






 Author Affiliations
Author Affiliations
Abstract
Background: Although body mass index (BMI) is a modifiable risk factor associated with respiratory and cardiovascular outcomes, little is known about its subclinical effects on Pacific medical students.
Aim: To evaluate the association between BMI and cardiopulmonary metrics in young individuals in a tropical academic setting, particularly systolic blood pressure (SBP), forced expiratory volume in one second (FEV₁), and peak expiratory flow rate (PEFR).
Methodology: A cross-sectional study was conducted among 59 medical students aged 18–25 years in a tropical academic setting. Participants were recruited by convenience sampling, with exclusion of individuals with known cardiovascular or chronic respiratory disease, recent respiratory infection, or use of medications affecting cardiopulmonary function. Height and weight were measured using standardized equipment to calculate BMI, which was classified according to World Health Organization criteria. Systolic blood pressure (SBP) was measured using a validated automated oscillometric device after a minimum of five minutes of seated rest, with two readings averaged for analysis. Pulmonary function was assessed using handheld spirometry, measuring FEV₁ and PEFR in accordance with standard guidelines; the highest values from at least three acceptable maneuvers were recorded. Associations between BMI and cardiopulmonary parameters were analysed using Pearson’s correlation coefficients, while differences in SBP across BMI categories were assessed using one-way analysis of variance (ANOVA), with statistical significance set at p < 0.05.
Result: Fifty-nine medical students aged 18–25 years were included in the analysis. Systolic blood pressure differed significantly across BMI categories, with a progressive increase observed as BMI increased (one-way ANOVA: F(3,55) = 6.91, p < 0.001). Pearson correlation analysis demonstrated a significant positive association between BMI and systolic blood pressure. In contrast, pulmonary function parameters showed inverse relationships with BMI. FEV₁ was negatively correlated with BMI (r = –0.28, p = 0.033), indicating lower expiratory volumes with increasing BMI. Similarly, PEFR demonstrated a stronger negative correlation with BMI (r = –0.35, p = 0.010). These findings suggest that higher BMI is associated with elevated systolic blood pressure and reduced pulmonary function even in young, apparently healthy individuals.
Conclusion: Students with elevated BMI have lower pulmonary function and greater systolic blood pressure. Results support the use of early cardiopulmonary screening in student health initiatives.
Keywords
Body mass index, Forced expiratory volume in one second, Peak expiratory flow rate, Pulmonary function, Tropical health, Obesity, Cardiovascular risk.
Introduction
It is commonly acknowledged that elevated BMI in young adult populations can cause early abnormalities in pulmonary function and blood pressure, frequently before overt non-communicable diseases (NCDs). In tropical environments such as Fiji, academic pressure, sedentary lifestyles, and environmental exposures may exacerbate physiological stressors among tertiary medical students. Finding modifiable risk factors early in childhood is crucial, as evidenced by the rising worldwide burden of NCDs. The BMI, a straightforward yet effective anthropometric index, has been widely used to predict the health risks associated with being overweight. Numerous adverse health effects, particularly those affecting the cardiovascular and pulmonary systems, are associated with elevated BMI.
Subtle alterations in physiological measures, such as blood pressure and lung function, may indicate early disease etiology in young adults. However, these signs are frequently overlooked, particularly in academic settings where health examinations are not commonplace. Despite their health literacy, medical students remain susceptible to these risks. This population may be more susceptible to early onset cardiovascular and pulmonary problems due to sedentary lifestyles, inconsistent sleep patterns, nutritional imbalances, and academic stress.
Additional environmental stresses may affect cardiac health in tropical environments such as Fiji. Overweight individuals may experience increased physiological strain due to high ambient temperatures and humidity, poor indoor air quality, and shifting eating patterns. Particularly in Pacific Island countries, these contextual elements remain insufficiently addressed in contemporary research. Furthermore, given climate change, the relationship between obesity, cardiovascular risk, and pulmonary impairment is becoming more and more significant. Ensuring the physical well-being of students is not only a moral imperative but also a strategic aim for medical schools that train future healthcare providers, as it helps strengthen the resilience of health systems.
Therefore, this study examines the relationships between BMI and important cardiopulmonary metrics among medical students in a tropical academic setting, including systolic blood pressure (SBP), forced expiratory volume in one second (FEV₁), and peak expiratory flow rate (PEFR). It aims to contribute to the body of knowledge on early detection and health promotion strategies for at-risk children in climate-vulnerable areas.
Despite evidence indicating that BMI influences SBP, FEV₁, and PEFR, cardiopulmonary screening is rarely prioritized in student health efforts. Nutritional shifts, indoor air quality, and tropical heat further complicate health dynamics in this population.
