







 Author Affiliations
Author Affiliations
Abstract
Background: The use of universal preventive measures is a standard measure of protection for health-care workers and patients from the spread of infections in health-care facilities, particularly in intensive care units (ICU). Although recommendations exist, adherence is inconsistent and can affect the safety of the patient and the healthcare results.
Aim: The purpose of this study was to assess the knowledge and compliance with universal safety information among the ICU nurses.
Methodology: This study adopted a descriptive cross-sectional survey design where 80 registered ICU nurses were conveniently recruited. These were developed from a structured self-completed questionnaire with questions intended to elicit respondents’ demographic characteristics, level of understanding of universal precaution measures, and observed behaviors. Frequency, descriptive, and inferential statistical tests were used to compare the knowledge and practice score means, to determine the relationship between knowledge and practice scores, education, and experience.
Results: The performed study revealed that 93.75% of interviewed nurses comprehend the meaning of universal precautions, and 97.5% of respondents knew how to perform correct hand hygiene. However, there were perceived gaps in their knowledge regarding equipment sterilization 81.25% and vaccination schedules 75%. Compliance with practices was inconsistent; 87.5% of participants uniformly wore gloves when dealing with body fluids; however, only 50% used a face shield or goggles. Nurses with university education attained a better result in the knowledge and practice tests than those with only a diploma or a certificate in nursing; and moreover, the more experienced the nurses, the better their scores in the knowledge and practice tests the scores in the two tests were highly correlated, knowledge and practice (r = 0.75 at
p = 0.01).
Conclusion: The study highlighted that while ICU nurses had good knowledge of universal precautions, gaps in applying this knowledge, particularly with protective gear, were evident. The strong correlation between knowledge and practice emphasizes the need for continuous training. Targeted interventions to improve compliance and resource availability are essential to enhance patient safety in critical care settings.
Keywords
Universal precautions, Intensive care unit nurses, Demographic information, Infection control, Healthcare compliance.
Introduction
Universal Precaution (UP) means measures or steps taken to minimize or offset the risk of infection from agents transmissible through the blood in all health care activities. These safety measures are wearing personal protective gear, safe handling and disposal of sharps, washing of hands, and safe injections. ICU is a hospital’s branch responsible for the recipients who are severely ill; it focuses on constant observation and the application of enhanced medical treatment.[1] UP is applied by ICU nurses, who are healthcare specialists who provide intensive care to relieve patients and HCWs from infection risks. This paper aims to investigate the knowledge of UP amongst the ICU nurses and their compliance level with these fundamental preventive measures against infections. [2]
The strategies in infection control known as the universal precautions were developed in the 1980’s largely due to rising incidences of human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) in health care facilities. Since then, UP has become a key principle of infection prevention and control, aiming at establishing perceptions that all human blood and certain body fluids can contain pathogens.[3] The research shows that UP is an important component in minimizing the development of healthcare-associated infections (HAIs) that have a negative impact on patient outcomes globally. Especially in the high-risk units such as the ICU, patients suffer from comorbidities and reduced immunity. Collectively, UP must be strictly followed to prevent the transmission of infection to vulnerable individuals and healthcare workers.[4]
ICU nurses are on the frontline when it comes to patients who are critically ill or acutely ill with life-threatening illnesses. This position entails them to carry out different invasive procedures such as inserting catheters, managing mechanical ventilators, and administering intravenous medications, hence predisposing them to contract diseases of body fluids.[5] As a result, the ICU nurses should be conversant with UP and, above all, practice the guidelines herein to avoid cross-contamination and infection. Evaluating their level of understanding and implementation of UP is important in order to find areas of deficiency that need to be rectified so as to raise infection control measures and enhance patient outcomes.[6]
ICU nurses’ level of knowledge about UP affects their adherence to these protocols since they are the ones who know the ICU environment best. Knowledge involves appreciation of the rationale for each precaution, identifying consequences of non-adherence to set guidelines, and knowing current measures on infection control.[7,8] Other research has revealed that only HCWs with a good understanding of UP practices are likely to adhere to set infection control measures. Thus, the assessment of the ICU nurses’ knowledge in this area is an important approach towards the positive enactment of the UP in the context of the ICU.
