






 Author Affiliations
Author Affiliations
Abstract
Background: Leukemia cutis (LC) is a rare extramedullary manifestation of leukemia characterized by the infiltration of malignant leukocytes into the epidermis, dermis, or subcutaneous tissue. It is uncommon in acute lymphoblastic leukemia (ALL) and is often considered a poor prognostic marker.
Case presentation: Our patient is a 21-year-old Ethiopian male who presented with a 6-month history of progressively worsening bilateral neck swelling, which was accompanied by difficulty swallowing, hoarseness, fever, night sweats, and 8 kg weight loss over the past 2 months. Complete blood count (CBC) revealed a white blood cell (WBC) count of 239,700/μL with a bone marrow aspiration of 98% lymphoblasts. Skin punch biopsy, which was evaluated via immunohistochemistry, was consistent with LC associated with T-cell ALL.
Conclusion: This case underscores the association between LC and T-ALL, emphasizing the need for early recognition and thorough diagnostic evaluation. It highlights the importance of timely diagnosis in improving outcomes, especially in resource-limited settings, where managing leukemia demands awareness and strategic clinical care.
Keywords
Leukemia cutis, T-cell acute lymphoblastic leukemia, Cutaneous infiltration, Immunohistochemistry, Hyperleukocytosis.
Introduction
Leukemia cutis (LC) is defined as the infiltration of malignant leukocytes into the skin in patients with underlying hematologic malignancies, presenting with varied cutaneous manifestations, including papules, nodules, and plaques.[1] LC can occur in different leukemia subtypes, including myeloid and lymphoid lineages, but is rare in acute lymphoblastic leukemia (ALL).[2] Although acute myeloid leukemia (AML) is most commonly associated with LC, T-cell ALL (T-ALL) rarely manifests with skin involvement.[3]
LC lesions may be localized or disseminated, affecting extremities, trunk, scalp, and face.[4] Histopathology and immunohistochemistry are essential for diagnosis, helping differentiate LC from primary cutaneous lymphomas or other dermatologic conditions.[5] Adult patients with LC often have more aggressive disease and a poorer prognosis.[6]
We report a rare case of T-ALL with LC in a 21-year-old Ethiopian male, highlighting the clinical, laboratory, and histopathological features and emphasizing the importance of early recognition of cutaneous manifestations in adult ALL.[7,8,9]
Case Presentation
A 21-year-old male presented with a 6-month history of progressive bilateral neck swelling accompanied by dysphagia for solids and liquids, hoarseness, constitutional symptoms (fever, night sweats), and an 8 kg unintentional weight loss over two months. Associated symptoms included exertional fatigue, lightheadedness, and tinnitus. Over the preceding two months, he had developed multiple asymptomatic cutaneous lesions beginning as small erythematous papules that progressed to larger, firm, bluish nodules distributed over his trunk and upper extremities. No bleeding tendency was reported. His medical history was otherwise unremarkable, except for a 4-day course of unspecified medications at a private hospital 2 months prior.
On physical examination, the general appearance was acute and sick-looking. His vital signs included a blood pressure of 102/59 mmHg, a pulse rate of 116 bpm, a respiratory rate of 22 breaths per minute, a temperature of 36.7°C, and an oxygen saturation of 97% on room air. A Head, Eyes, Ears, Nose, and Throat (HEENT) examination showed conjunctival hemorrhage and periorbital ecchymosis. Marked tonsillar swelling (Figure 1C) was noted along with extensive lymphadenopathy involving submandibular (largest 8×10 cm left submandibular node), submental, pre-/post-auricular, parotid (bilateral), axillary (2×3 cm), and inguinal (3 cm) regions. The abdominal examination demonstrated splenomegaly (6-8 cm below the Left Costal Margin (LCM)). Dermatologic examination revealed multiple non-tender, bluish-colored papules and nodules predominantly on upper extremities (Figure 1A and B) with Grade 1 pedal edema.
Laboratory and diagnostic findings: CBC revealed a WBC count of 239,700/μL, a hemoglobin level of 4.2 g/dL, a hematocrit of 12.2%, and a platelet count of 26,000/μL. Serum electrolytes included sodium at 125 mEq/L, potassium at 3.84 mEq/L, and chloride at 98.0 mEq/L. Liver enzymes were elevated, with aspartate aminotransferase (AST) at 116 U/L, alanine aminotransferase (ALT) at 10 U/L, and alkaline phosphatase (ALP) at 190 U/L, while total bilirubin was 0.8 mg/dL. Renal function tests revealed a creatinine level of 0.6 mg/dL and a urea level of 24 mg/dL. The serum albumin concentration was 3.1 g/dL.
Peripheral blood smear (Figure 3) and bone marrow aspiration (Figure 2) demonstrated 97-98% lymphoid blasts, consistent with ALL. Echocardiography revealed mild tricuspid regurgitation and pulmonary hypertension. Abdominal ultrasound confirmed splenomegaly with enlarged para-aortic and iliac lymph nodes. Computed tomography (CT) imaging of the neck demonstrated significant cervical and Waldeyer’s lymphadenopathy, suggestive of lymphoproliferative disease.
