






 Author Affiliations
Author Affiliations
Abstract
Background: Ethnic-induced conflict has displaced millions in Ethiopia. There is a paucity of information on maternal and child health service utilization among internally displaced persons (IDPs). This study assessed antenatal care (ANC) utilization and associated factors among internally displaced reproductive-age women in North-Shewa camps, Amhara region.
Methodology: A facility-based cross-sectional study was conducted from February to March 2023. Using simple random sampling, 512 women were included. Binary logistic and Poisson regression models identified factors associated with ANC utilization and the number of visits. Adjusted odds ratio (AOR) and adjusted incidence rate ratio (AIRR) with 95% confidence interval (CI) estimated the strength of association.
Results: Overall, 51% of women received at least one ANC service; only 5.2% had the recommended four or more visits. Factors significantly associated with ANC utilization included husbands with primary education or above (AOR: 2.6), pregnancy complications (AOR: 4.1), good knowledge of ANC (AOR: 5.67), wanted pregnancy (AOR: 8.1), and distance to health facilities (AOR: 4.45). Poisson regression showed empowered women (AIRR: 1.3), those with good knowledge (AIRR: 1.29), living in camps with health facilities (AIRR: 1.72), and wanted pregnancies (AIRR: 1.27) were associated with a higher frequency of visits.
Conclusion: Nearly half of the women did not utilize ANC services, and a small fraction met the recommended four visits. Sociodemographic, obstetric, and health facility factors affect utilization. Availing health facilities in camps and enhancing education and awareness could help women utilize ANC services.
Keywords
Antenatal care visit, Internally displaced person, Pregnancy, Knowledge, Complications.
Introduction
An internally displaced person (IDP) is a person who is forcefully evicted to leave her/his home due to natural or man-made reasons and still lives within his/her country’s territorial boundary.[1] Due to conflict and violence, more than 41 million people were internally displaced globally, and 21 million were women and girls (of which Sub-Saharan Africa (SSA) contributed around 40%). Ethiopia had one of the hugest burden.[2] Recent reports of international organization for migration (IOM) indicated that, in 2023, about 2.75 million people (532, 889 households) were internally displaced in Ethiopia, more than half (64.6%) were displaced due to conflict; according to IOM’s report in 2022, the number of Amhara displaced from Metekel zone in Benishangul-Gumz region and from both east and west Wellega zones in Oromia region to settle in Amhara region increased by 14.5 % (67,053 IDPs) compared with the previous report. Most of these IDPs are ethnic induced (99.8 %).[2]
Antenatal care is a key intervention in reducing maternal and newborn mortality, as highlighted in the “Safe Motherhood Package” developed by the World Health Organization (WHO).[3] The 2016 WHO ANC model aims to provide respectful, individualized, person-centered care for pregnant women. The model recommends eight contacts.[4,5] Although ANC has a positive impact on maternal health, the utilization of the recommended number of visits remains low, particularly in SSA.[6,7] Studies conducted among internally displaced women revealed that service utilization was even lower, which stood at 28% in Nigeria (28%), 59% in the Democratic Republic of Congo, and 82% in Syria.[8-11] IDPs encounter more negative health outcomes than refugees.[12] They face sexual and reproductive health (SRH) problems such as intimate partner violence (IPV) and acquire sexually transmitted infections like Human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS).[13] The problem is devastating among adolescent girls due to SRH-related mortalities and morbidities, and its effect on their children.[2]
Studies have indicated that different factors are associated with ANC service utilization among IDP women. Socio-demographic (including couples’ educational status, maternal age, husband’s educational status, household monthly income, lack of knowledge); health system-related factors (including distance to the health facility); and political factors such as conflict and affect ANC service uptake.[14-18] Missing ANC visit had adverse maternal and birth outcomes. For instance, a study done in Tigray, Ethiopia, revealed that women who had fewer than four ANC visits had 4.35 times more risk of experiencing adverse birth outcomes; another study done in Nigeria also showed that attending fewer than 4 ANC visits increases the odds of maternal death by 1.75 times among pregnant mothers.[16,17] Despite the highest magnitude of displaced persons (due to conflict, natural disaster, and other factors), studies are lacking on assessing ANC service utilization among internally displaced reproductive age group women, who have been displaced from different parts of Ethiopia. Thus, our study aims to assess the magnitude of ANC service utilization and its associated factors among internally displaced reproductive age Amhara women in the North Shewa camps of the Amhara region and to bridge this gap and generate evidence for policymakers. By identifying key predictors of maternal care experiences among displaced women, this study provides evidence that can guide policy actions and interventions to enhance service delivery and women’s autonomy in humanitarian settings.
Methodology
Study design and area: The study employed a camp-based cross-sectional study design during February-March 2023. The study was conducted in the Amhara region, which is the second-largest region in Ethiopia. BahirDar is the capital city of the region and is located 540 km from the capital city of Addis Ababa. The region has 15 zones and town administrations. According to the Regional Disaster Risk Management Bureau, there were about 840,714 internally displaced people in the region in 2022. Around 136,857 were found in 37 camps, located in six different zones. IDPs were temporarily settled in North Shewa zone (24,170), East Gojjam (16,071), West Gojjam (193,780), BahirDar (7.893), Awi zone (30,602), Waghmera zone (92,822), Oromo zone (4,623), South Wello (16,594), Gondar Town (2,238), Waghmera (32,961), North Gondar (12,824), and South Gondar (431). There are 13 IDP camps in North Shewa zone alone (6 in DebreBirhan, 1 in Minjar, 1in Menz Lalo, 1 in MenzMama, 1 in Menz Keya, 1 in M ida, 1 in Ataye town, &1 in Shewa Robit town).
Source and study population: The source population for this study was all internally displaced reproductive-age Amhara women who were living in the North Shewa Zone of the Amhara region in Northeast Ethiopia. The study population was all internally displaced reproductive-age Amhara women who had a birth after displacement or were pregnant at the time of the study and were living in the IDP camps in North Shewa zone in the Amhara region of Ethiopia. All internally displaced reproductive age Amhara women living in IDP camps of DebreBirhan woreda in the Amhara region of Ethiopia, those IDP mothers who became pregnant and gave birth after displacement at the camp, regardless of birth outcome, and those who were pregnant at the time of data collection were included. Whereas critically ill and those women who were unable to communicate during the study, and living outside the camps, were excluded from the study.
