







 Author Affiliations
Author Affiliations
Abstract
Background: Oxygen therapy is a critical intervention for managing patients in critical care units, particularly those with respiratory complications. Nurses play a pivotal role in administering oxygen therapy, and their knowledge, attitude, and practice (KAP) significantly affect patient outcomes. This study aimed to assess the KAP of nurses in oxygen therapy at a tertiary care hospital in Swat, Pakistan.
Methodology: A descriptive cross-sectional study was conducted among 80 nurses using a structured questionnaire. Participants were selected through convenient sampling. Data was analyzed using statistical package for the social sciences (SPSS) version 24, using descriptive and inferential statistical methods to evaluate replies related to KAP.
Results: The findings revealed that 90% of nurses knew oxygen as a drug, and 75% acknowledged its prescription necessity except in emergencies. However, gaps in understanding peripheral oxygen saturation (SpO2) levels and oxygen therapy for specific conditions, such as Chronic obstructive pulmonary disease (COPD), were observed. Attitudes towards guideline use and documentation were positive, but only 40% reported periodic review of protocols. Practice indicators highlighted strong knowledge of oxygen delivery devices but identified areas requiring further training, such as complications management.
Conclusion: While nurses demonstrated commendable baseline knowledge, significant misconceptions and practice gaps were identified. Regular training sessions and protocol updates are recommended to address these issues and ensure safer oxygen therapy administration.
Keywords
Oxygen therapy, Critical care, Knowledge, Attitudes, Practices, Patient safety.
Introduction
Oxygen therapy involves supplying a patient with additional oxygen when their blood oxygen concentrations are low or due to other medical needs. It is an effective measure, especially where there is an evident critical respiratory problem, as seen in patients in the intensive care unit. Oxygen therapy mainly focuses on the nurses. Therefore, nursing KAP significantly determines the efficiency of oxygen therapy.[1] Therefore, adequate knowledge of oxygen therapy devices, their application procedures, and the safety precautions necessary for the reduction of adverse impacts and enhancement of results should be developed. That is why the delivery of oxygen can have adverse effects, such as oxygen toxicity, hypoxemia, or tissue damage in the case of mismanagement.[2] Thus, evaluation and improvement of KAP in the indicated sphere of knowledge among nurses remains one of the urgent priorities for patient care.[3]
Oxygen therapy is one of the mainstays of management for conditions such as COPD, Acute Respiratory Distress Syndrome (ARDS), and post-COVID respiratory sequelae. It most emphatically has been the case in critical care units where life and death constantly hang in the balance: nurses expertly ordered the oxygen delivery systems to come to the rescue of their units.[4] This includes knowledge of oxygen delivery equipment and oxygen rates, flow, and patient assessment.[5] Nurses’ knowledge can be seen to play an immediate role in clients’ care, particularly in the prevention of complications such as respiratory failure or cardiovascular stress.[6] The accreditation of knowledge is required to determine what weaknesses there are that could potentially compromise the level and quality of care.[7] To overcome these gaps, continuous professional education is extremely important. The awareness on the part of nurses can be boosted to enhance the quality of the outcome for clients in critical care.[8]
Another important factor influencing oxygen therapy administration is aspects of attitudes. Fifty-eight percent of respondents consider that oxygen is safe as an adjunct therapy, while 80% stated that adjunct oxygen is important in nursing practice.[9] When a health care worker has a positive attitude towards a particular protocol, then they are more likely to adhere to and remain vigilant of the patient; however, misconceptions can be fatal.[10] For example, some nurses may consider oxygen therapy as safe without any risk factors, and as a result, important measures are not taken. Such perceptions are the misconceptions that need to be uncovered by attitudinal assessments to redesign interventions to change perceptions.[11] Attitudes toward proper oxygen therapy can be changed with training programs that address this issue as evidence-based. This means nurses remained safe and proactively minded in critical care areas.[12]
