






 Author Affiliations
Author Affiliations
Abstract
This report describes a case of antenatally detected pelvic abdominal cystic mass, bilateral hydronephrosis, and oligohydramnios. Antenatal ultrasound scans could not further characterise the mass, but noted debris within the mass. Two likely diagnoses, based on the ultrasound scan findings, were a haemorrhagic ovarian cystic mass and lower urinary tract obstruction with a distended bladder. Neonatal clinical findings and neonatal magnetic resonance imaging (MRI) confirmed a diagnosis of hydrometrocolpos secondary to a transverse vaginal septum. The neonate also had postaxial polydactyly on the right hand and foot. The neonate was vomiting after feeding and could only tolerate very small feeds at a time. She was passing urine and meconium well. A nasogastric tube was inserted, and a referral to paediatric surgeons was made. Initial drainage was done 3 days after delivery to relieve pressure effects on the gastrointestinal and urinary systems. The baby was able to feed normally after the surgery. A septectomy was done at 5 months of age, and a foley catheter was left in situ for 3 weeks before removal. No cardiac anomalies or any other abnormalities were noted in the neonate. She has been followed up to 10 months of age and has attained appropriate developmental milestones for her age. Molecular tests to establish whether there was a genetic cause to her condition could not be done.
Keywords
Hydrometrocolpos, Vaginal septum, Ultrasound scan, Magnetic resonance imaging, Polydactyly, Hydronephrosis, Antenatal.
Introduction
Foetal pelvic abdominal cystic masses are rare and may have various aetiologies. When they arise in female foetuses, they could have a gastrointestinal or genitourinary origin. Those of genitourinary origin include hydrometrocolpos, ovarian cysts, hydronephrosis, and a distended bladder due to lower urinary tract obstruction, among others.[1] Most of these cysts are incidental findings on routine third-trimester antenatal ultrasound scans. The location of the cystic mass, its relationship to surrounding structures, and morphology may help to reach an exact diagnosis on ultrasound scanning, but foetal MRI may be more useful. Neonatal clinical examination, including genital scrutiny and neonatal MRI, will reveal the exact diagnosis in most cases.
Case Presentation
A 41-year-old pregnant lady presented to our clinic for the first time at 36 weeks of gestation. It was her second pregnancy with a different partner from the first pregnancy. She had a history of caesarean section in the first pregnancy about 9 years prior, for foetal macrosomia (birth weight 4600 g). Diabetes screening was negative, but the mother had unexplained hypochromic microcytic anaemia of 6.4 g/dL. Her haemoglobin level improved to 11 g/dL after receiving 2 units of packed cell blood at the referring hospital and iron/folic acid supplements for 6 weeks.
Antenatal radiological assessment: An ultrasound scan done outside our unit, at about 32 weeks of gestation, revealed foetal bilateral hydronephrosis, query a distended foetal urinary bladder with debris, and oligohydramnios. A repeat ultrasound scan done at our unit showed a cystic mass measuring 6.47 x 5.78 x 6.15 cm with a volume of 120 ml arising from the pelvis and containing internal echoes, likely a haemorrhagic ovarian cyst. There was foetal hydroureteronephrosis. Oligohydramnios, with an amniotic fluid Index of 4.49 cm, was also noted. Dilatation of the maternal renal calyces and renal pelvis was found and thought to be physiological changes for pregnancy.

Figure 1: Repeat ultrasound scan showing the foetal pelvic cystic mass with internal echoes
The patient declined trial of labour after caesarean section and opted for elective caesarean and bilateral salpingectomy to prevent future conception. There was evident oligohydramnios during caesarean section done at 38 weeks +3 days gestation.
Postnatal physical examination: The genitals appeared normal. The neonate had fully developed extra digits on the right hand and right foot. The extra digits were on the side of the pinkie finger and the small toe, respectively.
Postnatal radiological investigation: A neonatal ultrasound scan was done, which revealed a cystic pelvic abdominal mass with internal echoes. An MRI was ordered on the second day post-delivery.
Case Management
Management of the neonate: A live baby girl was delivered with Apgar scores of 8/10 at 1 minute and then 10/10 at 5 minutes. Baby passed urine almost immediately from a patent urethra. The genitals appeared normal. The neonate had fully developed extra digits on the right hand and right foot. The extra digits were on the side of the pinkie finger and the small toe, respectively. The baby was, however, vomiting after feeds, and the paediatrician suggested small, frequent feeds through a nasogastric tube. The nasogastric tube was draining straw-coloured fluid with some ground coffee-like particles. An MRI was ordered which showed hydrometrocolpos and a vaginal septum. The patient was transferred to paediatric surgeon who confirmed a diagnosis of hydrometrocolpos and a transverse vaginal septum. The uterus was drained of the mucoid components through an abdominal incision and hysterotomy. This was done to reduce the pressure effects on the urinary tract and the stomach, which caused hydroureter, hydronephrosis, and vomiting after feedings.