This study aims to quantify relationships between BMI and cardiopulmonary variables in a cohort of medical students, and to consider their implications within a climate-sensitive health landscape. By identifying early risk markers, the findings may inform prevention strategies, pedagogical approaches, and environmental health awareness in academic institutions.
Methodology
Study design and setting: A cross-sectional observational study was conducted among undergraduate medical students in a tropical academic setting. The study was carried out within the university campus during scheduled practical or data collection sessions under controlled indoor conditions to minimize environmental variability.
Participants: Participants were undergraduate medical students aged 18–25 years enrolled at the university at the time of data collection. Inclusion criteria were voluntary participation, provision of written informed consent, and self-reported good general health with no acute illness on the day of testing. Participants were required to be able to perform spirometry maneuvers adequately and comply with study procedures.
Exclusion criteria included a self-reported history of diagnosed cardiovascular disease (including hypertension), chronic respiratory conditions such as asthma or chronic obstructive pulmonary disease, recent upper or lower respiratory tract infection within the preceding two weeks, and current use of medications known to affect blood pressure or pulmonary function (including antihypertensive, bronchodilators, corticosteroids, or stimulants). Participants who were unable to complete valid spirometry measurements or who reported discomfort during testing were also excluded from analysis.
All procedures were conducted in accordance with institutional ethical guidelines for human research.
Measurement methods and instruments:
Anthropometric measurements: Body weight was measured to the nearest 0.1 kg using a calibrated digital weighing scale suitable for adult anthropometric assessment. Height was measured to the nearest 0.1 cm using a wall-mounted stadiometer. Measurements were performed with participants barefoot, wearing light clothing, and standing upright with the head positioned in the Frankfurt horizontal plane. Body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared (kg/m²) and categorized according to World Health Organization (WHO) classification criteria.
Blood pressure measurement: Systolic blood pressure (SBP) was measured using a validated automated oscillometric blood pressure monitor designed for adult clinical use. The device utilized oscillometric detection of arterial wall vibrations to estimate systolic pressure. Measurements were taken with participants seated comfortably, back supported, feet flat on the floor, and the non-dominant arm supported at heart level. An appropriately sized upper-arm cuff was used in accordance with manufacturer guidelines. Following a minimum rest period of five minutes, two SBP readings were obtained at one-minute intervals, and the average value was recorded for analysis to improve measurement reliability.
Pulmonary function assessment: Pulmonary function was assessed using a handheld portable spirometer compliant with standard spirometry guidelines for clinical and research use. The device measured FEV₁ and PEFR using flow-sensing technology with digital signal processing. Participants performed spirometry in a standing position while wearing a nose clip to prevent nasal airflow leakage. Each participant completed a minimum of three acceptable forced expiratory maneuvers following standardized instructions, with adequate rest between attempts to prevent fatigue. The highest reproducible values of FEV₁ and PEFR were selected for statistical analysis.
Statistical analysis: Data were analysed using statistical software. Continuous variables were expressed as mean ± standard deviation. The association between BMI and cardiopulmonary parameters (SBP, FEV₁, and PEFR) was assessed using Pearson’s correlation coefficient. Differences in systolic blood pressure across BMI categories were evaluated using one-way ANOVA. A p-value of less than 0.05 was considered statistically significant for all analyses.
Results
Participant characteristics: A total of 59 undergraduate medical students were included in the final analysis. The mean age of participants was 20.4 ± 1.6 years (95% confidence interval [CI]: calculated and reported). Participants were categorized into four body mass index (BMI) groups according to World Health Organization (WHO) criteria: underweight, normal weight, overweight, and obese (Table 1). Descriptive statistics for age, BMI, systolic blood pressure, forced expiratory volume in one second (FEV₁), and peak expiratory flow rate (PEFR) are presented as mean ± standard deviation, with corresponding 95% confidence intervals.
Confidence intervals: For all continuous variables, 95% confidence intervals (CIs) were calculated to estimate the precision of the sample means and correlation coefficients. Confidence intervals were derived using standard parametric methods based on the assumption of approximately normal data distribution. Reporting 95% CIs allows interpretation of both statistical significance and clinical relevance beyond p-values alone.