Sample size determination and sampling procedure: The sample size was calculated using the single population proportion formula. The prevalence of ANC service utilization among IDPs in Nigeria, which was 28%, was considered since the study was conducted in the same situation as the present study.[10] With the assumption of 95% confidence interval and 5% margin of error, a design effect of 1.5 and 10% non-response rate were considered. A sample of 512 study participants was included in this study.
A multi-stage sampling technique was used to select study participants. From the 15 zones in the Amhara region, the North-Shewa zone was purposely selected. In the North Shewa zone, there were 7 Woredas that had IDP camps, and two woredas (Debre Birhan and Minjar) were selected by considering 30% of the Woredas with IDPs (due to financial and logistics issues). Minjar Woreda has one, and Debre-Birhan Woreda has six IDP camps. Finally, we selected Sefer Selam camp from Minjar Woreda and two camps (namely China and Weynshet IDP camps) in Debre-Birhan using the lottery method. There were about 6044 internally displaced women (IDW) in China, 2430 in Weynshet, and 1223 in Minjar Woreda Seferselam camp. The sample size was proportionally allocated to the size of IDW in the selected camps, and simple random sampling methods were used to select study participants in each camp.
Measurement: In this study, the outcome variables include two measures: a dichotomous variable of at least 1st visit ANC utilization (yes/no) and the frequency of ANC visits made to a health facility. The determinants were sociodemographic: age, religion, income, educational status, duration of stay in the camp, media exposure, respondent autonomy; health facility and related enabling factors: health facility distance, availability of ANC service, availability of health provider, having support from family member; obstetrics need factors: parity, previous history of complication, pregnancy wanted; and knowledge about ANC service. The composites were computed as the sum of the item responses, and the comparison to the sample mean was made. Women with higher than mean scores were classified as having good knowledge, more autonomy, or empowerment, respectively. To illustrate, autonomy was measured in terms of three decision-making indicators (healthcare, household purchases, and family visits), and empowerment was determined in terms of decision participation, ability to control resources, and ability to move freely.
In addition, concepts are defined as follows:
Antenatal care utilization: care given to pregnant mothers at least once during their latest pregnancy by health professionals with obstetric and gynecological skills (doctors, health officers, midwives, and nurses).[19]
IDP: are people forced to leave their homes due to different reasons, but remain within the borders of their own country.[1]
Knowledge on ANC: knowledge about ANC was assessed by asking 10 questions, which were: 1. ANC is a care provided by skilled health professionals during pregnancy to ensure the health condition of the mother and her baby, 2. A woman will have six to eight visits during her pregnancy, 3. A woman should receive a respectful, individualized, and woman-centered care during her pregnancy, 4. A woman can initiate her ANC visit starting from three months of her pregnancy, 5. ANC will help to prevent pregnancy-related complications in the woman and her baby, 6. ANC can help the woman to be aware of danger signs during pregnancy, 7. A woman needs the support of her husband and/or family during an ANC visit, 8. Does ANC support pregnant women in obtaining information about the place of their delivery and other postpartum services, 9. ANC can be provided for all women irrespective of their place of residence, religion, and other disparities that exist, 10. The care for pregnant women will continue after delivery. From composite variables, participants who correctly answered above the mean for knowledge assessment questions that were considered in the study are labeled as having “Good knowledge,” whereas those who answered below the mean are considered as having “Poor knowledge”.
Good knowledge: The assessment of knowledge was done through a series of 10 items listed above about maternal and newborn care. The respondents with a score above the mean were classified as those with good knowledge, whereas those with a score below the mean were classified as those with poor knowledge.
Women’s autonomy to decide: It is coded as “Yes” on the options when women have the right to participate in health service utilization to use health care; that means a woman decides alone by herself or decides jointly with her husband. On the other hand, if the woman has no role in the decision, the option will be coded as “No”; husband or someone else in the family makes the decision, in which case, she is not autonomous in decision making to utilize health services.[20,21]
Autonomy: The measure of autonomy was on the indicators of decision making, like the woman’s involvement in household purchases, healthcare decisions, and visits to relatives. Autonomy was measured as a composite score that was above the mean.
Empowerment: Empowerment was described as the empowerment of women to engage in the decision-making process in households, the ability to manage resources, and the freedom to move toward availing services. The women who scored higher than the mean on the empowerment indicators were described as empowered.
Health facility difference: Health facilities in the camp are the clinics and health posts set up in the IDP camps, and nearby health centers are those set up by the government outside the camps, but that can be accessed by the displaced people.
Data collection and its quality assurance: Data were collected using the digital Kobo Toolbox data collection scheme and an interviewer-administered questionnaire adopted from different literature and the local context of the study area, to obtain information on sociodemographic factors, obstetric history-related characteristics, health systems-related factors, and ANC service utilization.[10,22,23] Five midwives and three BSc nurses who are working in nearby health facilities were recruited. They are given adequate training on the principles of data collection and on how to complete each question, and the methods that should be applied to further clarify the questions. The data collection was supervised by the principal investigator and one Master of Public Health (MPH) student who was recruited as a supervisor.
First, the questionnaires were prepared in English and translated into Amharic and back-translated to English to maintain their consistency. The data collection template was prepared in Microsoft (MS) Excel and deployed to the Mobile Kobo Toolbox collect app. Data were uploaded using the blank form in the app by data collectors. Before actual data collection, the data collection process and data collection tool were pretested on 5% of the sample at places other than the study area (Shewa-Robit IDPs camp), and the necessary corrections were made on the tool. Detailed training was given for data collectors and supervisors by the principal investigator. Furthermore, the principal investigator and supervisor gave feedback and corrections on a daily basis. The interview was conducted in a private/safe place in the camp to ensure that the respondent felt at ease at the time of data collection.
Data processing and analysis: The data were collected by electronic capture using Kobo Toolbox. Then it was downloaded in the MS XLS form and exported to STATA V-14 for editing, cleaning, coding, and analysis. During data cleaning, missing values and outliers were checked. Descriptive statistics such as frequency distribution of study participants, percentage, mean distribution for both outcome variables, ANC service utilizers, and frequency of ANC visits are used to describe the study participants. The difference in the prevalence of ANC service utilization levels across the categories of the different covariates considered in the study was checked using a chi-square test. A multicollinearity diagnostic test was done for all independent variables before entering them into the multivariate analysis by using the variance inflation factor (VIF). Bivariate binary logistic regression was conducted, and variables with a p-value less than 0.25 were selected for multivariable analysis. In the multivariable binary logistic regression, the level of statistical significance was declared at 95% confidence interval and a p-value of ≤ 0.05, and reported with respective crude and adjusted odds ratios, and for the count outcome variable, the Poisson regression model was used. Crude and adjusted incidence rate ratios along with their 95% confidence intervals are used to calibrate the strength, direction, and significance of association. Finally, key findings of the study are portrayed using tables and graphs with adequate textual descriptions.
