






 Author Affiliations
Author Affiliations
Abstract
Aim: The primary aim is to assess the knowledge and awareness of oral piercing and related complications among students at Gulf Medical University (GMU), and the secondary aim is to evaluate the knowledge and awareness of oral piercings in relation to age, program, and frequency.
Methodology: A cross-sectional questionnaire was administered to 250 GMU students who were selected randomly. The survey consisted of questions regarding people’s interest in oral piercings and assessment of their knowledge and awareness of the complications of these piercings. After the survey was completed by respondents, the data was generated to validate the percentage and frequency of each question using Statistical Package for the Social Sciences (SPSS) software. The data was then clubbed according to the title and represented as different types of graphs that can lead us to write our discussion.
Results: The oral and perioral piercings have a long history that dates back to 4000-5000 years ago and were considered a significant cultural, religious, and sexual symbol. It was practiced by many tribes to portray individual identity and financial status according to groups of tribes. However, it is considered modern and a symbol of fashion today, and it is gaining popularity among teenagers. This article reviews current knowledge and awareness among GMU students about complications occurring with piercings, such as infection, poor oral hygiene, effect on dentition and alveolar bone, phonation problems, nerve damage, etc. According to the results, many teenagers (76.8%) were interested in or had acquaintances with piercings, the major reason being fashion (78%) and aesthetic reasons (46.8%). The majority of the students had knowledge about harmful metals (78%) used for piercings, as well as difficulty in maintaining oral hygiene (78.4%), resulting in bacterial plaque accumulation (75.6%). The students were aware of the high risk of infection (74.4%) and dental problems (56.8%). However, the students have very limited knowledge/awareness about other complications mentioned in this article.
Conclusion: This research is a baseline study that determines awareness and knowledge about oral/peri-oral complications among GMU students. This research can prove to be helpful for dentists so they can assess their patients with these complications or can be used for future studies for the prevention of complications among students.
Keywords
Oral piercings, Awareness, GMU students, Infection, Dentists.
Introduction
The art of piercing has been practiced for ages. This is evident through the piercings found on preserved bodies of people from 4000-5000 years ago. As it is considered modern and a symbol of fashion today. Many years ago, these piercings were a significant cultural, religious, and sexual symbol. This was practiced by many tribes such as African, Asia, and South America, Mayans, Aztecs, Tingit, and Halda. According to anthropologists, piercings in history were also used to portray an individual’s identity, such as the financial status, the type of group the individual belongs to, and financial and marital status.[1-5] The earliest piercing discovered in History dates back to 1500BC, in the figure of a dog in Egypt that was considered a sign of royalty.[5] For antiquated Mayans, piercing was a symbol of the most profound sense of being, strength, and virility. Eskimos practiced “labret” piercing that was embedded into the lower lip as an image of maturation and an entry to adulthood for boys and refinement in ladies. The piercings of lips, cheeks, or tongues were a conventional practice in Hindu, Chinese, and American Indian societies. In southern India, a tongue piercing was considered a vow of silence.
Still today, in some Third World territories, for reasons of strict, sexual, ancestral, or conjugal importance, oral piercings using ivory, wood, earthenware, or metal in the mouth are customs that keep on being polished. For instance, the Surma clan of Ethiopia wears huge plates on their lower lips. The wedded men and single men of the Suya clan of Brazil enhance the lower lip with painted wood circles. Different clans have different traditions, as some tribes wear plugs on the upper lip while others wear rings on the lower lip. Formal or ritual piercings can be brief and may last just hours. Body piercings are also mentioned in the bible, and tribes believe that these piercings are a way to please God.[5]
Ethiopian people have likewise been discovered to utilize different facial piercings. They accept that the lip plate in the ladies helps them acquire economic well-being and order a higher marriage cost. In Africa, numerous ancestral ladies wear lip plates called “Pelele” on their upper lip for sexual reasons. Puncturing the lips, particularly with a ring, is a custom of just two clans, the Dogon and the Nubas of Africa. The Aztecs and the Mayans pierced their lips with labrets, while the Makololo clans wore lip plates.[6] This is an old practice in certain spots of India, like West Bengal, Karnataka, and so on, where it is directed each year as a custom. On occasion, the iron bar is punctured through the tongue/cheek and eliminated once the devotee makes a round of the town gathering contributions, which generally requires about 60 minutes.[6]
Materials of piercing: Materials used for piercing should be particularly hypoallergic and non-toxic, for instance, 14k or 18k gold, stainless steel (25%), surgical steel, titanium (65%), niobium (5%), acrylic (6,3%) Tygon, silver, stone, bone, wood and ivory. Some metals could cause anaphylactic reactions; nickel is one of the metals that could lead to contact allergies. Prevalently reported anaphylactic reaction is contact dermatitis lead by nickel, nickel-cobalt, or chromium. In youth, sensitization to nickel could be heightened due to nickel-containing orthodontic appliances that cause obnoxious allergic reactions.
