medicine is hindered by poor oral absorption. Innovative approaches, such as nanotechnology, may help in maximizing its clinical benefits.
Conclusion: Berberine offers great potential for use as an adjuvant therapy in the treatment of MetS owing to its multitarget approach and relatively safe nature. However, more studies need to be done, especially in relation to better formulation approaches and clinical effects.
Keywords
Berberine, Metabolic syndrome, Pharmacological mechanism, Type 2 diabetes, Dyslipidemia, Berberine metabolite, Insulin resistance.
Introduction
Metabolic syndrome (MetS) is a worldwide epidemic that increases the likelihood of acquiring type 2 diabetes mellitus (T2DM), various cardiovascular diseases (CVD), and other health problems like coronary heart disease (CHD), dyslipidemia, diabetes, and hypertension.[1] Among the following metabolic diseases, insulin resistance (IR) and/or abdominal obesity, however, are currently thought to be the leading causes of the syndrome.[2]
First formulated by Reaven under the name of syndrome X, it describes the mechanism in which IR, the inability to maintain glucose control, and the subsequent appearance of T2DM and CHD interrelate with one another. The International Diabetes Federation (IDF), the World Health Organization (WHO), the American Association of Clinical Endocrinologists (AACE), the European Group on Insulin Resistance (EGIR), and the National Cholesterol Education Program- Adult Treatment Panel (ATP) have also conducted analyses that have enhanced the definition and description of MetS.[3] Despite a failure to converge on one definition, these organizations have nevertheless been successful in amalgamating the key themes of the obesity epidemic, IR, flawed glucose metabolism, hypertension, and crooked lipid profile.
| Organization | Year | Number of risk factors for diagnosis | Obesity criteria | Dyslipidemia
criteria |
Hyperglycemia criteria | Hypertension criteria | Additional components |
| WHO | 1999 | IR +2 or more risk factors | Waist-to-hip ratio: >0.9 (Male (M))
>0.85(Female (F)) OR body mass index (BMI)>30 kg/m2 |
Either triglycerides (TG) ≥1.7 mmol/L, high-density lipoprotein cholesterol (HDL-C) <0.91 mmol/L (M), or <1.0 mmol/L (F) |
2-hour oral glucose tolerance test (OGTT) >7.7 mmol/L OR fasting plasma glucose (FPG) ≥6.1 mmol/L |
Systolic blood pressure (SBP) ≥140 mmHg OR diastolic blood pressure (DBP) ≥90 mmHg |
Microalbuminuria (urinary albumin ≥20 µg/min) |
| EGIR | 1999 | IR + 3 or more risk factors | Waist circumference ≥94 cm (M), ≥80 cm (F) | HDL-C <1.0 mmol/L OR TG ≥2.0 mmol/L
|
FPG ≥6.1 mmol/L | SBP ≥140 mmHg OR DBP ≥90 mmHg | Excludes individuals with T2DM |
| National Cholesterol Education Program (NCEP)/ATP III | 2001 | 3 or more risk factors | Waist circumference ≥102 cm (M), ≥88 cm (F) | <1.3 mmol/L (F) OR TG ≥1.69 mmol/L,
HDL-C <1.0 mmol/L (M) |
FPG ≥6.1 mmol/L | SBP ≥130 mmHg OR DBP ≥85 mmHg | None |
| AACE | 2003 |
Impaired fasting glucose (IFG) or |
BMI ≥25 kg/m²* | HDL-C <1.0 mmol/L (M), <1.3 mmol/L (F) OR TG ≥1.69 mmol/L
|
FPG ≥5.6 mmol/L | SBP ≥130 mmHg OR DBP ≥85 mmHg | IR (T2DM family history, ethnicity, lifestyle, and polycystic ovary syndrome (PCOS)) |
| American Heart Association (AHA)/ National Heart, Lung, and Blood Institute (NHLBI)/ American Diabetes Association (ADA)(Updated ATP III) |
2004 | 3 or more risk factors | Waist circumference ≥102 cm (M), ≥88 cm (F) | <1.3 mmol/L (F) ,
TG ≥1.69 mmol/L OR HDL-C <1.0 mmol/L (M) |
FPG ≥5.6 mmol/L | SBP ≥130 mmHg OR DBP ≥85 mmHg | None |
| IDF | 2005 | Obesity (required) + 2 or more risk factors | Waist circumference ≥90 cm (Asian M), ≥80 cm (F)≥94 cm (M), | TG ≥1.7 mmol/L OR HDL-C <1.0 mmol/L (M), <1.3 mmol/L (F) | FPG ≥5.6 mmol/L | SBP ≥130 mmHg OR DBP ≥85 mmHg | None |
| Harmonized
definition |
2009 | 3 or more risk factors | Waist circumference based on ethnicity-specific values | HDL-C <1.0 mmol/L (M), <1.3 mmol/L (F) OR TG ≥1.7 mmol/L | FPG ≥5.6 mmol/L | SBP ≥130 mmHg OR DBP ≥85 mmHg | None |
Table 1: Comparison of the various definitions of MetS proposed by leading health organizations
Prevalence: MetS is a rising global health concern driven by dietary patterns, socioeconomic factors, and lifestyle changes. It is closely associated with obesity and T2DM. Due to decades of increasing obesity and diabetes rates, approximately one-third of individuals in the United States are estimated to have MetS. Certain ethnic groups, such as South Asian Americans, show higher rates of abdominal obesity and metabolic diseases. In China, the prevalence of MetS is increasing, with a growing proportion of overweight individuals, particularly in urban areas.
Globally, obesity rates have doubled in 73 countries since 1980, affecting more than 600 million adults and 100 million children. Notably, childhood obesity is rising at a faster rate than adult obesity. Low-income countries are experiencing the most rapid increases in obesity and related mortality. Although some individuals with obesity remain metabolically healthy, the majority are at a significantly higher risk of developing complications associated with MetS.[4-12]
| Region/Country | Trend/Statistics | Time period | Notes |
| USA | BMI increased by 0.37% per year (both genders), waist circumstances increased by 0.37% (M) & 0.27% (F) per year | 1988-2010 | National Health and Nutrition Examination Survey (NHANES) Data |
| 30.2 million adults (12.2%) had T2DM | 2017 | Centers for Disease Control and Prevention (CDC) Report | |
| 23.8% of people with diabetes people with diabetes were unaware of their condition | |||
| T2DM incidence is highest in seniors (25.2% in ≥65 years) | |||
| Prevalence of prediabetes/MetS ~3× T2DM cases (~1/3 of US adults) | |||
| Ethnic groups (USA) | T2DM incidence is 15% in American Indians | Highest risk | |
| 4.3% in Chinese Americans | Lowest risk | ||
| High MetS & abdominal obesity in South Asian Americans | |||
| China | Overweight & obesity increased from 14.6% → 21.8% (WHO criteria) | 1992-2002 | WHO Criteria |
| Using Chinese BMI cutoff: obesity increased from 20% → 29% | |||
| MetS prevalence urban: 8% → 10.6%, rural: 4.9% → 5.3% | An estimated 15.5% in 2017 | ||
| Global obesity (195 countries) | 604M adults & 108M children obese | 2015 | Global obesity survey |
| Obesity prevalence doubled in 73 countries since 1980 | 1980-2015 | ||
| Faster rise in obesity in children. | Concerning trend | ||
| Socioeconomic impact | and the most significant obesity increase in young men (25-29 yrs) in low-SDI countries | Socioeconomic Development Index (SDI) | |
| Global BMI-related deaths ↑ 28.3% (1990–2015) | |||
| 120 million DALYs lost due to obesity | Disability-Adjusted Life Years (DALYs) | ||
| Highest BMI-related mortality changes | Bangladesh: ↑ highest BMI-related deaths & DALYs | The poorest country with the fastest impact | |
| Turkey: ↓ BMI-related deaths (↓37.2%) & DALYs (↓43.7%) | Significant improvement | ||
| Metabolically Healthy Obese (MHO) | Some obese individuals have normal metabolisms (no hypertension/lipids) | The “MHO” group exists in all populations. | |
| CoLaus study (Switzerland) | Prevalence in Caucasians (35-70 years old): Overweight: 36.6%, Obesity: 15.7%, Hypertension: 36.7%, Hyperlipidemia: 34.2%, Diabetes: 6.6%, Microalbuminuria: 6.3% | Men had a higher prevalence than women. | |
| Global diabetes (IDF Atlas) | 8.8% prevalence (~415M cases in 2015) → expected 10.4% (~642M cases by 2040) | 2015-2040 | IDF |
| Highest diabetes prevalence in North America & the Caribbean (11.5%) | |||
| >50% of diabetics in Southeast Asia & Western Pacific | |||
| Future growth: The highest increase in diabetes is expected in sub-Saharan Africa (141%) & the Middle East/North Africa (104%) | Next 25 years | ||
| MetS global estimate | 1 billion+ people affected (~1/4 of the world population) | Based on the prevalence of diabetes, it is 1/3 of MetS cases. | |
| Prevalence variation by criteria | Iran (2007): MetS prevalence ATP III = 34.7%, IDF = 37.4%, and ATP III/AHA/NHLBI = 41.6% | Definition impacts estimates | |
| Tunisia: MetS IDF = 45.5%, ATP III = 24.3% | Higher prevalence in women than men (Middle East trend) |
Table 2: Global terms in MetS obesity and T2DM
Methodology
Literature search: A systematic literature search was conducted in PubMed, Web of Science, and Google Scholar, including the articles released until August 2025. The search strategy involved a combination of keywords and MeSH terms such as berberine, metabolic syndrome,” “insulin resistance, type 2 diabetes, obesity, dyslipidemia and hypertension combined with Boolean operators (AND, OR). Relevant papers were also screened in terms of their reference lists.