Figure 2: MRI of the baby showing hydrometocolpos (A) and Vaginal septum (B)
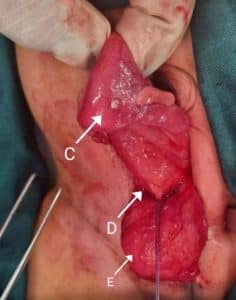
Figure 3: Picture showing collapsed uterus (C) after surgical drainage, drainage site (D), and urinary bladder (E)
Follow-up management: A size 4 foley catheter was left in situ for continuous drainage through the anterior abdominal wall, but it remained inactive after the procedure. It was removed after about 1 month. At 5 months of age, surgical management of the septum was instituted, and a size 4 Foley catheter was left in situ. This was removed after 3 weeks. The infant is, however, developing well and has attained all appropriate milestones to date. Mother’s recovery post-surgery was unremarkable. The mother could not afford the deoxyribonucleic acid (DNA) tests to assess for any molecular basis of the baby’s condition.
Patient perspective: The mother of the infant was very anxious about the antenatal diagnosis. The paediatrician explained that it was likely an ovarian cyst, based on the antenatal ultrasound scan findings, and this was a condition that could be surgically managed in the immediate neonatal period. The mother was reassured by this discussion. Postnatally, the vomiting was a concern for the mother, but the baby’s passing urine and meconium allayed her fears. The mother was happy about the results of the initial surgery. The major concern was the inactive drain, which she felt was an inconvenience for the whole month it was in situ. The mother is very happy with the progress the child has made, as she has attained all developmental milestones appropriately. She is also not concerned about the possibility of a genetic condition, as she does not intend to conceive in the future and has backed that up with bilateral tubal ligation.
Discussion
Hydrometrocolpos is caused by distal vaginal obstruction due to congenital urogenital anomalies or acquired aetiologies such as infection, trauma, or sexual abuse. Vaginal obstruction can occur with an imperforate hymen, a transverse septum in the vagina, vaginal atresia, or persistence of the urogenital sinus or cloaca.[1] Congenital anomalies causing hydrometrocolpos are classified into five types based on the level of obstruction and severity of the urogenital or cloacal malformation. Type I is associated with imperforate hymen, type II with a vaginal septum, type III with distal vaginal atresia, type IV is vaginal atresia with persistent urogenital sinus, and type V is associated with vaginal atresia with a cloacal anomaly. Inspection of external genitalia may provide clues for initial classification.[2] In our case, the cause of hydrometrocolpos was type II, with an associated transverse vaginal septum. Most cases of hydrometrocolpos are sporadic, but the condition may occur following prenatal dexamethasone treatment for congenital adrenal hyperplasia. It has also been associated with ambiguous genitalia in 45, X0/46, XY mosaicism, and McKusic–Kaufman syndrome.[3]
Haemato/Hydrometrocolpos typically presents late in pregnancy, at around 30 weeks on average. The earliest prenatal diagnosis of an imperforate hymen with hydrometrocolpos has been reported at 25 weeks of pregnancy.[4] In our case, the diagnosis was made after 32 weeks of gestation. This condition is relatively rare and occurs only in female foetuses. The reported incidence of hydrometrocolpos is around 0.006%.[5] During pregnancy, hormones produced in the mother cause increased secretions in the uterus, cervix, and vagina of the baby. When there is a blockage to the flow of secretions out of the vagina, they accumulate in the baby’s vagina and sometimes in the uterus. This causes the swelling detected on the prenatal scan as seen in our case with accumulation in the uterus and the vagina. After the initial drainage in theatre, 3 days after delivery in our case, the drain became inactive due to the withdrawal of maternal estrogen after delivery of the baby, which caused the secretions to dry out.[6]
Differential diagnosis of antenatal pelvic masses: Prenatally, the presence of a fluid–debris level inside a pelvic cystic anechoic mass must be considered a crucial finding. Multiple internal echoes are due to thick mucoid cervical or vaginal secretions. Prenatal cystic dilatation of the vagina is often misdiagnosed as a distended bladder, as the bladder is displaced anteriorly by the vagina making it difficult to identify.[7] This was the case with the initial ultrasound scan done by this patient, where lower uterine tract obstruction, causing bladder distension, was suspected. The ultrasound scan done within our unit suggested an ovarian cyst, which is a common differential diagnosis for a cystic mass in prenatal imaging. Prenatal ultrasound, therefore, has a definitive role in detecting an obstructed genital tract, allowing rapid postnatal treatment to drain the vagina and relieve the urinary tract obstruction. Foetal MRI is invaluable in confirming the ultrasound findings and improving diagnostic accuracy. The prognosis and neonatal management of isolated hydrocolpos differ greatly from those of hydrocolpos associated with a cloacal malformation associated with other anomalies, so it is important to get a prenatal diagnosis for planning purposes.[8,9]