The European Union announced the norm in mid-1990 regarding the maximum of nickel to be used in products that contact human tissue directly should be limited to the threshold of 0.05g. This suggests that the amount of nickel used in the oral/perioral piercings jewelry should be no more than 0.05 g. The suggested gold used for the cause stands to be at least 14k-18k.[7]
Prevalently, the materials used to make oral/perioral piercings are stainless steel, silver, gold, titanium, niobium, and metal alloys. With the increase in popularity and the evolving generation lately, synthetic materials such as Teflon, plastic, and nylon are being used. Generally, instead of metal piercings, a short plastic barrel is preferred. In the case of ingestion of piercing jewelry, Inert, biocompatible, and non-hazardous materials have a highlighted role in controlling the possibilities of complications and risk factors.[8]
Sites of piercing: There are several different sites for oral and perioral piercings, such as buccal mucosa, labial frenulum, lingual frenulum, tongue, gingiva, palate, uvula, along with perioral sites such as nose, eyebrows, and cheeks. The additional modification of the oral cavity leads to the division of the tongue into two lateral halves, which is also called the “forked” tongue.[9] The order of oral and perioral piercing is as follows: the tongue is the commonest, followed by the lips (including the philtrum and the labiomental groove), then comes the cheeks, maxillary labial or lingual frenum or the combination of the above is also used. Among all the ovulas, the least pierced is because it can lead to the aspiration of the jewelry both during placement and wearing. On the other hand, it is associated with complications like throat irritation, gagging, and dysphagia. The tongue piercings are done mainly on two surfaces, the dorsolateral and the dorsoventral. The latter is the most common and extremely safe, as it prevents the major blood vessels and nerves from penetrating. The piercing of the tongue is mainly done on the anterior compared to the posterior surface in the lingual frenulum, and the jewelry is worn such that the sphere is present on both the ventral and dorsal surfaces of the tongue. The former one is not safe because of the tongue’s vascularity and professional piercers do not perform this type of piercing. In this type of piercing, both spheres are present on the dorsal surface of the tongue, almost halfway anteroposteriorly and close to the lateral borders. The curvature of the barbell between the spheres is towards the ventral surface, and it resurfaces dorsally.[10]
Methodology
Research design: The research will be a cross-sectional questionnaire-based study to assess the knowledge and awareness of oral piercing and related complications among students at GMU, Ajman. Participants are expected to answer a questionnaire.
Study population: The study population will include students at GMU who have given consent for the study.
Sample size calculation: sample size will be 250 students
Sample size estimation
n0 = (Z2 · p · q) / e2
E is the desired level of precision (i.e., the margin of error),
P is the (estimated) proportion of the population which has the attribute in question, q is 1-p
We want 95% confidence, and at least 5 percent- plus or minus- precision. A 95% confidence level gives us Z values of 1.96, per the normal tables, so we get:
((1.96)2 (0.5) (0.5)/(0.05)2= 385
Since the population we’re studying is small, i.e., only GMU students, we can modify the sample size we calculated in the above formula by using this equation:
n =n0 / (1 + (n0 – 1 / N))
Where n0 is Cochran’s sample size recommendation, N is the population size, and n is the new, adjusted sample size. For approximately 700 students in the target population, we would calculate.
Study instrument and validation procedure: The data gathered for this study will be obtained by means of a questionnaire. The questionnaire designed will be validated. Once the questionnaire is approved by the experts, the validation process will be completed using a representative sample, i.e by conducting a pilot study to confirm reliability and validity.
Ethical issues:
- A standard written consent form will be
- The quality and integrity of the research will be
- We will respect the confidentiality and anonymity of the research
- The participants are voluntarily participating in the
- The research will be independent and
For conducting this research, a questionnaire was administered to 250 students of GMU who were selected randomly. The survey consisted of questions regarding people’s interest in oral piercings and assessment of their knowledge and awareness of the complications of these piercings. After the survey was completed by respondents, the data was generated to validate the percentage and frequency for each question using SPSS software. The data was then clubbed according to the title and represented as different types of graphs that can lead us to write our discussion.
Feasibility of the proposed research: The research is feasible because:
The study population is achievable
Data collection is not significantly time-consuming
Participation is free of cost.
Details of data storage: Data will be stored in the College of Dentistry at GMU.
Inclusion criteria: For all GMU students of all courses and years.
Exclusion criteria: Faculty and no-GMU students.
Data analysis: Data will be entered into Microsoft excel. Statistical analysis will be done by using SPSS software. It will be presented as percentages, tables, and graphs. The Chi square test will be used to compare among the groups.
