






 Author Affiliations
Author Affiliations
Abstract
Metformin and proton pump inhibitors (PPI’s) have been postulated to have an association with vitamin B12 deficiency. In our quality improvement study, we chose to look at patients using metformin and PPI’s. Patients at higher risk also include age over 60, malabsorption disorders such as Crohn’s disease, surgical procedures such as Roux-en-Y, pernicious anemia, elevated mean corpuscular volume (MCV), vegan diets, and alcohol use. Metformin interferes with five different pathways of vitamin B12 absorption versus the PPI’s which mainly decrease HCl production, which could explain why metformin presents a greater risk of vitamin B12 deficiency. Though there are no strict designated guidelines for vitamin B12 deficiency screening, consensus agrees that screening is encouraged with long-term metformin use and is not typically recommended for long-term PPI use, but can be considered in high-risk patients and if there are symptoms of B12 deficiency. Electronic medical records can be easily accessed to evaluate patients who would qualify for screening, especially older individuals. Early detection of vitamin B12 deficiency is critical as it can lead to subacute combined degeneration, which involves the demyelination of neurons in the spinal cord, causing irreversible loss of proprioception and fine touch primarily in the lower extremities and ataxia. Treatment of vitamin B12 deficiency through oral, sublingual, and intramuscular routes is equally efficacious; however, intramuscular B12 is preferred for patients with neurological symptoms.
Keywords
Vitamin B12 deficiency, Metformin, Proton pump inhibitors, Vitamin B12 screening, Mean corpuscular volume.
Introduction
Vitamin B12 is a water-soluble vitamin that is readily obtained through meat, eggs, dairy products, and fortified foods. Vitamin B12, initially bound to food protein, enters the stomach to be cleaved by hydrochloric acid and pepsin made by parietal cells and chief cells, respectively (Figure 1). In the stomach, vitamin B12 binds to the salivary R binder. Intrinsic factor (IF) by parietal cells travels with the protein-bound vitamin B12 to the small intestine, where the higher pH facilitates hydrolysis of R protein to vitamin B12, which allows vitamin B12 to bind with IF. The new complex travels to the ilium to bind cubulin and amnionless complex, a calcium (Ca2+) dependent channel, which is then internalized by