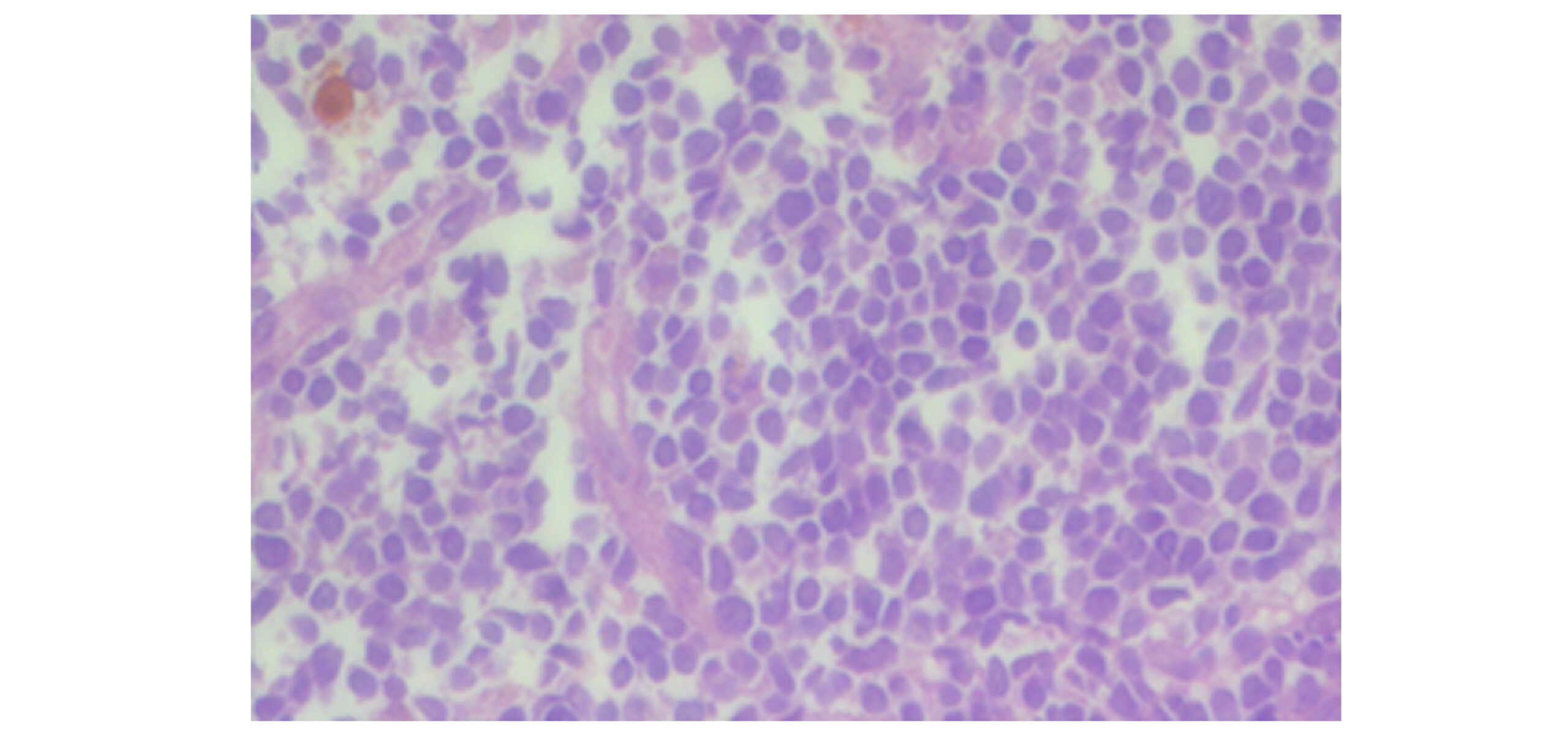
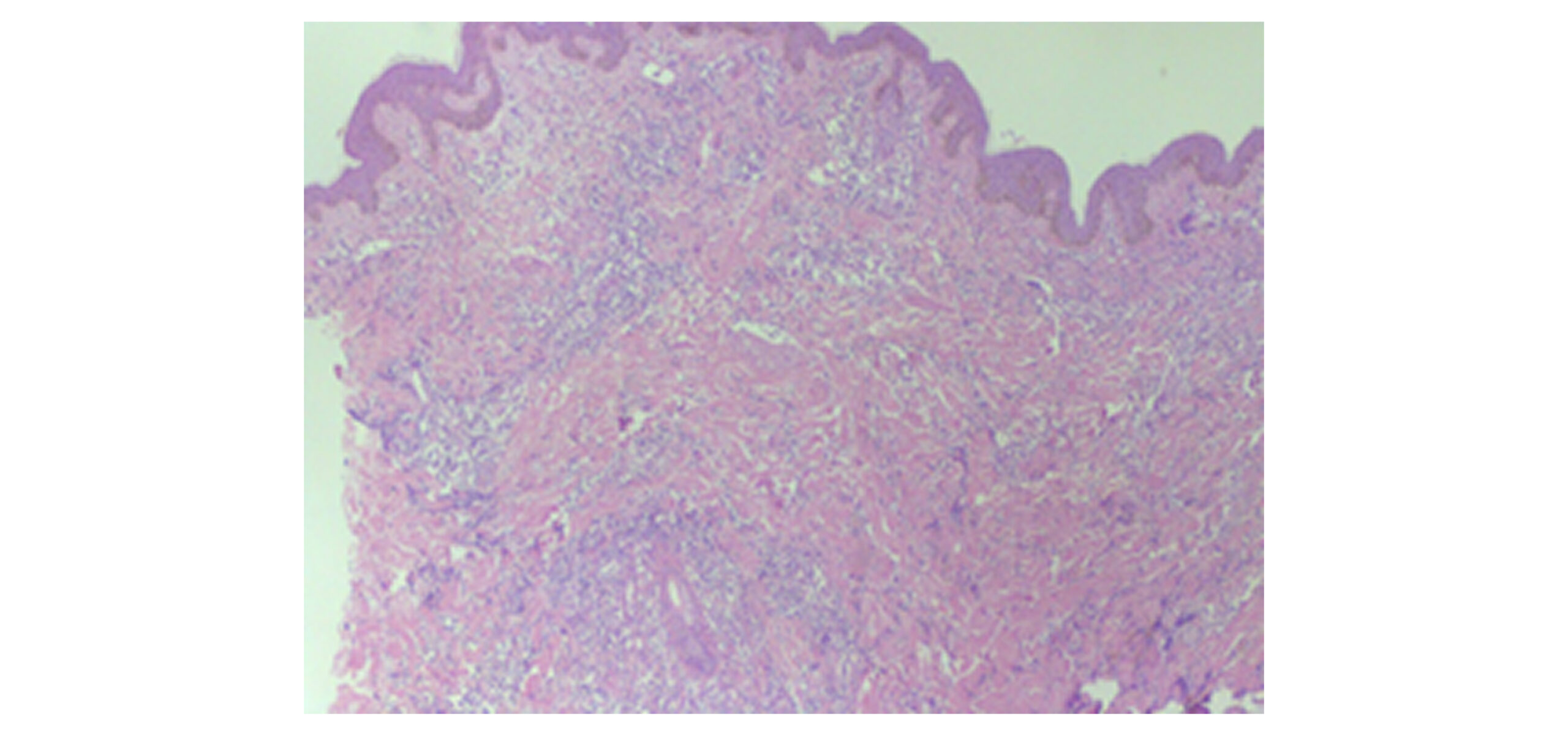
Histopathological examination of a right arm skin biopsy (Figure 4: A and B) revealed orthokeratosis with mild spongiosis. The dermis contained diffuse infiltrates of small-to-intermediate lymphoid cells displaying mild nuclear pleomorphism, hyperchromatic nuclei, and scant cytoplasm. Immunohistochemistry (Figure 5: A-D) was positive for Cluster of Differentiation (CD) 3 and CD 45 but negative for CD 20, with a high proliferative index (Ki67 55%). These findings confirmed a diagnosis of LC secondary to T-ALL.

A

B

C
Figure 1: (A and B) Solid, elevated, firm-to-the-touch lumps/nodules and plaques; (C): Bilateral erythematous tonsillar swelling
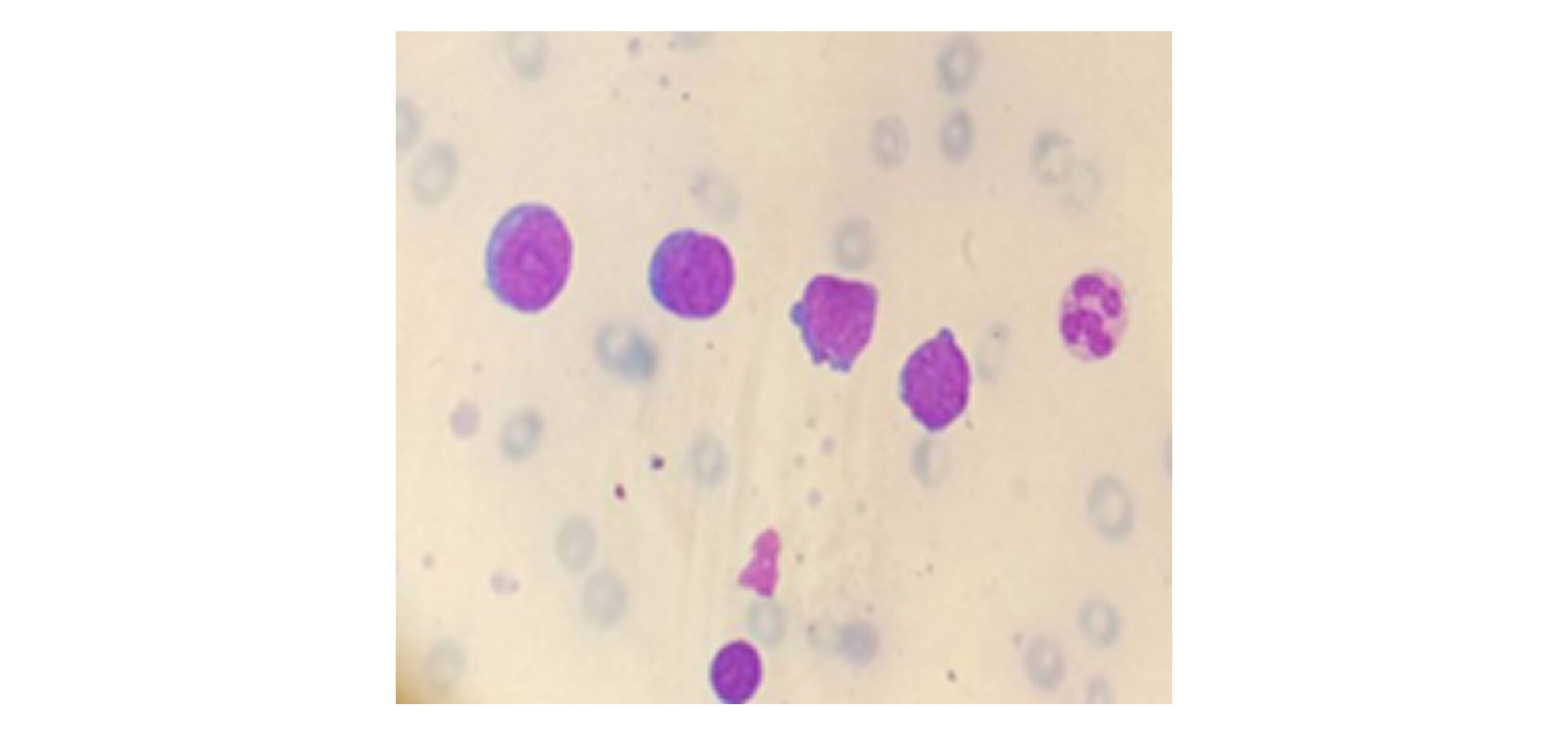
