






 Author Affiliations
Author Affiliations
Abstract
Background: International travel exposes patients to environmental changes, including humidity, air pollution, and allergens that may precipitate asthma exacerbations. Post-travel outcomes in Gulf populations remain poorly defined.
Objective: To assess asthma worsening and treatment escalation following international travel among UAE-based patients, and to evaluate variation by destination.
Methodology: In this retrospective study, 485 patients with established asthma who traveled internationally between January 2022 and June 2025 were included. Eligible patients had a clinic visit within three months post-travel with documented symptoms or treatment changes. Worsening was defined within four weeks of return as treatment escalation (inhaled/systemic corticosteroids or bronchodilators), unplanned healthcare visits, emergency department visit, or clinician-documented exacerbation. Analyses were performed using RStudio.
Results: Mean age was 41.5 ± 13.2 years; 50.3% were female. Among 136 patients (28.0%) with complete treatment data, 86.0% experienced deterioration. Treatment escalation included bronchodilators (66.7%), ICS (50.7%), and systemic steroids (33.1%). Worsening was highest among travelers to Southeast Asia (up to 100% in a subgroup) and lowest in Western Europe (28.6–32.3%). No significant differences were observed between South Asia and other regions (p = 0.23). Age, sex, and smoking were not associated with risk.
Conclusion: Asthma worsens after travel is frequent, particularly following exposure to humid or polluted environments. Targeted pre-travel counseling and post-travel follow-up may reduce morbidity. Prospective studies with objective measures are needed.
Keywords
Asthma exacerbation, International travel, Post-travel outcomes, Environmental exposure, Treatment escalation, Air pollution, Allergen.
Introduction
Asthma is a common chronic respiratory condition influenced by environmental factors such as humidity, air pollution, and airborne allergens.[1,2] International travel can expose individuals to unfamiliar climates and irritants, potentially triggering symptom exacerbation.[3] Despite the UAE’s status as a major global travel hub, there is limited data on how travel impacts asthma control in its adult population.[4]
Most existing studies on travel-related asthma outcomes have focused on pediatric or Western populations, leaving a significant knowledge gap in Gulf-region cohorts.[5,6] Given the high mobility of UAE residents and the diverse destinations they visit, understanding post-travel asthma patterns is crucial for personalized preventive care.[4]
This study aimed to evaluate the frequency and geographic patterns of worsening asthma symptoms following international travel among patients treated at the emergency department of a tertiary care center in Dubai. By identifying destination-specific risks, we hope to inform clinical counseling and optimize asthma management strategies during the post-travel period.
Methodology
Study design and setting: This is a retrospective, descriptive review conducted in the pulmonology outpatient department of King’s College Hospital, London, Dubai, between January 1, 2021, and December 31, 2024.
Participants: Patients were eligible for inclusion if they had a physician-diagnosed history of asthma prior to undertaking international travel, documented evidence of travel abroad within the past three years, and a follow-up visit within three months of their return. Only those with complete records of travel details and post-travel symptoms or treatment adjustments were included. Patients were excluded if travel dates were missing or unclear, if they had other chronic pulmonary diseases, or if their post-travel documentation was incomplete.
Variables:
Exposure variable – Travel region classification:
Travel destinations were classified a priori into ten regions—GCC/Arabian Gulf, South Asia, East & Southeast Asia, Western Europe, North America, Africa/non-GCC Middle East, Eastern Europe & Central Asia, Australia/New Zealand, “Frequent travelers” (multiple destinations), and “Unknown/not specified” to reflect distinct climatic and pollution profiles (e.g., desert dust in the GCC, high humidity in South Asia, temperate pollen seasons in Europe). Multi-country and missing entries were excluded from single-region analyses.
Outcome variables – Post-travel asthma outcomes:
- Asthma exacerbation: occurrence within four weeks of return, defined as new or increased inhaled/systemic corticosteroids, bronchodilator escalation, emergency department visit, or clinician documentation of a flare.
- Treatment change: initiation or escalation of bronchodilators, inhaled corticosteroids, systemic corticosteroids, or other new asthma therapies.