Inclusion criteria: peer-reviewed articles, original preclinical and clinical trials, authoritative organizational publications (WHO, Food and Agriculture Organization (FAO), World Organization for Animal Health (WOAH), United Nations (UN)) and high-impact review papers in relation to berberine and metabolic syndrome.
Exclusion criteria: Non-English papers (except those of high citation), non-peer-reviewed materials (blogs, newsletters, and conference abstracts), case reports, and papers not pertinent to berberine.
Study selection: Titles and abstracts were screened, followed by full-text assessment for eligibility. Two reviewers independently carried out the selection process, and disagreements were resolved by discussion. Only studies that met the inclusion criteria were considered. A total of 66 studies met the inclusion criteria and were included in this review.
Data extraction and synthesis: Data from the included studies were extracted and organized under five thematic categories: molecular mechanisms, clinical efficacy, pharmacokinetics, safety, and nanoformulation-based delivery systems.
Patterns in the association between metabolic disorders and cardiovascular disease: Prospective studies consistently demonstrate that MetS significantly increases CVD risk and mortality, often accelerating cardiovascular aging. The Vascular Risk in Navarre (RIVANA) cohort (Spain) showed that MetS individuals had 1.32x higher risk of major CVD events, 1.64x higher CVD mortality, and 1.45x higher all-cause mortality, experiencing CVD deterioration 3.2 years earlier. The Uppsala Longitudinal Study of Adult Men (ULSAM) reinforces these conclusions, indicating that even individuals of normal weight who have MetS are at a 1.63 times greater risk of CVD. In contrast, those with obesity and MetS encounter a 2.55 times higher risk. These results challenge the sole focus on obesity as the primary CVD driver, instead highlighting insulin resistance as a critical factor, even in “metabolically obese normal weight” individuals. ULSAM also revealed that metabolically healthy obesity (MHO) still carries an elevated CVD and mortality risk compared to normal-weight individuals, emphasizing that BMI alone is insufficient for assessing cardiovascular risk; metabolic health must also be considered.[13]
Japanese studies, although they exhibit lower obesity rates, affirm that MetS is a crucial predictor of CVD morbidity and mortality. A meta-analysis by Watanabe & Kotani of Japanese cohorts (Suita Study, Hisayama Study) found MetS increased CVD morbidity (hazard ratio (HR) = 1.71 for men, 1.89 for women) and mortality (HR = 1.68 for men, 1.73 for women), with a slightly higher risk in women. These studies underscore that while obesity contributes to MetS, other metabolic disturbances like hypertension and insulin resistance are equally crucial in driving CVD risk, particularly in populations with lower obesity prevalence.[14] The Second National Health and Nutrition Examination Survey (NHANES II) reported that MetS elevated the risk of CHD mortality by a factor of 2.02, CVD mortality by a factor of 1.82, and overall mortality by a factor of 1.40. Even non-diabetic individuals with MetS had elevated CHD (HR = 1.65) and CVD (HR = 2.32) mortality risks, indicating MetS’s independent contribution to cardiovascular death.[15] The Cardiovascular Health Study (CHS) in older adults found MetS increased risks for CHD (HR = 1.30-1.35), stroke (HR = 1.51 in men), and congestive heart failure (HR = 1.40-1.47). Hypertension was the strongest predictor of CHD, reinforcing findings from Japanese studies. The CHS also suggested that even mild metabolic disturbances contribute to CVD risk.[16]
Supplemental treatments for metabolic syndrome: Limitations of conventional treatments: Statins for cholesterol issues, blood pressure medications, and diabetic medications are often used as therapy for MetS. They still have certain restrictions, though. Statins can effectively reduce low density lipoprotein cholesterol (LDL-C) levels and the risk of heart disease, but they usually don’t treat other lipid problems, such as high triglycerides and low high-density lipoprotein (HDL). Additionally, statin use may occasionally result in increased liver enzymes, muscular weakness, and an increased risk of diabetes.[17,18] According to the Joint National Committee on Blood Pressure, the main approach to managing hypertension is to give regular pharmacological treatment and put little emphasis on food and lifestyle changes as the disease progresses. In addition, the unclear detection of IR (a prominent feature of MetS) and the limited options for treating it have led to the need for insulin to manage blood sugar, indicating the failure of controlling sugar as the key effort.[17,19]
Besides, issues with medication tolerance and patient compliance reduce how effective traditional regimens are. In specific individuals with MetS, liver issues resulting from statin use may be attributed to liver dysfunction or non-alcoholic fatty liver disease.[18]
An overview of berberine and metabolic syndrome
Berberine has a chemical representation of C₂0H₁8NO₄+ and its molar mass is 337.37 g/mol.[20] The protoberberine alkaloid is primarily extracted from the medicinal plants Berberis vulgaris, Berberis aquifolium, Berberis aristata, Coptis chinensis, and Phellodendron amurense.[21,22] Most alkaloids in these plants are in their roots, rhizomes, bark, stems, and leaves. Most often, they are taken to clinics using ethanol and methanol.[20]
For countless generations, both Traditional Chinese Medicine (TCM) and Ayurveda have depended on berberine to treat infections, inflammation, diabetes, and illnesses of the stomach. It was in early Assyrian texts from around 650 BC that we first read about using artemisia to cleanse the blood.[23]
Berberine has been found to support treatment in many studies concerning metabolic syndrome. New research has found that Berberine can reduce blood sugar, lower body fat, ease inflammation, and act against the effects of oxidative damage[20,24,25] Eating probiotics controls bacteria in your digestive system, helps reduce general swelling, and is helpful for MetS management.[22,26] As a result, cells take in more glucose, the body responds to insulin more effectively, and lipids are produced less.[24,27] Berberine helps lower blood sugar like metformin and thiazolidinediones, as it boosts energy-burning genes and decreases those that control lipid formation.[22] Furthermore, berberine enhances glycolysis, suppresses glucose production in the liver, and facilitates the activity of glycokinase. It also boosts the expression of glucose transporter type-4 (GLUT-4) and glucagon like peptide-1 (GLP-1), which helps the body use glucose properly and respond to insulin.[27]
The medication has been shown to be very effective in reducing lipid levels as well. It enhances the availability of LDL receptors on cells by stabilizing LDL receptor mRNA. It decreases the transcription rate of proprotein convertase subtilisin/Kexin type-9 (PCSK9), which results in a more efficient removal of LDL from the bloodstream. It acts as an anti-inflammatory agent in part by affecting transcription factors such as Peroxisome Proliferator Activated Receptor Gamma (PPARγ), turning off the Mitogen Activated Protein Kinase/Extracellular Signal Regulated Kinase (MAPK/ERK) pathway, and disrupting the activities of cyclooxygenase-2 (COX-2) and prostaglandin E2.[21,23,28]
As a result, these mechanisms make a difference in the health of people with MetS. Researchers in clinical trials have found that berberine supplementation can cut fasting plasma glucose (FPG), postprandial glucose (PPG), hemoglobin A1c (HbA1c), fasting plasma insulin (FPI), and hemostatic model assessment of insulin resistance (HOMA-IR), the main markers related to insulin resistance. In trials on patients with poorly controlled T2DM, berberine helped improve blood sugar and cholesterol levels in a way very similar to the standard medication metformin. Using berberine led to a cut in waist circumference, triglyceride levels, and systolic blood pressure, with the most effect seen in women who have MetS.[22,27]
According to Belwal et al., when treating non-alcoholic fatty liver disease, a disease that develops in MetS, using berberine along with lifestyle changes is superior to pioglitazone in lowering fat in the liver, changing lipid levels, and helping patients lose weight.[29]
Berberine helps the heart by increasing blood vessel dilation, reducing cholesterol levels, lowering inflammation, and improving endothelial health, all factors that protect against heart risks connected with MetS. Most people find that berberine is safe to use, though a few experience gentle gastrointestinal problems, like nausea or constipation. Because it can stop cytochrome P450 enzymes from working, patients should use it with care, together with prescription pharmaceuticals. Pregnant or breastfeeding women should not consume this food.[27]
Because of its actions on glucose and lipid metabolism, insulin, inflammation, and gut function, berberine may be helpful in treating metabolic syndrome in addition to standard treatments. Both its traditional roots and strong proof from science promote its increased influence on metabolic care.