The practice of oxygen therapy is where knowledge and attitude come into practice. Conventional practice implies properly choosing an oxygen delivery device, setting the right flow rate, and evaluating a patient’s reaction.[13] It also involves awareness of situations where patients develop complications, for example, hypoxemia or hyperoxia. Safe and effective patient care requires that critical care unit nurses produce evidence of competency in these practices.[14] Employee remunerations encourage the workers to undergo standard skills tests frequently, and feedback mechanisms suggest further development opportunities. By so doing, healthcare organizations can improve aspects related to the implementation of oxygen therapy. This avoids a lot of mistakes and has been proven to maintain standard protocols and procedures in line with clinical practice.[15]
Methodology
The study was conducted at Saidu Group of Teaching Hospital (SGTH), Swat, Khyber Pakhtunkhwa (KPK), Pakistan, a tertiary care hospital that serves a diverse population and has qualified staff. The study looked to assess the KAP of nurses concerning oxygen therapy in critical care units. The study was carried out using a descriptive cross-sectional design to assess the variables at a single point in time. According to Rao Soft, the calculated sample size was 80, with a total population of 100, using a 95% confidence interval, 5% margin of error, and 50% population proportion. Due to practical constraints, convenient sampling was performed, ensuring easy recruitment of the participants. Inclusion criteria consisted of registered nurses who had worked in critical care units for one year or more, including those willing to participate, while the exclusion criteria excluded interns, managerial/supervisor positions, and nurses who did not provide direct patient care.
Data collection procedure: The data was collected using an adopted structured questionnaire, and participants were given informed consent to participate in the study before the data was collected. Closely related to the problem, the confidentiality of all data used during the research was guaranteed. The questionnaire consisted of four sections: The first section involved demographic information, the second section involved knowledge, the third section involved attitudinal information, and the fourth section involved information on practice. The participants explained the objectives of the study and volunteered to be involved in the study. CA processes were followed by the researchers during the whole research process to ensure participants’ anonymity and confidentiality. In data collection methodology, to respect the rights of participants, the method adopted was ethical.
Data analysis procedure: Collected data were analyzed using SPSS version 24. In descriptive data analysis, mean, median, mode, and standard deviation were used on continuous variables. For nominal data, the frequency and percentage distributions were calculated. The analysis enabled the researcher to determine the dispersion and measure of the central tendency of the collected data. The data analysis method of the study was made easy by the SPSS software because it enabled easy organization of data in a systematic manner, which enabled easier interpretation of results. The use of statistical analysis capabilities provided a different appraisal of the study’s variables. These techniques are methods of gaining an understanding of the participant’s KAP.
Ethical consideration: Ethical Approval was received from the Medical Superintendent of the hospital. Ref No IRB/SGTH/2025/10. All participants provided written informed consent. Thus, they volunteered themselves, and anonymity was also ensured. The participants were made aware that the study would never harm or benefit any of them. To maintain anonymity and confidentiality, the participants’ identification was eliminated from the questionnaires, and the data were kept secure. The participants were told that their participation was voluntary and that all responses given would be kept anonymous. The data collected remained accessible only to the researcher and the authorized personnel involved in the study.
Results
Demographic characteristics of study participants: Demographic data, the study focused on the participants. 80 in total, which included 56.2% females and 43.8% males. Regarding age, 37.5% of the participants were within 20–30 years, and 31.3% within 31–40 years. In terms of education, 75 percent of the respondents had a bachelor’s degree; 21.2 percent had a Diploma, and 3.8 percent had a master’s degree. Most of the participants were from the Coronary Care Unit (CCU) 31.3%, then Neonatal intensive care unit (NICU) 25%, while others were in the Pediatric Intensive Care Unit (PEADS ICU), emergency, or other departments. The participants’ experience ranged as follows: 50% had 1 to 5 years; 25% had 6 to 10 years of experience. Also, only 6.2% of the respondents had work experience of more than 15 years. Of equal importance, concerning the participants, 75% of them said that they had never attended any workshop on the practice of oxygen therapy.