Methodology
Quantitative cross-sectional study was carried out at ICU of a tertiary care teaching hospital in Swat. The target population for this study encompassed 80 nurses practicing at the deferred critical care units: Geriatrics Intensive Care Unit (GICU), neuro high dependency unit (Neuro HDU), pediatric intensive care unit (PICU), and neonatal intensive care unit (NICU). A convenient sampling method was used to select participants.
Data collection procedure: Participants were given a complete questionnaire, and for most of the questions, the items used were originally developed from previous research. The questionnaire was divided into three sections:
Demographic information: This section obtained information concerning participants’ gender and age, their educational level, and experience in nursing.
Knowledge of universal precautions: This section evaluated the nurses’ understanding of universal precautions. The responses were available as yes, no, or don’t know.
Practices of universal precautions: This section compares how often the nurses employed universal precautions. Responses were measured on a Likert scale with the following options: The frequency response options are always, often, sometimes, seldom, never.
The participants were allowed adequate time to complete the allocated questionnaire, and researchers were on hand in case some clarification was needed.
Data analysis procedure: Data was analyzed using the statistical package for social sciences (SPSS) version 24. In the analysis, both frequency numbers and percentages, as well as analysis of variance procedures, were used. Descriptive techniques included phone number averages, number, frequency, and standard deviation that were used on the demographic data, as well as the number right plus the number wrong on the knowledge and practice items. The chi-square test was used to estimate the differences in knowledge and practices of universal precautions between different groups (educational level, length of service).
Ethical consideration: Ethical clearance to conduct the study was sought from the medical superintendent of the SGTH hospital. All participants provided written informed consent. Thus, they volunteered themselves, and anonymity was also ensured.
Results
Demographic characteristics of study participants: The demographic characteristics of the participants total 80 participants were chosen for the study. Of all the participants, most were male at 62.5% (Table 1).
| Demographic variable | Frequency (%) |
| Gender | |
| Female | 30 (37.5%) |
| Male | 50 (62.5%) |
| Age | |
| 20-30 years | 25 (31.25%) |
| 31-40 years | 35 (43.75%) |
| 41-50 years | 15 (18.75%) |
| 51+ years | 5 (6.25%) |
| Education level | |
| Diploma | 40 (50%) |
| Bachelor’s degree | 37 (46.3%) |
| Master’s degree | 03 (3.7%) |
| Years of experience | |
| 1-5 years | 25 (31.25%) |
| 6-10 years | 35 (43.75%) |
| 11+ years | 20 (25%) |
Table 1: Demographic characteristics of participants (n = 80)
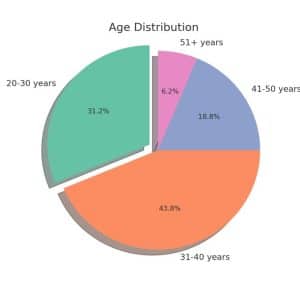
Figure 1: Age distribution of participants
The participants’ knowledge of healthcare and safety seems to indicate a good understanding of most of the measures in place, such as hand hygiene (Table 2).
| Knowledge item | Yes (%) | No (%) | Don’t Know (%) |
| Do you know what universal precautions are? | 75 (93.75%) | 5 (6.25%) | 0 (0%) |
| Are you familiar with the correct hand hygiene procedure? | 78 (97.5%) | 2 (2.5%) | 0 (0%) |
| Do you understand the need for personal protective equipment (PPE)? | 70 (87.5%) | 8 (10%) | 2 (2.5%) |
| Are you aware of the blood-borne pathogen risks? | 72 (90%) | 6 (7.5%) | 2 (2.5%) |
| Do you know the steps of sterilizing equipment? | 65 (81.25%) | 10 (12.5%) | 5 (6.25%) |
| Are you aware of the recommended vaccination schedule for healthcare workers? | 60 (75%) | 15 (18.75%) | 5 (6.25%) |
Table 2: Knowledge of universal precautions among ICU nurses
The majority continue to maintain proper hand hygiene, where 75% did so before touching any patient and 81.25% after meeting a patient (Table 3).