Mechanism of action of berberine: Regulation of glucose metabolism and insulin sensitivity.
AMPK activation and GLUT4 upregulation: Berberine stimulates AMPK, which improves glucose absorption in skeletal muscle and decreases hepatic gluconeogenesis. Additionally, it elevates the expression of GLUT4, thereby aiding in glucose uptake.[30]
Inhibition of α-glucosidase: Berberine acts as an inhibitor of α-glucosidase, which slows down the digestion of carbohydrates and the absorption of glucose in the intestine, thereby aiding in improved glycemic control.[30] Lipid metabolism modulation LDL receptor (LDL-R) upregulation and inhibition of PCSK9. Berberine promotes the clearance of LDL-C by increasing the expression of LDL receptors in hepatocytes. Additionally, it inhibits PCSK9, which improves the metabolism of cholesterol and LDLR integrity.[31]
Reduction in lipogenesis: Berberine inhibits the sterol regulatory element-binding protein 1c (SREBP-1c), leading to a decrease in the synthesis of fatty acids and triglycerides in the liver.[30]
Antihyperlipidemic activity of berberine: A significant role played by heterogeneous nuclear ribonucleoprotein I and K Homology (KH)-type regulatory proteins in modulating the stability of LDL-R mRNA in liver cells is inhibited by berberine. Furthermore, berberine enhances transcriptional activity of the LDL-R promoter through the c-Jun N-terminal kinase (JNK) pathway.[32] Additionally, it inhibits the degradation of LDL-R by obstructing the I gene, which is one of the most significant effectors of LDL-R degradation. Besides, berberine inhibits the action of PPAR-gamma, fatty-acid synthase, acetyl-CoA carboxylase, acyl-CoA synthas, and lipoprotein lipase, which influence the formation of lipids in the endoplasmic reticulum. Overall, the findings underscore the enhancing impact on liver function and the increased production of bile acids by berberine, thereby improving the lipid profile and likely contributing to the lipid-lowering efficacy of this compound. Given that barberry juice contains potent polyphenolic constituents, we can hypothesise that, in addition to the active polyphenolic fraction, the active chemical cerberin is associated with the cholesterol-lowering effect.[33,34]
Antioxidant and anti-inflammatory properties: Suppressing the nuclear factor kappa B (NF-κB) pathway: Berberine suppresses the activity of NF-κB, leading to a reduction in the synthesis of pro-inflammatory cytokines.[31]
Enhancing the nuclear factor erythroid 2-related factor 2 (Nrf2) pathway: Berberine stimulates Nrf2, enhancing the expression of antioxidant enzymes and reducing oxidative damage.[31]
Gut microbiota modulation
Increasing beneficial bacteria: Recent studies reinforce berberine’s ability to act on multiple pathways. This includes not only AMPK activation but also modulation of gut microbiota, which is now recognized as a very important factor in metabolic health.[33] Berberine positively influences gut microbiota composition, enhancing the growth of short-chain fatty acid (SCFA)-producing bacteria, which improves gut barrier integrity and metabolic functions.[31]
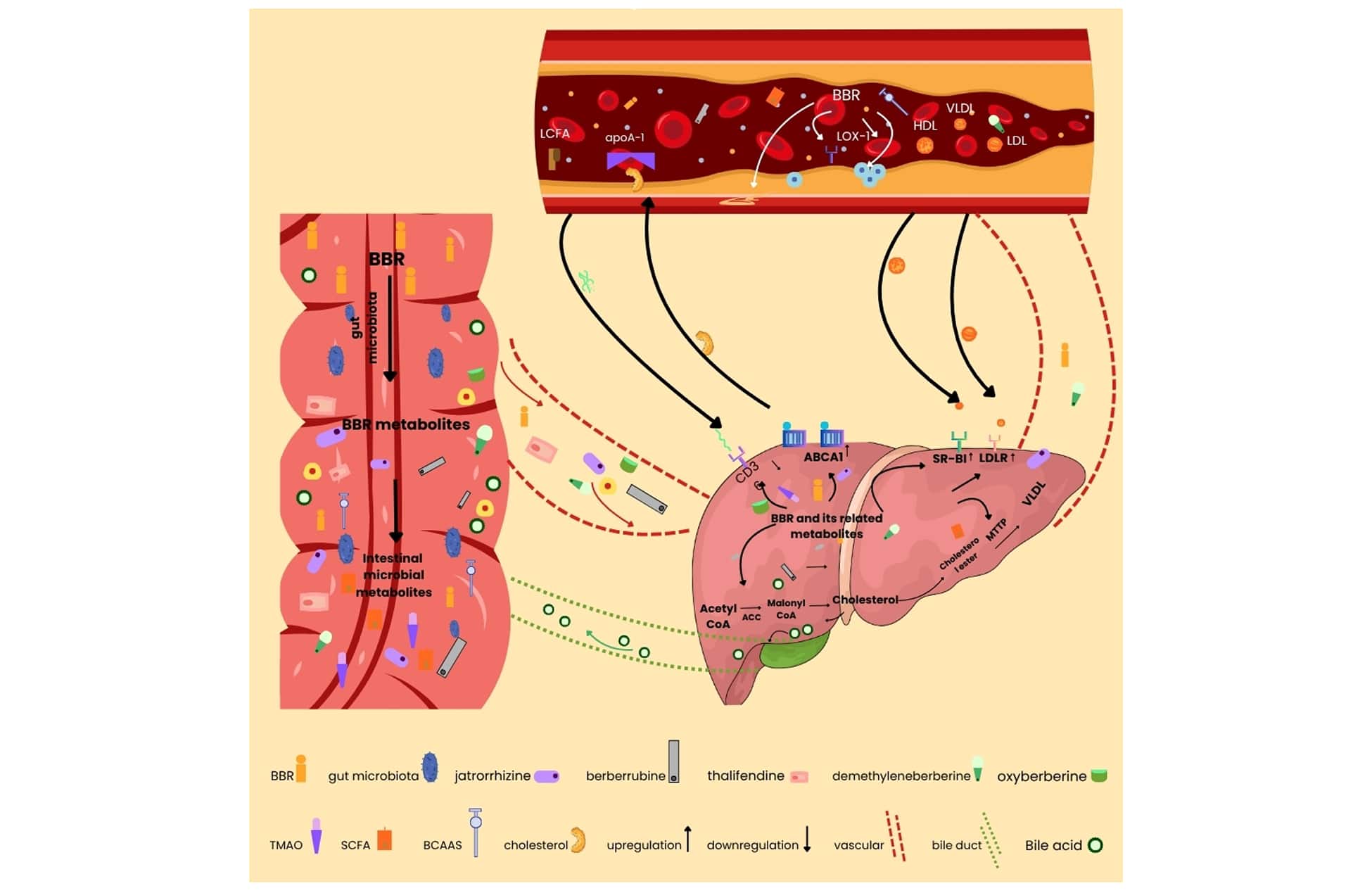
Figure 1: The image illustrates how berberine and gut microbiota influence cholesterol, lipid metabolism, and liver function through the gut-liver axis
The text outlines the hypothesis that focuses on the gut-to-liver pathway through which berberine may be utilized to prevent and manage lipid metabolic disorders. Upon oral intake, berberine interacts with the intestinal environment and acts as a substrate for the native bacterial enzymes; these microbial activities convert berberine into thalifendine, berberrubine, jatrorrhizine, and demethylberberine. Berberine and its subsequent metabolites affect intestinal and hepatic functions, thereby influencing the circulating lipid levels. Specifically, berberine inhibits trimethylamine-N-oxide (TMAO), SCFA, and intestinal branched-chain amino acids, along with metabolites generated in the intestine that enter the portal circulation. The liver’s clearance of circulating lipids and the suppression of hepatic lipogenesis are facilitated by the prevention of bile acid and LDL-R gene expression, as well as the activation of liver ATP-binding cassette transporter A1, scavenger receptor class B type 1, microsomal triglyceride transfer protein (MTTP), acetyl-CoA carboxylase (ACC), and liver cluster of differentiation 36, all stimulated by this flow of metabolites. Significantly, the absorption of these metabolites into the arterial blood tree inhibits the formation of macrophage foam cells, curtails the proliferation of vascular smooth muscle cells, and ultimately helps to prevent atherosclerosis. Key components involved in this system include apoA-1, HDL, long-chain fatty acids (LCFA), LDL, the lectin-like oxidized LDL receptor (LOX-1), and very low LDL.