| Variable | Frequency (n) | Percentage (%) |
| Gender | ||
| Male | 35 | 43.8 |
| Female | 45 | 56.2 |
| Age | ||
| 20–30 years | 30 | 37.5 |
| 31–40 years | 25 | 31.3 |
| 41–50 years | 20 | 25.0 |
| >50 years | 5 | 6.2 |
| Education level | ||
| Diploma | 17 | 21.2 |
| Bachelor’s degree | 60 | 75 |
| Master’s degree | 03 | 3.8 |
| Department | ||
| NICU | 20 | 25.0 |
| CCU | 25 | 31.3 |
| PEADS ICU | 15 | 18.7 |
| Emergency | 10 | 12.5 |
| Other | 10 | 12.5 |
| Work experience | ||
| 1–5 years | 40 | 50.0 |
| 6–10 years | 20 | 25.0 |
| 11–15 years | 15 | 18.7 |
| >15 years | 5 | 6.2 |
| Workshops on oxygen therapy | ||
| Yes | 20 | 25 |
| No | 60 | 75 |
Table 1: Demographic characteristics of participants
The study sample comprised 43.8% male and 56.2% female participants, indicating a higher representation of females in the study. This gender distribution reflects a typical balance observed in healthcare settings, where female healthcare workers (HCWs) often outnumber their male counterparts.
Figure 1: Gender of participants
Most participants (90%) recognized oxygen as a drug, demonstrating a strong awareness of its pharmacological classification. Most (75%) documented the need for oxygen prescription except in emergencies and displayed a good understanding of its controlled use. A high percentage (85%) of associates associate bluish discoloration around the mouth with respiratory distress and prominent knowledge of clinical signs. However, only 30% correctly identified SpO2 >98% as not typically indicating distress, indicating some misconceptions. Furthermore, awareness of symptoms of oxygen loss, such as dizziness and tingling, was evident in 70% of participants.
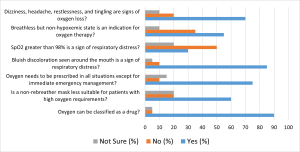
Figure 2: Knowledge of oxygen therapy
These responses suggest confident support when using expert guidelines or protocol in oxygen therapy, with 65% strongly agreeing with the statement and another 30% agreeing. Knowledge of the variety of oxygen delivery devices: 50% strongly agreed, 35% agreed, while 15% were not too sure or disagreed. On one hand, 75 percent strongly agreed on the worth of learning oxygen therapy procedures. However, only 40 percent provided guidelines periodically, indicating there could be weaknesses regarding updating these practices. Regarding the attitude towards caring about the patient’s comfort during the therapy, the majority, 60% of participants, strongly agreed with this option. Probably the most important aspect they got right is the documentation of records of oxygen therapy, which is of high importance, with 70% strongly agreeing.
| Statement | Strongly agree (%) | Agree (%) | Disagree (%) | Strongly disagree (%) |
| Using expert guidelines or protocols on oxygen therapy is advantageous to intuition. | 65.0 | 30.0 | 5.0 | 0.0 |
| I am familiar with different oxygen delivery devices. | 50.0 | 35.0 | 10.0 | 5.0 |
| Guidelines on O2 therapy are reviewed periodically. | 40.0 | 30.0 | 20.0 | 10.0 |
| The oxygen therapy procedure is a worthwhile learning experience. | 75.0 | 20.0 | 5.0 | 0.0 |
| Do you ensure patient comfort during oxygen therapy? | 60.0 | 30.0 | 5.0 | 5.0 |
| Do you address patient anxiety related to oxygen therapy? | 50.0 | 30.0 | 15.0 | 5.0 |
| Do you prevent oxygen therapy-related complications? | 55.0 | 30.0 | 10.0 | 5.0 |
| Do you accurately document oxygen therapy records? | 70.0 | 20.0 | 5.0 | 5.0 |
Table 2: Attitude towards oxygen therapy
The results also reveal that 90% of participants provided the right answer for pulse oximetry, estimating the arterial oxygen saturation. A significant number of them (85%) realize that it is used to boost blood oxygen concentration to normal levels. Yet only 30% of participants think that COPD is a relative indication for oxygen therapy, while 60% disagree with it. 80% of the participants concur that the flow rate of oxygen therapy needs to be increased if the saturation level of the patient remains low, and only 70% appreciate the value of measuring the saturation level every 30 minutes during the oxygen therapy. Moreover, 75% of them affirm that oxygen therapy could be applied during cardiac arrest, while 65% correctly deny that oxygen therapy should be stopped suddenly. Finally, 85% acknowledge the accuracy of Venturi masks in providing a fraction of inspired oxygen (FiO2).