| Practice item | Always (%) | Often (%) | Sometimes (%) | Seldom (%) | Never (%) |
| Hand hygiene before patient contact | 60 (75%) | 15 (18.75%) | 5 (6.25%) | 0 (0%) | 0 (0%) |
| Hand hygiene after patient contact | 65 (81.25%) | 10 (12.5%) | 5 (6.25%) | 0 (0%) | 0 (0%) |
| Wearing gloves when handling bodily fluids | 70 (87.5%) | 8 (10%) | 2 (2.5%) | 0 (0%) | 0 (0%) |
| Wearing masks while treating suspected infectious patients | 60 (75%) | 15 (18.75%) | 5 (6.25%) | 0 (0%) | 0 (0%) |
| Disposing of needles and sharp objects safely | 55 (68.75%) | 15 (18.75%) | 10 (12.5%) | 0 (0%) | 0 (0%) |
| Disinfecting surfaces after patient contact | 50 (62.5%) | 20 (25%) | 10 (12.5%) | 0 (0%) | 0 (0%) |
| Use of face shields or goggles during patient care | 40 (50%) | 20 (25%) | 15 (18.75%) | 5 (6.25%) | 0 (0%) |
Table 3: Practices of universal precautions among ICU nurses
The mean knowledge and practice scores of the identified nurses with reference to their educational attainment and years of experience, as well as the associated p-values (Table 4).
| Variable | Mean knowledge Score (±SD) | Mean practice Score (±SD) | p-value |
| Nurses with diploma education | 7.5 (±0.8) | 4.2 (±0.6) | 0.04 |
| Nurses with bachelor’s degree | 7.5 (±0.8) | 4.2 (±0.6) | 0.03 |
| Nurses with master’s degree | 6.9 (±1.2) | 3.5 (±0.8) | 0.005 |
| Nurses with 1-5 years of experience | 6.5 (±1.0) | 3.3 (±0.7) | 0.04 |
| Nurses with 6-10 years of experience | 7.4 (±0.9) | 4.0 (±0.6) | 0.02 |
| Nurses with 11+ years of experience | 7.8 (±0.7) | 4.5 (±0.5) | 0.04 |
Table 4: Relationship between knowledge and practices of universal precautions
Discussion
Education and its impact on knowledge and practice: The study found that the level of education had a positive relationship with both knowledge and practice scores, with individuals holding higher educational qualifications (Baccalaureate and master’s degrees) performing better in both knowledge and practice compared to those with a Diplomate level of education. This may be due to the more comprehensive infection control training provided in higher education programs. This finding is consistent with other research, which has shown that healthcare workers with higher levels of education tend to have better knowledge and practices related to infection control.[9] A study on nursing staff in various hospital settings highlighted that nurses with advanced degrees or certifications were more likely to follow infection control guidelines than those with lower education levels. This suggests that education plays a crucial role in ensuring a strong understanding and adherence to infection prevention measures.[10]
Experience and its role in practice: Nurses with over ten years of practice scored higher in infection control practices, suggesting that experience in real-life situations contributes to better adherence to universal precautions. This finding aligns with the idea that prolonged exposure to infection control measures and practical situations enhances compliance.[11] Similarly, studies have indicated that healthcare workers with more years of experience are more likely to follow infection control protocols due to constant exposure to infection control practices and direct patient care.[12] A study in an ICU setting found that experienced nurses were better at handling infection control measures, such as proper disposal of sharps and wearing personal protective equipment (PPE). This highlights the value of practical experience in improving adherence to infection control protocols.[13]
Impact of demographics on knowledge and practice: The chi-square tests revealed significant relationships between demographic variables (education level and years of experience) and both knowledge and practice of infection control. This underscores the importance of ongoing professional development to maintain high standards in infection control.[14] Many studies have emphasized the importance of continuous professional development in improving infection control practices. A study in a hospital setting found that regular training and updates on infection prevention significantly improved compliance among healthcare workers, particularly in high-risk areas like ICUs. This reinforces the idea that knowledge and practice are closely tied to education, experience, and continuous learning.[15]
Barriers to infection control practice: Despite high knowledge and positive attitudes, gaps were identified in specific practices, such as PPE usage and the safe disposal of sharps. Notably, 50% of workers reported always wearing face shields or goggles, suggesting a need for additional training and policy review to increase compliance.[16] This finding is consistent with studies that have found barriers to full adherence to infection control practices, particularly in high-risk areas like the ICU. While healthcare workers may be aware of the importance of PPE, factors like fatigue, workload, and lack of consistent reminders can affect their behavior.[17] Research has shown that targeted interventions, such as regular audits, reminders, and reinforcement, can help address these gaps in practice and increase PPE usage.[18]
Limitations of the study: There were several main limitations of this study that need to be taken into consideration when analyzing the results. First, this research was done only in one tertiary care hospital in Swat, which would in a way restrict the findings to the same hospital and area where the study was conducted. Consequently, the knowledge and practice of ICU nurses, as described in the study, may not reflect the whole picture of the other healthcare organizations or regions.