Data collection: All data were extracted directly from the Cerner electronic medical record system. Travel details, outcomes, and treatment changes were taken from structured visit notes, prescription records, and clinician documentation.:
Statistical analysis: Continuous variables were summarized as means ± standard deviation (SD) or medians with interquartile range (IQR), and categorical variables as counts (%). Analyses were performed using RStudio (R version 4.x) with the tidyverse package suite.
Results
Gender distribution: A total of 485 patients were included in this analysis, with sex recorded for each individual. The pie chart in Figure 1 illustrates the proportion of male versus female subjects in the study population. In this study, 244 were female patients (50.3%) and 241 male patients (49.7%). The even split confirms our sample is demographically balanced, enhancing the generalizability of findings across sexes. This reduces the risk that gender differences will skew analyses of age, travel destinations, or treatment‐related outcomes.
Figure 1: Proportion of female and male subjects
Age distribution across decades: The full cohort of 485 patients is partitioned into ten-year age brackets to illustrate the overall sample structure. Figure 2 presents a bar chart where each bar’s height corresponds to the number of individuals in that decade.
In the chart, the 30-39-year-old group is the largest (172 patients, 35%), followed by the 40-49-year-old group (130 patients, 27%). The 20-29 years bracket contains 40 patients (8%), and the 50-59 years bracket has 58 (12%). Younger individuals (10-19 years) number 29 (6%), while the older age spans break down into 60-69 years (54 patients, 11%), 70-79 years (16 patients, 3%), 80-89 years (5 patients, 1%), and 90+ years (3 patients, < 1%). The roughly bell-shaped profile centered on the 30-49 years range indicates a predominantly adult sample with smaller tails at the youngest and oldest extremes.
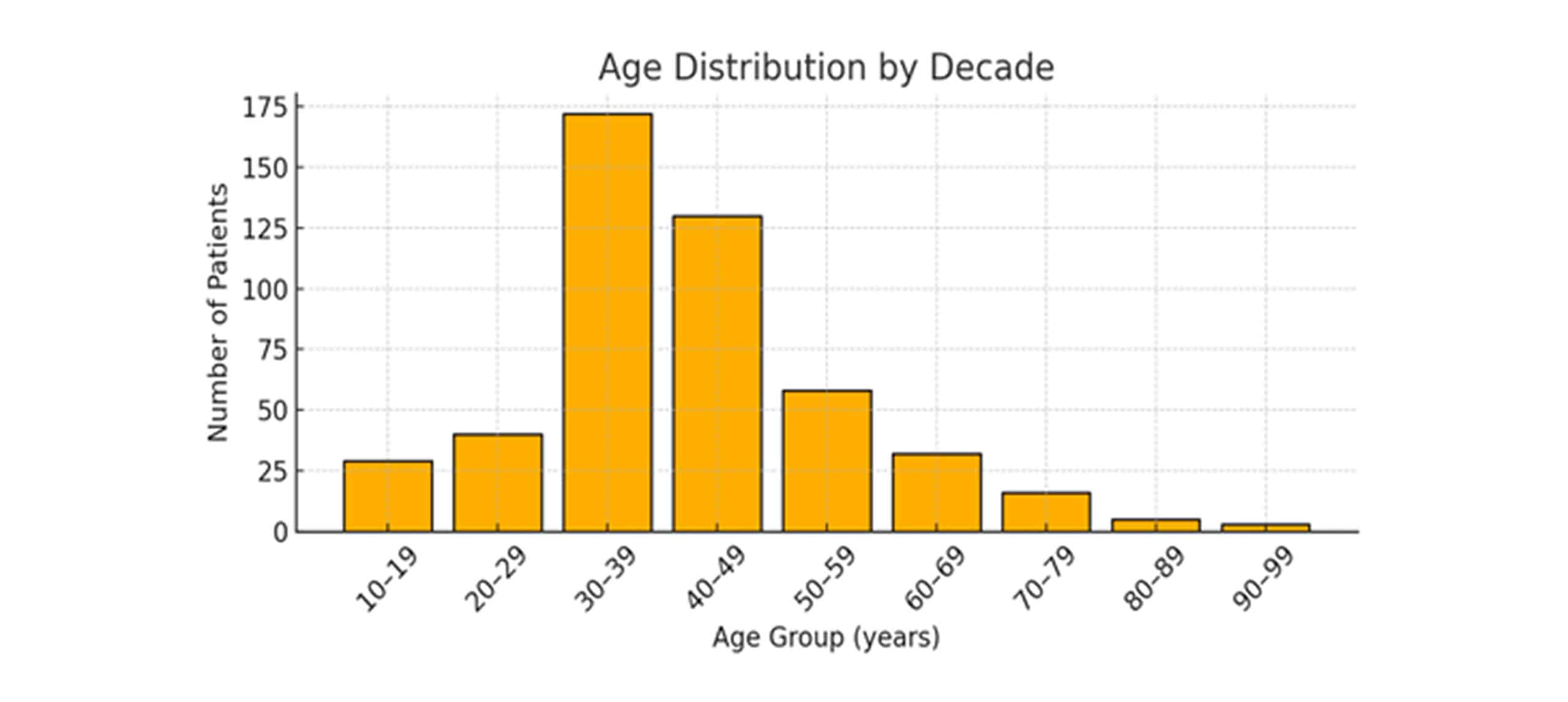
Figure 2: Histogram showing age distribution across decades