| Statement | Yes (%) | No (%) | Not Sure (%) |
| Pulse oximetry estimates the arterial oxygen saturation of hemoglobin? | 90.0 | 5.0 | 5.0 |
| Is the primary goal of oxygen therapy to increase oxygen levels in the blood? | 85.0 | 5.0 | 10.0 |
| Is COPD a contraindication for oxygen therapy? | 30.0 | 60.0 | 10.0 |
| Should you increase the oxygen flow rate if a patient’s oxygen saturation level remains low? | 80.0 | 10.0 | 10.0 |
| Should you assess a patient’s oxygen saturation level every 30 minutes during oxygen therapy? | 70.0 | 20.0 | 10.0 |
| Can oxygen therapy be used to treat cardiac arrest? | 75.0 | 15.0 | 10.0 |
| Can oxygen therapy be discontinued abruptly? | 25.0 | 65.0 | 10.0 |
| Venturi mask delivers precise FiO2? | 85.0 | 10.0 | 5.0 |
Table 3: Practice on oxygen therapy
The table shows the correlation of demographic variables with knowledge and practice of oxygen therapy. There were perceived strong correlations of knowledge and practices in oxygen therapy with gender (male), age (20-30 and 31–40 years), educational attainment (bachelor’s and master’s degrees), and years of work experience (1-5 and 6–10 years). Moreover, participants who had been trained in oxygen therapy workshops also showed improvement. However, the gender role of females, age 41–50 years, diploma education level, and work experience of more than 10 years were not significant predictors. The study emphasizes that age, education, and training should be employed to improve oxygen therapy knowledge.
| Demographic variable | Category | Chi-square value | p-value | Significance |
| Gender | Male | 3.89 | 0.049 | Significant |
| Female | 2.56 | 0.110 | Not Significant | |
| Age | 20–30 years | 5.12 | 0.023 | Significant |
| 31–40 years | 6.45 | 0.011 | Significant | |
| 41–50 years | 2.56 | 0.110 | Not significant | |
| Education level | Diploma | 3.21 | 0.071 | Not significant |
| Bachelor’s Degree | 7.80 | 0.005 | Significant | |
| Master’s Degree | 4.92 | 0.027 | Significant | |
| Work experience | 1–5 years | 6.78 | 0.009 | Significant |
| 6–10 years | 4.31 | 0.038 | Significant | |
| 11–15 years | 3.12 | 0.077 | Not significant | |
| Workshops on oxygen therapy | Yes | 9.23 | 0.002 | Significant |
| No | 3.14 | 0.090 | Not significant |
Table 4: Comparison of demographic variables with KAP
Discussion
According to the findings of the present study, there were considerable results in terms of KAP of the study sample regarding oxygen therapy. Most participants identified oxygen correctly as a drug, and 90% agreed with this classification. This is in line with the earlier findings showing that while general knowledge of oxygen therapy and its pharmacological classification can go a long way in ensuring patient safety in healthcare practice, more complex and heightened levels of understanding are required moving forward.[16] However, although 97% were aware that oxygen is a drug, only 30% pointed out that SpO2 above 98 % is not indicative of respiratory distress; this is in contrast to other works where greater knowledge of these clinical signs was observed. This could be due to a lack of practical experience in college or the fact that some hospitals have different teaching methods.[17]
The research also showed that seventy-five percent of the respondents agreed with the fact that oxygen should be prescribed except in emergency cases. This result is by clinical recommendations that have cautioned practitioners against the excessive prescription of oxygen in non-critical care settings.[18] The same observation has been made by other researchers: the results showed that those HCWs who have been trained in oxygen therapy understand more about its prescribed use. However, this study also pointed out an error-understanding scenario regarding the appropriateness of non-rebreather masks for patients with high oxygen demands, which is opposite to many other studies conducted where such misunderstandings were not present at higher frequencies.[19] This might mean that the participants in this study did not undergo thorough training in oxygen delivery devices.[20]