receptor-mediated endocytosis (Figure 1). IF is degraded by lysosomes, freeing up vitamin B12, which is released into the cytoplasm, traveling into the portal circulation either bound to transcobalamin to be transported to the tissue or haptocorrin to be transported to the liver. Vitamin B12 plays a key role in several metabolic pathways. It aids in the transfer of methyl groups to produce methionine for deoxyribonucleic acid (DNA) and red blood cell synthesis. Secondly, it acts as a cofactor for methylmalonyl coenzyme A (CoA) mutase, which facilitates an intermediate step in the oxidation of odd-chain fatty acids, which is vital for myelin synthesis in nerves and catabolism of ketogenic amino acids. The mechanism of metformin in vitamin B12 deficiency is not fully understood; however, there are several hypotheses. Metformin reduces adenosine triphosphate (ATP) production in the mitochondria, which increases adenosine monophosphate (AMP) signaling, leading to increased insulin sensitivity, promotion of glycolytic pathways, and inhibition of gluconeogenesis. It is postulated to inhibit the Ca2+ influenced binding of IF-vitamin B12 to the cubulin- amnionless receptor complex in the ilium (Figure 1). PPIs block gastric hydrogen/potassium adenosine triphosphatase (H+/K+ATPase), which pumps out H+ ions in gastric parietal cells into the lumen to combine with chloride ions (Cl-) to form hydrochloric acid (HCl). When H+ ions are blocked from the lumen, the lumen pH decreases, reducing digestive capacity. Vitamin B12 in foods is released, which leads to a significant decrease in protein-bound vitamin B12.[1]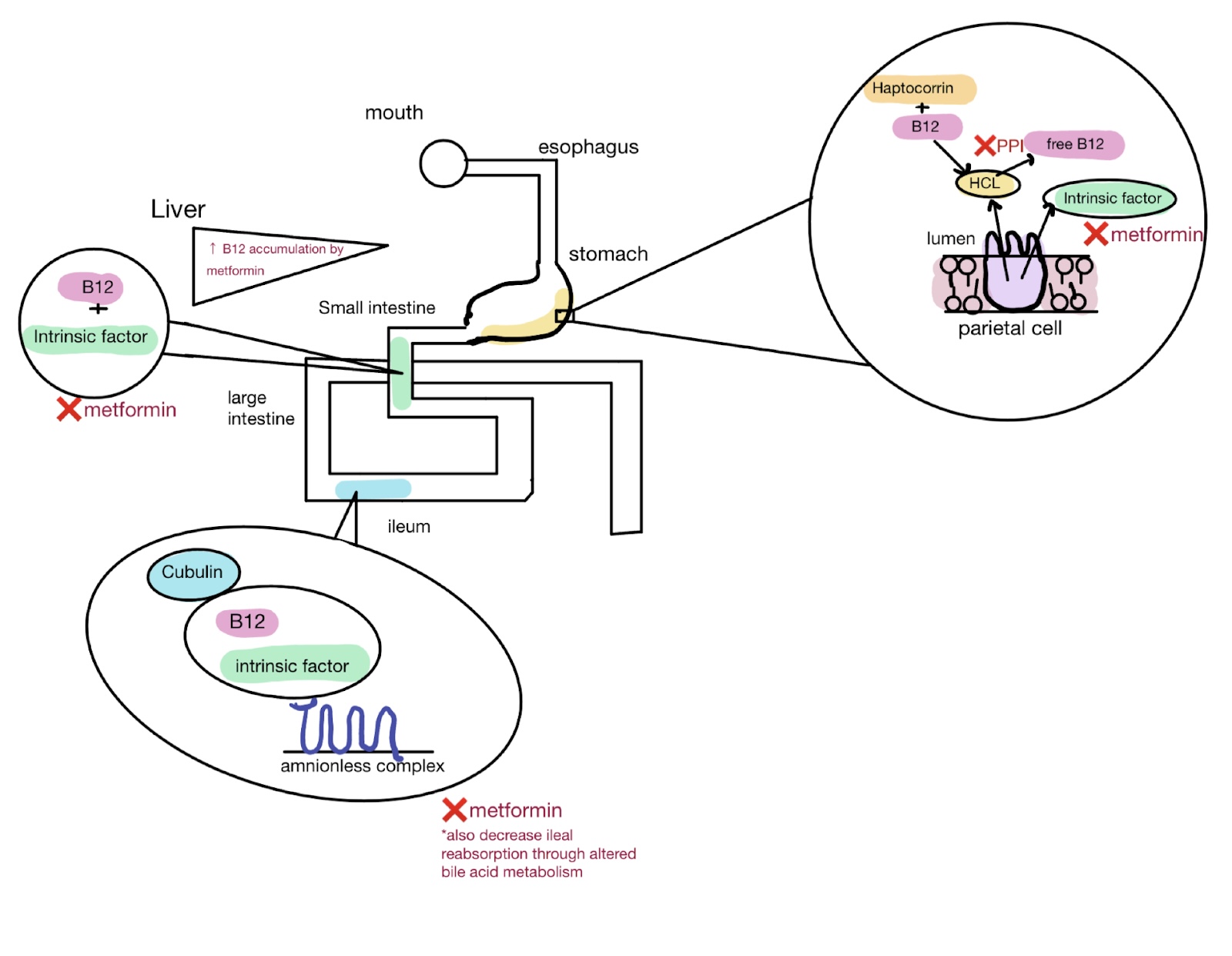
Figure 1: Processing and absorption of vitamin B12
Vitamin B12 starts by binding R protein or haptocorrin in the mouth, which travels to the stomach to get hydrolyzed by HCl from parietal cells. Parietal cells also secrete IF, which binds vitamin B12 in the small intestine. B12 is then absorbed in the ilium by the cubulin amnionless receptor complex and is transported to the liver by haptocorrin and transcobalamin to tissues. Metformin decreases IF, bile acid metabolism for ileal reabsorption, binding of vitamin B12 and IF in the small intestine, decreases cubulin-B12-IF complex binding to amnionless complex, and increases vitamin B12 accumulation in the liver.[2] PPI’s decrease H secretion to form hydrochloric acid in the stomach; therefore, less vitamin B12 is freed up and is usable.