The age distribution (n = 485) is approximately bell‑shaped, centered in mid‑adulthood with a mean of 41.5 ± 13.2 years.
Regional breakdown of patients: Figure 3 illustrates the geographic distribution of the 213 patients (excluding the 272 with unknown travel data) who returned from international destinations over the past three years. Each bar represents the number of patients whose most recent trip fell into that region group.
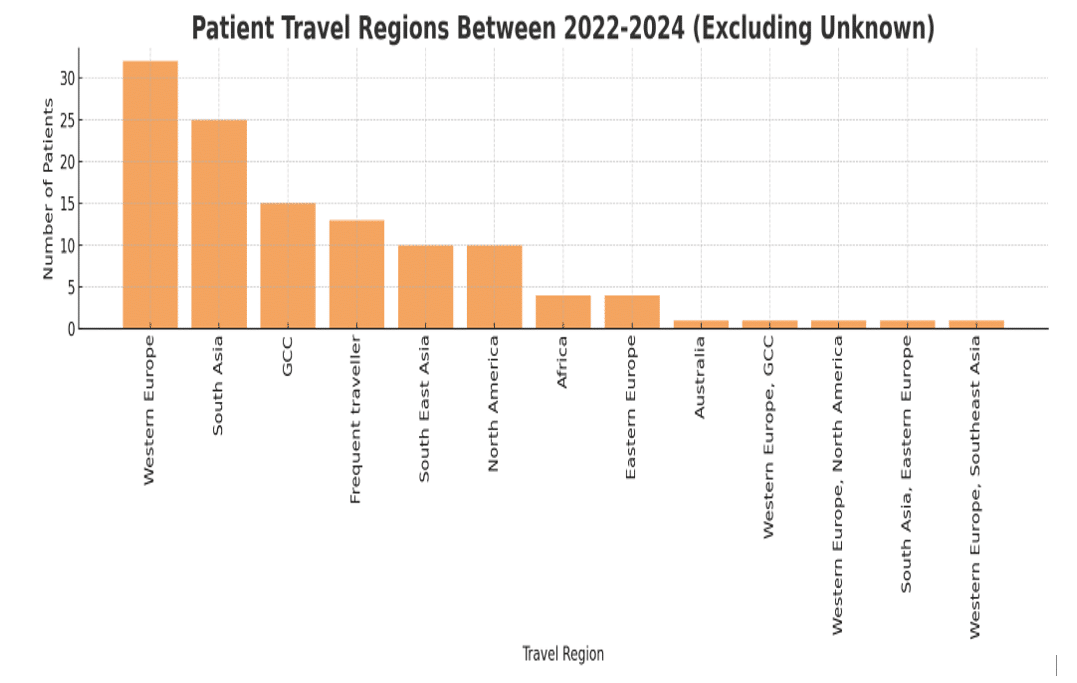
Figure 3: Distribution of patient travel regions within the last three years (2022-2024)
Among patients with a recorded region of travel, the largest proportion visited Western Europe (n = 32; 15%), reflecting its popularity as a destination for both business and leisure among our UAE cohort. South Asia (n = 25; 12%) and the GCC/Arabian Gulf countries (n = 15; 7%) were also frequent destinations, likely influenced by close cultural and economic ties as well as the convenience of short flight durations. A smaller subset of patients was categorized as “Frequent Travelers” (pilots, cabin crew, and business professionals with mixed destinations; n = 13; 6%), while travel to North America was reported in 10 patients (5%), both groups potentially facing unique exposures related to long-haul flights and cabin air recirculation. Other regions were less commonly represented, including South and Southeast Asia (n = 10; 5%), Africa excluding the GCC (n = 4; 2%), Eastern Europe and Central Asia (n = 4; 2%), and Australia/New Zealand (n = 2; 1%). Travel to rare destinations, each reported by a single patient, was grouped under “Other” for subsequent analyses due to sparse counts limiting region-specific inferences.
| Travel region | Count | Male | Female |
| Unknown | 353 (72.8%) | 173 (35.7%) | 180 (37.1%) |
| Western Europe | 35 (7.2%) | 19 (3.9%) | 16 (3.3%) |
| South Asia | 27 (5.6%) | 15 (3.1%) | 12 (2.5%) |
| GCC | 19 (3.9%) | 9 (1.9%) | 10 (2.1%) |
| Frequent traveller | 13 (2.7%) | 5 (1.0%) | 8 (1.6%) |
| Southeast Asia | 10 (2.1%) | 4 (0.8%) | 6 (1.2%) |
| North America | 11 (2.3%) | 5 (1.0%) | 6 (1.2%) |
| Africa | 5 (1.0%) | 4 (0.8%) | 1 (0.2%) |
| Eastern Europe | 5 (1.0%) | 4 (0.8%) | 1 (0.2%) |