Results
Demographic description of the sample: The sample study includes 250 clinical and pre-clinical students at GMU, Ajman. Most of our study sample age is greater than or equal to 21 years (81.2%), with females as the majority (74.8%). This is because there are more females’ students in the university. Most of our sample comprises of Middle East (50.4%) and Asian (39.2%) ethnicity. Majority of our subjects are from Bachelor of Dental Surgery (BDS) program (54.0%) and 3rd year of study (32.4%) followed by first year (28.4%). This survey consists of students from years 1,2,3,4, and 5th.
| Social demographic characteristics | Number | Percentage | Total | |
| Age | <= 21 years | 203 | 81.2 | 250 |
| >21 years | 47 | 18.8 | ||
| Gender | Males | 63 | 25.2 | 250 |
| Females | 187 | 74.8 | ||
| Ethnicity | Middle East | 126 | 50.4 | 250 |
| Asia | 98 | 39.2 | ||
| Africa | 20 | 8.0 | ||
| America | 3 | 1.2 | ||
| Europe | 3 | 1.2 | ||
| Year of study | 1 | 71 | 28.4 | 250 |
| 2 | 63 | 25.2 | ||
| 3 | 81 | 32.4 | ||
| 4 | 3 | 1.2 | ||
| 5 | 32 | 12.8 | ||
| Program | BDS | 135 | 54.0 | 250 |
| Bachelor of Physiotherapy (BPT) | 25 | 10.0 | ||
| Bachelor of Biomedical Science (BBMS) | 44 | 17.6 | ||
| Bachelor of Medicine, Bachelor of Surgery (MBBS) | 12 | 4.8 | ||
| Bachelor of Health Science (BHS) | 2 | 0.8 | ||
| PHARM-D | 24 | 9.6 | ||
| Nursing | 7 | 2.8 | ||
| Health care management | 1 | 0.4 | ||
Table 1: Demographic description of the sample
The number of people that are interested in piercings compared to people who have piercings: The following bar graph shows that (18.8%) (n = 47/250 x 100) of the subjects are interested in having an oral/peri-oral piercing whereas only (4.4%) (n = 11/250 x 100) are having oral/peri- oral piercings. (27.6%) (n = 69/250 x 100) of the subjects have acquaintances who bare oral/peri-oral piercings.
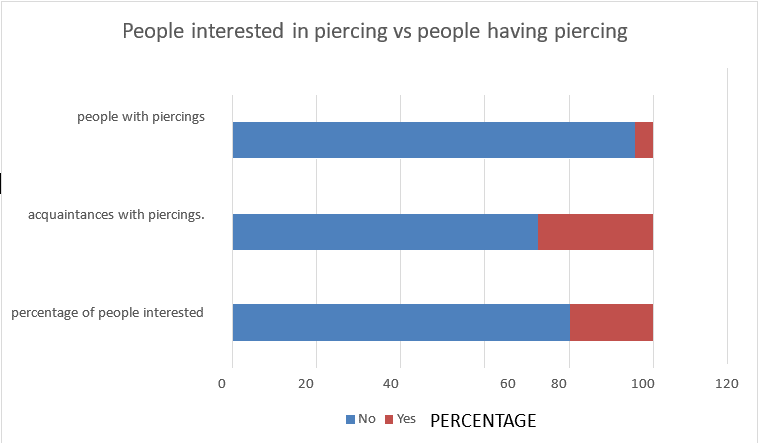
Figure 1: People interested in piercing vs people having piercing
Duration of oral piercings: This pie chart shows that the majority of the people having peri oral piercings have it for years (50%) (n = 13/250 x 100) compared to months (27%) (n = 7/250 x 100) and weeks (23%) (n = 6/250 x 100) , suggesting they could be aware of long term complications.
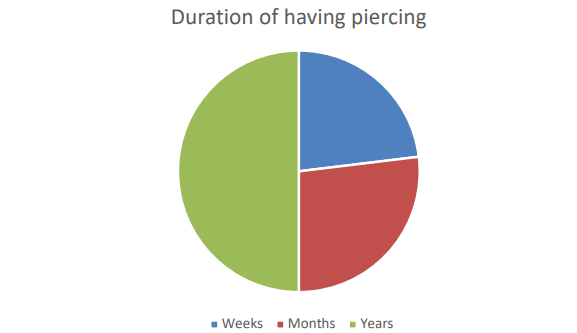
Figure 2: Duration of having piercing
Age and oral piercing: The line graph below clearly shows that as the age increases the frequency of having an oral piercing decrease. According to the subjects of the survey, the majority think that piercings are most found in teenagers (76.8%) (n = 197/250 x 100) compared to adulthood (26.4%) (n = 66/250 x 100), mid age (9.6%) (n = 24/250 x 100) and old age (2.4%) (n = 6/250 x 100).