Clinical evidence of berberine in metabolic syndrome: To assess berberine’s cardiovascular effects, a phase 2/3 mechanistic randomized controlled clinical trial was carried out. 84 Chinese men with hyperlipidemia, ages 20 to 65, were involved in the study. Strict inclusion criteria were applied to carefully select the participants and include the absence of any congenital or infectious diseases, anemia, glucose-6-phosphate dehydrogenase deficiency, no berberine or any trademark of traditional Chinese medicine bearing any berberine components have been taken during the last month, and they have not undergone hormonal replacement therapy (including testosterone replacement) in the previous 12 months. Additionally, people having a history of chronic illnesses such as cancer, diabetes, myocardial infarction, stroke, ischemic cardiovascular disease, liver or kidney disease, and gastrointestinal issues are included. Over the course of 12 weeks, the individuals were observed. The results showed that berberine raised male serum testosterone levels while also successfully lowering total cholesterol and LDL-C levels. Crucially, no severe side effects were recorded, indicating that berberine was well tolerated. HDL-C, TG, thromboxane A2, blood pressure, waist-to-hip ratio, and BMI, however, did not change significantly.[34]
In the same tune, Phase 4 double-masked, placebo-controlled clinical trials were executed among individuals with moderate to low risk of hypercholesterolemia (R4 33) to establish long-term safety and tolerability of combination of nutraceuticals consisting of red yeast rice, policosanols, and berberine myelin basic protein-noncomplex (MBP-NC). Sixty individuals between the ages of 18 and 60 who had just been diagnosed with primary hypercholesterolemia and had not previously received treatment were included in the trial. Participants were eligible if their BMI was between 18.5 and 29.9 kg/m2, their serum levels of LDL were greater than 150 mg/dL, and their Framingham risk score indicated that their 10-year cardiovascular risk was under 20 percent after three weeks of a stable hypolipidemic diet.[35]
In another line of investigation, Phase 2 clinical studies have been conducted to evaluate the effect of berberine hydrochloride in preventing the recurrence of colorectal adenomas. The study included 1,108 adults aged 18 to 75 years who had between one and six colorectal adenomas removed within six months prior to enrollment. Participants with a family history of hereditary adenomatous polyps, hereditary colorectal cancer without polyposis (Hereditary Non-Polyposis Colorectal Cancer, or Lynch syndrome), subtotal or total gastrointestinal surgery, or partial bowel resection were not allowed to participate in the study if their adenomas had not been removed during a prior colonoscopy. The study evaluated changes in fecal microbiota, polypoid lesions, advanced colorectal adenomas, colorectal cancer, and the recurrence rate of colorectal adenomas. According to the promising results, berberine hydrochloride at a dosage of 0.3 g twice a day was safe and effective, effectively reducing the incidence of colorectal adenoma recurrence.[36]
Moreover, Phase 4 clinical trials were conducted to assess the effects of berberine on clinical symptoms and metabolic disturbances in patients with schizophrenia. Sixty-five people between the ages of 18 and 65 who satisfied the DSM-IV diagnostic criteria for schizophrenia were included in the study. Every participant had a Positive and Negative Syndrome Scale (PANSS) score of at least 60 and had been receiving atypical antipsychotic monotherapy for at least four weeks. Patients were given Berberine along with their continued antipsychotic medication for eight weeks. The findings showed that berberine injection significantly decreased LDL-C and plasma total cholesterol (TC) levels. Furthermore, a significant decline in HOMA-IR and fasting insulin levels was noted. The patients’ metabolic response to berberine appeared to be BMI-dependent, with those exhibiting higher serum prolactin levels experiencing a diminished therapeutic effect.[37]
In an early-phase investigation, a Phase 1 clinical study was conducted to evaluate the effects of berberine in individuals with diabetes mellitus. The study included 15 healthy male adults between the ages of 18 and 45 who had a BMI of 18 to 25 kg/m2, a standard oral glucose tolerance test before enrollment, no family history of diabetes mellitus, and no history of medication use during the study period or in the four weeks prior to the baseline visits. The outcomes demonstrated that the berberine enhanced the insulin release in dependence on the available glucose. Although it did not affect the release of insulin with low glucose concentrations, it also significantly induced insulin secretion in a dose-dependent manner with high glucose levels. Furthermore, berberine was shown to enhance insulin release through blockade of KCNH6 channels in a glucose-dependent or hyperglycemic context. Significantly, berberine did not induce hypoglycemia, indicating its potential safety in modulating insulin dynamics.[38]
Comparative studies with standard medications
T2DM: Patients with T2DM have shown great success with berbehaemoglobin A1c levels, TC, LDL-C, FBG and postprandial blood glucose levels (PPBG). In comparison with rosiglitazone and metformin, berberine has a similar hypoglycemic effect, but its effect on serum TG and TC levels is stronger and more substantial. In clinical settings, berberine is commonly used in conjunction with glipizide, metformin, and glimepiride, among other oral hypoglycemic medications. As a result of combining berberine with these drugs, patients with T2DM have been shown to have lower blood glucose levels and better lipid profiles than those treated with monotherapy. Berberine has also been shown to decrease insulin resistance, a key pathological feature of diabetes. Several clinical trials have demonstrated that berberine significantly increases 1-hour and 2-hour postprandial insulin levels, indicating its ability to enhance insulin secretion. In addition to its metabolic effects, berberine also exhibits anti-inflammatory properties. It significantly reduces the levels of pro-inflammatory cytokines such as interleukin-6, tumor necrosis factor-alpha (TNF-α)), and C-reactive protein (CRP) in diabetic patients, contributing to improved insulin sensitivity and glycemic control.[39]
Hyperlipidemia: The effectiveness of berberine as a therapy for hyperlipidemia was initially documented in 2004. For three months, people with hypercholesterolemia were given 0.5 g of berberine twice a day as part of a placebo-controlled clinical experiment. When compared to a placebo, the medication significantly decreased the levels of TG, LDL-C, and TC. Furthermore, by considerably reducing serum levels of hepatic health indicators such as alanine aminotransferase (ALT), gamma-glutamyl transpeptidase, and aspartate aminotransferase (AST), berberine showed a positive impact on liver function.[40]
A comparative study assessed the therapeutic effects of berberine in comparison to simvastatin and atorvastatin in patients suffering from hyperlipidemia. After eight weeks of treatment, berberine significantly decreased TC, TG and LDL-C levels. Importantly, berberine was more effective in lowering TC levels than simvastatin and more efficient in reducing TG levels than atorvastatin. Furthermore, the combination of berberine with simvastatin yielded superior lipid-lowering effects compared to either medication used alone. These results indicate that berberine may act as an ideal adjunct to statin therapy, presenting a promising strategy for the advancement of new treatments for hyperlipidemia.[41]
Gout: Berberine has shown encouraging clinical effectiveness in treating hyperuricemia and gout. A study conducted by Wu et al. revealed that the oral intake of berberine in conjunction with or period led to a significant decrease in serum uric acid (UA) levels among patients suffering from hyperuricemia, resulting in an effective rate of 83%. These results underscore the potential of berberine as a viable therapeutic alternative for the management of hyperuricemia and its related complications.[42]
Recently, Wang and colleagues conducted a study on the effectiveness of berberine when used alongside benzbromarone for treating patients suffering from gout. Their results indicated that berberine notably reduced serum UA levels and enhanced related metabolic disorders.[43] Furthermore, the combination of berberine with amlodipine has shown substantial clinical benefits in elderly patients suffering from both gout and hypertension, effectively reducing blood pressure as well as serum UA levels.[44]
Safety Profile and Adverse Effects: Although berberine shows great potential in the treatment of metabolic diseases, its safety and potential side effects warrant careful consideration. Most animal studies and clinical trials have demonstrated low toxicity associated with berberine administration.[45]
Huang et al. evaluated the cytotoxicity and acute toxicity of berberine in vitro and in vivo, reporting half maximal inhibitory concentration (IC₅₀) values of 48.17 μg/mL in HepG2 cells and 41.76 μg/mL in 3T3-L1 adipocytes. The 50% lethal dose (LD₅₀) in acute toxicity assays was determined to be 713.57 mg/kg in mice. Furthermore, rats treated with berberine at 156 mg/kg/day for three months showed no signs of mortality or morbidity.[46]
Belwal et al. highlighted that the LD₅₀ of berberine varies depending on the route of administration: intravenous and intraperitoneal injections had LD₅₀ values of 9.04 mg/kg and 57.61 mg/kg, respectively, while no LD₅₀ was observed following oral administration. Clinically, berberine doses ranging from 0.4 g/day to 1.5 g/day have been used for treating various metabolic conditions without observable adverse effects on the liver.[47]
A few clinical studies have shown modest gastrointestinal adverse effects, such as anorexia, nausea, vomiting, diarrhea, constipation, and flatulence, that are associated with berberine administration. A study of 59 patients who received 0.5 g of berberine three times a day for 13 weeks, for example, found that 34.5% of them had gastrointestinal side effects, most of which were temporary and occurred within the first four weeks. Notably, reducing the dose to 0.3 g thrice daily eliminated these adverse effects.[48]
Overall, berberine-induced side effects in humans are generally mild, transient, and dose-dependent. Considering its substantial health benefits, the safety profile of berberine appears favorable. However, despite promising data from animal and short-term human studies, long-term toxicity studies in humans remain insufficient, underscoring the need for further research.