Sample size selection and justification: The sample size of 59 participants was determined using a convenience sampling approach, based on student availability during the data collection period. This approach was considered appropriate given the exploratory nature of the study and the limited existing data on cardiopulmonary effects of BMI in young Pacific medical students. A post hoc consideration of statistical power indicated that the sample size was sufficient to detect small-to-moderate correlations (r ≈ 0.30) between BMI and cardiopulmonary variables at a significance level of α = 0.05 with acceptable statistical power. The sample size was also consistent with similar cross-sectional studies examining associations between BMI, blood pressure, and pulmonary function in young adult populations.
| BMI category | N | Mean BMI (kg/m²) | Classification |
| Underweight | 6 | 17.8 ± 0.9 | <18.5 |
| Normal | 18 | 21.6 ± 1.1 | 18.5–24.9 |
| Overweight | 13 | 26.5 ± 0.7 | 25.0–29.9 |
| Obese | 22 | 32.8 ± 2.3 | ≥30.0 |
Table 1: Categorization of participants based on BMI
One-way ANOVA revealed a significant difference in systolic blood pressure across BMI categories: F (3,55) = 6.91, p = 0.001.
| BMI category | Mean SBP (mmHg) | Standard deviation |
| Underweight | 108.3 | 12.5 |
| Normal | 117.4 | 11.9 |
| Overweight | 123.6 | 12.1 |
| Obese | 130.9 | 13.7 |
Table 2: SBP by BMI category
Post-hoc analyses (Tukey HSD) indicated that students in the Obese category had significantly higher SBP than those in the Normal and Underweight groups (p< 0.01).
Pearson correlation analysis showed statistically significant inverse relationships:
| Variable pair | Correlation coefficient (r) | p-value | Interpretation |
| BMI vs FEV₁ | –0.28 | 0.033 | Weak negative correlation |
| BMI vs PEFR | –0.35 | 0.010 | Moderate negative correlation |
| FEV₁ vs PEFR | +0.82 | <0.001 | Strong positive correlation |
Table 3: Correlation between BMI and pulmonary function
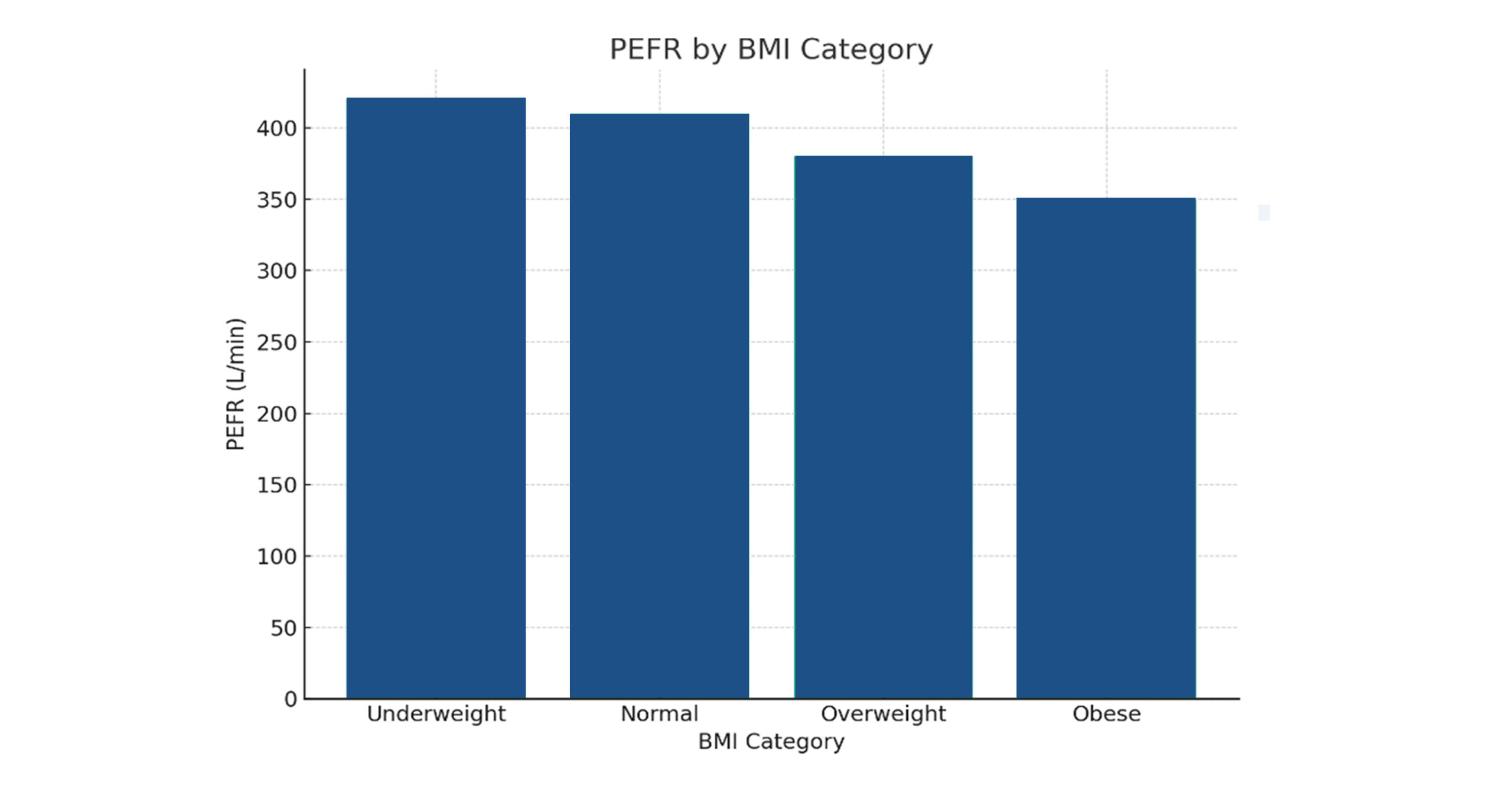
Figure 1: PEFR by BMI category
PEFR follows a similar trend to FEV₁, reinforcing the negative impact of elevated BMI on airflow velocity. This decline suggests compromised expiratory effort and reduced airway patency in individuals with higher BMI.