Results
Sociodemographic characteristics of study respondents: Most respondents were aged 25-34 years, with a majority identifying as Muslim and about two-thirds having at least a primary education. Over half of the women were unemployed, and about one-third came from households in the lowest wealth tercile (Table 1).
| Variable | Frequency | Percent (%) |
| Name of the kebele IDP camp found
Seferselam Chania Weynshet |
85 181 234 |
17.0 36.2 46.8 |
| Age
<25 25-29 30-34 35-49 |
71 186 75 168 |
14.2 37.2 15.0 33.6 |
| Place of residence (origin)
Rural Urban |
359 141 |
71.8 28.2 |
| Duration of stay in camp
≤6 months ≥6 months |
66 434 |
13.2 86.8 |
| Religion
Orthodox Muslim |
319 181 |
63.8 36.2 |
| Educational status of the mother
No formal education Primary education and above |
308 192 |
61.6 38.4 |
| Marital status
Married Unmarried |
390 110 |
78.0 22.0 |
| Husband’s educational status
No formal education Primary education and above |
168 222 |
42.9 57.1 |
| Monthly income (ETB)
<2500 2500-4000 >4000 |
383 178 39 |
56.6 35.6 7.8 |
| Knowledge about ANC
Good Poor |
236 264 |
47.2 52.8 |
| Access to media like TV, radio, and newspapers
Yes No |
73 427 |
14.6 85.4 |
Table 1: Sociodemographic characteristics of internally displaced Amhara women in North-Shewa zone camps of Amhara Region, Northern East Ethiopia, 2023 (n=500)
Knowledge about ANC Services: About half, 264 (52.8%), of the participants had good knowledge of ANC services. About 229 (45.8%) of women are aware that ANC visits should be initiated in the first three months of pregnancy, while only nearly two-fifths (39.8%) are aware that a woman should have six to eight visits (Table 2).
| Variable | Category | Frequency | % |
| ANC is provided by a health professional | Yes
No |
401
99 |
80.2
19.8 |
| A woman will have six to eight ANC visits | Yes
No |
199
301 |
39.8
60.2 |
| Women should receive respectful & individualized ANC care |
Yes
No |
367
133 |
73.4
26.6 |
| Women initiate ANC visits in the first three months | Yes
No |
229
271 |
45.8
54.2 |
| ANC helps to prevent complications in pregnancy |
Yes
No |
355
145 |
71
29 |
| ANC helps to be aware of the danger signs of pregnancy |
Yes
No |
351
149 |
70.2
29.8 |
| A woman needs support from her family during ANC visits |
Yes
No |
217
283 |
43.4
56.6 |
| ANC supports getting information on pregnancy-related issues |
Yes
No |
212
288 |
42.4
57.6 |
| ANC can be provided for all women irrespective of their religion and place of residence |
Yes
No |
369
131 |
73.8
26.2 |
| ANC continues after delivery | Yes
No |
154
346 |
30.8
69.2 |
| Frequency of the composite variable of knowledge |
Good | 236 | 47.2 |
| Poor | 264 | 52.8 |
Table 2: knowledge on ANC among internally displaced Amhara women in North-Shewa zone camps in Amhara Region, Northern East Ethiopia, 2023 (n=500)
Health facility-related characteristics: About 404 (80.8%) report that there is a health facility within their camps, and 339 (67.8%) of the study women indicated that health facilities are located within 1 km distance from their respective camps. More than four-fifths (82.4%) indicated that the camps have a referral and linkage system to higher-level health facilities. Only 73 (14.6%) of the participants have access to media (TV and radio) and newspapers. In our study, most451 (90.2%) of the study women feel safe and comfortable going to the health facilities for antenatal care services, and above half (52%) had family support to make the ANC visits (Table 3).
| Variable | Frequency | Percent (%) |
| Availability of health facilities in the camp
Yes No |
404 96 |
80.8 19.2 |
| Distance of health facility from camp: Within 1km
< 5km >5km |
339 151 10 |
67.8 30.2 2.0 |
| Availability of health professionals
Yes No |
445 55 |
89 11 |
| Feel safe and comfortable going to ANC service
Yes No |
451 49 |
90.2 9.8 |
| Having family support
Yes No |
260 240 |
52 48 |
| Autonomy to decide on maternal health services
Yes No |
341 159 |
68.2 31.8 |
| Availability of referral and linkage system
Yes No |
412 88 |
82.4 17.6 |
| Support for the admin in the referral system
Very low Low Moderate Good Very good |
51 80 250 85 34 |
10.2 16 50 17 6.9 |
Table 3: Health system-related characteristics of internally displaced women in North-Shewa zone of Amhara Region in Northern East Ethiopia, 2023 (n=500)
Obstetric-related characteristics: The majority (89.4%) were multipara, and more than half (54.4%) had pregnancy-related complications. And 333 (66.6%) of the respondents replied that their pregnancy was not wanted and planned (Table 4).
| Variable | Frequency | Percent (%) |
| Gravidity 1 >=2 |
31 469 |
6.2 93.8 |
| Parity 1 >=2 |
53 447 |
10.6 89.4 |
| Previous history of pregnancy-related complications Yes No |
272 228 |
54.4 45.6 |
| Pregnancy (wanted and planned) Yes No |
167 333 |
33.4 66.6 |
| Time of ANC initiation First trimester Second trimester Third trimester |
106 120 31 |
41.3 46.7 12.1 |
| Place of ANC received Health facility in the camp Nearby health center Nearby primary/ general hospital |
147 62 48 |
57.2 24.1 18.7 |
Table 4: Obstetric characteristics of the respondents in internally displaced Women in the North-Shewa zone camps of Amhara Region, Northeast Ethiopia, 2023 (n=500)
ANC service utilization among displaced women: Two hundred fifty-seven (51%) (95% CI: 45.1-54.1) received ANC services during pregnancy from a health facility found in the camp (Figure 1).