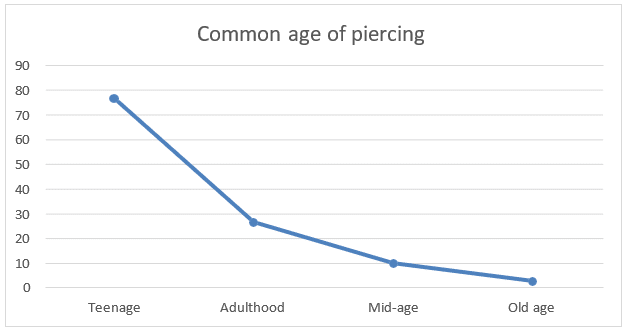
Figure 3: Age and oral piercing
Reason for oral piercings: In the following bar it is shown that, people perform piercings because of multiple reasons the highest number being fashion (78%) (n= 195/250 x 100) followed by aesthetic reasons (46.8%) (n= 133/250 x 100) and tribe (21.2%) (n= 53/250 x 10) and the lowest is religious beliefs (18.4%) (n= 46/250 x 100).
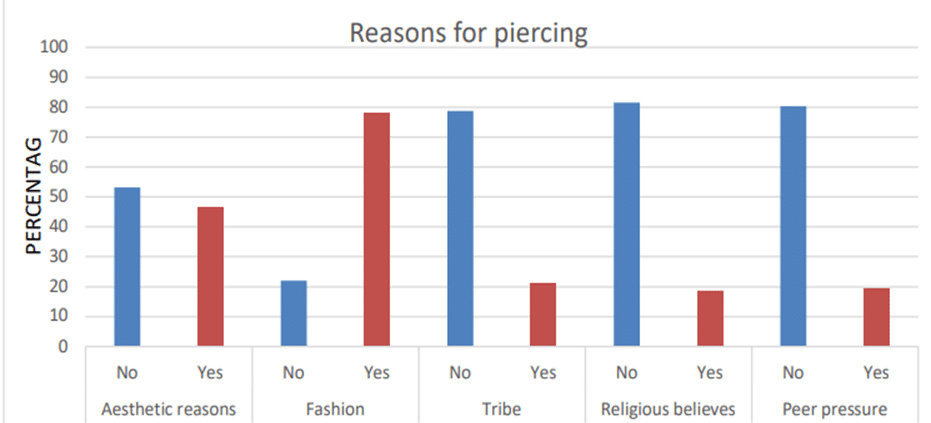
Figure 4: Reasons for piercing
Knowledge about complications of oral/peri oral piercings: One of the goals of the survey conducted was to assess the knowledge of the students regarding the possible complications that can occur before, while or after oral piercings. Most of the students have the knowledge about which metals can be harmful for the oral cavity (78%) (n = 195/250 x 100) and how difficult it is to maintain oral hygiene with presence of piercings therefore, the students also have knowledge about increase in bacterial plaque (75.6%) (n = 183/250 x 100) because of the poor oral hygiene (78.4%) (n= 196/250 x 100) many people are knowledgeable about the scarring caused by systemic diseases or smoking habits (74.8%) (n= 187/250 x 100) whilst having a piercing. However, very few people have the knowledge of anaphylactic reactions (41.2%) (n= 103/250 x 100) and most common locations (18.8%) (n = 47/250 x 100) of piercings.
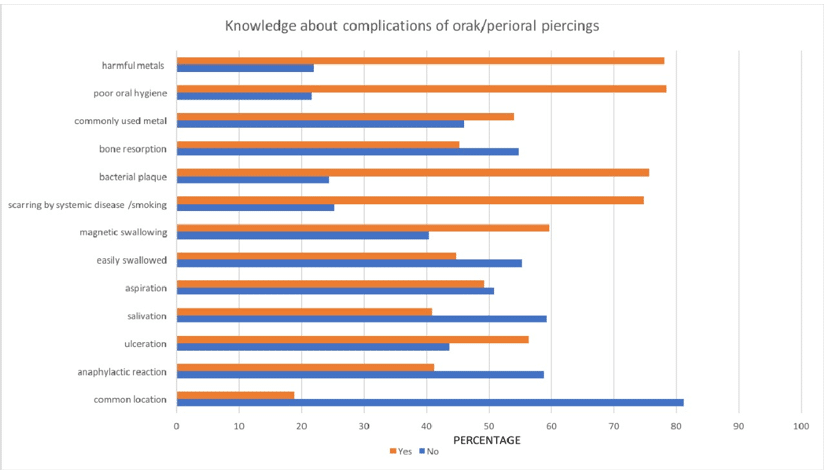
Figure 5: Knowledge about complications of oral/peri oral piercings
Awareness about complications of oral/peri oral piercings: In the following bar graph, it is shown that the subjects are aware that piercings can cause high risk of infection (74.4%) (n = 186/250 x 100) it is also considered the most commonly occurring complication, the second most positive response was awareness about dental problems occurring with oral piercing, the number of responses that were definite are as follows:(56.8%) (n = 142/250 x 100) and (26.4%) (n= 66/250 x 100) respondents thought it may be possible. Whereas awareness about hematoma (31.2%) (n = 78/250 x 100) responses being sure and (33.2%) (n = 83/250 x 100) maybe and local tumor (28.8%) (n = 72/250 x 100) occurrence due to piercings is very low compared to others.