Drug interactions of berberine
| Interaction | Effect | Mechanism |
| Doxorubicin | Synergistic Anticancer Effect | Sensitization of cells to doxorubicin, enhancing its anticancer efficacy |
| L-DOPA | Antagonistic effect on dopaminergic neurons | In the substantia nigra, chronic co-administration causes dopaminergic neurons to degenerate. |
| β-Lactam Antibiotics | Synergistic effect against Methicillin-Resistant Staphylococcus aureus (MRSA) | This increases the sensitivity of MRSA to oxacillin, cefazolin, and ampicillin. |
| Fluconazole | Enhanced activity against fluconazole-resistant Candida albicans | Potent in vitro synergism, improving antifungal efficacy against resistant strains |
| Cisplatin | Enhanced cytotoxic effect | Activates caspases, causes mitochondrial membrane potential to drop, and releases cytochrome-c, all of which contribute to cell death.
|
| Warfarin, Thiopental | Precipitation of toxicity | Displacement from protein binding sites results in elevated levels of free drug in the bloodstream. |
| Cyclosporin-A | Increase in blood concentration | Inhibition of CYP3A4, leading to reduced metabolism and increased blood levels of cyclosporin-A |
| Tetrandrine | Potentiation of Berberine’s hypoglycemic effect | Inhibition of P-glycoprotein efflux leads to improved absorption and bioavailability of berberine. |
| Metformin | Synergic hypoglycemic effect | Berberine obstructs the movement of metformin via OCT1 and OCT2, which may lead to an increase in plasma concentration and the effects of metformin. |
| Sulfonylureas (Glyburide, Gliclazide) | Synergic hypoglycemic effect | Berberine is a strong competitive inhibitor of the CYP3A and CYP2C isozymes, thereby reducing sulfonylurea’s metabolism and increasing the levels of sulfonylureas, subsequently intensifying their hypoglycemic effects. |
| Simvastatin | Increased statin effect | Inhibits CYP3A4 and P-glycoprotein, reducing statin metabolism and clearance. |
Table 3: shows drug interactions of Berberine, highlighting potential pharmacokinetic and pharmacodynamic implications[49-57]
Limitations and challenges of berberine: Berberine exhibits low oral bioavailability due to its inadequate absorption in the intestinal tract. It is categorized as a Class III substance in the Biopharmaceutics Classification System (BCS), characterized by high solubility but low permeability. Consequently, small amounts of the orally administered berberine reach systemic circulation. Even this minute amount absorbed is thoroughly metabolized within the liver and intestines prior to producing systemic effects. This “first-pass effect” involves cytochrome P450 enzymes, where berberine is converted into inactivated or less active metabolites, reducing its plasma concentration. Even though berberine has been designated as highly water-soluble, its inherent solubility in biological fluids is relatively low, and that lowers its oral absorption. A low solubility makes its aqueous or injectable formulation more difficult.[58] Berberine has a low and limited half-life (a few hours), and this necessitates frequent dosing to provide sustained plasma levels. This is problematic in chronic treatment, particularly in conditions such as diabetes or hyperlipidemia, where sustained drug exposure is required.[59] Because berberine is widely sold as a dietary supplement, it is not subject to pharmaceutical-grade regulations. Over-the-counter products vary extensively in the accuracy of their dosing, purity, and dissolution profiles, thus compromising clinical effect and safety. Variability in the berberine quality and concentration present in commercial supplements is a problem. Irreproducibility of clinical results and complicating regulatory monitoring can result from inconsistent formulations.[60]
Prospects: advancing berberine for metabolic syndrome management
Nano formulations: Future research should focus on addressing Berberine’s major limitation: its low oral bioavailability and extensive first-pass metabolism, which significantly hinders its therapeutic potential despite its promising pharmacological properties. The most promising approach is the development and optimization of sophisticated nanoformulations. Strategies such as polymeric nanoparticles for instance, polylactic co-glycolic acid (PLGA) a chitosan, solid lipid nanoparticles (SLNs), nanostructured lipid carriers (NLCs), liposomes, and self-micro emulsifying drug delivery systems (SMEDDS) offer significant potential.[61] When exposed to a low pH environment, like the stomach, the nanoparticles can load berberine very steadily. Nevertheless, in a high pH environment, such as that found in the intestine, they are capable of releasing berberine with greater ease.[62] These nanocarriers can improve berberine’s solubility, safeguard it from degradation in the gastrointestinal tract, encourage lymphatic absorption to circumvent first-pass metabolism, and enable sustained or targeted release. Future research must concentrate on not only proving improved absorption and systemic exposure in rigorous preclinical models but also on optimizing manufacturing processes, guaranteeing long-term stability, thoroughly assessing nanocarrier toxicity, and maneuvering through the intricate regulatory frameworks necessary for the clinical implementation of these advanced delivery systems.[63]
Combination therapies: Due to the intricate and multiple pathophysiology of MetS, monotherapy frequently proves inadequate. Subsequent research should thoroughly examine the potential of berberine in systematic combination tactics. This encompasses synergistic combinations with other recognized nutraceuticals (e.g., curcumin, resveratrol, omega-3 fatty acids, cinnamon extract, probiotics aimed at the gut microbiome) and conventional pharmaceuticals (e.g., metformin, statins, gloxazones, SGLT2 inhibitors, GLP-1 receptor agonists).[64] Research should advance beyond basic additive effect studies to clarify the specific molecular mechanisms that underpin potential synergies, including complementary actions on AMPK activation, insulin signaling, inflammatory pathways such as NF-κB, NOD-, LRR-, and pyrin domain-containing protein 3 NLRP3 inflammasome, lipid metabolism regulators such as Sterol Regulatory Element-Binding Proteins (SREBP), PPARs, and the composition/function of gut microbiota. Essential future research entails identifying the most effective and safe combination partners, establishing optimal dosing regimens (sequential versus concurrent), evaluating potential pharmacokinetic interactions, and assessing long-term safety profiles of these combinations in pertinent preclinical models prior to advancing to human trials. Integrating Berberine’s multiple effects with medicines possessing complementary mechanisms presents an effective technique for attaining enhanced management of MetS.[65]
Large-scale clinical trials: Although current clinical data on berberine for the components of MetS (insulin resistance, dyslipidemia, hypertension, adiposity) is promising, it is significantly limited by factors including small sample sizes, brief study durations, diverse study designs, inconsistent sources/formulations of berberine, and occasionally insufficient control groups.[66] Designing and executing large, multicenter, randomized, double-masked, placebo-controlled clinical trials (RCTs) with extended follow-up periods (e.g., 1-2 years or more) is the crucial next step. Clinically relevant primary endpoints (e.g., incidence of type 2 diabetes or cardiovascular events, changes in validated MetS severity scores) must be used in these trials, along with well-defined MetS populations, standardized, high-quality berberine formulations (possibly including optimized nano formulations), and comprehensive secondary endpoints that cover all MetS components and safety considerations.[67] Future studies should investigate the effects of berberine on different MetS phenotypes and ethnic groups, incorporate biomarker discovery (e.g., omics methodologies) to find responders, assess the long-term sustainability of benefits and safety, and, if feasible, evaluate its impact on definitive cardiovascular outcomes. Moreover, comparative effectiveness research against existing standard-of-care drugs is essential to determine berberine’s true therapeutic position in MetS management, as some studies show benefits while others report modest or inconclusive outcomes. Additionally, real-world evidence studies needed to assess its practical significance, long-term effectiveness, and variability in patient responses across routine clinical settings.[68,69]
Results
Because of its multiple mechanisms of action, including AMPK activation, control of glucose and fatty acid metabolism, antioxidant and anti-inflammatory effects, manipulation of the microbiota of the gut, and support for cardiovascular health, berberine shows great promise as an adjunctive treatment for MetS. Clinical studies show that, in addition to performing as well as certain conventional medications, it can enhance body composition, lipid profiles, glycemic control, and overall metabolic health. It does, however, face challenges like low bioavailability and wildly inconsistent clinical results. When combined with other medications, new developments in nanoforms could be beneficial. Anyone interested in natural or integrative methods should give berberine some thought because it has a natural origin and a better risk profile than any allopathic medication. Berberine displays a better safety profile than any allopathic therapy and has a natural origin, making berberine a reasonable consideration for anyone interested in natural/integrative approaches. Larger, well-designed trials are warranted to clarify its long-term efficacy and rationalize its clinical applications.
