






 Author Affiliations
Author Affiliations
Abstract
The treatment of patients with atrophic ridges, who need functional and esthetic rehabilitation, is a common problem encountered in our daily practice as oral surgeons, which prevents ideal implant placement. Alveolar ridge splitting is a minimally invasive surgical technique that expands the alveolar bone, particularly in the maxilla, which has inherent flexibility properties, to create an optimal site for dental implant placement. This technique improves the quantity and quality of bone around the implant in both crestal and apical directions. It is indicated for the alveolar ridge with adequate height and minimal width, enabling direct implant placement with reduced morbidity and overall treatment time compared to other augmentation techniques. The technique was introduced in the 1970s by Dr. Hilt Tatum, with later refinement in 1994 by Summers, who advocated the use of osteotomes. This case report describes a maxillary ridge splitting procedure for a missing left central incisor, involving simultaneous implant placement and a 24-month follow-up.
Introduction
Dental implants are now the treatment of choice for edentulous ridges; however, insufficient bone width can compromise this outcome. Several surgical techniques for horizontal augmentation have been described in the literature, including guided bone regeneration, block bone grafting, the ridge split technique, ridge expansion, and distraction osteogenesis.[1-13] These techniques are used with some limitations to enhance the bone volume in the case of a narrow alveolar ridge.[14,15] While the GBR procedure can be performed with simultaneous implant placement, only grafting implies a reconsolidation time of at least three months to enable implant placement in a staged procedure.[16-19] Many studies have demonstrated the success of these well-documented surgical approaches. Still, donor site morbidity, unexpected bone resorption, block consolidation at the site of grafting, and infection are among the drawbacks of these conventional techniques.[20,21]
The technique of ridge split, or ridge expansion, was introduced in the early 1970s for horizontal ridge augmentation while maintaining periosteal attachment by carefully expanding the cortical plates. This approach was further developed by Summers (1994), who advocated the use of osteotomes to progressively increase the diameter and create an osteotomy bed for implant placement. This technique had the added advantage of augmentation and implant placement in a single sitting. Ridge-splitting techniques are useful for managing narrow edentulous ridges (˂3.5 mm) for implant placement, yielding a predictable outcome in the maxilla more often than in the mandible.[22]
Proper case selection and evaluation are important to achieving a successful surgical and prosthetic outcome. Another advantage in our case was the use of a piezoelectric device to ensure atraumatic bone separation, thereby decreasing the risk of bone fracture due to expansion; this makes the bone more elastic.[23-26]
Case Presentation
A 19-year-old female patient presented with a missing maxillary left central incisor (tooth number 21); the medical history was noncontributory. The width of the alveolar crest was 3.1mm, which could not allow for any implant insertion (Figure 1 and 2).

Figure 1 and 2: Photo showing the volume loss in the buccal side and cross-sectional image measuring the bucco-lingual thickening of residual bone
Case Management
The split technique was employed to facilitate the suitable positioning of the osseous implant. A crestal and intra-sulcular incision was performed extending from the distal aspect of the maxillary right canine to the maxillary left canine, with an additional releasing incision on the distal aspect of the left canine.
A mucoperiosteal flap was raised, then crestal osteotomy preparation was performed with an ultrasonic piezo device using an insert that cuts the bone into two parts, buccal 2.1mm and 1mm palatal. Supplementary mesial and distal osteotomies were added to ensure easy bone separation. Immediate implant site preparation, aimed at maintaining the expanded space, was performed using a Lindemann burr and bone expander kit (Figure 3-6).
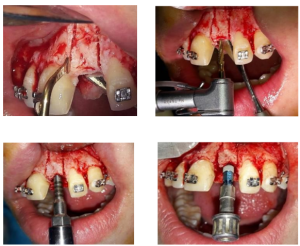
Figure 3-6: Buccal osteotomy using piezo surgery- Lindemann burr preparing implant bed- Bone expander creating more space- Implant placement
A Straumann bone level tapered (BLT) implant with a 3.3 mm diameter and 11 mm length, classified as a rock-solid type of dental implant, was then placed (Figure 7 and 8).