| Western Europe, South Asia | 2 (0.4%) | 2 (0.4%) | 0 (0.0%) |
| Australia | 1 (0.2%) | 0 (0.0%) | 1 (0.2%) |
| Western Europe, GCC | 1 (0.2%) | 0 (0.0%) | 1 (0.2%) |
| Western Europe, North America | 1 (0.2%) | 1 (0.2%) | 0 (0.0%) |
| South Asia, Eastern Europe | 1 (0.2%) | 0 (0.0%) | 1 (0.2%) |
| Western Europe, Southeast Asia | 1 (0.2%) | 0 (0.0%) | 1 (0.2%) |
Table 1: Regional travel patterns by male and female patients
Western Europe was the most frequently documented travel destination (excluding unknown), with 35 patients (7.2%) exhibiting a slight male predominance (54% vs. 46%). South Asia was next, accounting for 27 patients (5.6%) and similarly skewed toward men (56% vs. 44%). Travel to GCC countries involved 19 patients (3.9%) and showed near gender parity (47% male vs. 53% female). Pilots, cabin crew, and other frequent flyers comprised 13 patients (2.7%) and were predominantly female (62%).
North America (11 patients, 2.3%) and Southeast Asia (10 patients, 2.1%) both had modest representation, each with a slight female majority. In contrast, Africa and Eastern Europe each accounted for only five patients (1.0%), both groups being 80% male. Finally, several mixed‐region entries (e.g., Western Europe/South Asia) appeared in two patients or fewer; these rare categories may be consolidated under “Other” for clarity.
Frequency of new symptoms by travel destination: In this section, we examine the proportion of patients who developed new or worsened asthma symptoms within four weeks of returning from travel, stratified by geographic destination. Using data from the 136‐patient subset with complete post-travel treatment records (excluding multi-country and Australia trips due to low counts), Figure 4 presents stacked bars showing the absolute number and percentage of individuals with and without new symptoms for each region. This analysis highlights regional variations in post-travel respiratory outcomes, allowing us to identify destinations associated with higher rates of symptom emergence and inform hypotheses about environmental or allergenic exposures specific to those areas.
