






 Author Affiliations
Author Affiliations
Abstract
Background: Laparoscopic cholecystectomy has become the gold standard for gallbladder removal due to its minimally invasive nature. Many patients also present with coexisting conditions requiring simultaneous surgical management. These may include obesity, GI and hepatobiliary diseases, hernias, gynaecological and renal disorders & among others.
Methodology: We studied 31 patients who underwent laparoscopic cholecystectomy combined with a second surgical procedure in the same session, between July 2016 and January 2025. Follow-ups were completed in most cases. The primary procedure was either simple or complex laparoscopic cholecystectomy, combined with additional surgeries such as mucosectomy, subtotal cholecystectomy, endoscopic retrograde cholangiopancreatography (ERCP), common bile duct (CBD), stenting/exploration, bariatric procedures, hernia repair, hysterectomy (Total laparoscopic hysterectomy (TLH)\Vaginal hysterectomy (VH)), ovarian surgery, cystocele/rectocele repair, tubal ligation/vasectomy, transurethral resection of the prostate (TURP), percutaneous nephrolithotomy (PCNL), perianal procedures, and benign breast surgeries. We prioritized combining clean or clean-contaminated procedures to reduce operative risk and improve recovery.
Result & Conclusion: All patients had favourable outcomes. A few developed controlled bile leaks, managed successfully with ERCP and CBD stenting, and were not considered complications. Postoperative pain was minimal, hospital stay averaged 2–3 days, with 2–3 follow-up visits. No complications were linked to the additional procedures, and no long-term issues were reported.
Keywords
Endoscopic retrograde cholangiopancreatography, Common bile duct, Laparoscopic subtotal cholecystectomy, Mucosectomy, Calculus cholecystitis, Minimally invasive surgery, Complex or complicated cholecystectomy, Combined procedures.
Introduction
Laparoscopic cholecystectomy, either simple or complex, has become the gold standard technique over open cholecystectomy in recent years, owing to its minimally invasive nature. Often, patients present with coexisting pathologies that require equal surgical attention. In such cases, after evaluating the patient’s general condition, comorbidities, and overall surgical safety, it is feasible to perform an additional procedure during the same session. These may include subtotal cholecystectomy, mucosectomy, CBD exploration, bariatric surgery, hernia repair with meshplasty (open/ Total extra peritoneal (TEP)/ Transabdominal preperitoneal (TAPP)), hysterectomy (TLH/VH), ovarian cyst removal, cystocele or rectocele repair, family planning procedures, renal stone management (PCNL, prostatectomy, TURP), perianal procedures for fissure or haemorrhoids, and benign breast surgeries. Preoperative evaluation is crucial and should include specific pathological and radiological investigations tailored to the patient’s associated condition.[1-3]
This study aimed to evaluate the safety, feasibility, and outcomes of performing laparoscopic cholecystectomy in combination with a second elective surgical procedure during the same operative session. Given the increasing prevalence of patients presenting with coexisting conditions such as obesity, gastrointestinal and hepatobiliary disorders, hernias, gynaecological and renal diseases, this study investigates whether combining procedures can minimize surgical burden, reduce hospital stay, and promote faster recovery without increasing complication rates.
Methodology
We prefer the three-port technique with the patient in the supine position, combined with head-up and left tilt positioning for laparoscopic cholecystectomy. However, depending on the nature and requirements of the additional procedure, the patient’s position may be adjusted to supine, prone, lateral, reverse Trendelenburg, lithotomy, or extended lithotomy as appropriate.
Technique: Following necessary preoperative haematological and radiological investigations, along with thorough evaluation of the patient’s general condition and cardiac status, informed written and video consent is obtained from the patient and their attendant.
The patient is initially placed in the supine position for intubation. Nasogastric tube insertion is generally avoided as gastric decompression is not typically required. A 10 mm camera port is inserted at the supraumbilical position, and carbon dioxide (CO₂) insufflation is initiated, maintaining an intra-abdominal pressure of 10–12 mm Hg with a flow rate of 4–6 liters per minute. Under direct vision via the camera port, a 10 mm working port is introduced in the epigastric region, and a 5 mm working port is placed in the right midclavicular line, maintaining an approximate 60-degree angle between all three ports (Figure 1).