Recommendations: To improve compliance with universal precautions among ICU nurses, the following recommendations are proposed: implement regular training, ensure consistent availability of PPE, provide targeted support for less qualified nurses, establish monitoring and feedback systems, enforce clear protocols, promote a safety-focused culture, and conduct periodic evaluations to refine strategies and enhance patient safety.
Conclusion
While there is a high awareness of these issues and the knowledge levels are generally high, a major concern arises from the variance between these knowledge levels and practice, identifying room for improvement in training familiarization resources and compliance with infection prevention measures. They could also assist in ensuring that knowledge transforms into practice, which will reduce the risks involved between healthcare workers and new patients in high-risk ICUs. The findings throw light upon the need to upgrade oneself, particularly in matters concerning the nursing profession, and hence reduce this healthcare-acquired infection. Subsequent studies could address these questions in other healthcare environments and aim to design effective adherence-raising programs for the use of nursing personnel.
References
- Delgado PEJ, Pérez Olmos LM, Celis Salazar O. Intervention model for exposure and control of biological risk: Study of universal precautions in nursing staff. Techno Rev Int. 2023;15(1):2-9. doi:10.37467/revtechno.v13.4963
Crossref | Google Scholar - World Health Organization. Guidance on ensuring a sufficient supply of safe blood and blood components during emergencies. 2023 Guidance on ensuring a sufficient supply of safe blood and blood components during emergencies
- Shah SR, Aziz S, Cheema OA, Dar SF, Ateeq M. A survey of awareness, training, and compliance regarding universal precautions among house officers in a peripheral teaching hospital in an HIV endemic area. Prof Med J. 2020;27(9):1936-1941. doi:10.29309/TPMJ/2020.27.09.4492 Crossref | Google Scholar
- Isma M, Extension K. Assessment of infection control measures and risk factors at Kampala International University Teaching Hospital in Bushenyi District: A study on staff awareness and implementation. Kiu Publication. 2023;12(2):132-146. doi:10.59298/INOSRES/2023/2.10.1000 Crossref
- Okore LA. Experiences of Critical Care Nurses in End-of-life Care to Adult Patients in the Critical Care Unit, Kenyatta National Hospital. (Doctoral dissertation). University of Nairobi; 2023 Experiences of Critical Care Nurses in End-of-life Care to Adult Patients in the Critical Care Unit, Kenyatta National Hospital
- Gordon JM, Magbee T, Yoder LH. The experiences of critical care nurses caring for patients with COVID-19 during the 2020 pandemic: A qualitative study. Appl Nurs Res. 2021;59:151418. doi:10.1016/j.apnr.2021.151418
PubMed | Crossref | Google Scholar - Hallgren J, Larsson M, Kjellén M, Lagerroth D, Bäckström C. “Who will do it if I don’t?” Nurse anaesthetists’ experiences of working in the intensive care unit during the COVID-19 pandemic. Aust Crit Care. 2022;35(1):52-58. doi:10.1016/j.aucc.2021.11.003 PubMed | Google Scholar
- Morris KY, Jakobsen R. Central venous catheter access and procedure compliance: A qualitative interview study exploring intensive care nurses’ experiences. Intensive Crit Care Nurs. 2022;69:103182. doi:10.1016/j.iccn.2021.103182 PubMed | Crossref | Google Scholar
- Kluck JP, Stoyanova F, Krämer NC. Putting the social back into physical distancing: The role of digital connections in a pandemic crisis. Int J Psychol. 2021;56(4):594-606. doi:10.1002/ijop.12746 PubMed | Crossref | Google Scholar