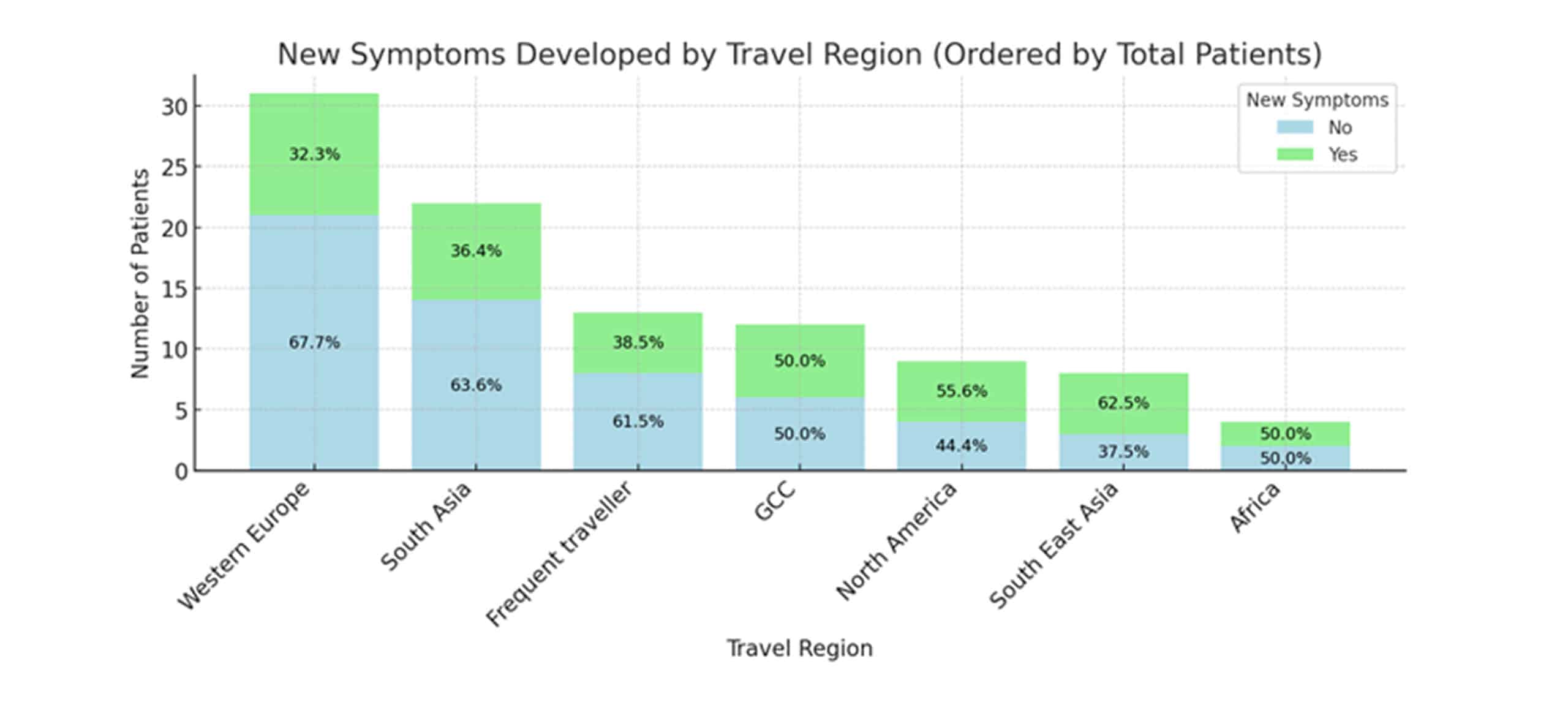
Figure 4: New symptoms developed by travel region
Among the 136 patients with complete post-travel treatment data, 117 (86%) developed new or worsened asthma symptoms within four weeks of return. Western Europe accounted for the largest group (n = 31) but had the lowest symptom‐development rate (32%), whereas Southeast Asia (n = 8) and North America (n = 9) showed the highest rates at 63% and 56%, respectively. South Asia (n = 22) and frequent travelers (n = 13) had intermediate rates of 36% and 38%. GCC travelers (n = 12) and Africa (n = 4) each had a 50% rate. Because only one or two patients traveled to several of the listed regions, their individual symptom rates swing wildly, sometimes 0%, sometimes 100%, so combining these into a single “Other” group produces more stable and interpretable results. Furthermore, we observed that travelers to particularly humid areas and those on long‐haul flights tended to report new or worsened asthma symptoms more often. To confirm and quantify these geographic effects, we will need larger patient samples from each region and statistical models that adjust simultaneously for age, sex, and smoking history.