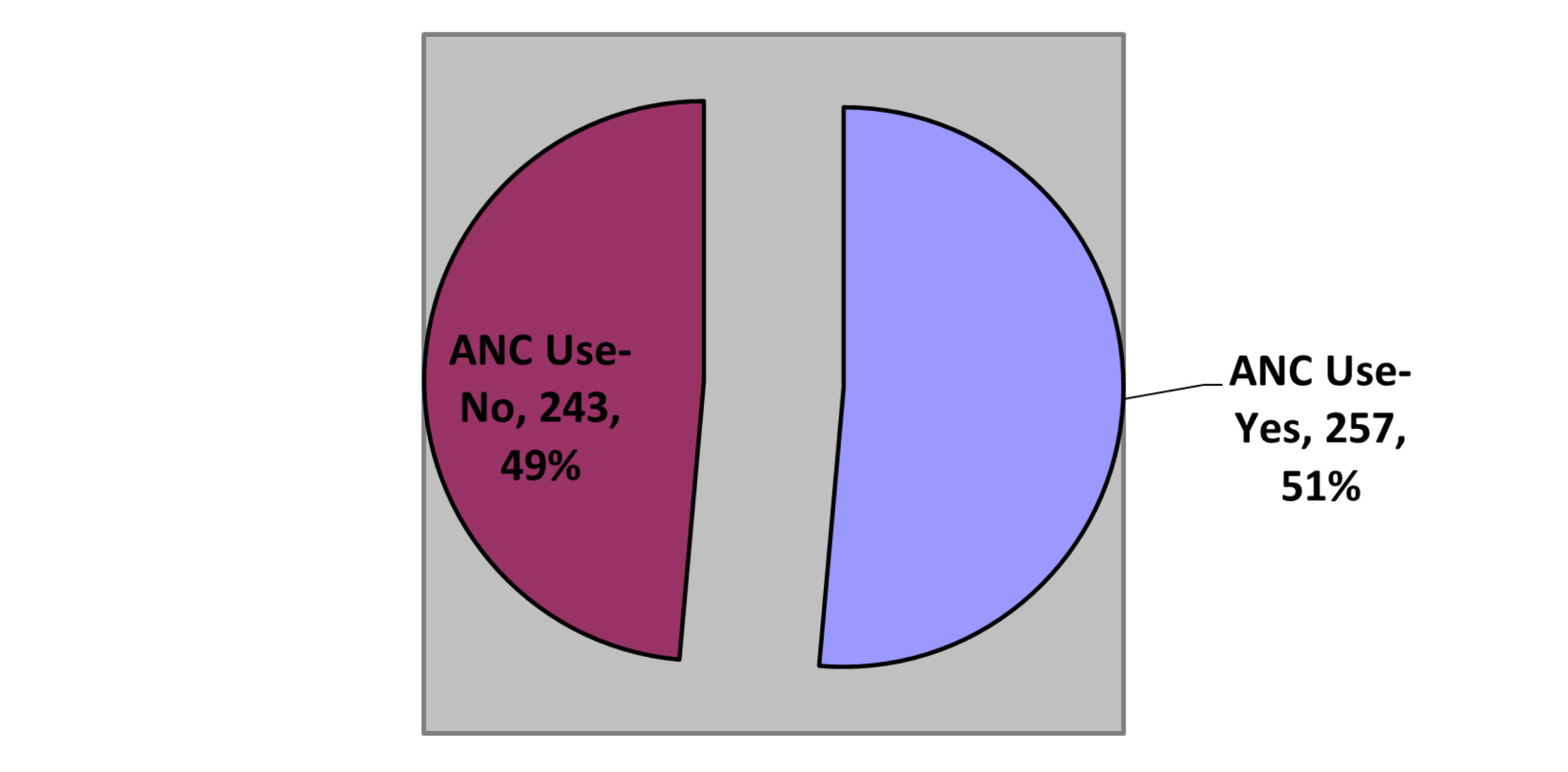
Figure 1: ANC service utilization among internally displaced Amhara women in North-Shewa zone camps of Amhara Region, Northern East Ethiopia, 2023
Number of ANC visits: The mean number of ANC visits in our study was two, with a minimum of visits 0 and a maximum of 5 visits, and a SD of 1.34. About half of the women (49%) didn’t have any visits, while nearly one fourth (23%) had two visits. Only a small proportion (5.2%) of women had the recommended number of four or more visits (Figure 2).
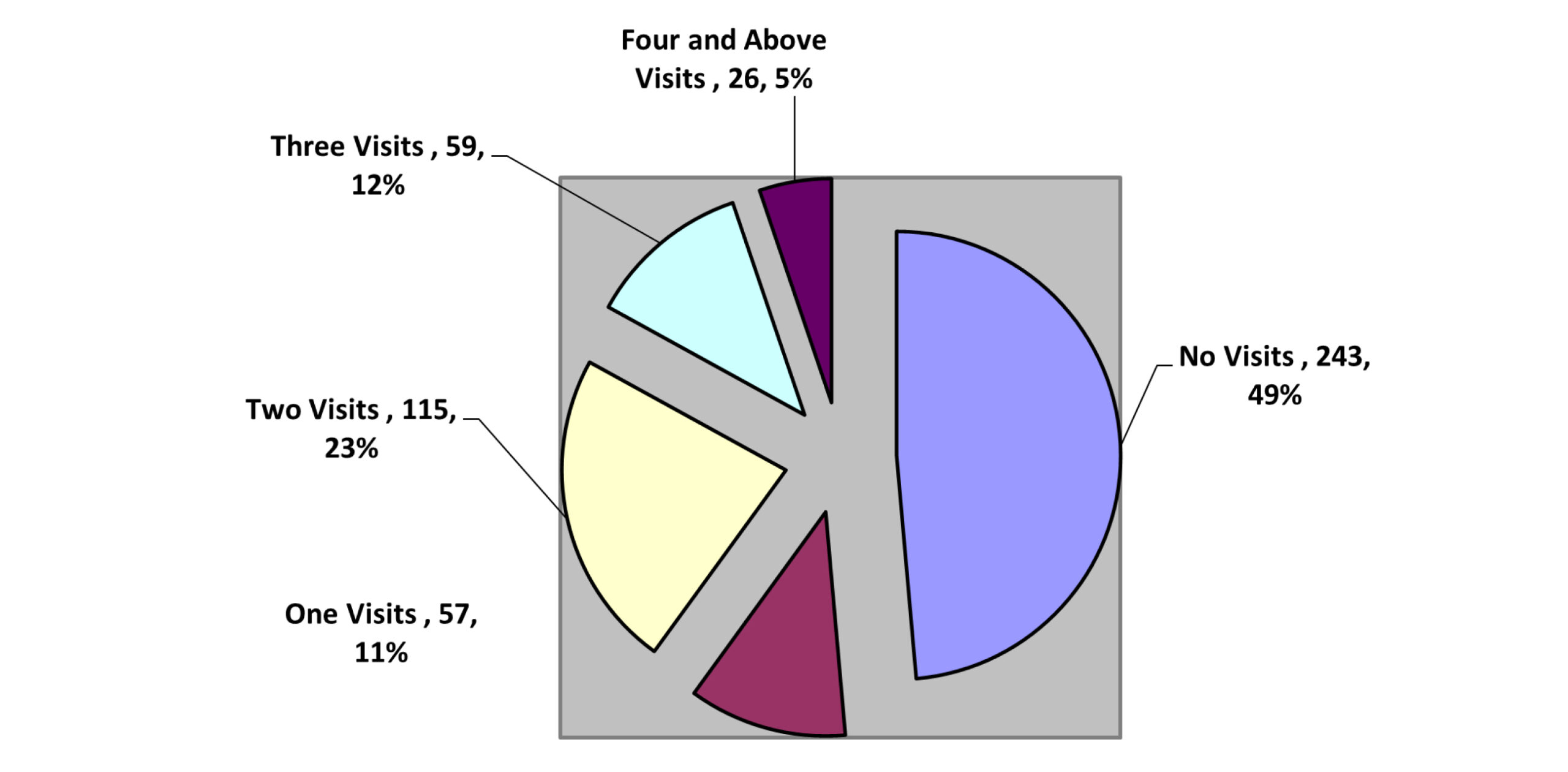
Figure 2: Number of ANC Visits among IDWs in Semen-Shewa zone, Amhara Region, Northern Ethiopia, 2023
Factors associated with at least 1st ANC visit service utilization: To identify factors, bivariate and multivariable binary logistic regression analysis was carried out for twelve explanatory variables. In multi-variable analysis (seven); educational status of the husband (AOR: 2.56, 95% CI: (1.24-5.27)), pregnancy complications (AOR: 4.09, 95% CI: (2.07-8.07)), wanted pregnancy (AOR: 8.1, 95% CI: (3.97-16.55)), distance to health facility (AOR: 4.45. 95% CI: (2.07-9.45)) and knowledge about ANC (AOR: (5.67, 95% CI: (2.93-10.99)) have significant association with ANC service utilization (Table 6).
| Variables | ANC service utilization among IDPs | |||
| Categories | Crude odds ratio (COR) (95% CI) | AOR (95% CI) | P>|z| | |
| Age of respondent | <25years | 1 | ||
| 25-29 | 0.56 (32-98) | 0.45 (0.18-1.12) | 0.86 | |
| 30-34 | 1.1 (0.57-2.12) | 1.09 (0.37-3.26) | 0.87 | |
| 35-49 | 0.84 (0.48-1.47) | 0.96 (0.37-2.51) | 0.94 | |
| Husband education | No formal education | 1 | ||
| Primary and above | 4.08 (2.66-6.24) | 2.56 (1.24-5.27) | 0.01 | |
| Educational status of the mother | No formal education | 1 | ||
| Primary and above | 2.77 (1.9-4.04) | 1.07 (0.55-2.09) | 0.83 | |
| Respondent income (ETB) | <2500 | 1 | 1 | |
| 2500-4000 | 3.00 (2.02-4.44) | 1.41 (0.71-2.79) | 0.32 | |
| >4000 | 3.43 (1.67-7.06) | 0.73 (0.21-2.34) | 0.58 | |
| Knowledge about ANC | Good | 8.49 (5.66-12.73) | 5.67 (2.93-10.99) | 0.00 |