Figure 2: Bone marrow aspiration shows 98% infiltration by lymphoid blasts, consisting of large cells with a high nuclear-cytoplasmic ratio, irregular nuclear contours, inconspicuous nucleoli, and a scant cytoplasmic rim. These findings indicate acute leukemia, with a diagnosis favoring ALL
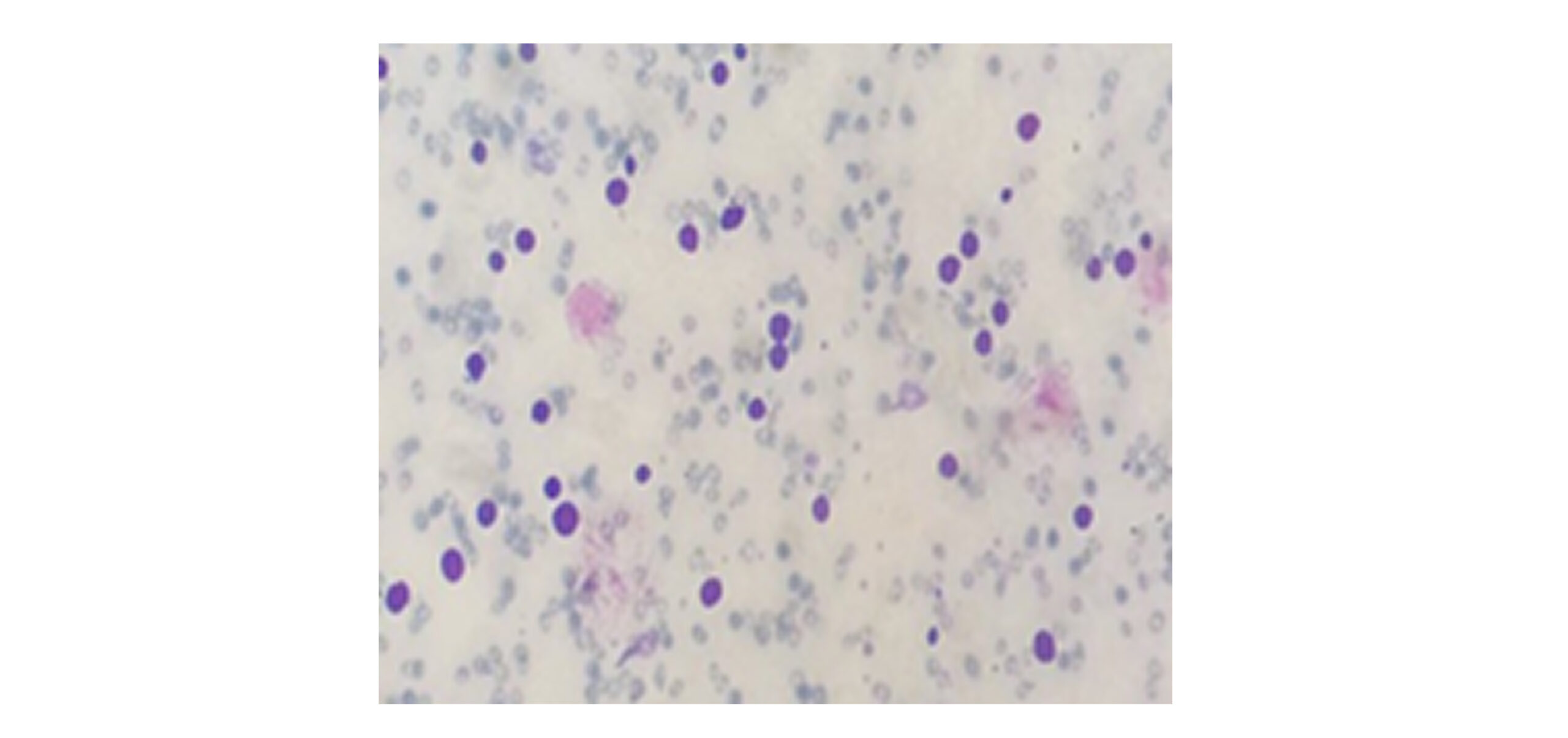
Figure 3: Peripheral smear analysis reveals mild anisopoikilocytosis of red blood cells (RBCs), normochromic with a few microcytes. The WBC count is elevated, with a differential neutrophil count of 1%, a lymphocyte count of 1%, and a blast count of 97%. The blasts exhibited a lymphoid morphology characterized by large cells with a high nuclear‒cytoplasmic ratio, irregular nuclear contours, inconspicuous nucleoli, and a scant rim of cytoplasm. These findings are consistent with acute leukemia, suggesting a diagnosis of ALL