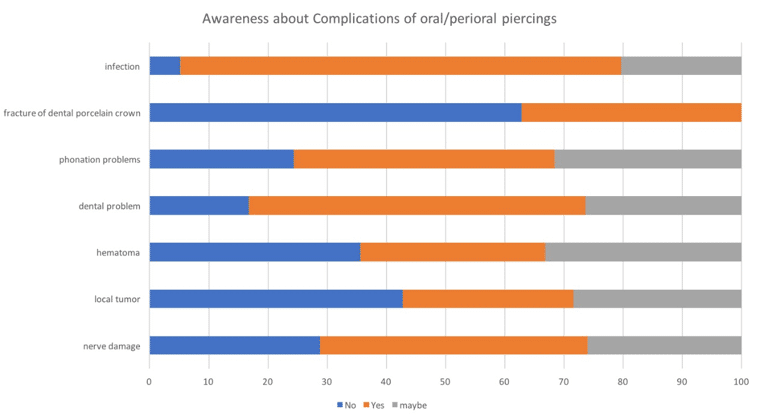
Figure 6: Awareness about complications of oral/peri oral piercings
Discussion
Body piercing refers to the piercing of a body part to enable jewelry to be worn. Oral piercing has become increasingly common in recent years, particularly among young adults. The biggest motivation for young people to have their bodies pierced is the need to have a chic kind of body adornment. Body art, or the deliberate altering of natural human anatomy to create a required look, is a common procedure that has contributed to an increase in the number of people who have oral piercings. The first article on oral piercing appeared in the dental literature in 1992, under the title ‘Tongue piercing: a new fad in body art.[11] Oral piercings, on the other hand, have been more common than a fad. The tongue and lips are the most common locations for oral piercings, but additional anatomical locations, such as the cheeks and frenulum, are becoming more popular.[12] Body piercing should be treated as a medical technique for all intents and purposes and should be done only by trained personnel who can maintain strict levels of integrity in sanitary facilities.
Young adults are often misinformed about the dangers they face as a result of intraoral piercing, and even healthcare providers are frequently unaware of the dangers and complications that may occur as a result of this surgical technique.[13,14] It is important to evaluate the knowledge and awareness of oral piercings, which was carried out among our subjects, the majority being females of Asian and Middle Eastern ethnicity BDS programmed as per Table 1. Very few subjects were piercing bearers in comparison to the people who were interested and knew piercing-bearing acquaintances. Many of our subjects are widely unaware of or unsure of the necessary complications occurring with oral piercings, the reason being they are not bearing a piercing.
According to the survey we conducted, the subject’s idea of common age to bear piercing ranges mostly between teenage and adulthood, as seen in Figure 3. As age increases, the interest to bear piercings decreases. Also, regarding the reasons for getting an oral piercing, the most common reason, according to the results, seems to be fashion and aesthetics. According to the research conducted by Francesco Covello, Camilla Salerno, Valentina Giovannini, Denise Corridore, Livia Ottolenghi, and Iole Vozza in 2020 shows that 117 (30.2%) said they did it for aesthetics, 170 said it was for artistic reasons (43.9%), 51 said it was for sexual reasons (13.2%), 45 said it was for fashion (11.6%), and four said it was because of peer pressure (1 percent ). Furthermore, 53.2 percent said they were told about the negative effects of piercings on their overall well-being, while 46.8% said they were not. These results correlate with this research as the predominant reasons are fashion and aesthetics.[15]
The primary objective of the study was to assess the Knowledge of the participants regarding the complications. The results show that most of the participants have the Knowledge about the harmful metals that are used to make ornaments which are in contact with oral cavities. They also had Knowledge about the most common and frequent complications, such as the inability to maintain good oral hygiene that causes increased bacterial plaque and scarring caused by systemic diseases and smoking whilst bearing a piercing, commonly used metals, and the ease of swallowing magnetic piercings. However, very few people have knowledge about aspiration, salivation, ulceration, common location, anaphylactic reaction, and bone resorption.