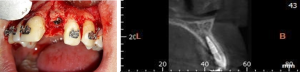
Figure 7 and 8: Final implant position and CBCT control image two years later
Discussion
Generally, after tooth extraction, an average 40–60% decrease of horizontal as well as vertical dimensions of the alveolar ridge occurs during the first 2 years.[27] Bone resorption and three-dimensional changes of the crest are predominantly more pronounced at the buccal than on the lingual aspect of the extraction socket.[28] The aim of this case report was to demonstrate a successful clinical implant installation in a patient with a 3.1 mm alveolar width, utilizing the splitting technique.
Different splitting modifications have been documented in the literature, such as the two-stage technique specifically designed for the mandible, or how to address the gap created between the two cortices. In our case, a simultaneous implant installation was the solution to preserve the space created in only one intervention and avoid bone graft harvesting from secondary donor sites.[29,30]
However, ridge expansion also discloses certain technical and physiological limitations. One major drawback of alveolar bone splitting is the requirement of a trabecular bone compartment between the buccal and lingual plates to allow separation.
Jensen et al. indirectly demonstrate the rare usage of the ridge splitting technique in the lower jaw compared to the upper, mainly due to the rigidity of the mandibular cortical bone.[31]
Another disadvantage of the alveolar bone splitting technique, which can be quite severe, is the risk of bone resorption due to malnutrition of the laterally displaced buccal bone wall.[27] Although some approaches have been proposed to reduce bone resorption, evidence for their efficacy remains lacking.[32,33]
Conclusion
In conclusion, the most important factors for successful ridge split cases are careful patient selection and thorough bone evaluation. Although this surgical approach can be used in both jaws, it is more suitable for the maxilla. Thus, to achieve the ideal goals of implant dentistry, augmentation of deficient alveolar ridges is a crucial aspect of dental implant therapy, with the ultimate goal of providing a functional restoration that is in harmony with the adjacent natural dentition, as in this case report.
References
- Chen ST, Wilson TG Jr, Hämmerle CH. Immediate or early placement of implants following tooth extraction: review of biologic basis, clinical procedures, and outcomes. Int J Oral Maxillofac Implants. 2004;19 Suppl:12-25. Immediate or early placement of implants following tooth extraction: review of biologic basis, clinical procedures, and outcomes
- Kim YK, Ku JK. Guided bone regeneration. J Korean Assoc Oral Maxillofac Surg. 2020;46(5):361-366. doi:10.5125/jkaoms.2020.46.5.361 PubMed | Crossref | Google Scholar
- Tang YL, Yuan J, Song YL, Ma W, Chao X, Li DH. Ridge expansion alone or in combination with guided bone regeneration to facilitate implant placement in narrow alveolar ridges: a retrospective study. Clin Oral Implants Res. 2015;26(2):204-211. doi:10.1111/clr.12317 PubMed | Crossref | Google Scholar
- Ma G, Wu C, Shao M. Simultaneous implant placement with autogenous onlay bone grafts: a systematic review and meta-analysis. Int J Implant Dent. 2021;7(1):61. Published 2021 Apr 30. doi:10.1186/s40729-021-00311-4 PubMed | Crossref | Google Scholar
- Pikos MA. Block autografts for localized ridge augmentation: Part II. The posterior mandible. Implant Dent. 2000;9(1):67-75. doi:10.1097/00008505-200009010-00012 PubMed | Crossref | Google Scholar
- Cordaro L, Amadé DS, Cordaro M. Clinical results of alveolar ridge augmentation with mandibular block bone grafts in partially edentulous patients prior to implant placement. Clin Oral Implants Res. 2002;13(1):103-111. doi:10.1034/j.1600-0501.2002.130113.x PubMed | Crossref | Google Scholar
- Coatoam GW, Mariotti A. The segmental ridge-split procedure. J Periodontol. 2003;74(5):757-770. doi:10.1902/jop.2003.74.5.757 PubMed | Crossref | Google Scholar