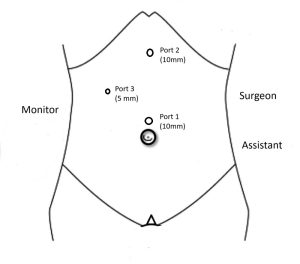
Figure 1: Port position for cholecystectomy
Following full insufflation, the patient is placed in a head-up, left-tilted position to facilitate exposure. All abdominal quadrants are assessed to identify any associated pathology or trocar entry-related injury. Using the left-hand instrument (3rd port), the fundus of the gallbladder is identified and grasped with assistance from the right-hand instrument (2nd port). The hepatobiliary anatomy is evaluated, including the presence of adhesions, oedema, and gallbladder wall thickness. Upon completion of simple or complex laparoscopic cholecystectomy, a transversus abdominis plane (TAP) block is administered to optimize postoperative pain control and minimize the need for additional analgesia. If a second procedure is planned, the patient’s position is adjusted accordingly. This may include repositioning to supine, prone, lateral, reverse Trendelenburg, lithotomy, or extended procedures; additional ports may be inserted as necessary. Examples are shown in Figures 2 to 5, which include gynaecological surgery (Figure 2), bariatric procedures (Figure 3), appendectomy (Figure 4), and TEP hernia repair (Figure 5). For open procedures, additional ports are typically not required. At the end of the procedure, all ports are closed in two layers, and sterile, waterproof dressings are applied.
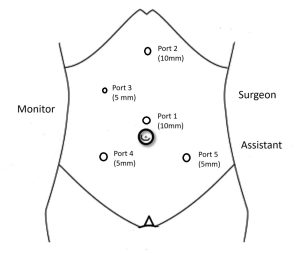
Figure 2: Port position for gynaecological surgery

Figure 3: Port position for bariatric procedure
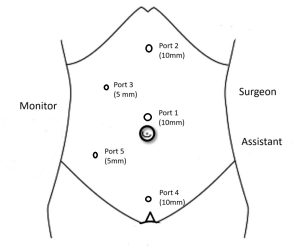
Figure 4: Port position for appendix surgery
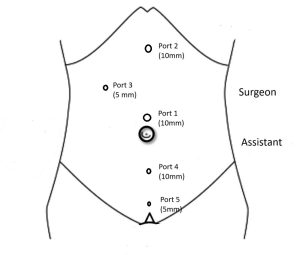
Figure 5: Port position for hernia (TEP) surgery
In applicable cases, ERCP with CBD stone removal and stenting is performed by a gastroenterologist either immediately after the cholecystectomy or preoperatively, based on the clinical scenario. This approach facilitates the safe and efficient performance of a second surgical procedure in the same session, even after a complex cholecystectomy, particularly when combining two clean surgeries.