When surveyed by Francesco Covello, Camilla Salerno, Valentina Giovannini, Denise Corridore, Livia Ottolenghi, and Iole Vozza if they were knowledgeable of the potential for gingival risks because of piercings, 273 subjects (70.6 percent) said they were not, while 114 subjects (29.4%) said they were. In the dental sector, 234 (60.4%) of the participants reported that they were not educated about the dangers of piercings on the teeth. However, 153 (39.6%) of the participants appeared to have been aware of the risks. This study correlated with the respective research results as many subjects are not knowledgeable enough about all the possible complications stated above, as seen in Figure 5. These complications can occur while or after the piercing is done; for instance, excess salivation is a very frequent side effect that happens when you put the jewelry in your mouth, and it usually disappears over time. However, in some circumstances, it can cause drooling because the oral cavity needs time to adjust to a foreign material (piercing), which increases salivary gland activity. Excess saliva is useful for caries prevention, but drooling can be serious at times, interfering with everyday lives and causing social issues.[16] An allergic response happens when the immune system of the host rejects a non-toxic foreign material. Contact dermatitis caused by copper, chromium, or nickel-cobalt is the most common hypersensitive reaction to piercing.
The European Union has issued a directive limiting the amount of nickel in all products that come into close contact with human tissue. Nickel used in oral/perioral adornments is subject to a 0.05 percent limit. It also implies that nickel used in oral/perioral adornments is nickel-free. It also implies that the gold used for this use should be at least 14k-18k. A few people have knowledge about Aspiration and inhalation of piercings, the reason being magnetic piercings are not quite adhesive; this is a normal occurrence. Uvula piercings have a greater risk of aspiration because they are quickly removed. Nasal rings may be inhaled or aspirated, resulting in serious complications such as chronic pneumonia and infection. Flexible fiberoptic bronchoscopy is commonly used to treat aspirated piercing under general anesthesia.[17]
The jewelry’s continuous damage to the local bone may result in horizontal bone degradation at the same location. The mandibular gingiva may be traumatized, resulting in bone dehiscence at the wound site. Gingival recession, which is generally determined by Miller’s classification, is the most common aftereffect of a piercing. The mandibular incisors’ labial and lingual surfaces are affected by recession. The mandibular incisors’ labial and lingual surfaces are affected by recession. According to a study, the lingual recession will occur two years after the piercing. It also indicates that age is a factor in predicting lingual recession and the number of places where it occurs. A recession is a narrow wound that seems like a cleft. The depth could be estimated up to 2-3 mm or more at facial and lingual sites. They sometimes stretch through or past the muco-gingival junction. Even if the recession seems to be brief, extreme attachment loss can occur. The use of the word ‘labret’ has been used to observe Miller’s classes I and II. Lower lip piercings, on the other hand, affect the buccal surface with no impact on the pocket depth.
Tongue piercings may cause recession of the gingiva on the lingual surface of mandibular incisors, resulting in an increase in pocket dept. The dentist may perform practical or aesthetic repairs for certain problems.[18] The predominant result of awareness amongst the subjects was about infection occurring with oral piercings because of The inappropriate method of piercing by untrained practitioners, there is a risk of cross-infection from one individual to another, resulting in the transmission of blood-borne diseases such as (Herpes simplex virus, hepatitis B, C, D, and G, human immunodeficiency virus, Epstein-Barr virus), syphilis, tetanus, and tuberculosis or infection can be caused after the piercing is done because of lack of good oral hygiene, followed by dental problems due to long-standing oral piercings teeth undergo traumatic injury like; chipping, pulpal damage, fracture of tooth or restorative structure.
Very few people were aware of serious complications such as local tumors, nerve damage, hematoma, and phonation problems. Piercers should use caution when doing piercings because the sensory and motor nerve components are more susceptible to damage. The lingual frenum may be injured during tongue piercing, resulting in deglutition, mastication, and speech problems. The regular working atmosphere is hampered by the inclusion of jewelry in the oral cavity, especially the tongue, which alters the pronunciation of sounds such as ‘s’, sh’, th’, ph’, t’, and ‘v′. Tongue piercings can lead to painful fibroma in the long run. Fibroma is a benign tumor that appears in a localized region of injury, which can be caused by piercing, has a smooth consistency, and is the same color as the mucosa. Many of the piercers, in particular, are unable to inform consumers of the risks that piercings can bring to teeth and gums, such as fractures and gingival regression or frenula thickening, as well as how to disinfect the piercings, which is critical in preventing gingivitis and periodontitis.[19-21]
Bone et al. study on the level of awareness of possible oral piercing risks ranges from pierce to pierce. According to one survey of 110 pieces, 70.9 percent were unaware that oral piercings could influence their overall well-being, and 26.4 percent were unaware of possible dental problems. 24 According to similar research, about 46–57.8% of piercings are unaware of the risks involved with oral piercings.[22] As a result, the dentist and dental hygienist must cope with reminding their patients who have piercings of the details. Maspero C. et al. analyzed the importance of the dental staff in 2014. Oral piercings are the cause of a variety of complications, including dental abrasions, dental fractures, gingival recessions, and loss of attachment of periodontal tissues, as well as temporomandibular joint problems, as reported by Mejersjö in 2016.