- Mestas G, Alarcón M, Chambrone L. Long-Term Survival Rates of Titanium Implants Placed in Expanded Alveolar Ridges Using Split Crest Procedures: A Systematic Review. Int J Oral Maxillofac Implants. 2016;31(3):591-599. doi:10.11607/jomi.4453 PubMed | Crossref | Google Scholar
- Beolchini M, Lang NP, Viganò P, Bengazi F, Triana BG, Botticelli D. The edentulous ridge expansion (ERE) technique an experimental study in the dog. Clin Oral Implants Res. 2014;25(10):1207-1211. doi:10.1111/clr.12263 PubMed | Crossref | Google Scholar
- Scipioni A, Bruschi GB, Calesini G, Bruschi E, De Martino C. Bone regeneration in the edentulous ridge expansion technique: histologic and ultrastructural study of 20 clinical cases. Int J Periodontics Restorative Dent. 1999;19(3):269-277. Bone regeneration in the edentulous ridge expansion technique: histologic and ultrastructural study of 20 clinical cases
- Sethi A, Kaus T. Maxillary ridge expansion with simultaneous implant placement: 5-year results of an ongoing clinical study. Int J Oral Maxillofac Implants. 2000;15(4):491-499. Maxillary ridge expansion with simultaneous implant placement: 5-year results of an ongoing clinical study
- Takahashi T, Funaki K, Shintani H, Haruoka T. Use of horizontal alveolar distraction osteogenesis for implant placement in a narrow alveolar ridge: a case report. Int J Oral Maxillofac Implants. 2004;19(2):291-294. Use of horizontal alveolar distraction osteogenesis for implant placement in a narrow alveolar ridge: a case report
- Laster Z, Rachmiel A, Jensen OT. Alveolar width distraction osteogenesis for early implant placement (published correction appears in J Oral Maxillofac Surg. 2006 Mar;64(3):566). J Oral Maxillofac Surg. 2005;63(12):1724-1730. doi:10.1016/j.joms.2005.09.001 PubMed | Crossref | Google Scholar
- Donos N, Mardas N, Chadha V. Clinical outcomes of implants following lateral bone augmentation: systematic assessment of available options (barrier membranes, bone grafts, split osteotomy). J Clin Periodontol. 2008;35(8 Suppl):173-202. doi:10.1111/j.1600-051X.2008.01269.x PubMed | Crossref | Google Scholar
- Cordaro L, Amadé DS, Cordaro M. Clinical results of alveolar ridge augmentation with mandibular block bone grafts in partially edentulous patients prior to implant placement. Clin Oral Implants Res. 2002;13(1):103-111. doi:10.1034/j.1600-0501.2002.130113.x PubMed | Crossref | Google Scholar
- Aghaloo TL, Moy PK. Which hard tissue augmentation techniques are the most successful in furnishing bony support for implant placement? Int J Oral Maxillofac Implants. 2007;22 Suppl:49-70. Which hard tissue augmentation techniques are the most successful in furnishing bony support for implant placement?
- Zitzmann NU, Schärer P, Marinello CP. Long-term results of implants treated with guided bone regeneration: a 5-year prospective study. Int J Oral Maxillofac Implants. 2001;16(3):355-366. Long-term results of implants treated with guided bone regeneration: a 5-year prospective study
- McAllister BS, Haghighat K. Bone augmentation techniques. J Periodontol. 2007;78(3):377-396. doi:10.1902/jop.2007.060048 PubMed | Crossref | Google Scholar
- Buser D, Dula K, Hirt HP, Schenk RK. Lateral ridge augmentation using autografts and barrier membranes: a clinical study with 40 partially edentulous patients. J Oral Maxillofac Surg. 1996;54(4):420-433. doi:10.1016/s0278-2391(96)90113-5 PubMed | Crossref | Google Scholar
- Machtei EE. The effect of membrane exposure on the outcome of regenerative procedures in humans: a meta-analysis. J Periodontol. 2001;72(4):512-516. doi:10.1902/jop.2001.72.4.512 PubMed | Crossref | Google Scholar
- Chiapasco M, Zaniboni M, Boisco M. Augmentation procedures for the rehabilitation of deficient edentulous ridges with oral implants. Clin Oral Implants Res. 2006;17 Suppl 2:136-159. doi:10.1111/j.1600-0501.2006.01357.x PubMed | Crossref | Google Scholar
- Summers RB. The osteotome technique: Part 4–Future site development. Compend Contin Educ Dent. 1995;16(11):1090-1099. The osteotome technique: Part 4–Future site development
- Rahnama M, Czupkałło L, Czajkowski L, Grasza J, Wallner J. The use of piezosurgery as an alternative method of minimally invasive surgery in the authors’ experience. Wideochir Inne Tech Maloinwazyjne. 2013;8(4):321-326. doi:10.5114/wiitm.2011.35144 PubMed | Crossref | Google Scholar