Benefits: This combined surgical approach offers several benefits to the patient. It eliminates the need for additional hospital admission, repeated exposure to anaesthesia, relief from dual postoperative pain, and the costs associated with two separate procedures, including medications, investigations, and hospital charges. Even after undergoing dual procedures in a single session, patients are typically able to tolerate oral intake within 4–6 hours postoperatively, remain ambulatory, and experience minimal discomfort. Most patients can be safely discharged by the 2nd postoperative day with follow-up planned under oral medications and antibiotics. This strategy not only reduces overall hospital stay and associated expenses but also helps prevent hospital-acquired infections and promotes early recovery from both conditions addressed during surgery.[4-6]
Results
| Parameter | Findings | Discussion |
| Study period | July 2016 – January 2025 | The study was conducted over 8.5 years, offering both short and long-term outcomes for combined procedures. |
| Sample size | 31 patients | A modest sample, but adequate to demonstrate trends in dual surgical procedures. |
| Age distribution | 27–78 years
(Mean: 46.29 years) |
The majority were middle-aged, indicating the typical demographic for gallbladder and associated pathologies. |
| Body mass index (BMI) | 23.78–48.65
(Mean: 35.84) |
Most patients were overweight or obese; 87% had a BMI >30, which may influence comorbidities and surgical decisions. |
| BMI distribution | ||
| Less than 25 | 1 | 3.22% |
| 25-30 | 3 | 9.67% |
| 30-35 | 11 | 35.48% |
| 35-40 | 10 | 32.25% |
| Above 40 | 6 | 19.35% |
| Gender distribution | Male: 12.9% Female: 87.1% |
Predominantly female, consistent with higher incidence of gallbladder diseases and gynaecological conditions. |
| Education level | Undergraduate: 32.25% Graduate: 45.16% Postgraduate: 22.58% |
A well-educated cohort aids in informed consent and postoperative compliance. |
| Ethnicity | Hindu: 87.09%
Muslim: 12.90% |
A large group of Hindus has more complications due to their complicated lifestyle. |
| Pain duration before diagnosis | >120 days: 45.16% | Chronicity of symptoms highlights delayed presentation, which is common in gallbladder and hernia cases. |
| Pain duration before diagnosis | ||
| 0-30 days onset | 9 | 29.03% |
| 30-60 days onset | 2 | 6.45% |
| 60-90 days onset | 3 | 9.67% |
| 90-120 days onset | 3 | 9.67% |
| 120-150 days onset | 14 | 45.16% |
| Preoperative imaging | Ultrasound: 100% USG + MRCP/CT: 6.44% |
Ultrasound was the baseline modality; advanced imaging was used selectively. |
| Prevalence of coexisting conditions | Hernia: 35.48% Gynaecological: 67.75% Renal: 6.45% Obesity: 9.67% |
The majority of patients had additional surgical conditions, justifying a dual procedure approach. |
| Preoperative hernia duration | ||
| 0-12 months onset | 1 | 3.22% |
| 12-24 months onset | 2 | 6.45% |
| 24-36 months onset | 3 | 9.67% |
| 36-48 months onset | 5 | 16.12% |
| No hernia noted | 20 | 64.51% |
| Preoperative gynaecological complaints | ||
| 0-12 months onset | 4 | 12.90% |
| 12-24 months onset | 2 | 6.45% |
| 24-36 months onset | 7 | 22.58% |
| 36-48 months onset | 8 | 25.80% |
| No gynaecological complaints noted | 10 | 32.25% |
| Preoperative renal complaints | ||
| 24-36 months onset | 1 | 3.22% |
| 36-48 months onset | 1 | 3.22% |
| No renal complaints noted | 29 | 93.54% |
| Preoperative obesity | ||
| More than 48 Months Onset | 3 | 9.67% |
| No weight-related complaints noted | 28 | 90.32% |
| Port usage | 3 ports: 70.96% 4–5 ports: 29.04% |
Most cases used minimal port techniques, with additional ports added as needed. |
| Surgical approach | Total Laparoscopic: 22.58% Hybrid: 77.41% |
The hybrid approach allowed flexibility and safety during complex multi-organ surgeries. |