Methodology
Our study originally began as a quality project to look into vitamin B12 monitoring for patients. We decided to start by searching a panel of patients on higher-risk medications. We chose metformin and PPI. After institutional review board (IRB) approval, we used our Epic electronic medical record’s slicer-dicer tool. We chose a panel of patients on metformin or PPI and checked if a vitamin B12 level was drawn in the prior three years. After further review of the literature, we narrowed this number down by choosing to look only at patients over 75 on a PPI, since general screening of all PPI patients is not recommended. At that point, we reviewed each patient’s chart for other risk factors such as macrocytosis, being on both medications, etc. We also reviewed whether they had a vitamin B12 level in other medical record systems. We reached out to those at highest risk primarily via their patient portal. If they had upcoming visits, we ordered a vitamin B12 level with the other labs appropriate for their visit and asked the staff to request the patients to obtain those labs roughly a week before their upcoming visit.
Results
Out of a sample population of 1126, 195 were regularly prescribed a PPI and 89 were on metformin. Seventeen patients were on both medications. The dosages per day for the PPI’s and metformin ranged from 10-40 mg and 500-2000 mg respectively; also, a vitamin B12 was ordered for 62 patients on PPI and 32 on metformin. Patients were notified of the lab order and were requested to have blood drawn at their convenience. Because this was a quality improvement study, there have only been 10 results that have come back so far. All have been in the lower normal range, which may be why there are no concrete recommendations to screen all patients on PPIs. None of our patients have obtained the four-test panel yet for confirmation, though that may be our next step.
Discussion
Starting as early as the 1960, research has consistently suggested a clinical association with long-term metformin use (>4.3 years) and vitamin B12 deficiency, with an associated increased risk over time of 13% per year and an overall increased risk of 41%.[3,4] One study has shown that out of 13,489 long-term metformin users, 44.9% were tested for vitamin B12 deficiency, where 3.3% were shown to be deficient.[5] Older populations (50-59 years and >80 years) were also identified to have a 2.4-fold risk of not being tested.[6] This highlights the potential issue of a lack of surveillance and treatment among metformin users. Consequences of untreated vitamin B12 deficiency among metformin users include a statistically significant increase in peripheral neuropathy with an odds ratio of 1.65, compounded by the increase in methylmalonic acid (MMA), along with jaundice and macrocytic anemia.[7,8] It is also crucial to pay attention to other symptoms of vitamin B12 deficiency that would be observable during a physical exam: glossitis, diarrhea, headaches, and neuropsychiatric disturbances.[9]
The question is: who gets screened, and what are the guidelines? The American Geriatrics Society, British Society for Haematology, American Diabetes Association, Agency for Healthcare Research and Quality, and American Family Physicians do not recommend global screening, but there are some recommendations for older patients with increased risk factors. Increased risk factors include concurrent PPI use of >12 months with metformin use of >4 months, malabsorptive disorders, lack of IF, such as pernicious anemia, transcobalamin II deficiency, vegan diet, comorbid conditions, and alcohol abuse.[9] Suspected vitamin B12 deficiency should be followed up with vitamin B12 levels (<150 pg/mL for deficiency) and a complete blood count (CBC). Though clinicians should be aware of false elevations such as alcohol use, liver disease, and cancer.[8] A four-test panel, including homocysteine, MMA, vitamin B12, and holotranscobalamin (HoloTC), as well as antibody tests such as Anti-Intrinsic Factor and Anti-Parietal Cell, can confirm vitamin B12 deficiency and investigate the underlying cause, especially for those at risk for false normal vitamin B12 levels. The American Diabetes Association recommends that those >65 years old using metformin for 3-5 years with risk factors (prediabetes, peripheral neuropathy, or anemia) should be screened for vitamin B12 deficiency with a grade B level of evidence.[7]
American Family Physicians recommended screening for B12 deficiency for patients at risk, with a B12 level and CBC, with a grade C level of evidence.[8] Most studies agree that metformin use is time and dose-dependent. For example, a study showed fold increased risk of vitamin B12 deficiency in the elderly >65 years old and had a rate of 4.2% vs 2.5% in younger patients and each 100 mg dose increase in metformin increased the risk of vitamin B12 deficiency by 8% and overall risk was increased with a metformin dose of >2000 mg.[7] In our study, we screened for vitamin B12 deficiency for all ages on metformin. The goal is to screen for vitamin B12 deficiency in patients at risk as a part of secondary prevention to improve care.