A
B
Figure 4: Hematoxylin and eosin staining of skin biopsy, Figure (A) at high-power magnification and (B) at low-power magnification: orthokeratosis with mild spongiosis. The dermal layer contains diffuse sheets of small to intermediate-sized lymphoid cells, exhibiting mild nuclear pleomorphism with ovoid to angulated hyperchromatic nuclei and a scant rim of cytoplasm
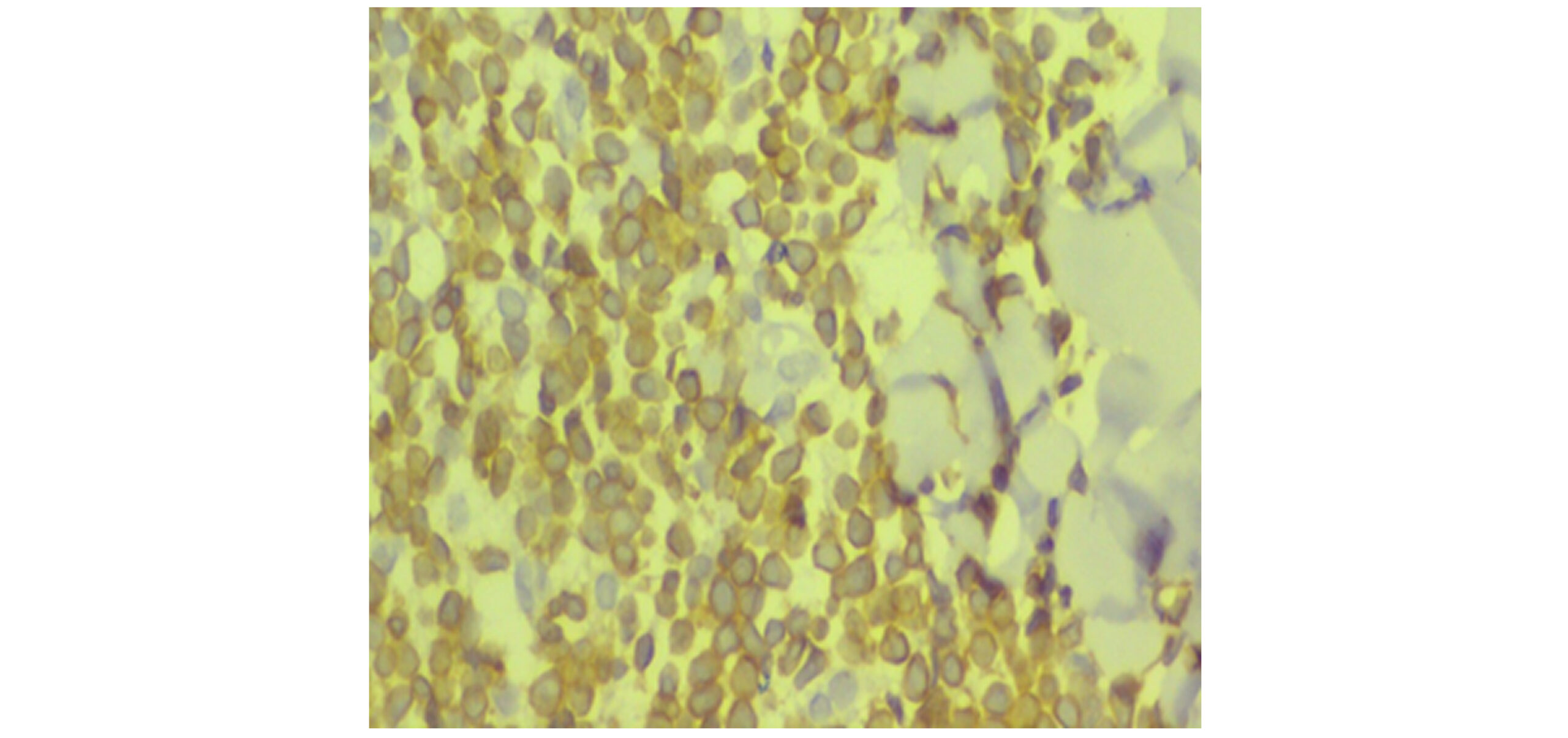
Figure 5A: CD3 at the highest magnification
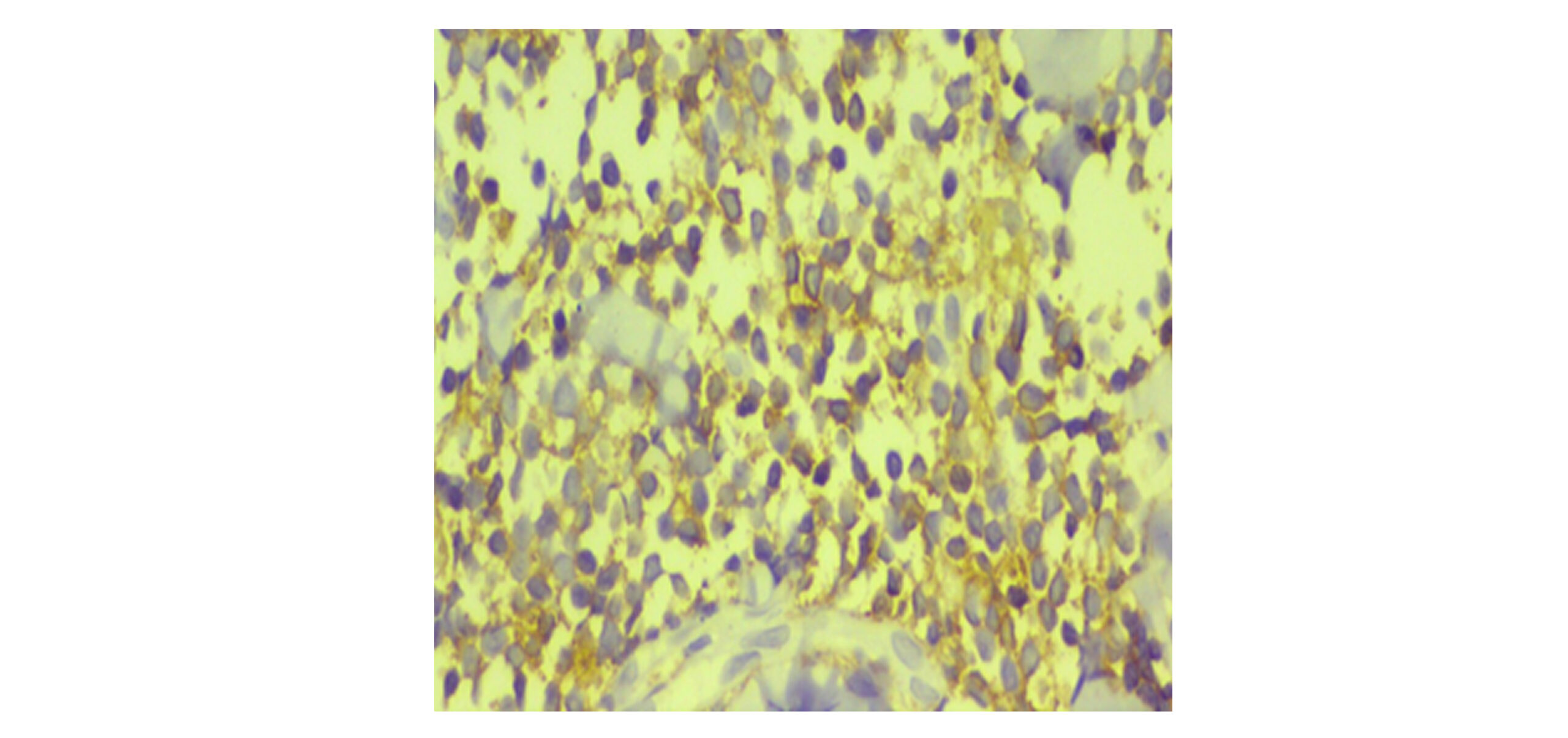
Figure 5B: CD45 at the highest magnification
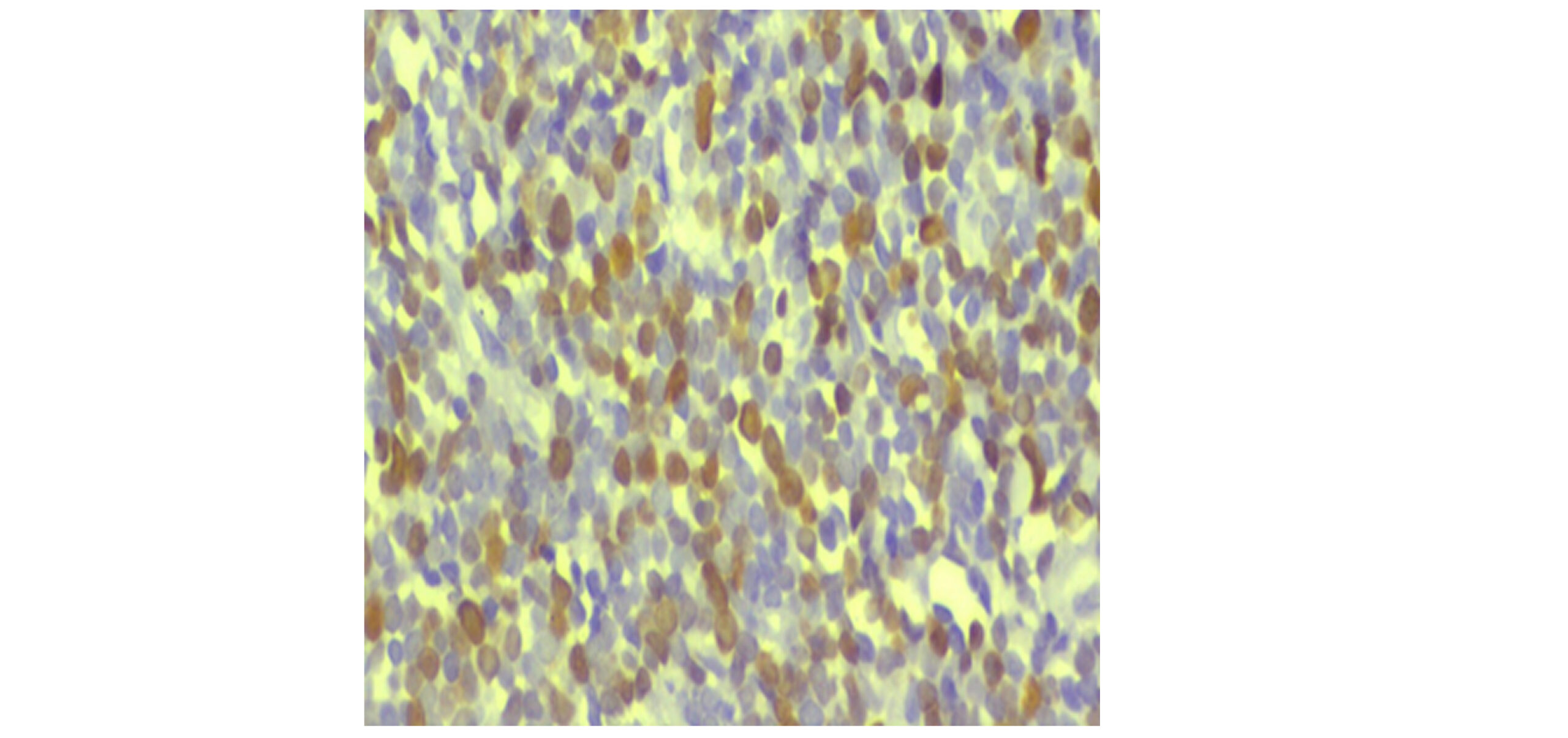
Figure 5C: Ki-67 at higher magnification
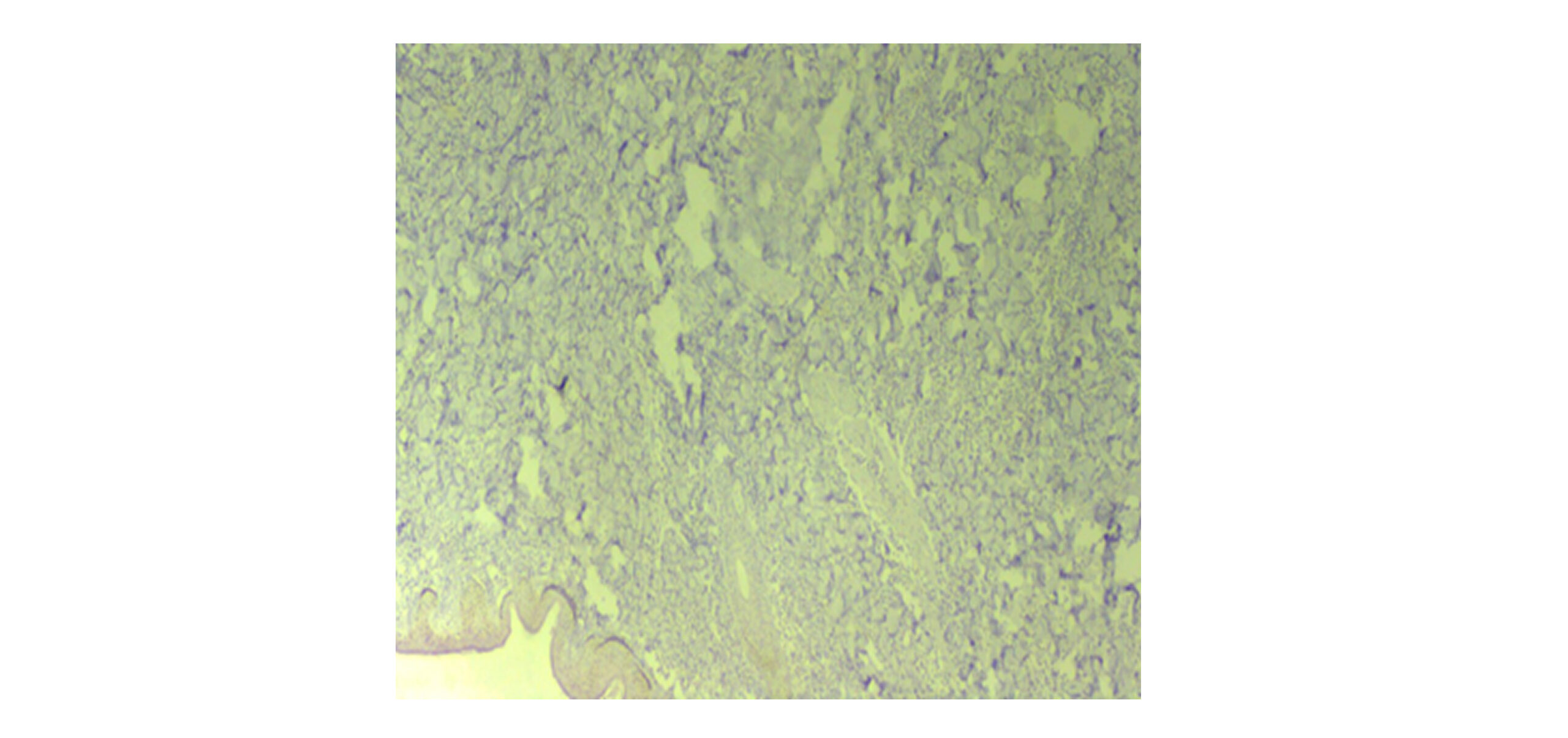
Figure 5D: CD20-negative
Case Management