Discussion
MetS refers to a cluster of clinical syndromes that are determined by heredity, environment, habits of living, and other factors, whose primary mechanism is insulin resistance. Symptoms in patients include central obesity, atherosclerosis, increase in blood lipid, Patho glycemia and hypertension increase, which can be accompanied by microalbuminuria, hyperuricemia and chronic inflammatory cytokine rise lasting for an extended period of time. The current review has demonstrated the superior protective action of berberine on diverse metabolic disorders of MetS, which has merits of extensive medicinal herbs resources, low cost, smaller side reactions, and being safe and easy. Berberine activates AMPK, suppresses α-glucosidase, enhances the removal of LDL-C, suppresses NF-κB, activates Nrf2.[70] Berberine assists the heart by enhancing blood vessel relaxation, decreasing cholesterol levels, decreasing inflammation, lowering blood glucose, decreasing BMI and enhancing endothelial function. Our review also assessed that berberine is of poor oral bioavailability because it is not well absorbed in the intestine. Although berberine has been classified as highly water-soluble, its intrinsic solubility in biological media is somewhat low, and that decreases its oral absorption. The half-life of berberine is low and restricted (a few hours), and this requires dosing frequently in order to achieve sustained plasma levels. Over-the-counter formulations vary widely in the reliability of their dosage, purity, and dissolution profiles and therefore compromise both clinical efficacy and safety. Irreproducibility of clinical outcomes and confounding regulatory tracking can follow from variable formulations.[71,72]
Before we can interpret our results further, we should note a sequence of critical limitations. It does not explore extensively regulatory gaps and quality control issues in the’ sale of berberine-like dietary supplements in most areas. It does not talk about pharmacogenomic variability and personalized response as these factors influence safety and efficacy profiles. Though gut microbiota discussed, greater emphasis is required on how it not only alters berberine metabolism but also how it works as a biomarker for predicting therapeutic outcome. There is increasing interest in application of berberine for PCOS, obesity, and oncology adjunct therapies, which are not addressed in our articles.[73]
From our analysis, various issues still exist to be addressed concerning the administration of berberine. For the first time, the oral bioavailability of berberine in vivo is low because of first-pass elimination. It thus becomes imperative to explore other modes and mechanisms of drug delivery with a focus on enhancing the bioavailability of berberine. Various researchers have demonstrated that strategic application of nanotechnology, such as appropriately designed nanocarriers, liposomes, and microfluidic technology-enabled preparation techniques, may enhance berberine bioavailability for application in metabolic disorders.[74] In HepG2 liver cancer cells, water-soluble and synthetic berberine derivatives with modified 9-O-monosaccharides (given at concentrations of 0.2, 1, and 5 μg/ml) exhibited antidiabetic activity, with less cytotoxicity and a IC50 almost 1.5 times smaller than that of unmodified berberine. Berberine structural modification can also enhance bioavailability and activity while minimizing unfavorable drug effects. This review also indicated that little research has been conducted on the toxicity of berberine and its analogues. Systematic toxicology studies, particularly those considering cumulative toxicity in vivo, need to be conducted given the long-term establishment for preventing and treating metabolic diseases. If the side effects caused by drug accumulation are to be minimized, it is also essential to consider addressing berberine’s toxicity and efficacy for application in human pharmacokinetic studies. The determination of the most appropriate dosage is equally essential. Standardizing the dosage, route of administration, administration period, and side effect of berberine could thus be explored in clinical trials with the aim of optimizing therapeutic effectiveness as well as safety.[75]
Conclusion
Berberine shows significant promise as an adjunct therapy for the management of MetS due to its multi-target mechanisms and generally favorable safety profile. However, further research is required, particularly focusing on improved formulation strategies and more robust clinical evidence to better establish its therapeutic efficacy.
References
- Oda E. Metabolic syndrome: its history, mechanisms, and limitations. Acta Diabetol. 2012;49(2):89-95. doi:10.1007/s00592-011-0309-6
PubMed | Crossref | Google Scholar - Kassi E, Pervanidou P, Kaltsas G, Chrousos G. Metabolic syndrome: definitions and controversies. BMC Med. 2011;9:48. doi:10.1186/1741-7015-9-48
PubMed | Crossref | Google Scholar - Bangash SA, Sharma RD, Rehman S et al. Unraveling the efficacy of traditional herbal remedies against multi-drug resistant bacterial infections: a comprehensive study of pathological impact, microbial resistance mechanisms, clinical relevance, and biochemical pathways. Kurdish Stud. 2024;12:1764-1769. doi:10.53555/ks.v12i4.3650
Crossref | Google Scholar - Saklayen MG. The global epidemic of the metabolic syndrome. Curr Hypertens Rep. 2018;20(2):12. doi:10.1007/s11906-018-0812-z
Crossref | Google Scholar - Herman WH, Rothberg AE. Prevalence of Diabetes in the United States: A Glimmer of Hope? JAMA. 2015;314(10):1005-1007. doi:10.1001/jama.2015.10030
Crossref | Google Scholar - Palaniappan LP, Wong EC, Shin JJ, Fortmann SP, Lauderdale DS. Asian Americans have greater prevalence of metabolic syndrome despite lower body mass index. Int J Obes (Lond). 2011;35(3):393-400. doi:10.1038/ijo.2010.152
PubMed | Crossref | Google Scholar - Delavari A, Forouzanfar MH, Alikhani S, Sharifian A, Kelishadi R. First nationwide study of the prevalence of the metabolic syndrome and optimal cutoff points of waist circumference in the Middle East: the national survey of risk factors for noncommunicable diseases of Iran. Diabetes Care. 2009;32(6):1092-1097. doi:10.2337/dc08-1800
PubMed | Crossref | Google Scholar - Wildman RP, Muntner P, Reynolds K, et al. The obese without cardiometabolic risk factor clustering and the normal weight with cardiometabolic risk factor clustering: prevalence and correlates of 2 phenotypes among the US population (NHANES 1999-2004). Arch Intern Med. 2008;168(15):1617-1624. doi:10.1001/archinte.168.15.1617
Crossref | Google Scholar - Wang Y, Mi J, Shan XY, et al. Is China facing an obesity epidemic and the consequences? The trends in obesity and chronic disease in China. Int J Obes. 2007;31:177-188. doi:10.1038/sj.ijo.0803354
Crossref | Google Scholar - Ogurtsova K, da Rocha Fernandes JD, Huang Y, et al. IDF Diabetes Atlas: global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res Clin Pract. 2017;128:40-50. doi:10.1016/j.diabres.2017.03.024
Crossref | Google Scholar - Firmann M, Mayor V, Vidal PM, et al. The CoLaus study: a population-based study to investigate the epidemiology and genetic determinants of cardiovascular risk factors and metabolic syndrome. BMC Cardiovasc Disord. 2008;8. doi:10.1186/1471-2261-8-6
PubMed | Crossref | Google Scholar - GBD 2015 Obesity Collaborators. Health effects of overweight and obesity in 195 countries over 25 years. N Engl J Med. 2017;377(1):13-27. doi:10.1056/NEJMoa1614362
PubMed | Crossref | Google Scholar - Guembe MJ, Fernandez-Lazaro CI, Sayon-Orea C, Toledo E, Moreno-Iribas C; RIVANA Study Investigators. Risk for cardiovascular disease associated with metabolic syndrome and its components: a 13-year prospective study in the RIVANA cohort. Cardiovasc Diabetol. 2020;19(1):195. doi:10.1186/s12933-020-01166-6
PubMed | Crossref | Google Scholar - Watanabe J, Kotani K. Metabolic Syndrome for Cardiovascular Disease Morbidity and Mortality Among General Japanese People: A Mini Review. Vasc Health Risk Manag. 2020;16:149-155. doi:10.2147/VHRM.S245829
PubMed | Crossref | Google Scholar - Malik S, Wong ND, Franklin SS, et al. Impact of the metabolic syndrome on mortality from coronary heart disease, cardiovascular disease, and all causes in United States adults. Circulation. 2004;110(10):1245-1250. doi:10.1161/01.CIR.0000140677.20606.0E
PubMed | Crossref | Google Scholar - Mozaffarian D, Kamineni A, Prineas RJ, Siscovick DS. Metabolic syndrome and mortality in older adults: the Cardiovascular Health Study. Arch Intern Med. 2008;168(9):969-978. doi:10.1001/archinte.168.9.969
PubMed | Crossref | Google Scholar - Scheen AJ. Management of the metabolic syndrome. Minerva Endocrinol. 2004;29(2):31-46.