| Mesh sizes for hernia repair | 6×11 cm: 33.3% 15×15 cm: 22.2% 30×30 cm: 44.4% |
Mesh size was tailored based on hernia type and defect size. Use of a large size of hernia mesh indicates the complexity of the hernia & its defect size. |
| Anaesthesia | General Anaesthesia (GA): 100% | Standardized GA ensured a controlled environment for multi-procedure sessions. |
| Postoperative pain | Mild-Moderate: 41.93% Moderate-Severe: 58.06% |
Pain levels were acceptable and managed postoperatively with TAP blocks and analgesics. |
| Drain use | Hepatobiliary: 32.26% Hernia: 22.59% Renal: 3.22% Bariatric: 0% |
Drains were selectively placed, mostly in hepatobiliary procedures. |
| Drain kept for hepatobiliary procedures | ||
| 0-7 days | 1 | 3.22% |
| 8-14 days | 2 | 6.45% |
| 15-21 days | 4 | 12.90% |
| 22-28 days | 3 | 9.67% |
| Not require | 21 | 67.74% |
| Drain kept for hernia procedures | ||
| 0-7 days | 0 | 0.00% |
| 8-14 days | 1 | 3.22% |
| 15-21 days | 6 | 19.35% |
| 22-28 days | 0 | 0.00% |
| Not require | 24 | 77.41% |
| Drain kept for renal procedures | ||
| 0-7 days | 1 | 3.22% |
| Not require | 30 | 96.77% |
| Drain kept for bariatric procedures | ||
| Not kept | 0 | 0.00% |
| Not require | 31 | 100.00% |
| Complications | Wound gapping: 3.22% Re exploration: 3.22% Seroma: 0% |
Complication rates were minimal, with only one patient requiring re-exploration who had a wound gapping. |
| Scar outcome | Acceptable: 100% | Cosmetic results were excellent, affirming laparoscopic and minimal access benefits. |
| Hernia recurrence | None reported | Indicates effective meshplasty and surgical technique. |
| Hospital stays | 1 day: 12.9% 2 day: 25.80%3 day61.29%2-3 days: 87.1%(Average: 2.48 days) |
Short hospital stays support the safety and efficiency of combining procedures. |
| Common combined procedures | Hepatobiliary + Gynaecological: 64.51% Hepatobiliary + Hernia: 29.03%Hepatobiliary + Renal: 3.22%Hepatobiliary + Bariatric: 3.22% |
Dual surgeries allowed the resolution of multiple conditions in one admission. |
| Common combined procedures | ||
| Hepatobiliary (Open & Laparoscopic): Laparoscopic cholecystectomy, laparoscopic subtotal cholecystectomy, mucosectomy, ERCP, CBD Stenting, CBD exploration |
31 | 100.00% |
| Gynaecological (Open & Laparoscopic): Vaginal hysterectomy, total laparoscopic hysterectomy, ovarian cyst excision, tubal ligation, AP repair |
20 | 64.51% |
| General (Open & Laparoscopic): Umbilical hernia, inguinal hernia, incisional hernia, meshplasty, abdominoplasty, umbilical reposition |
9 | 29.03% |
| Renal (Open & Laparoscopic): PCNL |
1 | 3.22% |
| Weight loss: Laparoscopic sleeve gastrectomy |
1 | 3.22% |
Table 1: Summary of findings and surgical details for combined procedures (n=31)
Chi-square analysis: Two Chi-square tests were conducted to assess whether there was a statistically significant association between the type of cholecystectomy (simple v/s complex):
- Whether ERCP and CBD stenting were performed.
- Whether associated surgical procedures were performed in the same session.
Association between cholecystectomy type and ERCP/CBD stenting:
| ERCP & CBD stenting: Yes | ERCP & CBD stenting: No | Total | |
| Simple cholecystectomy | 12 | 10 | 22 |
| Complex cholecystectomy | 7 | 2 | 9 |
| Total | 19 | 12 | 31 |
Table 2: Association between cholecystectomy type and ERCP/CBD stenting
| Yes (Expected) | No (Expected) | |
| Simple cholecystectomy | 13.48 | 8.52 |
| Complex cholecystectomy | 5.52 | 3.48 |
Table 3: Chi-square test calculation
Chi-square value (χ²) = 0.727
Degrees of freedom = (2 – 1) × (2 – 1) = 1
p-value ≈ 0.394 → Not statistically significant at p < 0.05
Interpretation: There is no statistically significant association between the complexity of cholecystectomy and the performance of ERCP with CBD stenting. Thus, ERCP/CBD stenting appears to be independent of cholecystectomy type.