We also asked the participants for clinical signs of respiratory distress, and 85% said the bluish color around the mouth was a sign of distress. This is in concordance with clinical reasoning and practice evidenced in other studies, and identifying signs of hypoxia: skin color change is an indispensable component of oxygen therapy management.[21] With clinical knowledge and practices observed in other studies, recognition of visible symptoms of hypoxia is a critical part of managing oxygen therapy.[22] But half of the sample in this study got it wrong; they did not understand that more than 98% indicated a lack of respiratory distress. Nine previous investigations also reported that HCWs have a relatively accurate perception of normal SpO2 compared with this study’s findings.[23] The difference might be because of inadequate training on how to interpret oxygen saturation numbers or different clinical practices that were practiced at the study site.[24]
Concerning the understanding of oxygen therapy guidelines, 75% of the participants believed learning the oxygen therapy procedure to be worthwhile, while 70% estimated the accurate documentation of oxygen therapy to be important.[25] This finding emphasizes the necessity of record keeping for safety, which includes an important feature of clinical practice in other work too. However, only 40% strongly agreed that guidelines on oxygen therapy were reviewed periodically, like in what others establish settings, for example, a failure in continuous education and reviewing.[26] This gap could be due to compliance with up-to-date practices, which are hard to maintain in busy clinic settings, or due to the absence of good
programs.[27]
In the practice session, over ninety percent of the participants were able to correctly answer the questionnaire item. According to pulse oximetry, this is an estimate of arterial O2 saturation. The majority (85%) also knew the main purpose of oxygen therapy, which is to raise the oxygen concentrations in the blood.[28] From these results, it can be inferred that the majority of the participants seemed to have a considerable understanding of the cardinal rules of oxygen administration.[29] Nevertheless, as much as 60% of the respondents disagreed with COPD being a contraindication for oxygen therapy, which is quite contrary to other studies where patients with COPD had a fairly good understanding of oxygen therapy. This might be attributed to the differences in the healthcare facilities’ management of COPD or incomplete or unclear information relayed by the study kits.[30]
Limitations of the study: This study had a small sample, which probably did not allow for the representation of the broader healthcare population. The specificity of departments and regions from which participants were recruited has limited the generalization of the findings across all healthcare contexts that could represent a combination of organizations in developing countries. Selecting a larger and more diverse number of participants would have given better, more reliable, and generalizable findings.
The cross-sectional design of this study collects information at just one point. Because of this, it cannot generalize about the progression or change of knowledge, attitudes, or practices. A longitudinal design would allow for a long-term examination of trends and the influence of interventions on oxygen therapy practice. Self-reported data used in this study may be subject to some bias. The chances were high that participants reported inflated measures of knowledge or an answer with the socially acceptable stance. Using tools such as direct observation and audits would have given a more accurate picture of the actual practices.