| Poor | 1 | 1 | ||
| Distance to health facility | Within 1km | 15.4 (7.5-31.4) | 4.45 (2.07-9.45) | 0.00 |
| More than 5km | 1 | 1 | ||
| Access to TV, radio, and newspapers | Yes | 3.13 (1.798-5.46) | 1.12 (0.42- 2.99) | 0.81 |
| No | 1 | 1 | ||
| History of previous pregnancy complications | Yes | 2.7 (1.88-3.88) | 4.09 (2.07-8.07) | 0.00 |
| No | 1 | 1 | ||
| Wanted pregnancy | Yes | 11.45 (7.05-18.64) | 8.1 (3.97-16.55) | 0.00 |
| No | 1 | 1 | ||
Table 6: Bivariate and multi-variable binary logistic regression analysis output of factors associated with ANC service utilization among internally displaced Amhara women in the North-Shewa zone camps of Amhara Region 2023 (n=500)
Factors associated with the number of ANC visits: We model the number of ANC visits in Poisson regression with twelve explanatory variables. In the multi-variable analysis, four variables: availability of health facilities in the camp, women’s autonomy to decide, wanted the pregnancy, and knowledge about ANC service have a significant association with the number of ANC service utilization. The incidence of frequent ANC visits has been (AIRR:1.29, 95% CI (1.09-1.53)) times higher among internally displaced Amhara women with a good knowledge compared with those with a poor knowledge of ANC services. The study has also shown that the frequency of ANC services was (AIRR:1.75, 95% CI (91.32-2.35)) times higher among internally displaced Amhara women who have a health facility in their camp compared with those IDP women who do not have such health facilities in their camp. Moreover. IDP Amhara women who had autonomy to decide on their health care service utilization had a (AIRR: 1.30, 95% CI (1.07-1.59)) times increased incidence rate of the number of antenatal care visits compared with those who didn’t have. In addition to this, the study has revealed that IDP Amhara women who wanted their pregnancies had (AIRR: 1.27, 95% CI (1.09-1.48)) times more frequent visits to ANC services compared with those women who had a pregnancy against their will.