The patient was admitted to the hematology ward with a diagnosis of ALL complicated by hyperleukocytosis and upper airway obstruction (UAO) secondary to a tonsillar mass. Initial management included transfusion of packed RBCs and platelets, followed by initiation of standard chemotherapy. During the first cycle of chemotherapy, the patient developed neutropenic fever with a gastrointestinal focus, which resolved with appropriate treatment, allowing chemotherapy to continue. However, following the second chemotherapy cycle, he presented with a persistent fever and productive cough. Physical examination revealed coarse crackles in the right lower lung field.
Microbiological workup identified multidrug-resistant Escherichia coli (sensitive to meropenem and gentamicin) in sputum cultures. A chest CT scan demonstrated multifocal centrilobular nodules with a tree-in-bud pattern, along with enlarged axillary and mediastinal lymph nodes, consistent with bronchopneumonia. Additionally, a GeneXpert test confirmed a Mycobacterium tuberculosis infection. Combination therapy with antituberculosis drugs and meropenem was initiated, leading to clinical improvement. The patient was subsequently discharged in stable condition with close outpatient follow-up for continued management of ALL and tuberculosis.
Discussion
LC represents a rare extramedullary manifestation of leukemia resulting from the infiltration of malignant lymphoblasts into the skin.[1,2] While LC is more frequently observed in AML, it is uncommon in T-ALL, with an incidence of only 1-3%.[3,5] Our patient presented with multiple bluish papules and nodules predominantly on the upper extremities, massive cervical lymphadenopathy, and splenomegaly, reflecting aggressive systemic T-ALL.[6]
The pathogenesis of LC involves migration of malignant lymphoblasts to the skin, potentially mediated by adhesion molecules and chemokine signaling.[1,2] In T-ALL, chromosomal rearrangements and somatic mutations drive leukemogenesis and may facilitate extramedullary infiltration.[3,4]
Histopathologically, LC in T-ALL is characterized by dense dermal infiltrates of small-to-intermediate lymphoid cells with hyperchromatic nuclei, scant cytoplasm, and a high nuclear-to-cytoplasmic ratio. Tumor cells typically express T-cell markers (CD3, CD45), are negative for B-cell markers (CD20), and show high proliferative activity, as seen in our patient (Ki-67 55%).[7,8] This concordance between bone marrow and cutaneous findings confirms LC secondary to T-ALL.