Similar to metformin, it has been postulated that chronic use of 3-5 years of PPI can contribute to vitamin B12 deficiency, though absolute changes were noted to be small.[1] Additionally, distributors of omeprazole and lansoprazole are not aware of any cases of cobalamin deficiency or megaloblastic anemia.[10] Most studies agree that patients at risk of vitamin B12 deficiency are >60 years and/or with nutritional issues or concurrent metformin use.[1,11] The American Gastroenterology Association (AGA) indicates that screening/monitoring for vitamin B12 deficiency with chronic use of PPI is not recommended due to a lack of evidence of proven benefit, but can be considered.[11] However, AGA does admit chronic use of PPI’s is associated with a 2-4-fold increase in vitamin B12 deficiency. Therefore, older patients at risk, according to most studies, should be monitored for vitamin B12 periodically.[1,12,13] To encompass the older population, our study observed patients >75 years. Again, our goal is to provide early detection of vitamin B12 deficiency to decrease morbidity and healthcare costs.
Interestingly, most studies agree that using PPI along with metformin increases risk of vitamin B12 deficiency.[3] In our study, out of 94 patients who had a vitamin B12 level drawn, 17 patients were on both PPI and metformin. Two out of nine patients had a high MCV that was on metformin only, and three out of nine had an elevated MCV that was on PPI only. Though it is important to note that other underlying pathologies might not be due to the medication, but rather from environmental sources such as alcoholism. Two patients on metformin and three patients on a PPI had an elevated MCV; two of those patients were on both metformin and PPI. These patients would benefit from additional testing to confirm vitamin B12 deficiency using HoloTC (bioactive protein-bound form), homocysteine, and MMA. Elevated levels of homocysteine and MMA and low levels of HoloTC confirm vitamin B12 deficiency (Figure 2).[7]
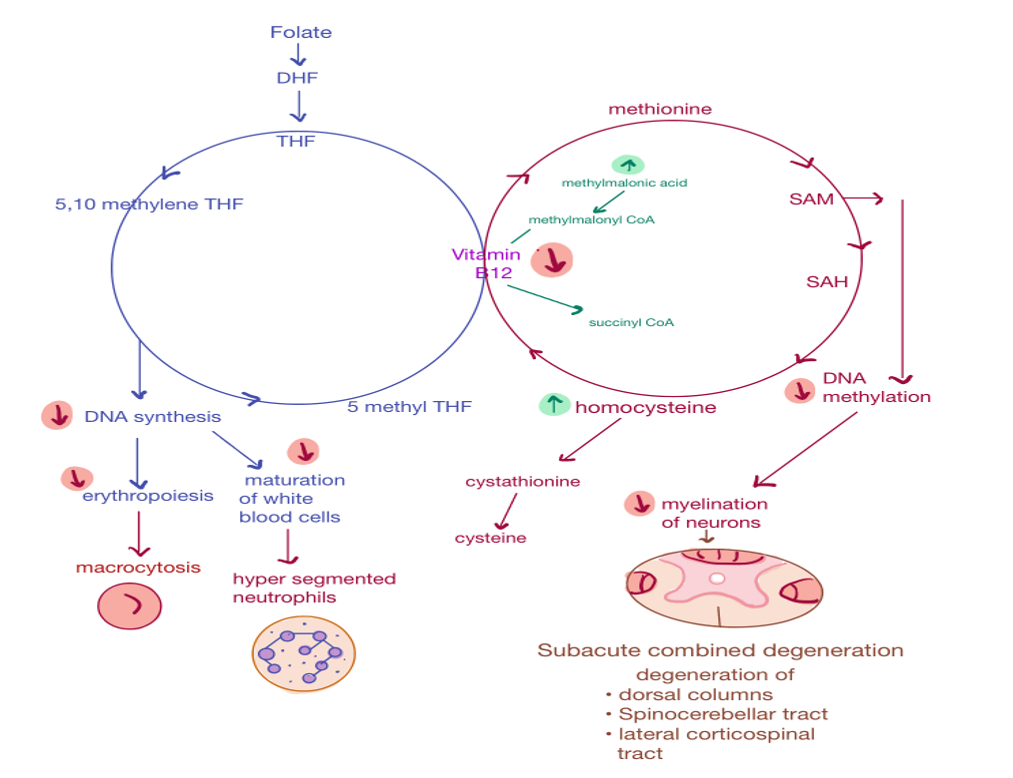
Figure 2: Folate and methionine cycle
Vitamin B12 deficiency leads to a decrease in S-adenosylmethionine (SAM), which decreases DNA methylation and myelination of neurons. This leads to demyelination in the dorsal columns, spinocerebellar tract, and lateral corticospinal tract, leading to Subacute Combined Degeneration. Decrease in DNA synthesis leads to abnormal erythropoiesis, resulting in macrocytosis and hypersegmentation of neutrophils.