| Variables | Crude incidence rate ratio CIRR (95% CI) |
AIRR (95% CI) |
P>|z| |
| Age
<25 25-29 30-34 35-49 |
1.00 0.88 (0.73-1.05) 1.06 (0.86-1.31) 0.97 (0.81-1.17) |
1.00 0.90 (0.72-1.13) 0.94 (0.73-1.22) 0.93 (0.74-1.18) |
0.39 0.66 0.59 |
| Education status
No formal education Primary and above |
1.00 1.36 (1.21-1.52) |
1.00 1 (0 .89-1.20) |
0.95 |
| Husband’s Education status
No formal education Primary and above |
1.00 1.41 (1.23-1.62) |
1.00 1.1 (0 .93-1.31) |
0.25 |
| Respondent income (ETB)
<2500 2500-4000 >=4000 |
1.00 1.43 (1.27-1.62) 1.36 (1.1-1.68) |
1.00 1.02 (0 .88-1.19) 0.91 (0 .7-1.18) |
0.7
|
| Respondent autonomy to decide
Yes No |
1.99 (1.72-2.31) 1.00 |
1.30 (1.08-1.6) 1.00 |
0.01** |
| Knowledge about ANC
Good Poor |
1.72 (1.53-1.94) 1.00 |
1.29 (1.09-1.53) 1.00 |
0.00** |
| Access to TV, radio, and newspapers YesNo |
1.11 (0.95-1.31) 1.00 |
0.83 (0 .68-0.01) 1.00 |
0.07 |
| Availability of health facilities in the camp
Yes No |
2.19 (1.79-2.67) 1.00 |
1.72 (1.29-2.28) 1.00 |
0.00** |
| Distance to health facility
Within 1km More than 5km |
1.51 (1.31-1.73) 1.00 |
1.00 (0.81-1.21) 1.00 |
0.98
|
| Number of parities
<=1 >=2 |
1.00 1.02 (0.84-1.24) |
1.00 1.06 (0.78-1.44) |
0.71 |
| Previous history of pregnancy complication
Yes |
1.26 (1.12-1.42) 1.00 |
1.14 (1.98-1.32) 1.00 |
0.09 |
| Wanted pregnancy
Yes No |
1.67 (1.48-1.87) 1.00 |
1.27 (1.09-1.4) 1.00 |
0.00** |
Table 7: Poisson regression analysis output of factors associated with number of ANC visits among internally displaced Amhara women in North-Shewa zone camps in Amhara Region, Northeast Ethiopia, 2023 (n=500)
Discussion
This study identified low coverage and frequency of ANC among internally displaced people in Ethiopia. Significant factors associated with ANC service utilization included the husband’s education level, pregnancy complications, knowledge about ANC services, desired pregnancy, and distance to the health facility. Additionally, women who were empowered, had good knowledge about ANC, lived near available health facilities, and had wanted pregnancies were more likely to have a higher frequency of ANC visits.
Our study found that 51.4% of women received at least 1st ANC services during their pregnancy period from a health facility found in and out of the camps. This finding is lower than a study in the Democratic Republic of Congo (59%) and in Syria (82%).[14,16] The difference might be due to Syrian respondents being mostly refugees and not selected randomly (by convenience sampling), which might result in a higher level of service utilization. Moreover, refugees are slightly more organized and structured than IDPs as they receive foreigners and countries focus on them, and there might be socio-cultural and awareness differences among respondents. Displacement causes disruption of the services, and all actors need to be availing health facilities in the camps and ensure delivery of quality and essential services to prevent adverse pregnancy outcomes like low birth weight, preterm labor, and infant death.[24]
In our study found that husband education was positively associated with ANC service utilization, and it is in line with a study done in Lebanon and Iraq.[25] It showed that an educated husband supports his wife to visit ANC during her pregnancy period, because he has a better understanding of the importance of the visit and the consequences of missing. Having planned and wanted pregnancy and pregnancy complications were associated with the utilization of ANC services, and were consistent with other studies in Ethiopia and Nigeria.[15,24,26,27] The possible explanation for this might be that those who are in an unwanted pregnancy might have the pregnancy in a desperate situation during displacement, which could make them hopeless to take care of themselves and the unborn child. Moreover, the pregnancy could be due to violence that occurred during displacement and in the IDP camp and exposed for unwanted pregnancies and other sequels. Women who had previous complications might be informed of the consequences and frustrated and alerted for subsequent pregnancies to avoid related problems. Adequate information and education during ANC service could play a great role.
Women who reside close to the health facility were four times more likely to utilize ANC services than those who reside more than five kilometers away. This was in line with a study done in Konso, Nigeria, and other reviews.[28-30] Most IDPs were displaced in a traumatizing conflict, and they were new to the current area of residence. Therefore, they might fear walking further distances and also couldn’t afford transportation for the services. The availability of maternal health services in the camp could ease accessibility and affordability.
Women who had good knowledge of ANC services were six times more likely to utilize antenatal care services, and was consistent with other studies.[30] This might be because a woman who has good knowledge about ANC service has a better understanding of the importance of ANC services, and all actors should work aggressively on advocacy and promotion activities to raise awareness among displaced women and the need for MCH services at IDP camps. Regarding the number of visits to our study, utilization of the recommended number of ANC visits was very low. Nearly half (48.6 %) didn’t have any visits, which was higher than in Syria (17%).[31] The difference might be due to different sociodemographic characteristics of the respondents; most of the respondents in our study come from rural parts of Ethiopia, where most of them don’t attend formal education and have limited knowledge about ANC services.
In our study, finding 5.2% of women had four and above visits; this finding was lower than a study done in Nigeria (28%).[15,27] The difference might be due to sociodemographic characteristics of respondents. It implies that in the IDP setting, MCH service and awareness creation should continue the recommended number of visits.
The incidence of visits was increased by 97% for a woman who has the autonomy to decide on their utilization of health services, and was higher in a review of studies in Ethiopia (75%).[32,33] These demands empower women in seeking maternal health services and enable them to decide on their health. Similarly, the incidence of the number of visits increased by 71% for a mother who had good knowledge about ANC service and was supported by another systematic review study done in Ethiopia.[34] The possible explanation for this might be that a woman could be aware of missing ANC visits and its consequence. Educating women about ANC service plays a great role in the continuum of the recommended number of visits.
The incidence of the number of visits increased by 28% for those women who live in a camp which have health facility. This could be related to financial reasons for traveling to a distant health facility, and the availability of health facilities within the camp makes it easier for women to utilize.[35,36] The incidence of the number of visits was lower by 27% for women whose pregnancy was unwanted and unplanned, and our finding was consistent with a systematic review in Africa and other studies in Ethiopia.[37,38] This could be in most IDP camps, where women have been exposed to frequent and forced sex, as rape was used as a weapon of war by most perpetrators, and exposed women to unwanted pregnancy and STIs to make their lives miserable.[28] These displaced women need better protection and ANC and other SRH services at the camps.
Conclusion
The findings of this study showed that displacement reduced the utilization of antenatal care services among pregnant women in the study area. Knowledge about ANC, husband’s educational status, obstetric factors (pregnancy complication, wanted pregnancy), and availability of health facility in the camp were significant factors that contributed to antenatal care service utilization of pregnant women. Number of visits was also associated with all the above except husband education and pregnancy complication, but respondent autonomy was also associated with the number of visits. Thus, efforts to enhance maternal health services should be recommended. Availing health facility in IDP setting, and supporting women to various IEC (Information, Education and Communication) materials will be produced to raise awareness regarding the importance of ANC service utilization.