To avoid the above problems identified by Silk H et al., Junco P et al., and McGeary SP et al., it is important to develop education programs in schools between dentistry students and dentists themselves.[23]
To avoid a lack of knowledge and awareness, it is important to educate students about risks and prevention of complications, such as eating a cold liquid diet and soft food for 24 hours after piercing, not oral rinsing for 24 hours, and then continuing to use chlorhexidine for next 10 days, avoid smoking, alcohol and caffeine for first few days as it can lead to pain, bleeding and swelling, avoid chewing nails, tobacco and gums to avoid further microlesions, avoid excessive talking as the mouth suffers from trauma during eating and speaking and regularly check oral and perioral piercings for any infections.[24]
Conclusion
In conclusion, oral piercings can lead to many serious complications during or after piercings, and they can be local or systemic. Teenagers these days are easily attracted to these perioral piercings for multiple reasons, such as the latest trends, fashion, and aesthetics. As seen in most of the subjects, they were interested in or had acquaintances with piercings; thus, they had knowledge about poor oral hygiene, which metals are harmful to the oral cavity, bacterial plaque accumulation, and scarring due to systemic disease or smoking. Although many of them have knowledge about the above-mentioned complications, many don’t seem to be knowledgeable enough about anaphylactic reactions, excess salivation, bone resorption, and the common location of oral piercing. On the other hand, awareness of the subjects about infection and dental problems is good. However, hematoma, local tumor, and phonation problems don’t exhibit awareness. Future studies can be performed on knowledge and awareness of preventive methods among students as well as dentists to help guide their patients.
References
- Escudero-Castaño N, Perea-García MA, Campo-Trapero J, Cano-Sánchez J, Bascones-Martínez A. Oral and perioral piercing complications. Open Dent J. 2008;2:133-136. doi.10.2174/1874210600802010133
PubMed | Crossref | Google Scholar - Stom BJ. Complications of oral piercing. Balkan J Stomatol. 2013;17:117-121. Complications-of-oral-piercing.pdf
- Whittle JG, Lamden KH. Lip and tongue piercing: Experiences and views of general dental practitioners in South Lancashire. Prim Dent Care. 2004;11(3):92-96. doi.10.1308/135576104323117455 PubMed | Crossref | Google Scholar
- Levin L, Zadik Y, Becker T. Oral and dental complications of intra-oral piercing. Dent Traumatol. 2005;21(6):341-343. doi.10.1111/j.1600-9657.2005.00314.x PubMed | Crossref | Google Scholar
- Mandabach MG, McCann DA, Thompson GE. Body art: Another concern for the anesthesiologist. Anesthesiology. 2007;88(1):279-280. doi.10.1097/00000542-199801000-00058 PubMed | Crossref | Google Scholar
- Khalia N, Metha DS, Vemanaradhya G. Oral piercing: Style statement or a state of disharmony? Int J Oral Health Sci. 2014;3(2):84-91. doi.10.4103/2231-6027.149588 Crossref | Google Scholar
- Reiss M, Reiss G. Piercing: Medical problems from an otorhinolaryngological point of view. Med Monatsschr Pharm. 2007;30:441-447. Piercing–medical problems from otorhinolaryngological point of view – PubMed
- Peticolas T, Tilliss TS, Cross-Poline GN. Oral and perioral piercing: A unique form of self-expression. J Contemp Dent Pract. 2008;1:30-46. Oral and perioral piercing: a unique form of self-expression – PubMed
- Berenguer G, Forrest A, Horning GM, Towle HJ, Karpinia K. Localized periodontitis as a long-term effect of oral piercing: A case report. Compend Contin Educ Dent. 2006;27(1):24-27. Localized periodontitis as a long-term effect of oral piercing: a case report – PubMed
- Brennan M, O’Connell B, O’Sullivan M. Multiple dental fractures following tongue barbell placement: A case report. Dent Traumatol. 2006;22(1):41-43. doi.10.1111/j.1600-9657.2006.00337.x PubMed | Crossref | Google Scholar
- Chen M, Scully C. Tongue piercing: A new fad in body art. Br Dent J. 1992;172:87. doi.10.1038/sj.bdj.4807704
PubMed | Crossref | Google Scholar - Covello F, Salerno C, Giovannini V, Corridore D, Ottolenghi L, Vozza I. Piercing and oral health: A study on the knowledge of risks and complications. Int J Environ Res Public Health. 2020;17(2):613. doi.10.3390/ijerph17020613
PubMed | Crossref | Google Scholar - Bone A, Ncube F, Nichols T, Noah ND. Body piercing in England: A survey of piercing at sites other than the earlobe. BMJ. 2008;336(7658):1426-1428. doi.10.1136/bmj.39580.497176.25 PubMed | Crossref | Google Scholar