| Travel region | No (n, %) | Yes (n, %) | Total |
| Western Europe | 21 (67.7 %) | 10 (32.3 %) | 31 |
| South Asia | 14 (63.6 %) | 8 (36.4 % | 22 |
| Frequent traveller | 8 (61.5 %) | 5 (38.5 % | 13 |
| GCC | 6 (50.0 %) | 6 (50.0 %) | 12 |
| North America | 4 (44.4 %) | 5 (55.6 %) | 9 |
| South East Asia | 3 (37.5 %) | 5 (62.5 %) | 8 |
| Africa | 2 (50.0 %) | 2 (50.0 %) | 4 |
| Western Europe, South Asia | 1 (50.0 %) | 1 (50.0 %) | 2 |
| Australia | 0 (0.0 %) | 1 (100.0 %) | 1 |
| Western Europe, GCC | 0 (0.0 %) | 1 (100.0 %) | 1 |
| Western Europe, North America | 0 (0.0 %) | 1 (100.0 %) | 1 |
| South Asia, Eastern Europe | 0 (0.0 %) | 1 (100.0 %) | 1 |
| Western Europe, Southeast Asia | 1 (100.0 %) | 0 (0.0 %) | 1 |
Table 2: Regional breakdown of post-travel asthma symptom development
Discussion
This retrospective study highlights that post-travel asthma symptom worsening is common in patients with asthma.[7] Our findings align with previous research linking environmental exposures like humidity and pollution to asthma exacerbations.[1,8] The lower rate of worsening observed in Western Europe may reflect better air quality and fewer allergens.[9] Despite the high frequency of travel to South Asia, symptom worsening rates were moderate, potentially due to varying climatic conditions and traveler adaptation.[7,10] Clinically, these results emphasize the importance of pre-travel asthma counseling tailored to destination-specific risks and underscore the need for close post-travel follow-up to identify and manage asthma exacerbations promptly.[3,4,7]
The limitations of this study include its retrospective design, incomplete data for many patients, and a lack of spirometry or objective environmental exposure measures.[4] The relatively small sample size for some regions limits the statistical power to detect differences. Future prospective studies incorporating objective lung function testing, allergen exposure assessment, and longer-term follow-up will provide more robust data to inform clinical guidelines for asthma management in travellers.[3,6,8]
Conclusion
Asthma symptom worsening is frequent after international travel among UAE patients, with geographic variation suggesting environmental factors play a key role. Personalized counseling and post-travel monitoring are essential to improve patient outcomes.