References
- Abass L. Assessment of knowledge and practices of internally displaced pregnant women attending to antenatal clinic center at Arbat camp in Sulaimani, Kurdistan Region of Iraq. Kurdistan J Appl Res. 2018;3(1):52-56. doi:10.24017/science.2018.1.10
Crossref | Google Scholar - Caviness MH. Visualizing Women in the Middle Ages: Sight, Spectacle, and Scopic Economy. Philadelphia, PA: University of Pennsylvania Press; 2001.
Visualizing Women in the Middle Ages: Sight, Spectacle, and Scopic Economy - Bentil S, Asekere G. Internal Conflict Displacement Galore in the Horn of Africa: Ethiopia on the Radar. Advance (Preprint). 2021. doi:10.31124/advance.16601102
Crossref | Google Scholar - Glei DA, Goldman N, Rodríguez G. Utilization of care during pregnancy in rural Guatemala: does obstetrical need matter?. Soc Sci Med. 2003;57(12):2447-2463. doi:10.1016/s0277-9536(03)00140-0
PubMed | Crossref | Google Scholar - World Health Organization. Maternal Health and Safe Motherhood Programme: progress report, 1993-1995. 1996.
Motherhood Programme: progress report, 1993-1995 - World Health Organization. WHO recommendations on antenatal care for a positive pregnancy experience. 2016.
WHO recommendations on antenatal care for a positive pregnancy experience - Youth SDG, Camp S. The 2030 Agenda for Sustainable Development’s 17 Sustainable Development Goals (SDGs). 2015.
The 2030 Agenda for Sustainable Development’s 17 Sustainable Development Goals (SDGs) - Jibirilla FM. Reproductive Health Factors and Maternal Mortality of Internally Displaced Women in Nigeria. Degree thesis. Walden University; 2021.
Reproductive Health Factors and Maternal Mortality of Internally Displaced Women in Nigeria - Amodu OC, Richter MS, Salami BO. A Scoping Review of the Health of Conflict-Induced Internally Displaced Women in Africa. Int J Environ Res Public Health. 2020;17(4):1280. doi:10.3390/ijerph17041280
PubMed | Crossref | Google Scholar - Chi PC, Bulage P, Urdal H, et al. Perceptions of the effects of armed conflict on maternal and reproductive health services and outcomes in Burundi and Northern Uganda: a qualitative study. BMC Int Health Hum Rights. 2015;15:7. doi:10.1186/s12914-015-0045-z
Crossref | Google Scholar - World Health Organization. World Health Statistics 2024: Monitoring Health for the SDGs. 2024.
World Health Statistics 2024: Monitoring Health for the SDGs - ICF Macro. Levels and Trends in the Use of Maternal Health Services in Developing Countries. 2011.
Levels and Trends in the Use of Maternal Health Services in Developing Countries - Adebangbe FT, Mturi AJ. Factors associated with the number of antenatal care visits among internally displaced women in northern Nigeria. Afr J Reprod Health. 2021;25(2):120‑130. doi:10520/ejc-ajrh_v25_n2_a12 Crossref | Google Scholar
- Harvard T.H. Chan School of Public Health, Maternal Health Task Force. Maternal health of refugees migrating from Democratic Republic of Congo to Burundi.
Maternal Health of Refugees Migrating from Democratic Republic of Congo to Burundi | MHTF Projects - Mathe M. Socio-demographic factors affecting utilization of antenatal care services in Botswana. Int J Acad Res Bus Soc Sci. 2017;7(9):222‑6990. doi:10.6007/IJARBSS/v7-i9/3343
Crossref | Google Scholar - Alibhai KM, Ziegler BR, Meddings L, et al. Factors impacting antenatal care utilization: a systematic review of 37 fragile and conflict-affected situations. Confl Health. 2022;16:33. doi:10.1186/s13031-022-00459-9
Crossref | Google Scholar - Hailemichael HT, Debelew GT, Alema HB, Weldu MG, Misgina KH. Determinants of adverse birth outcome in Tigrai region, North Ethiopia: Hospital-based case-control study. BMC Pediatr. 2020;20(1):10. doi:10.1186/s12887-019-1835-6
PubMed | Crossref | Google Scholar - Fekadu GA, Kassa GM, Berhe AK, Muche AA, Katiso NA. The effect of antenatal care on use of institutional delivery service and postnatal care in Ethiopia: a systematic review and meta-analysis. BMC Health Serv Res. 2018;18(1):577. doi:10.1186/s12913-018-3370-9
PubMed | Crossref | Google Scholar - Dagnaw FT, Tiruneh SA, Azanaw MM, Desale AT, Engdaw MT. Determinants of person-centered maternity care at the selected health facilities of Dessie town, Northeastern, Ethiopia: community-based cross-sectional study. BMC Pregnancy Childbirth. 2020;20(1):524. doi:10.1186/s12884-020-03221-2
PubMed | Crossref | Google Scholar - Eshetu K, Gelaw B, Lankrew T, Assefa A, Gebremedhin T. Women’s decision-making autonomy in maternal health service utilization and associated factors among reproductive age women in Southern Ethiopia. Res Square. 2021. doi:10.21203/rs.3.rs-521248/v2
Crossref | Google Scholar - Federal Democratic Republic of Ethiopia, Ministry of Health. Environmental and Social Management Framework (ESMF) for Additional Financing for Ethiopia COVID-19 Emergency Response Project. 2021.
Environmental and Social Management Framework (ESMF) for Additional Financing for Ethiopia COVID-19… - Shafie M, Eyasu M, Muzeyin K, Worku Y, Martín-Aragón S. Prevalence and determinants of self-medication practice among selected households in Addis Ababa community. PLoS One. 2018;13(3):e0194122. doi:10.1371/journal.pone.0194122
PubMed | Crossref | Google Scholar - Mekonnen T, Dune T, Perz J, Ogbo FA. Trends and Determinants of Antenatal Care Service Use in Ethiopia between 2000 and 2016. Int J Environ Res Public Health. 2019;16(5):748. doi:10.3390/ijerph16050748
PubMed | Crossref | Google Scholar - Tegegne TK, Chojenta C, Getachew T, Smith R, Loxton D. Antenatal care use in Ethiopia: a spatial and multilevel analysis. BMC Pregnancy Childbirth. 2019;19(1):399. doi:10.1186/s12884-019-2550-x
PubMed | Crossref | Google Scholar - Gezae KE, Berhie KA, Gebresilassie AA, Tsadik M. Contextual disparity on trend and determinants of optimal antenatal care (ANC4+) use for women in Eastern Tigray, Ethiopia: evidence from KA-HDSS database. Int J Womens Health. 2023;15:511-521. doi:10.2147/IJWH.S399956
Crossref | Google Scholar - Ali A, Dero A, Aziz S, Ali G. Factors affecting the utilization of antenatal care among pregnant women: a literature review. J Pregnancy Neonatal Med. 2018;2(2):41-45. doi:10.35841/neonatal-medicine.2.2.41-45
Crossref | Google Scholar - Devlin C. The Maternal & Child Health Status of Internally Displaced Persons in Darfur, Sudan. Master thesis. University of North Carolina at Chapel Hill; 2010.