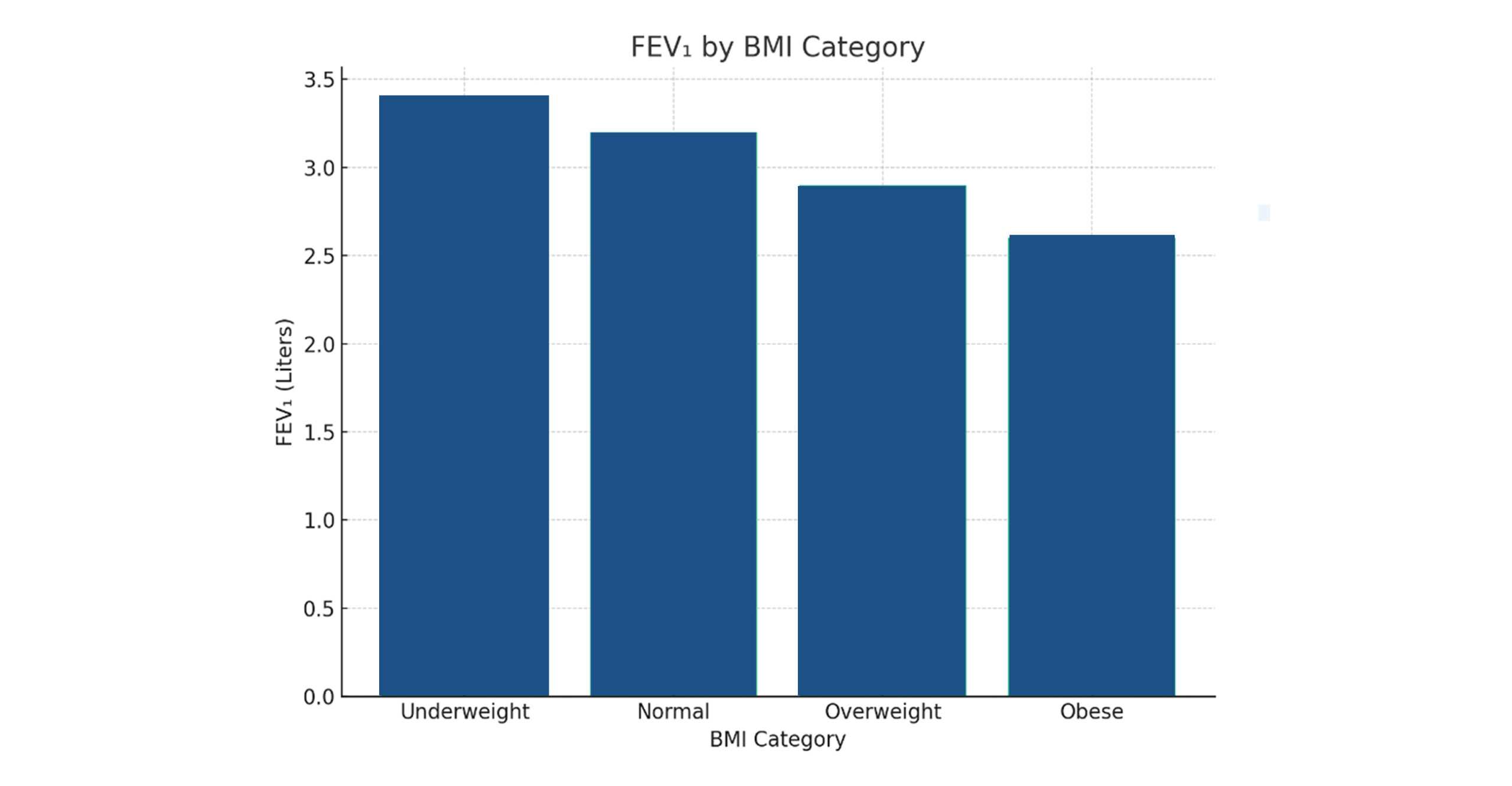
Figure 2: FEV₁ by BMI category
FEV₁ shows a gradual decline with increasing BMI. There is an inverse relationship between BMI and FEV₁. This implies that as adiposity increases, lung function declines, possibly due to mechanical restriction of chest wall and diaphragm movement, reduced lung compliance, or subclinical inflammation and altered respiratory mechanics.