Moreover, the study was purely quantitative and did not take this opportunity to investigate the underlying rationale for certain practices or gaps in knowledge with qualitative methods, such as interviews or focus groups. This has crippled the understanding of the driving factors behind the attitudes and actions of HCWs. Lastly, the clinical elements of oxygen therapy focused on in this study are recovery rates of patients, complications, and any administration errors not addressed. Their inclusion would have provided a fuller picture of how HCWs’ knowledge and practices could impact patient care and safety. Future studies addressing these limitations would carry forward the outcomes as well as provide a holistic understanding of oxygen therapy in critical care contexts.
Conclusion
Therefore, this study offers relevant knowledge, attitudes, and practices of oxygen therapy among HCWs. From the results shown above, it can be assumed that the subject’s knowledge of oxygen therapy is quite profound, and the participants’ understanding of oxygen therapy as a drug and its purpose in raising the blood oxygen level is vivid. However, several significant knowledge deficits have been identified, including knowledge deficits about SpO2 and the use of oxygen therapy in clinical conditions like COPD. This is why there is a need for encoding and refreshing knowledge through seminars, training, and periodic workshops to complement the inadequacies. In addition, considerable relationships between demographic variables, including gender, age, education, and working experience, also strengthen the justification of subsequent educational prevention based on such variables. It is apparent from the study results that there is scope for further improvement and upgrading the training sessions dealing with oxygen therapy and the clinical guidelines and practices.
References
- Ortega MA, Fraile-Martinez O, García-Montero C, et al. A general overview on the hyperbaric oxygen therapy: applications, mechanisms and translational opportunities. Medicina (Kaunas). 2021;57(9):864. doi:10.3390/medicina57090864 PubMed | Crossref | Google Scholar
- Sonners J. Hyperbaric oxygen and regenerative medicine: non-traditional uses to help reduce inflammation, stimulate cell regeneration and improve healing. Integr Complement Ther. 2022;28(4):166-171. doi.10.1089/ict.2022.29033.jso Crossref | Google Scholar
- Kooner HK. Structure and function of long-COVID evaluated using pulmonary imaging. Doctoral dissertation. The University of Western Ontario; 2024. Structure and Function of Long-COVID Evaluated Using Pulmonary Imaging
- Peck TJ, Hibbert KA. Recent advances in the understanding and management of ARDS. F1000Res. 2019;8:F1000 Faculty Rev-1959. doi:10.12688/f1000research.20411.1 PubMed | Crossref | Google Scholar
- El Haddaoui S, Amekran Y, El Hangouche AJ. Pulmonary rehabilitation following the 2019 novel coronavirus infection. Pneumologia. 2020;69(4):197-208. doi.10.2478/pneum-2021-0013 Crossref | Google Scholar
- Yogesh M, Kadalarasu D, Gandha K, Gandhi R. An evaluation of knowledge, attitudes, practice, and associated factors regarding oxygen therapy among resident doctors in a tertiary care teaching hospital: a mixed-methods study. J Educ Health Promot. 2024;13(1):382. doi.10.4103/jehp.jehp_1954_23 PubMed | Crossref | Google Scholar
- Getahun YA, Bizuneh YB, Melesse DY, Chekol WB. Assessment of practice and barriers of oxygen therapy in critically ill patients among nurses: a survey from University of Gondar Comprehensive Specialized Hospital Northwest, Ethiopia, 2021. Ann Med Surg (Lond). 2022;76:103481. doi.10.1016/j.amsu.2022.103481