It should be noted that homocysteine and MMA can be elevated in folate deficiency, though MMA is typically normal; a folate level can be ordered to differentiate (Figure 2). Both MMA and homocysteine can also be elevated in renal impairment.[7] Once vitamin B12 deficiency is diagnosed, oral, sublingual, or IM 1000-2000 mcg of vitamin B12 administration is appropriate. About 0.5-4% of oral vitamin B12 is absorbed; therefore, a dose of 1000 mcg will deliver 5-40 mcg of vitamin B12, which meets the recommended daily intake.[7] Oral calcium supplementation has also been shown to reverse vitamin B12 malabsorption caused by metformin.[7] All three methods of administration have fairly equal efficacy, though intramuscular (IM) administration is typically preferred in patients with problems with malabsorption and neurological symptoms.[14] One may ask: Why screen for vitamin B12 when we can just give patients routine supplementation? Currently, there is no standardized vitamin B12 treatment with the exception of patients with gastric bypasses. However, the active form of vitamin B12 (methylcobalamin) is more bioavailable than the synthetic form (cyanocobalamin).[15] The synthetic form of B12 should be used with caution in patients with renal impairment due to possible accumulation of aluminum, used in the preparation of synthetic vitamin B12.[15] Hydroxocobalamin is another alternative offered as an injection with a longer half-life and is safe for patients with renal impairment. As we have discussed previously, many factors can cause vitamin B12 deficiency, and vitamin B12 deficiency can present with a variety of signs and symptoms.[9] First, we want to confirm that vitamin B12 deficiency is in fact the cause of the presenting symptoms, and we want to find out the overall cause of the vitamin B12 deficiency, such as a malabsorptive disorder or pernicious anemia.[8] Both would require vitamin B12 supplementation, but the management of these conditions may differ.[16]
Conclusion
It is reasonable to conclude that while there are no aggressive guidelines recommending vitamin B12 screening for all metformin or PPI use, clinically it can be useful for certain higher-risk populations such as patients >65 years old, use of metformin with PPI’s, elevated MCV, malabsorption disorders, symptoms of neuropathy, or alcohol use. Getting a vitamin B12 level allows for targeted treatment, prevention of misdiagnosis, and treatment delays in diseases unrelated to vitamin B12.[16] Additional panel testing can help identify causes of vitamin B12 deficiency to aid in disease management. Electronic medical records can be easily used to assist in identifying at-risk populations to improve care delivery.
References
- Mumtaz H, Ghafoor B, Saghir H, et al. Association of Vitamin B12 deficiency with long-term PPIs use: A cohort study. Ann Med Surg (Lond). 2022;82:104762. doi:10.1016/j.amsu.2022.104762
PubMed | Crossref | Google Scholar - Miller JW. Proton Pump Inhibitors, H2-Receptor Antagonists, Metformin, and Vitamin B-12 Deficiency: Clinical Implications. Adv Nutr. 2018;9(4):511S-518S. doi:10.1093/advances/nmy023
PubMed | Crossref | Google Scholar - Aroda VR, Edelstein SL, Goldberg RB, et al. Long-term Metformin Use and Vitamin B12 Deficiency in the Diabetes Prevention Program Outcomes Study. J Clin Endocrinol Metab. 2016;101(4):1754-1761. doi:10.1210/jc.2015-3754
PubMed | Crossref | Google Scholar - Hurley-Kim K, Vu CH, Dao NM, et al. Effect of Metformin Use on Vitamin B12 Deficiency Over Time (EMBER): A Real-World Evidence Database Study. Endocr Pract. 2023;29(11):862-867. doi:10.1016/j.eprac.2023.06.013
PubMed | Crossref | Google Scholar - Martin D, Thaker J, Shreve M, Lamerato L, Budzynska K. Assessment of vitamin B12 deficiency and B12 screening trends for patients on metformin: a retrospective cohort case review. BMJ Nutr Prev Health. 2021;4(1):30-35. doi:10.1136/bmjnph-2020-000193
PubMed | Crossref | Google Scholar - Kancherla V, Elliott JL Jr, Patel BB, et al. Long-term Metformin Therapy and Monitoring for Vitamin B12 Deficiency Among Older Veterans. J Am Geriatr Soc. 2017;65(5):1061-1066. doi:10.1111/jgs.14761
PubMed | Crossref | Google Scholar - Infante M, Leoni M, Caprio M, Fabbri A. Long-term metformin therapy and vitamin B12 deficiency: An association to bear in mind. World J Diabetes. 2021;12(7):916-931. doi:10.4239/wjd.v12.i7.916
PubMed | Crossref | Google Scholar - Langan RC, Goodbred AJ. Vitamin B12 Deficiency: Recognition and Management. Am Fam Physician. 2017;96(6):384-389.