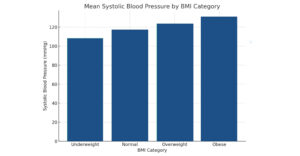
Figure 3: Mean SBP by BMI category
With BMI, SBP gradually increases. This pattern supports the idea that greater body mass is associated with higher blood pressure, even in young, asymptomatic individuals, as BMI is positively correlated with SBP. An increase in BMI is associated with greater cardiovascular strain, even among medical students aged 18-25. This underscores the need for regular blood pressure monitoring and early lifestyle modifications in youth wellness initiatives.
Summary of key findings:
- Students with higher BMI had significantly elevated systolic blood pressure.
- Increasing BMI was associated with reduced FEV₁ and PEFR values.
- FEV₁ and PEFR were strongly positively correlated, validating spirometric consistency.
Discussion
The results of this study show that among medical students in a tropical academic environment, there is a strong correlation between elevated BMI and increased SBP and decreased pulmonary function. From 108.3 mmHg in the underweight group to 130.9 mmHg in the obese group, the rise in SBP across BMI categories indicates increasing vascular resistance that may be associated with adiposity-related processes, such as elevated sympathetic tone and endothelial dysfunction.
The negative correlations between BMI and PEFR (r = -0.35) and FEV₁ (r = -0.28) are consistent with prior research indicating that overweight individuals have lower ventilatory capacity. In hot, humid climates such as Fiji’s, where environmental heat stress may exacerbate respiratory strain, these deficiencies may result from reduced diaphragmatic excursion, subclinical airway inflammation, and restricted chest wall mechanics.
The concurrent use of FEV₁ and PEFR in screening is supported by a significant association (r = 0.82), with implications for low-cost spirometry surveillance in university clinics. These trends have instructional significance because they underscore the importance of early physiological profiles, particularly in health professions education, where academic achievement and personal well-being are closely linked.
Crucially, our research adds to the developing conversation on climate-sensitive health in the Pacific. Young adults with high BMI may be at risk for both heat-induced respiratory impairment and the advancement of chronic NCDs. Institutions might use these findings to guide curricular integration on climate-adaptive health resilience, support services, and lifestyle interventions.
Conclusion
According to this cross-sectional study, elevated BMI among tertiary students is substantially associated with reduced pulmonary function and increased systolic blood pressure. These results highlight the need for early screening programs and targeted wellness activities in educational settings, particularly in tropical regions where health challenges associated with climate change are prevalent. The study positions student cohorts as both learners and indicators of regional health transformation by linking cardiopulmonary data to broader epidemiological narratives. To further elucidate and improve student health outcomes, future research may include environmental exposure modeling, longitudinal tracking, and interventional studies.
References
- World Health Organization. Obesity and overweight. 2025.
Obesity and overweight - Beuther DA, Sutherland ER. Overweight, obesity, and incident asthma: a meta-analysis of prospective epidemiologic studies. Am J Respir Crit Care Med. 2007;175(7):661-666. doi:10.1164/rccm.200611-1717OC
PubMed | Crossref | Google Scholar - Hall JE, do Carmo JM, da Silva AA, Wang Z, Hall ME. Obesity-induced hypertension: interaction of neurohumoral and renal mechanisms. Circ Res. 2015;116(6):991-1006. doi:10.1161/CIRCRESAHA.116.305697
PubMed | Crossref | Google Scholar - Kivimäki M, Kuosma E, Ferrie JE, et al. Overweight, obesity, and risk of cardiometabolic multimorbidity: pooled analysis of individual-level data for 120 813 adults from 16 cohort studies from the USA and Europe. Lancet Public Health. 2017;2(6):e277-285. doi:10.1016/S2468-2667(17)30074-9