Persistent urogenital sinus was at the top of the list of differential diagnoses for the patient on presentation to the paediatric surgeons. The presence of a persistent urogenital sinus is associated with uterine anomalies (bicornuate uterus, cervical atresia), vaginal atresia or duplication, hydronephrosis, renal agenesis, imperforate anus, polycystic kidneys, oesophageal atresia and sacral hypoplasia. This was ruled out when the patient was found to have a normal urethra, rectum, and otherwise well-developed vagina, albeit with a transverse vaginal septum.[1]
Other findings: The antenatal ultrasound scans reported oligohydramnios. The amniotic fluid volume varies in the different cases of hydrometrocolpos listed in the literature. Some cases present with polyhydramnios, whilst others, like this case, have oligohydramnios.
Another interesting finding was postaxial polydactyly. This is a frequent congenital hand malformation characterized by fifth-digit duplications in hands and/or feet. Its prevalence is estimated between 1/630 and 1/3300 in the Caucasian race and between 1/100 and 1/300 in the Black race. In the Type A phenotypic category, the extra digit is well formed and articulates with the fifth or an extra metacarpal. This was exactly like our case. Type B phenotype is characterised by a rudimentary extra fifth digit, which is usually represented by an extra skin tag. Both types can be inherited by an autosomal dominant or recessive trait.[10]
McKusick-Kaufman syndrome (MKKS): MKKS is a condition characterized by extra fingers and/or toes (polydactyly), congenital heart defects, and genital abnormalities. The most common genital abnormality is hydrometrocolpos. The extra digits are typically on the same side of the hand or foot as the pinkie or little toe (postaxial polydactyly), which was the case in our patient. The congenital heart defects in individuals with MKKS can include an atrial septal defect or a ventricular septal defect.[6] No cardiac abnormalities were detected in our patient. MKKS is an autosomal recessive disease. It was first described by McKusick in 1964 in two Amish siblings. This disease occurs due to a mutation in the MKKS gene at the 20p12 location. Mutations in the MKKS gene result in the formation of a defective protein that is similar to the members of the chaperonin family, leading to anomalous limbs, heart, and reproductive system.[7] Cardinal features of MKKS in females are hydrometrocolpos and polydactyly. Polydactyly is present in 90% of cases. It is predominantly post-axial and rarely mesoaxial. Syndactyly may also be encountered. MKKS shows association with congenital heart defects such as atrioventricular canal defects, ventricular septal defects, and hypoplastic left heart in 10% to 20% of cases. Other less commonly associated findings are gastrointestinal abnormalities (28%) that consist of imperforate anus, rectovaginal or vesicovaginal fistula, Hirschsprung’s disease, and malrotation. Abnormalities of the eyes (5%) are also mentioned in the literature.[7] Although no cardiac abnormalities were detected in our patient, MKKS is a strong possibility in this patient because of the hydrometrocolpos, the most common genital abnormality in MKKS. The extra digits on the same side of the hand or foot as the pinkie or little toe (postaxial polydactyly) are typical of MKKS.
Conclusion
Congenital hydrometrocolpos is a rare condition that can be detected on a prenatal ultrasound scan. It presents as a cystic pelvic abdominal mass that may cause pressure effects on surrounding organs. There is a wide spectrum of differential diagnoses. Foetal MRI is useful for definitive prenatal diagnosis, but this was not available for our patient, so the actual diagnosis was made postnatally. Scrutiny of the genitalia and clinical examination is crucial, and this, in addition to imaging, will provide a definite diagnosis. Hydrometrocolpos with postaxial polydactyly may be associated with MKKS, a genetic disorder. Genetic tests were invaluable for this diagnosis to be confirmed, but were not done.