- Inchingolo F, Tatullo M, Abenavoli F, et al. Oral piercing and oral diseases: A short-time retrospective study. Int J Med Sci. 2011;8(8):649-652. doi.10.7150/ijms.8.649 PubMed | Crossref | Google Scholar
- King EM, Brewer E, Brown P. Oral piercings and their complications – how confident are we as a profession? Br Dent J. 2018;224(11):887-895. doi: 10.1038/sj.bdj.2018.435. PubMed | Crossref | Google Scholar
- Randall JA, Sheffield D. Just a personal thing? A qualitative account of health behaviors and values associated with body piercing. Perspect Public Health. 2013;133(2):110-115. doi.10.1177/1757913912464835
PubMed | Crossref | Google Scholar - Ziebolz D, Hornecker E, Mausberg RF. Microbiological findings at tongue piercing sites: implications to oral health. Int J Dent Hyg. 2009;7(4):256-262. doi.10.1111/j.1601-5037.2009.00381.x PubMed | Crossref | Google Scholar
- Plessas A, Pepelassi E. Dental and periodontal complications of lip and tongue piercing: Prevalence and influencing factors. Aust Dent J. 2012;57(1):71-78. doi.10.1111/j.1834-7819.2011.01647.x PubMed | Crossref | Google Scholar
- Laumann AE, Derick AJ. Tattoos and body piercings in the United States: A national data set. J Am Acad Dermatol. 2006;55(3):413-421. doi.10.1016/j.jaad.2006.03.026 PubMed | Crossref | Google Scholar
- Vozza I, Fusco F, Corridore D, Ottolenghi L. Awareness of complications and maintenance of oral piercing in a group of adolescents and young Italian adults with intraoral piercing. Med Oral Patol Oral Cir Bucal. 2015;20(4):e413-418. doi.10.4317/medoral.20487 PubMed | Crossref | Google Scholar
- Jeger F, Lussi A, Zimmerli B. Oral jewelry: a review. Schweiz Monatsschr Zahnmed. 2009;119(6):615-631. Oral jewelry: a review – PubMed
- Ziebolz D, Stuehmer C, van Nüss K, Hornecker E, Mausberg RF. Complications of tongue piercing: a review of the literature and three case reports. J Contemp Dent Pract. 2009;10(6):E065-71. doi:10.5005/jcdp-10-6-65
PubMed | Crossref | Google Scholar - Hickey BM, Schoch EA, Bigeard L, Musset AM. Complications following oral piercing: a study among 201 young adults in Strasbourg, France. Community Dent Health. 2010;27(1):35-40. Complications following oral piercing. A study among 201 young adults in Strasbourg, France – PubMed
- Oberholzer TG, George R. Awareness of complications of oral piercing in a group of adolescents and young South African adults. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;110(6):744-747. doi.10.1016/j.tripleo.2010.07.012 PubMed | Crossref | Google Scholar
Acknowledgments
Firstly, we are thankful to our supervisor, Dr. Sura Ali Ahmed Fuoad, for organizing and directing this course at ease for the entire team. Also, for her immense supervision, expert advice, and valuable feedback that helped bring the best out of us. Without her support, guidance, and patience, this research wouldn’t have been conducted smoothly. Secondly, we would also like to thank Dr. Anusha Sreejith for getting us through the statistical work on this research project.
Lastly, we would like to extend our gratitude to the students at GMU for taking their valuable time to fill out our questionnaire and giving us their input, which helped us reach our desired sample size and result.
Funding
The work had no special funding.
Author Information
Corresponding Author:
Pritika Valechha
Department of Oral Medicine
Gulf Medical University, UAE
Email: [email protected]
Co-Authors:
Sathvica Chaparala, SimranJeet Kaur, Sura Ali Ahmed Fuoad Al-Bayati
Department of Oral Medicine
Gulf Medical University, UAE
Authors Contributions
Pritika Valechha was responsible for conceptualization, data collection, methodology, manuscript drafting, literature review, and writing. Sathvica Chaparala contributed to conceptualization, data collection, data analysis, manuscript drafting, literature review, and writing. SimranJeet Kaur handled conceptualization, data collection, data organization, manuscript drafting, literature review, and writing. Sura Ali Ahmed Fuoad Al-Bayati oversaw the supervision, proofreading, revision, and final approval of the manuscript.
Ethical Approval
This research was conducted within the university as a student project; obtaining IRB approval was not mandatory. We confirm that there are no conflicts of interest. All participants provided written informed consent before data collection, agreeing to participate in the study.
Conflict of Interest Statement
The authors declare that there are no conflicts of interest.
DOI
Cite this Article
Pritika V, Sathvica C, SimranJeet K, Sura Ali Ahmed FA-B. Awareness and Knowledge Among GMU Students About Complications of Oral or Peri-Oral Piercings. medtigo J Med. 2025;3(1):e30623131. doi:10.63096/medtigo30623131 Crossref