- Moro A, Gasparini G, Foresta E, et al. Alveolar Ridge Split Technique Using Piezosurgery with Specially Designed Tips. Biomed Res Int. 2017;2017:4530378. doi:10.1155/2017/4530378 PubMed | Crossref | Google Scholar
- Labanca M, Azzola F, Vinci R, Rodella LF. Piezoelectric surgery: twenty years of use. Br J Oral Maxillofac Surg. 2008;46(4):265-269. doi:10.1016/j.bjoms.2007.12.007 PubMed | Crossref | Google Scholar
- Happe A. Use of a piezoelectric surgical device to harvest bone grafts from the mandibular ramus: report of 40 cases. Int J Periodontics Restorative Dent. 2007;27(3):241-249. Use of a piezoelectric surgical device to harvest bone grafts from the mandibular ramus: report of 40 cases
- Johnson K. A study of the dimensional changes occurring in the maxilla following tooth extraction. Aust Dent J. 1969;14(4):241-244. doi:10.1111/j.1834-7819.1969.tb06001.x PubMed | Crossref | Google Scholar
- Araújo MG, Lindhe J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J Clin Periodontol. 2005;32(2):212-218. doi:10.1111/j.1600-051X.2005.00642.x PubMed | Crossref | Google Scholar
- Demarosi F, Leghissa GC, Sardella A, Lodi G, Carrassi A. Localised maxillary ridge expansion with simultaneous implant placement: a case series. Br J Oral Maxillofac Surg. 2009;47(7):535-540. doi:10.1016/j.bjoms.2008.11.012 PubMed | Crossref | Google Scholar
- Sethi A, Kaus T. Maxillary ridge expansion with simultaneous implant placement: 5-year results of an ongoing clinical study. Int J Oral Maxillofac Implants. 2000;15(4):491-499. Maxillary ridge expansion with simultaneous implant placement: 5-year results of an ongoing clinical study
- Jensen OT, Cullum DR, Baer D. Marginal bone stability using 3 different flap approaches for alveolar split expansion for dental implants: a 1-year clinical study. J Oral Maxillofac Surg. 2009;67(9):1921-1930. doi:10.1016/j.joms.2009.04.017 PubMed | Crossref | Google Scholar
- Scipioni A, Bruschi GB, Giargia M, Berglundh T, Lindhe J. Healing at implants with and without primary bone contact. An experimental study in dogs. Clin Oral Implants Res. 1997;8(1):39-47. doi:10.1111/j.1600-0501.1997.tb00006.x PubMed | Crossref | Google Scholar
- Basa S, Varol A, Turker N. Alternative bone expansion technique for immediate placement of implants in the edentulous posterior mandibular ridge: a clinical report. Int J Oral Maxillofac Implants. 2004;19(4):554-558. Alternative bone expansion technique for immediate placement of implants in the edentulous posterior mandibular ridge: a clinical report
Acknowledgments
My first gratitude goes to the surgery department and the faculty of dental medicine at the Lebanese University for providing me with this opportunity. I would also like to thank Dr. Charbel Choubaya and Dr. Jean Nassar for their valuable contributions. Finally, I am deeply grateful to my wife for her continuous support and love.
Funding
No funding was received to conduct this case report.
Author Information
Corresponding Author:
Jean Saade
Department of Surgery
Faculty of Dental Medicine, Lebanese University
Email: jean.saadeh1@hotmail.com
Co-Authors:
Jean Nassar
Department of Periodontology
Faculty of Dental Medecine, Lebanese University
Charbel Choubaya
Department of Surgery
Faculty of Dental Medicine, Lebanese University
Authors Contributions
All authors worked collaboratively to complete the manuscript. Photographs used in the paper were sourced from clinical cases provided by Dr. Charbel Choubaya. The accompanying case descriptions were written by Dr. Jean Saade and were subsequently revised and referenced by Dr. Jean Nassar.
Informed Consent
Informed consent was received from the patient.
Conflict of Interest Statement
The authors declare no conflicts of interest.
Guarantor
This article received no specific grant from any funding agency in the public, commercial, or profit sectors.
DOI
Cite this Article
Saade J, Nassar J, Choubaya C. Alveolar Split Procedure: Advancing Precision in Dental Surgery. medtigo J Med. 2025;3(2):e30623223. doi:10.63096/medtigo30623223 Crossref