Vitamin B12 Deficiency: Recognition and Management - Ankar A, Kumar A. Vitamin B12 Deficiency. eBook. StatPearls Publishing; 2024.
Vitamin B12 Deficiency - Richter JE. Should patients receiving long-term gastric acid inhibition therapy be evaluated for vitamin B12 deficiency?. Cleve Clin J Med. 2000;67(11):785-787. doi:10.3949/ccjm.67.11.785
PubMed | Crossref | Google Scholar - Freedberg DE, Kim LS, Yang YX. The Risks and Benefits of Long-term Use of Proton Pump Inhibitors: Expert Review and Best Practice Advice From the American Gastroenterological Association. Gastroenterology. 2017;152(4):706-715. doi:10.1053/j.gastro.2017.01.031
PubMed | Crossref | Google Scholar - Dharmarajan TS, Kanagala MR, Murakonda P, Lebelt AS, Norkus EP. Do acid-lowering agents affect vitamin B12 status in older adults?. J Am Med Dir Assoc. 2008;9(3):162-167. doi:10.1016/j.jamda.2007.10.004
PubMed | Crossref | Google Scholar - Dougherty TR, Sekaran A, Borum M. Chronic proton pump inhibitor use is not associated with vitamin B12 deficiency: 132. The American Journal of Gastroenterology. 2013;108:S42.
Chronic Proton Pump Inhibitor Use Is Not Associated with Vitamin B12 Deficiency: 132 - Wang H, Li L, Qin LL, Song Y, Vidal-Alaball J, Liu TH. Oral vitamin B12 versus intramuscular vitamin B12 for vitamin B12 deficiency. Cochrane Database Syst Rev. 2018;3(3):CD004655. doi:10.1002/14651858.CD004655.pub3
PubMed | Crossref | Google Scholar - Paul C, Brady DM. Comparative Bioavailability and Utilization of Particular Forms of B12 Supplements With Potential to Mitigate B12-related Genetic Polymorphisms. Integr Med (Encinitas). 2017;16(1):42-49.
Comparative Bioavailability and Utilization of Particular Forms of B12 Supplements With Potential to Mitigate B12-related Genetic Polymorphisms - UCSF Health. Vitamin B12 Level. 2024.
Vitamin B12 Level
Acknowledgments
We would like to thank medtigo for peer review and publication, and the patients, faculty, and staff at St. Joseph’s Hospital in Syracuse, NY.
Funding
No funding
Author Information
Corresponding Author:
Lauren Whitney
Department of Medicine
Medical Student, University of New England, USA
Email: [email protected]
Co-Author:
Stephen Hoag
Department of Family Medicine
Associate Professor, Upstate Medical University, New York
Family Medicine Program Director, St. Joseph’s Hospital, United States
Authors Contributions
Author Whitney was primarily responsible for the abstract, introduction, discussion, conclusion, and preparation of diagrams. Author Hoag was primarily responsible for the study concept, development of the data collection methodology, data analysis, and follow-up with participating patients regarding their overall care. Both authors contributed to the conceptualization, investigation, and data curation by acquiring and critically reviewing the selected articles. They participated in writing the original draft and in reviewing and editing the manuscript to refine its content. Additionally, both authors supervised the work to ensure accuracy and completeness. The final manuscript was reviewed and approved by both authors for submission to the journal.
Ethical Approval
This study (IRB# 25-0624-3) was reviewed by the IRB of St. Joseph’s Health/St. Peter’s Health Partners (SJH/SPHP) on June 25, 2025. The IRB determined that the proposed activity does not meet the definition of human subjects’ research, and therefore, IRB review and approval were not required.
Conflict of Interest Statement
The authors declare no conflicts of interest.
Guarantor
Authors Whitney and Hoag are responsible for the integrity of the work.
DOI
Cite this Article
Whitney L, Hoag S. Analysis of Vitamin B12 Levels in Metformin and PPI Use for Quality Improvement. medtigo J Pharmacol. 2025;2(3):e3061236. doi:10.63096/medtigo3061236 Crossref