PubMed | Crossref | Google Scholar - Jacobs SS, Krishnan JA, Lederer DJ, et al. Home oxygen therapy for adults with chronic lung disease: an official American Thoracic Society clinical practice guideline. Am J Respir Crit Care Med. 2020;202(10):e121-141. doi.10.1164/rccm.202009-3608ST PubMed | Crossref | Google Scholar
- Holland AE, Cox NS, Houchen-Wolloff L, et al. Defining modern pulmonary rehabilitation: an official American Thoracic Society workshop report. Ann Am Thorac Soc. 2021;18(5):e12-29. doi.10.1513/AnnalsATS.202012-1524ST PubMed | Crossref | Google Scholar
- Franklin D, Babl FE, George S, et al. Effect of early high-flow nasal oxygen vs standard oxygen therapy on length of hospital stay in hospitalized children with acute hypoxemic respiratory failure: the PARIS-2 randomized clinical trial. JAMA. 2023;329(3):224-234. doi.10.1001/jama.2023.4587 Crossref | Google Scholar
- Emeka N. Nurses’ attitudes towards caring for older patients with delirium – A systematic literature Review. Degree thesis. The Novia University of Applied Sciences; 2020. Nurses’ attitudes towards caring for older patients with delirium – A systematic literature Review
- Rege S, Bavadekar A, Vernekar D. Mistreatment of women in labor room: perceptions of healthcare providers. In: Handbook on Sex, Gender and Health: Perspectives from South Asia. Singapore: Springer Nature; 2024:1-22. doi.10.1007/978-981-19-9265-0_27-1 Crossref | Google Scholar
- Gottlieb J, Capetian P, Hamsen U, et al. German S3 guideline: oxygen therapy in the acute care of adult patients. Respiration. 2022;101(2):214-252. doi.10.1159/000520374 PubMed | Crossref | Google Scholar
- MacLeod M, Papi A, Contoli M, et al. Chronic obstructive pulmonary disease exacerbation fundamentals: Diagnosis, treatment, prevention and disease impact. Respirology. 2021;26(6):532-551. doi:10.1111/resp.14041
PubMed | Crossref | Google Scholar - Jacobs SS, Krishnan JA, Lederer DJ, et al. Home oxygen therapy for adults with chronic lung disease: an official American Thoracic Society clinical practice guideline. Am J Respir Crit Care Med. 2020;202(10):e121-141. doi.10.1164/rccm.202009-3608ST PubMed | Crossref | Google Scholar
- Stawicki SP, Jeanmonod R, Miller AC, et al. The 2019–2020 novel coronavirus (severe acute respiratory syndrome coronavirus 2) pandemic: A joint American College of Academic International Medicine–World Academic Council of Emergency Medicine multidisciplinary COVID-19 working group consensus paper. J Glob Infect Dis. 2020;12(2):47-93. doi.10.4103/jgid.jgid_86_20 PubMed | Crossref | Google Scholar
- Dardas LA, Khalaf I, Nabolsi M, Nassar O, Halasa S. Developing an understanding of adolescents’ knowledge, attitudes, and practices toward COVID-19. J Sch Nurs. 2020;36(6):430-441. doi.10.1177/1059840520957069
PubMed | Crossref | Google Scholar - Maude RR, Jongdeepaisal M, Skuntaniyom S, et al. Improving knowledge, attitudes, and practice to prevent COVID-19 transmission in healthcare workers and the public in Thailand. BMC Public Health. 2021;21(1):749. doi.10.1186/s12889-021-10768-y PubMed | Crossref | Google Scholar
- Hajjar LA, Costa IBSDS, Rizk SI, et al. Intensive care management of patients with COVID-19: a practical approach. Ann Intensive Care. 2021;11(1):36. doi:10.1186/s13613-021-00820-w PubMed | Crossref | Google Scholar
- Ospina-Tascón GA, Calderón-Tapia LE, García AF, et al. Effect of high-flow oxygen therapy vs conventional oxygen therapy on invasive mechanical ventilation and clinical recovery in patients with severe COVID-19: a randomized clinical trial. JAMA. 2021;326(21):2161-2171. doi:10.1001/jama.2021.20714 PubMed | Crossref | Google Scholar
- Adewale GO. Educating Nurses on Failure to Rescue Due to Treatment Delay. Doctoral dissertation. Walden University; 2023. Educating Nurses on Failure to Rescue Due to Treatment Delay