Association between cholecystectomy type and additional surgical procedures:
| Associated surgical procedures: Yes | Associated surgical procedures: No | Total | |
| Simple cholecystectomy | 10 | 1 | 11 |
| Complex cholecystectomy | 18 | 2 | 20 |
| Total | 28 | 3 | 31 |
Table 4: Association between cholecystectomy type and additional surgical procedures
| Yes (Expected) | No (Expected) | |
| Simple cholecystectomy | 9.94 | 1.06 |
| Complex cholecystectomy | 18.06 | 1.94 |
Table 5: Chi-square test calculation
Chi-square value (χ²) = 0.012
Degrees of freedom = (2 – 1) × (2 – 1) = 1
p-value ≈ 0.94 → Not statistically significant at p < 0.05
Interpretation: There is no statistically significant association between the type of cholecystectomy and the performance of additional surgical procedures during the same session.
| Test compared | Chi-square value (X2) | p-value | Significance (p<0.05) |
| Cholecystectomy type (ERCP & CBD stenting) | 0.727 | 0.394 | No |
| Cholecystectomy type (Associated procedures) | 0.012 | 0.913 | No |
Table 6: Summary of both tables
Interpretation of statistical findings: The results of both Chi-square tests indicate that
- The complexity of the cholecystectomy (simple v/s complex) does not significantly influence the decision to perform ERCP/CBD stenting.
- Similarly, the decision to perform additional surgical procedures during the same session is not significantly associated with the type of cholecystectomy performed.
These findings suggest that both ERCP/CBD stenting and associated procedures were selected based on independent clinical indications, rather than being dictated by the complexity of the gallbladder surgery itself.
Discussion
The findings from this study support the feasibility and safety of performing simultaneous laparoscopic cholecystectomy with an additional elective procedure in appropriately selected patients. The majority of the cohort consisted of middle-aged, obese female patients, reflecting a demographic commonly afflicted with both gallbladder pathology and gynaecological conditions. Notably, the use of 3-port laparoscopic techniques in over 70% of cases underscores the potential for maintaining a minimally invasive approach even when multiple procedures are undertaken during the same operative session. Despite the increased procedural complexity, there were no major complications, no long-term adverse outcomes, and no hernia recurrences. All patients achieved satisfactory cosmetic results, reinforcing the procedural benefits of this hybrid surgical model.
Effective postoperative pain control was achieved using TAP blocks, coupled with enhanced recovery protocols such as early mobilization and oral intake initiated within 4–6 hours postoperatively. These strategies contributed to a mean hospital stay of just 2.48 days, indicating a smooth and expedited recovery process for most patients. In addition to clinical outcomes, the study highlights several logistical and economic advantages. This combined surgical approach reduces cumulative anaesthesia exposure, eliminates the need for multiple hospital admissions, and streamlines patient management, a particularly valuable strategy in resource-constrained settings or for patients requiring multi-system surgical interventions.[7-10]
Conclusion
This study demonstrates that simultaneous laparoscopic cholecystectomy with an additional surgical procedure in a single operative session is both safe and effective when performed on appropriately selected patients. The majority of patients were middle-aged, obese females, many of whom presented with coexisting pathologies such as hernias, gynaecological conditions, or obesity related issues. With a mean operative hospital stay of just 2.48 days, minimal postoperative complications, and excellent cosmetic outcomes, the combined surgical approach significantly reduces the need for multiple hospital admissions, anaesthesia exposures, and postoperative recoveries. The use of a hybrid surgical approach and careful intraoperative planning enabled optimal surgical outcomes, with no reported long-term complications or hernia recurrences.
Furthermore, the approach is cost-effective, decreases patient morbidity, and enhances recovery while maintaining surgical safety and efficacy. This dual procedure strategy may be especially valuable in resource-limited settings, offering comprehensive care in a single session without compromising patient outcomes.
In conclusion, performing dual or multi-organ surgeries in a single operative session, centered around laparoscopic cholecystectomy, is a viable and patient-friendly approach that aligns with modern surgical principles of minimally invasive, cost-effective, and outcome-oriented care.