Diagnosis requires clinical suspicion, histopathology, and immunophenotyping. Adult patients with LC often present with systemic disease, necessitating evaluation of bone marrow, peripheral blood, and imaging for extramedullary involvement.[5,9]. In our patient, profound leukocytosis (WBC: 239,700/μL), severe anemia (Hb: 4.2 g/dL), thrombocytopenia, and massive lymphadenopathy highlighted the aggressive nature of adult T-ALL with LC.
Management focuses on treating the underlying leukemia. Systemic chemotherapy is the mainstay, often resulting in regression of skin lesions. Supportive care, including transfusions and management of airway obstruction or hyperleukocytosis, is critical in acute presentations.[6,7] Hematopoietic stem cell transplantation may be considered for long-term remission in selected patients.[8]
This case emphasizes the importance of recognizing cutaneous lesions as early indicators of aggressive T-ALL in adults. Prompt histopathological and immunophenotypic evaluation is crucial for accurate diagnosis and guiding therapy, given the rarity and prognostic significance of LC in T-ALL.[9]
Conclusion
This report emphasizes that LC, though rare in T-ALL, is a critical diagnostic clue to the underlying systemic disease. Early recognition and aggressive treatment are essential to improving outcomes in these complex cases. The unique aspects of this case, including its presentation, diagnostic workup, and therapeutic challenges, make it a valuable addition to the medical literature.
References
- Wagner G, Fenchel K, Back W, Schulz A, Sachse MM. Leukemia cutis – epidemiology, clinical presentation, and differential diagnoses. J Dtsch Dermatol Ges. 2012;10(1):27-36. doi:10.1111/j.1610-0387.2011.07842.x
PubMed | Crossref | Google Scholar - Sander CA, Medeiros LJ, Abruzzo LV, Horak ID, Jaffe ES. Lymphoblastic lymphoma presenting in cutaneous sites: A clinicopathologic analysis of six cases. J Am Acad Dermatol. 1991;25(6):1023-1031. doi:10.1016/0190-9622(91)70302-i
PubMed | Crossref | Google Scholar - Li L, Wang Y, Lian CG, Hu N, Jin H, Liu Y. Clinical and pathological features of myeloid leukemia cutis. An Bras Dermatol. 2018;93(2):216-221. doi:10.1590/abd1806-4841.20186327
PubMed | Crossref | Google Scholar - Weedon D. Weedon’s Skin Pathology. Expert Consult – Online and Print. eBook. Elsevier Health Sciences; 2009.
Weedon’s Skin Pathology - Bakst RL, Tallman MS, Douer D, Yahalom J. How I treat extramedullary acute myeloid leukemia. Blood. 2011;118(14):3785-3793. doi:10.1182/blood-2011-04-347229
PubMed | Crossref | Google Scholar - Rafei H, Kantarjian HM, Jabbour EJ. Recent advances in the treatment of acute lymphoblastic leukemia. Leuk Lymphoma. 2019;60(11):2606-2621. doi:10.1080/10428194.2019.1605071
PubMed | Crossref | Google Scholar - Lee E, Park HJ, Cho BK, et al. Leukemia cutis as early relapse of T-cell acute lymphoblastic leukemia. Int J Dermatol. 2010;49:335-337. doi:10.1111/j.1365-4632.2009.04255.x
PubMed | Crossref | Google Scholar - Arora P, Sinha N, Malhotra P, et al. T-cell acute lymphoblastic leukemia with a rare chromosomal translocation presenting as leukemia cutis. Int J Dermatol. 2022;61:e120-123. doi:10.1111/ijd.15757
PubMed | Crossref | Google Scholar - Campuzano-Garcia AE, Torres-Alvarez B, Castanedo-Cazares JP. Leukemia cutis in a patient with pre-B-cell acute lymphoblastic leukemia. JAAD Case Rep. 2015;1(6):364-367. doi:10.1016/j.jdcr.2015.08.005
PubMed | Crossref | Google Scholar
Acknowledgments
None
Funding
None
Author Information
Corresponding Author:
Yadelew Jember Kassie
Department of Internal Medicine
Saint Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia
Email: [email protected]
Co-Authors:
Helen Hilawi, Mustejib Abdela Hussen, Tariku Endale, Amanuel Tsedale
Department of Internal Medicine
Saint Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia
Mulatu Birhanu Gurara
Department of Pathology
Saint Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia
Authors Contributions
All authors contributed to the Conceptualization, investigation, and Data Curation by acquiring and critically reviewing the selected articles. They were collectively involved in the Writing, Original Draft preparation and Writing, Review & Editing to refine the manuscript. Additionally, all authors participated in the supervision of the work, ensuring accuracy and completeness. The final manuscript was approved by all named authors for submission to the journal.
Ethical Approval
None
Conflict of Interest Statement
The authors declare no conflicts of interest.
Guarantor
None
DOI
Cite this Article
Kassie YJ, Hilawi H, Hussen MA, Gurara MB, Endale T, Tsedale A. A Rare Case of Leukemia Cutis in T-Cell Acute Lymphoblastic Leukemia: A Report from a Resource-Limited Setting. medtigo J Med. 2026;4(2):e3062428. doi:10.63096/medtigo3062428 Crossref