- Alotaibi NE. Factors influencing intensive care nurses’ adherence to “prevention of ventilator-associated pneumonia” clinical practice guidelines in Saudi Arabia: A mixed-methods study. Saudi Digital Library; 2023 Factors influencing intensive care nurses’ adherence to “prevention of ventilator-associated pneumonia” clinical practice guidelines in Saudi Arabia: A mixed-methods study
- Alsaqr AM. Remarks on the use of Pearson’s and Spearman’s correlation coefficients in assessing relationships in ophthalmic data. Afr Vision Eye Health. 2021;80(1):1-10. doi:10.4102/aveh.v80i1.612 Crossref | Google Scholar
- Shah H, Sardar A, Dildar M, Ejaz HK, Muhammad A. Effect of demonstration regarding percutaneous endoscopic gastrostomy tube feeding among caregivers of patients diagnosed with esophageal carcinoma. medtigo J Med. 2024;2(4):e14324867. doi:10.5281/zenodo.14324867 Crossref | Google Scholar
- Smethers JD. The role of the academic dean in higher education in the United States. (PhD dissertation). University of Tennessee; 2020. The role of the academic dean in higher education in the United States
- Xie L, Liu Z, Hao S, et al. Assessment of knowledge, attitude, and practice towards pulmonary rehabilitation among COPD patients: A multicenter and cross-sectional survey in China. Respir Med. 2020;174:106198. doi:10.1016/j.rmed.2020.106198 PubMed | Crossref | Google Scholar
- Al Shraah A, Abu-Rumman A, Al-Madi F, Ali F, Alhammad F, Aljboor A. The impact of quality management practices on knowledge management processes: A study of a social security corporation in Jordan. TQM J. 2021;ahead-of-print. doi:10.1108/TQM-08-2020-0183 Crossref | Google Scholar
- Hall S, Johnson P, Bailey C, Gould Z, White R, Crook B. Evaluation of face shields, goggles, and safety glasses as a virus transmission control measure to protect the wearer against cough droplets. Ann Work Expo Health. 2023;67(1):36-49. doi:10.1093/annweh/wxac047 PubMed | Crossref | Google Scholar
- Bauhoff S. Self-report bias in estimating cross-sectional and treatment effects. In: Encyclopedia of Quality of Life and Well-Being Research. Springer International Publishing; 2024:6277-6279. doi:10.1007/978-3-031-17299-1_4046 Crossref | Google Scholar
Acknowledgments
Not reported
Funding
Not reported
Author Information
Corresponding Author:
Muhammad Shoaib
Department of Nursing
Saidu Group of Teaching Hospital Swat, Pakistan
Email: mshoaib6587@gmail.com
Co-Authors:
Abbas Khan
Department of Nursing
Saidu Group of Teaching Hospital Swat, Pakistan
Shah Hussain
Department of Nursing
Zalan College of Nursing Swat Pakistan
Authors Contributions
All authors contributed to the conceptualization, investigation, and data curation by acquiring and critically reviewing the selected articles. They were collectively involved in the writing – original draft preparation, and writing – review & editing to refine the manuscript. Additionally, all authors participated in the supervision of the work, ensuring accuracy and completeness. The final manuscript was approved by all named authors for submission to the journal.
Ethical Approval
Ethical clearance to conduct the study was sought from the medical superintendent of the SGTH hospital. All participants provided written informed consent. Thus, they volunteered themselves, and anonymity was also ensured.
Conflict of Interest Statement
Not reported
Guarantor
None
DOI
Cite this Article
Muhammad S, Abbas K, Shah H. Assessment of Knowledge and Practices of Universal Precautions Among Intensive Care Unit Nurses at Tertiary Care Hospital Swat. medtigo J Med. 2025;3(1):e30623113. doi:10. 63096/medtigo30623113 Crossref