References
- Lucocq J, Hamilton D, Scollay J, Patil P. Subtotal Cholecystectomy Results in High Peri-operative Morbidity and Its Risk-Profile Should be Emphasised During Consent. World J Surg. 2022;46(12):2955-2962. doi:10.1007/s00268-022-06737-0 PubMed | Crossref | Google Scholar
- Ben Hmida W, Jerraya H, Nasseh S, Haloui N, Khalfallah M, Nouira R. The complications of subtotal cholecystectomy: A case report. Int J Surg Case Rep. 2021;83:105950. doi:10.1016/j.ijscr.2021.105950 PubMed | Crossref | Google Scholar
- Jara G, Rosciano J, Barrios W, et al. Laparoscopic subtotal cholecystectomy: a surgical alternative to reduce complications in complex cases. Cir Esp. 2017;95(8):465-470. doi:10.1016/j.ciresp.2017.07.013 PubMed | Crossref | Google Scholar
- Strasberg SM, Pucci MJ, Brunt LM, Deziel DJ. Subtotal Cholecystectomy-“Fenestrating” vs “Reconstituting” Subtypes and the Prevention of Bile Duct Injury: Definition of the Optimal Procedure in Difficult Operative Conditions. J Am Coll Surg. 2016;222(1):89-96. doi:10.1016/j.jamcollsurg.2015.09.019 PubMed | Crossref | Google Scholar
- Lunevicius R. Laparoscopic subtotal cholecystectomy: a classification, which encompasses the variants, technical modalities, and extent of resection of the gallbladder. Ann R Coll Surg Engl. 2020;102(4):315-317. doi:10.1308/rcsann.2020.0007 PubMed | Crossref | Google Scholar
- Ie M, Katsura M, Kanda Y, Kato T, Sunagawa K, Mototake H. Laparoscopic subtotal cholecystectomy after percutaneous transhepatic gallbladder drainage for grade II or III acute cholecystitis. BMC Surg. 2021;21(1):386. doi:10.1186/s12893-021-01387-w PubMed | Crossref | Google Scholar
- Elshaer M, Gravante G, Thomas K, Sorge R, Al-Hamali S, Ebdewi H. Subtotal Cholecystectomy for “Difficult Gallbladders”: Systematic Review and Meta-analysis. JAMA Surg. 2015;150(2):159–168. doi:10.1001/jamasurg.2014.1219 PubMed | Crossref | Google Scholar
- Savita K, Khedkar I, Bhartia VK. Combined procedures with laparoscopic cholecystectomy. Indian J Surg. 2010;72(5):377-380. doi:10.1007/s12262-010-0117-1 PubMed | Crossref | Google Scholar
- Baillie J, Testoni PA. Same-day laparoscopic cholecystectomy and ERCP for choledocholithiasis. Gastrointest Endosc. 2016;84(4):646-648. doi:10.1016/j.gie.2016.05.008 PubMed | Crossref | Google Scholar
- Muhammedoğlu B, Kale IT. Comparison of the safety and efficacy of single-stage endoscopic retrograde cholangiopancreatography plus laparoscopic cholecystectomy versus two-stage ERCP followed by laparoscopic cholecystectomy six-to-eight weeks later: A randomized controlled trial. Int J Surg. 2020;76:37-44. doi:10.1016/j.ijsu.2020.02.021 PubMed | Crossref | Google Scholar
Acknowledgments
Not Reported
Funding
None
Author Information
Corresponding Author:
Jitenkumar H Panchal
Department of General Surgery
Narayan Medical College & Hospital, Jamuhar, Bihar, India
Email: [email protected]
Co-Author:
Ved Prakash
Department of General Surgery
Narayan Medical College & Hospital, Jamuhar, Bihar, India
Authors Contributions
Both authors contributed to conceptualization, clinical investigation, and data curation by acquiring and critically reviewing relevant literature. They were jointly involved in the preparation of the original draft and in the writing, review, and editing to refine the manuscript. Additionally, both authors participated in supervising the work to ensure its accuracy and completeness. The final manuscript was approved by both authors for submission to the journal.
Informed Consent
Comprehensive informed consent, including both written and video documentation, was obtained from the patient and their attendant prior to the procedure.
Conflict of Interest Statement
The authors declare no conflicts of interest.
Guarantor
None
DOI
Cite this Article
Panchal JH, Prakash V. A Study of Laparoscopic (Simple or Complex) Cholecystectomy with or without ERCP and CBD Stenting Associated with Other General, Bariatric, Gynaecological, and Renal Surgical Procedures in a Single Session. medtigo J Med. 2025;3(2):e30623225. doi:10.63096/medtigo30623225 Crossref