Management of the metabolic syndrome - Patti AM, Al-Rasadi K, Giglio RV, et al. Natural approaches in metabolic syndrome management. Arch Med Sci. 2018;14(2):422-441. doi:10.5114/aoms.2017.68717
PubMed | Crossref | Google Scholar - Hollander JM, Mechanick JI. Complementary and alternative medicine and the management of the metabolic syndrome. J Am Diet Assoc. 2008;108(3):495-509. doi:10.1016/j.jada.2007.12.007
Crossref | Google Scholar - Mana T, Devi OB, Singh YD. Therapeutic application of berberine: a consolidated review. Curr Pharmacol Rep. 2023;9:329-340. doi:10.1007/s40495-023-00330-2
Crossref | Google Scholar - Och A, Och M, Nowak R, Podgórska D, Podgórski R. Berberine, a Herbal Metabolite in the Metabolic Syndrome: The Risk Factors, Course, and Consequences of the Disease. Molecules. 2022;27(4):1351. doi:10.3390/molecules27041351
PubMed | Crossref | Google Scholar - Rochlani Y, Pothineni NV, Kovelamudi S, Mehta JL. Metabolic syndrome: pathophysiology, management, and modulation by natural compounds. Ther Adv Cardiovasc Dis. 2017;11(8):215-225. doi:10.1177/1753944717711379
PubMed | Crossref | Google Scholar - Ilyas Z, Perna S, Al-thawadi S, et al. The effect of berberine on weight loss in order to prevent obesity: a systematic review. Biomed Pharmacother. 2020;127:110137. doi:10.1016/j.biopha.2020.110137
Crossref | Google Scholar - Tabeshpour J, Imenshahidi M, Hosseinzadeh H. A review of the effects of Berberis vulgaris and its major component, berberine, in metabolic syndrome. Iran J Basic Med Sci. 2017;20(5):557-568. doi:10.22038/IJBMS.2017.8682
PubMed | Crossref | Google Scholar - Shi L, Wang W, Jing C, et al. Berberine and health outcomes: an overview of systematic reviews. BMC Complement Med Ther. 2025;25:147. doi:10.1186/s12906-025-04872-4
Crossref | Google Scholar - Jael Teresa de Jesús QV, Gálvez-Ruíz JC, Márquez Ibarra AA, Leyva-Peralta MA. Perspectives on Berberine and the Regulation of Gut Microbiota: As an Anti-Inflammatory Agent. Pharmaceuticals (Basel). 2025;18(2):193. doi:10.3390/ph18020193
PubMed | Crossref | Google Scholar - Derosa G, Maffioli P, Cicero AF. Berberine on metabolic and cardiovascular risk factors: an analysis from preclinical evidences to clinical trials. Expert Opin Biol Ther. 2012;12(8):1113-1124. doi:10.1517/14712598.2012.704014
PubMed | Crossref | Google Scholar - Bellavite P, Fazio S, Affuso F. A Descriptive Review of the Action Mechanisms of Berberine, Quercetin and Silymarin on Insulin Resistance/Hyperinsulinemia and Cardiovascular Prevention. Molecules. 2023; 28(11):4491. doi:10.3390/molecules28114491
Crossref | Google Scholar - Belwal T, Bisht A, Devkota HP, et al. Phytopharmacology and Clinical Updates of Berberis Species Against Diabetes and Other Metabolic Diseases. Front Pharmacol. 2020;11:41. doi:10.3389/fphar.2020.00041
PubMed | Crossref | Google Scholar - Firouzi S, Malekahmadi M, Ghayour-Mobarhan M, Ferns G, Rahimi HR. Barberry in the treatment of obesity and metabolic syndrome: possible mechanisms of action. Diabetes Metab Syndr Obes. 2018;11:699-705. doi:10.2147/DMSO.S181572
PubMed | Crossref | Google Scholar - Cao RY, Zheng Y, Zhang Y, et al. Berberine on the Prevention and Management of Cardiometabolic Disease: Clinical Applications and Mechanisms of Action. Am J Chin Med. 2021;49(7):1645-1666. doi:10.1142/S0192415X21500762
PubMed | Crossref | Google Scholar - Liu W, Tang F, Deng Y, et al. Berberine reduces fibronectin and collagen accumulation in rat glomerular mesangial cells cultured under high glucose conditions. Mol Cell Biochem. 2009;325(1-2):99-105. doi:10.1007/s11010-008-0024-y
PubMed | Crossref | Google Scholar - Liu YF, Wang HH, Geng YH, Han L, Tu SH, Wang H. Advances of berberine against metabolic syndrome-associated kidney disease: Regarding effect and mechanism. Front Pharmacol. 2023;14:1112088. doi:10.3389/fphar.2023.1112088
Crossref | Google Scholar - Zhao JV, Yeung WF, Chan YH, et al. Effect of Berberine on Cardiovascular Disease Risk Factors: A Mechanistic Randomized Controlled Trial. Nutrients. 2021;13(8):2550. doi:10.3390/nu13082550
PubMed | Crossref | Google Scholar - Gonnelli S, Caffarelli C, Stolakis K, Cuda C, Giordano N, Nuti R. Efficacy and Tolerability of a Nutraceutical Combination (Red Yeast Rice, Policosanols, and Berberine) in Patients with Low-Moderate Risk Hypercholesterolemia: A Double-Blind, Placebo-Controlled Study. Curr Ther Res Clin Exp. 2014;77:1-6. doi:10.1016/j.curtheres.2014.07.003
PubMed | Crossref | Google Scholar - Chen YX, Gao QY, Zou TH, et al. Berberine versus placebo for the prevention of recurrence of colorectal adenoma: a multicentre, double-blinded, randomised controlled study. Lancet Gastroenterol Hepatol. 2020;5(3):267-275. doi:10.1016/S2468-1253(19)30409-1
PubMed | Crossref | Google Scholar - Li M, Liu Y, Qiu Y, et al. The effect of berberine adjunctive treatment on glycolipid metabolism in patients with schizophrenia: A randomized, double-blind, placebo-controlled clinical trial. Psychiatry Res. 2021;300:113899. doi:10.1016/j.psychres.2021.113899
Crossref | Google Scholar - Zhao MM, Lu J, Li S, et al. Berberine is an insulin secretagogue targeting the KCNH6 potassium channel. Nat Commun. 2021;12(1):5616. doi:10.1038/s41467-021-25952-2
PubMed | Crossref | Google Scholar - Du J, Zhu Y, Yang X, et al. Berberine attenuates obesity-induced insulin resistance by inhibiting miR-27a secretion. Diabet Med. 2024;41(7):e15319. doi:10.1111/dme.15319
PubMed | Crossref | Google Scholar - León-Martínez JM, Martínez-Abundis E, González-Ortiz M, Pérez-Rubio KG. Effect of Berberine Plus Bezafibrate Administration on the Lipid Profile of Patients with Mixed Dyslipidemia: A Pilot Clinical Trial. J Med Food. 2021;24(2):111-115. doi:10.1089/jmf.2020.0029
Crossref | Google Scholar - Yang YN, Wang QC, Xu W, Yu J, Zhang H, Wu C. The berberine-enriched gut commensal Blautia producta ameliorates high-fat diet (HFD)-induced hyperlipidemia and stimulates liver LDLR expression. Biomedicine and Pharmacotherapy. 2022;155. doi:10.1016/j.biopha.2022.113749
Crossref | Google Scholar - Li Q, Huang Z, Liu D, et al. Effect of Berberine on Hyperuricemia and Kidney Injury: A Network Pharmacology Analysis and Experimental Validation in a Mouse Model. Drug Des Devel Ther. 2021;15:3241-3254. doi:10.2147/DDDT.S317776
Crossref | Google Scholar - Wu F, Chen L, Du Y. Comparison of the efficacy and safety of benzbromarone and febuxostat in gout and hyperuricemia: a systematic review and meta-analysis. Clin Rheumatol. 2024;43(5):1745-1754. doi:10.1007/s10067-024-06933-4
PubMed | Crossref | Google Scholar - Tung BT, Nguyen NN, Nguyen BK, Keservani RK. Plant metabolites and vegetables for gout prevention and treatment. Apple Academic Press; 2024. doi:10.1201/9781032680125-10
Crossref | Google Scholar - Mohammadzadeh N, Mehri S, Hosseinzadeh H. Berberis vulgaris and its constituent berberine as antidotes and protective agents against natural or chemical toxicities. Iran J Basic Med Sci. 2017;20(5):538-551. doi:10.22038/IJBMS.2017.8678
PubMed | Google Scholar - Huang YH, Liu GH, Hsu TY, et al. Effective Dose of Rhizoma Coptidis Extract Granules for Type 2 Diabetes Treatment: A Hospital-Based Retrospective Cohort Study. Front Pharmacol. 2021;11:597703. doi:10.3389/fphar.2020.597703
PubMed | Crossref | Google Scholar - Belwal T, Bisht A, Devkota HP, et al. Phytopharmacology and Clinical Updates of Berberis Species Against Diabetes and Other Metabolic Diseases. Front Pharmacol. 2020;11:41. doi:10.3389/fphar.2020.00041
PubMed | Crossref | Google Scholar - Han Y, Xiang Y, Shi Y, et al. Pharmacokinetics and Pharmacological Activities of Berberine in Diabetes Mellitus Treatment. Evid Based Complement Alternat Med. 2021;2021:998709. doi:10.1155/2021/9987097
PubMed | Crossref | Google Scholar - Gonnelli S, Caffarelli C, Stolakis K, et al. Efficacy and tolerability of a nutraceutical combination (red yeast rice, policosanols, and berberine) in patients with low–moderate risk hypercholesterolemia: a double-blind, placebo-controlled study. Curr Ther Res Clin Exp. 2014;77:1-6. doi:10.1016/j.curtheres.2014.07.003