- Arabani Nezhad M, Ayatollahi H, Heidari Beigvand H. Development and evaluation of an e-learning course in oxygen therapy. BMC Med Educ. 2022;22(1):776. doi.10.1186/s12909-022-03838-1 PubMed | Crossref | Google Scholar
- Rhagnanan-Kramer V. Critical Care Nurses’ Perceptions of Safety Related to Using Complex Medical Devices in Daily Nursing Practice. Doctoral dissertation. Nova Southeastern University; 2020. Critical Care Nurses’ Perceptions of Safety Related to Using Complex Medical Devices in Daily Nursing Practice
- Mwima RJ. Clinical Placement Support as a Means of Enhancing Critical Care Competences Among ICU Nursing Trainees: A Case of Uganda Heart Institute, Mulago. Master’s thesis. Kyambogo University; 2023. Clinical Placement Support as a Means of Enhancing Critical Care Competences Among ICU Nursing Trainees
- Ochoki NO. Factors Associated with Adherence to Tracheostomy Care Guidelines Among Critical Care Nurses at Kenyatta National Hospital. Master’s thesis. Jomo Kenyatta University; 2016. Factors Associated with Adherence to Tracheostomy Care Guidelines Among Critical Care Nurses at Kenyatta National Hospital
- Zhang M, Jin A, Zhou X, et al. A quasi-experimental study on couple-based exercise program improving cardiac rehabilitation exercise compliance in post-PCI patients. BMC Cardiovasc Disord. 2024;24(1):640. doi.10.1186/s12872-024-04282-3 PubMed | Crossref | Google Scholar
- Curtis BR, Rak KJ, Richardson A, et al. Perceptions of hyperoxemia and conservative oxygen therapy in the management of acute respiratory failure. Ann Am Thorac Soc. 2021;18(8):1369-1379. doi.10.1513/AnnalsATS.202007-802OC PubMed | Crossref | Google Scholar
- Khalid Ahmed A, Elsayed Ouda W, Saied El-Nagger N, Mohamed Hafez M. Pitfalls in nurses’ performance regarding oxygen therapy administration at neonatal intensive care units: an assessment study. Egypt J Health Care. 2024;15(3):462-476. doi.10.21608/ejhc.2024.376621 Crossref | Google Scholar
- Gottlieb ER, Ziegler J, Morley K, et al. Assessment of racial and ethnic differences in oxygen supplementation among patients in the intensive care unit. JAMA Intern Med. 2022;182(8):849-858. doi.10.1001/jamainternmed.2022.2587 PubMed | Crossref | Google Scholar
- Melesse DY, Chekol WB. The management of patients with coronavirus disease 2019 in intensive care unit (ICU) in low-income countries: A review article. Clin Nutr Open Sci. 2021;37:60-72. doi:10.1016/j.nutos.2021.05.001
Crossref | Google Scholar
Acknowledgments
Not reported
Funding
Not reported
Author Information
Corresponding Author:
Nasar Mian
Department of Nursing
National College of Nursing, Swat, Pakistan
Email: nasarmian819@gmail.com
Co-Authors:
Abdul Sami
Department of Emergency Medicine
Shifa International Hospital, Islamabad, Pakistan
Shah Hussain
Department of Nursing
Zalan College of Nursing, Swat, Pakistan
Authors Contributions
Nasar Mian was responsible for data collection and data analysis. Abdul Sami contributed to data collection, while Shah Hussain handled data analysis.
Ethical Approval
Ethical Approval was received from the Medical Superintendent of the hospital with Ref No IRB/SGTH/2025/10. All participants provided written informed consent. Thus, they volunteered themselves, and anonymity was also ensured. All participants provided written informed consent.
Conflict of Interest Statement
Not reported
Guarantor
None
DOI
Cite this Article
Nasar M, Sami A, Shah H. Assessing Knowledge, Attitude, and Practice of Nurses Regarding Oxygen Therapy in the Critical Care Units at Tertiary Care Hospital Swat, Pakistan. medtigo J Emerg Med. 2025;2(1):e3092216. doi:10.63096/medtigo3092216 Crossref