References
- Mahboub B, Vats M, Afzal S, Sharif W, Iqbal M. Environmental exposure and nonadherence with medicines directly correlate with exacerbations and hospitalization for asthma: a population-based survey from UAE. ISRN Pulmonology. 2012;2012:831687. doi:10.5402/2012/831687
Crossref | Google Scholar - Alzaabi A, Al Busaidi N, Pradhan R, et al. Over-prescription of short-acting β2-agonists and asthma management in the Gulf region: a multicountry observational study. Asthma Res Pract. 2022;8(1):3. doi:10.1186/s40733-022-00085-5
PubMed | Crossref | Google Scholar - Golan Y, Onn A, Villa Y, et al. Asthma in adventure travelers: a prospective study evaluating the occurrence and risk factors for acute exacerbations. Arch Intern Med. 2002;162(21):2421-2426. doi:10.1001/archinte.162.21.2421
PubMed | Crossref | Google Scholar - Abuzakouk M, Ghorab OKHA, Mahboub B, et al. Demographic and clinical patterns of severe asthma in the Middle East. Ann Thorac Med. 2021;16(2):172-177. doi:10.4103/atm.ATM_131_20
PubMed | Crossref | Google Scholar - Mireku N, Wang Y, Ager J, Reddy RC, Baptist AP. Changes in weather and the effects on pediatric asthma exacerbations. Ann Allergy Asthma Immunol. 2009;103(3):220-224. doi:10.1016/S1081-1206(10)60185-8
PubMed | Crossref | Google Scholar - Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention, 2023. Updated July 2023.
Global Strategy for Asthma Management and Prevention, 2023 - D’Amato G, Bergmann KC, Cecchi L, et al. Climate change and air pollution: Effects on pollen allergy and other allergic respiratory diseases. Allergo J Int. 2014;23(1):17-23. doi:10.1007/s40629-014-0003-7
PubMed | Crossref | Google Scholar - Agency for Toxic Substances and Disease Registry. Environmental Triggers of Asthma. 2014.
Environmental Triggers of Asthma - Wang Z, Li Y, Gao Y, et al. Global, regional, and national burden of asthma and its attributable risk factors from 1990 to 2019: a systematic analysis for the Global Burden of Disease Study 2019. Respir Res. 2023;24(1):169. doi:10.1186/s12931-023-02475-6
PubMed | Crossref | Google Scholar - Al-Ahmad M, Mobayed H, Al Busaidi N, et al. Severe asthma treatment patterns: A multicenter observational study in the Gulf region. World Allergy Organ J. 2022;15(5):100647. doi:10.1016/j.waojou.2022.100647
PubMed | Crossref | Google Scholar
Acknowledgments
None
Funding
This research received no external funding.
Author Information
Corresponding Author:
Safeena Imran
Department of Medical-Surgical
King’s College Hospital London, Dubai
Email: safeenaimran1@gmail.com
Co-Authors:
Sneha Celine Jossie, Neusha Haque
Medical Intern
King’s College Hospital London, Dubai
Jonathan Figy John
Statistician
University of Leeds, England
Umer Shabbir
Medical Officer
Midciti Hospital, Karachi
Muhammad Shahid Peerbhoy, Syed Arshad Husain
Department of Pulmonology
King’s College Hospital London, Dubai
Authors Contributions
Safeena Imran coordinated the overall study, served as the corresponding author, and oversaw data collection, manuscript preparation, drafting, submission, and communication during the peer-review process. Sneha Celine Jossie contributed to data collection, data verification, literature review, and manuscript drafting and editing. Neusha Haque assisted with data collection, data organization, and manuscript preparation. Jonathan Figy performed the statistical analysis and contributed to data interpretation and presentation of results. Umer Shabbir contributed to the literature review, manuscript drafting, and editing. Muhammad Shahid Peerbhoy and Syed Arshad Husain supervised the study, contributed to the study design, and provided critical intellectual input. All authors reviewed and approved the final manuscript and agreed to be accountable for all aspects of the work in accordance with the ICMJE authorship criteria.
Ethical Approval
This study was reviewed and approved by the Institutional Research Ethics Board (IRB) of King’s College Hospital London, Dubai. The requirement for individual informed consent was waived by the Ethics Committee because this was a retrospective observational study using anonymized routinely collected clinical data, with no direct patient contact and no impact on patient care.
Conflict of Interest Statement
The authors declare no conflicts of interest.
Guarantor
None
DOI
Cite this Article
Imran S, Jossie SC, Haque N, et al. A Retrospective Study of Post-Travel Asthma Worsening in a UAE Cohort (2021–2024). medtigo J Emerg Med. 2026;3(1):e3092311. doi:10.63096/medtigo3092311 Crossref