Crossref | Google Scholar - Qi H, Wang W, Zhang X, Shang B. Pharmacokinetics Study of Herb-Drug Interaction of Berberine and Glipizide in Beagle Dogs Using UPLC-MS/MS. Int J Anal Chem. 2025;2025:7941435. doi:10.1155/ianc/7941435
PubMed | Crossref | Google Scholar - Wang H, Zhu C, Ying Y, et al. Metformin and berberine, two versatile drugs in treatment of common metabolic diseases. Oncotarget. 2018;9(11):10135-10146. doi:10.18632/oncotarget.20807
PubMed | Crossref | Google Scholar - Shan YQ, Zhu YP, Pang J, et al. Tetrandrine potentiates the hypoglycemic efficacy of berberine by inhibiting P-glycoprotein function. Biol Pharm Bull. 2013;36(10):1562-1569. doi:10.1248/bpb.b13-00272
Crossref | Google Scholar - Wu X, Li Q, Xin H, Yu A, Zhong M. Effects of berberine on the blood concentration of cyclosporin A in renal transplanted recipients: clinical and pharmacokinetic study. Eur J Clin Pharmacol. 2005;61(8):567-572. doi:10.1007/s00228-005-0952-3
PubMed | Crossref | Google Scholar - Kou Y, Tong B, Wu W, Liao X, Zhao M. Berberine Improves Chemo-Sensitivity to Cisplatin by Enhancing Cell Apoptosis and Repressing PI3K/AKT/mTOR Signaling Pathway in Gastric Cancer. Front Pharmacol. 2020;11:616251. doi:10.3389/fphar.2020.616251
PubMed | Crossref | Google Scholar - Xu Y, Quan H, Wang Y, et al. Requirement for Ergosterol in Berberine Tolerance Underlies Synergism of Fluconazole and Berberine against Fluconazole-Resistant Candida albicans Isolates. Front Cell Infect Microbiol. 2017;7:491. doi:10.3389/fcimb.2017.00491
PubMed | Crossref | Google Scholar - Yu HH, Kim KJ, Cha JD, et al. Antimicrobial activity of berberine alone and in combination with ampicillin or oxacillin against methicillin-resistant Staphylococcus aureus. J Med Food. 2005;8(4):454-461. doi:10.1089/jmf.2005.8.454
Crossref | Google Scholar - Tong N, Zhang J, Chen Y, et al. Berberine sensitizes multiple human cancer cells to the anticancer effects of doxorubicin in vitro. Oncol Lett. 2012;3(6):1263-1267. doi:10.3892/ol.2012.644
Crossref | Google Scholar - Solnier J, Zhang Y, Kuo YC, et al. Characterization and Pharmacokinetic Assessment of a New Berberine Formulation with Enhanced Absorption In Vitro and in Human Volunteers. Pharmaceutics. 2023;15(11):2567. doi:10.3390/pharmaceutics15112567
PubMed | Crossref | Google Scholar - Yin J, Xing H, Ye J. Efficacy of berberine in patients with type 2 diabetes mellitus. Metabolism. 2008;57(5):712-717. doi:10.1016/j.metabol.2008.01.013
PubMed | Crossref | Google Scholar - Funk RS, Singh RK, Winefield RD, et al. Variability in Potency Among Commercial Preparations of Berberine. J Diet Suppl. 2018;15(3):343-351. doi:10.1080/19390211.2017.1347227
PubMed | Crossref | Google Scholar - Jan N, Shah H, Khan S, et al. Old drug, new tricks: polymer-based nanoscale systems for effective cytarabine delivery. Naunyn Schmiedebergs Arch Pharmacol. 2024;397(6):3565-3584. doi:10.1007/s00210-023-02865-z
PubMed | Crossref | Google Scholar - Zuo F, Wang B, Wang L, He J, Qiu X. UV-Triggered Drug Release from Mesoporous Titanium Nanoparticles Loaded with Berberine Hydrochloride: Enhanced Antibacterial Activity. Molecules. 2024;29(7):1607. doi:10.3390/molecules29071607
PubMed | Crossref | Google Scholar - Thomas A, Kamble S, Deshkar S, Kothapalli L, Chitlange S. Bioavailability of berberine: challenges and solutions. Istanbul Journal of Pharmacy. 2021;51(1):141-153.
Bioavailability of berberine: challenges and solutions - Wang S, Ren H, Zhong H, et al. Combined berberine and probiotic treatment as an effective regimen for improving postprandial hyperlipidemia in type 2 diabetes patients: a double blinded placebo controlled randomized study. Gut Microbes. 2022;14(1):2003176. doi:10.1080/19490976.2021.2003176
PubMed | Crossref | Google Scholar - Cao C, Su M. Effects of berberine on glucose-lipid metabolism, inflammatory factors and insulin resistance in patients with metabolic syndrome. Exp Ther Med. 2019;17(4):3009-3014. doi:10.3892/etm.2019.7295
PubMed | Crossref | Google Scholar - Guo J, Chen H, Zhang X, et al. The Effect of Berberine on Metabolic Profiles in Type 2 Diabetic Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Oxid Med Cell Longev. 2021;2021:2074610. doi:10.1155/2021/2074610
PubMed | Crossref | Google Scholar - Cicero AF, Ertek S. Metabolic and cardiovascular effects of berberine: from preclinical evidence to clinical trial results. Clin Lipidol. 2009;4(5):553-563. doi:10.2217/clp.09.41
Crossref | Google Scholar - Ji L, Ma J, Ma Y, et al. Berberine Ursodeoxycholate for the Treatment of Type 2 Diabetes: A Randomized Clinical Trial. JAMA Netw Open. 2025;8(3):e2462185. doi:10.1001/jamanetworkopen.2024.62185
PubMed | Crossref | Google Scholar - Ye Y, Liu X, Wu N, et al. Efficacy and Safety of Berberine Alone for Several Metabolic Disorders: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Front Pharmacol. 2021;12:653887. doi:10.3389/fphar.2021.653887
PubMed | Crossref | Google Scholar - García-Muñoz AM, Victoria-Montesinos D, Ballester P, Cerdá B, Zafrilla P. A Descriptive Review of the Antioxidant Effects and Mechanisms of Action of Berberine and Silymarin. Molecules. 2024;29(19):4576. doi:10.3390/molecules29194576
PubMed | Crossref | Google Scholar - Affuso F, Mercurio V, Fazio V, Fazio S. Cardiovascular and metabolic effects of Berberine. World J Cardiol. 2010;2(4):71-77. doi:10.4330/wjc.v2.i4.71
PubMed | Crossref | Google Scholar - Lei L, Li J, Wang B. Efficacy and safety profile of berberine treatment in improving risk factors for cardiovascular disease: a systematic review and meta-analysis of randomized double-blind trials. Cardiology Discovery. 2023;3:112-121. doi:10.1097/CD9.0000000000000087
Crossref | Google Scholar - Och A, Och M, Nowak R, Podgórska D, Podgórski R. Berberine, a Herbal Metabolite in the Metabolic Syndrome: The Risk Factors, Course, and Consequences of the Disease. Molecules. 2022;27(4):1351. doi:10.3390/molecules27041351
PubMed | Crossref | Google Scholar - Cao C, Su M. Effects of berberine on glucose-lipid metabolism, inflammatory factors and insulin resistance in patients with metabolic syndrome. Exp Ther Med. 2019;17(4):3009-3014. doi:10.3892/etm.2019.7295
PubMed | Crossref | Google Scholar - Feng X, Sureda A, Jafari S, et al. Berberine in Cardiovascular and Metabolic Diseases: From Mechanisms to Therapeutics. Theranostics. 2019;9(7):1923-1951. doi:10.7150/thno.30787
PubMed | Crossref | Google Scholar
Acknowledgments
No external assistance was received.
Funding
This literature review was self-funded. No external funding was received.
Author Information
Corresponding Author:
Armaghan Muneer
Department of Pharmacy
Islamia University of Bahawalpur, Pakistan
Email: [email protected]
Co-Authors:
Maida Noor
Department of Pharmacy
Quaid-I-Azam University, Islamabad, Pakistan
Smavia Jamshed, Aneesa Anjum
Department of Pharmacy
Quaid-I-Azam University, Islamabad, Pakistan
Amna Shahid
Department of Pharmacy
Quaid-I-Azam University, Islamabad, Pakistan
Fareeha Parveen
Department of Pharmacy
College of Pharmacy, University of the Punjab, Lahore, Pakistan
Abdul Rahman
Department of Pharmacy
Islamia University of Bahawalpur, Pakistan
Pir Asif Ali
Department of Pharmacy
Shaheed Zulfiqar Ali Bhutto Medical University, Islamabad, Pakistan
Authors Contributions
Armaghan Muneer was responsible for the origination and supervision of the review and performed a rigorous revision of the entire manuscript. Maida Noor conducted the literature search, drafted the initial version, and organized the manuscript structure. Smavia Jamshed, Amna Shahid, and Pir Asif Ali assisted with data extraction from the literature and contributed to refining the manuscript structure. Aneesa Anjumand and Fareeha Parveen reviewed and evaluated relevant studies, handled referencing, and performed proofreading of the final version.
Conflict of Interest Statement
The authors reported no conflict of interest.
Ethical Approval
Not Applicable
Guarantor
None
DOI
Cite this Article
Muneer A, Noor M, Jamshed S, et al. Berberine as a Phytochemical in Metabolic Syndrome Management: Mechanistic Insights and Clinical Evidence. medtigo J Pharmacol. 2026;3(2):e3061322. doi:10.63096/medtigo3061322 Crossref