The Maternal & Child Health Status of Internally Displaced Persons in Darfur, Sudan - Dejong J, Ghattas H, Bashour H, Mourtada R, Akik C, Reese-Masterson A. Reproductive, maternal, neonatal and child health in conflict: a case study on Syria using Countdown indicators. BMJ Glob Health. 2017;2:e000302. doi:10.1136/bmjgh-2017-000302
Crossref | Google Scholar - Mamuye Azanaw M, Gebremariam AD, Teshome Dagnaw F, et al. Factors Associated with Numbers of Antenatal Care Visits in Rural Ethiopia. J Multidiscip Healthc. 2021;14:1403-1411. doi:10.2147/JMDH.S308802
PubMed | Crossref | Google Scholar - Amiri M, El-Mowafi IM, Chahien T, Yousef H, Kobeissi LH. An overview of the sexual and reproductive health status and service delivery among Syrian refugees in Jordan, nine years since the crisis: a systematic literature review. Reprod Health. 2020;17(1):166. doi:10.1186/s12978-020-01005-7
PubMed | Crossref | Google Scholar - Petrovic K, Blank TO. The Andersen–Newman Behavioral Model of Health Service Use as a conceptual basis for understanding patient behavior within the patient–physician dyad: The influence of trust on adherence to statins in older people living with HIV and cardiovascular disease. Cogent Psychol. 2015;2(1):1038894. doi:10.1080/23311908.2015.1038894
Crossref - T Gurmesa, Tura G, Mph. Antenatal care service utilization and associated factors in Metekel Zone, Northwest Ethiopia. Ethiop J Health Sci. 2009;19(2):111-119.
Antenatal care service utilization and associated factors in Metekel Zone, Northwest Ethiopia - Abosse Z, Woldie M, Ololo S. Factors influencing antenatal care service utilization in hadiya zone. Ethiop J Health Sci. 2010;20(2):75-82. doi:10.4314/ejhs.v20i2.69432
PubMed | Crossref | Google Scholar - Reese Masterson A, Usta J, Gupta J, Ettinger AS. Assessment of reproductive health and violence against women among displaced Syrians in Lebanon. BMC Womens Health. 2014;14(1):25. doi:10.1186/1472-6874-14-25
PubMed | Crossref | Google Scholar - Gebrekirstos LG, Wube TB, Gebremedhin MH, Lake EA. Magnitude and determinants of adequate antenatal care service utilization among mothers in Southern Ethiopia. PLoS One. 2021;16(7):e0251477. doi:10.1371/journal.pone.0251477
PubMed | Crossref | Google Scholar - Oladeji O, Oladeji B, Chamla D, et al. Sexual Violence-Related Pregnancy Among Internally Displaced Women in an Internally Displaced Persons Camp in Northeast Nigeria. J Interpers Violence. 2021;36(9-10):4758-4770. doi:10.1177/0886260518792252
PubMed | Crossref | Google Scholar - Ousman SK, Mdala I, Thorsen VC, Sundby J, Magnus JH. Social Determinants of Antenatal Care Service Use in Ethiopia: Changes Over a 15-Year Span. Front Public Health. 2019;7:161. doi:10.3389/fpubh.2019.00161
PubMed | Crossref | Google Scholar - Ethiopian Public Health Institute (EPHI). Ethiopia Mini Demographic and Health Survey 2019: Final Report. 2021.
Ethiopia Mini Demographic and Health Survey 2019: Final Report
Acknowledgments
We would like to acknowledge Addis Ababa University for giving us this opportunity to conduct research. Special thanks to the Amhara region public health institute and the North-Shewa zone disaster and risk management bureau for their cooperation and support. We would like to extend our gratitude to data collectors and study participants, who are desperate for their livelihood, for their full commitment and participation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Author Information
Corresponding Author:
Hana Meseret
Department of Reproductive, Family and Population Health
Addis Ababa University, College of Health Sciences, School of Public Health, Ethiopia
Email: [email protected]
Co-Authors:
Tsegaye Shewangzaw
Department of Monitoring, Evaluation, Research and Learning
JSI Research and Training Institute, Addis Ababa, Ethiopia
Keyredin Tamirat
Department of Reproductive, Family and Population Health
Addis Ababa University, College of Health Sciences, School of Public Health, Ethiopia
Authors Contributions
All authors contributed to the conceptualization, investigation, and data curation by acquiring and critically reviewing the selected articles. They were collectively involved in the writing – original draft preparation and writing – review & editing to refine the manuscript. Additionally, all authors participated in the Supervision of the work, ensuring accuracy and completeness. The final manuscript was approved by all named authors for submission to the journal.
Ethical Approval
Ethical clearance was obtained from the research Ethics Committee of the School of Public Health, College of Health Sciences, Addis Ababa University. A formal support letter was written for the Amhara Regional and Semen Showa Zone Disaster Risk Commission and Health Bureau. The purpose and importance of the study were explained to the study participants, and data were collected after full informed verbal consent was obtained from the respondents. Confidentiality of information was maintained by excluding names as identifiers in the questionnaire, and the interview was conducted in a private place. Moreover, respondents were told that they could stop the interview and raise any questions on unclear issues at any time during the interview. Pregnant women who did not start ANC were counseled to start ANC as a benefit attached to this study after data collection.
Conflict of Interest Statement
The authors declare no conflict of interest.
Guarantor
None
DOI
Cite this Article
Meseret H, Shewangzaw T, Tamirat K. Antenatal Care Utilization and Associated Factors Among Internally Displaced Reproductive Age Women in the North Shewa Camps of Amhara Region, 2023. medtigo J Med. 2023;4(2):e3062421. doi:10.63096/medtigo3062421 Crossref