References
- Singh S, Singh P, Singh RJ. Persistent urogenital sinus. J Anat Soc India. 2010;59(2):242-244.
doi:10.1016/s0003-2778(10)80034-6 Crossref | Google Scholar - Tegene D, Assefa T, Edris A. Neonatal hydrometrocolpos secondary to imperforate hymen presented with acute urinary retention: Case report. Res Rep Neonatol. 2023;13:23-28. doi:10.2147/rrn.s433727 Crossref | Google Scholar
- Hydrocolpos/Hydrometrocolpos. updated January 2021. Hydrocolpos/Hydrometrocolpos
- Kurniawati EM, Zaki A, Yanuar J, Utomo SA. Hydrometrocolpos in neonate with imperforate hymen: Diagnosis and treatment. Eurasia J Biosci. 2020;14:3273-3277. Hydrometrocolpos in neonate with imperforate hymen: Diagnosis and treatment
- Chen MC, Chang YL, Chao HC. Hydrometrocolpos in Infants: Etiologies and Clinical Presentations. Children (Basel). 2022;9(2):219. doi:10.3390/children9020219 PubMed | Crossref | Google Scholar
- Scott CA, Marsden AN, Rebagliati MR, et al. Nuclear/cytoplasmic transport defects in BBS6 underlie congenital heart disease through perturbation of a chromatin remodeling protein. PLoS Genet. 2017;13(7):e1006936. doi:10.1371/journal.pgen.1006936 PubMed | Crossref | Google Scholar
- Yewalkar SP, Yadav VK, Khadse G. The McKusick-Kaufman hydrometrocolpos-polydactyly syndrome: A rare case report. Indian J Radiol Imaging. 2013;23(2):183-185. doi:10.4103/0971-3026.116573
PubMed | Crossref | Google Scholar - Taori K, Krishnan V, Sharbidre KG, et al. Prenatal sonographic diagnosis of fetal persistent urogenital sinus with congenital hydrocolpos. Ultrasound Obstet Gynecol. 2010;36(5):641-643. doi:10.1002/uog.7721
PubMed | Crossref | Google Scholar - Bhagat AC, Gupta RS, Malik R. Antenatal diagnosis of hydrometrocolpos with Mullerian duplication on ultrasound and fetal MRI: case report and literature review. BJR Case Rep. 2023;9(3):20230024. doi:10.1259/bjrcr.20230024
PubMed | Crossref | Google Scholar - Kyriazis Z, Kollia P, Grivea I, Stefanou N, Sotiriou S, Dailiana ZH. Polydactyly: Clinical and molecular manifestations. World J Orthop. 2023;14(1):13-22. doi:10.5312/wjo.v14.i1.13 PubMed | Crossref | Google Scholar
Acknowledgments
I would like to acknowledge the mother of the patient described in the case report, who allowed us to write up this case and updated us on all developments with her child. I would also like to acknowledge Riverside hospital for allowing us to publish the case report, the Radiology department for their keen interest in the case and providing the images as requested, the paediatrician who assessed the baby soon after birth and transferred the neonate to the paediatric surgeons promptly, and the paediatric surgeons at Bokamoso hospital who promptly undertook the immediate and subsequent surgical management.
Funding
There was no funding received for this case report.
Author Information
Corresponding Author:
Plaxcedes S Chikwema
Department of Obstetrician and Gynaecology
Riverside Hospital, Francistown, Botswana
Email: [email protected]
Co-Authors:
Andrew Ojuka
Department of General Surgery
Riverside Hospital, Francistown, Botswana
Christian Jabo
Department of Radiology
Riverside Hospital, Francistown, Botswana
Authors Contributions
Plaxcedes S. Chikwema was responsible for patient care, manuscript development, literature review, and write-up. Andrew Ojuka handled proofreading and editing. Mothusi M. Gaiketse provided initial care to the neonate and facilitated the referral to the paediatric surgeon. Christian Jabo performed and reported on the ultrasound scans at their unit.
Ethical Approval
Consent to publish this case report was sought from the mother of the infant presented in the case report. The hospital ethics review board approved the case report.
Conflict of Interest Statement
The author declares no conflict of interest.
Guarantor
None
DOI
Cite this Article
Plaxcedes SC, Andrew O, Mothusi MG, Christian J. Antenatal Hydrometrocolpos with Transverse Vaginal Septum and Polydactyly. medtigo J Med. 2025;3(1):e3062311. doi:10.63096/medtigo3062311 Crossref













