






 Author Affiliations
Author Affiliations
Abstract
Ceruminous adenocarcinoma is a rare malignant neoplasm of the ceruminous glands of the external auditory canal (EAC), representing less than 0.0003% of all tumors. Due to its rarity and morphologic overlap with other glandular neoplasms, its diagnosis can be challenging. We report a case of a 60-year-old male presenting with a complaint of decreased hearing and ear discharge. Computed tomography (CT) imaging revealed a well-defined soft tissue lesion with internal calcifications and erosion of the anterior mastoid wall, raising clinical suspicion of cholesteatoma or aural polyp. An incisional biopsy was performed. Histopathological examination of the tumor cells showed that they were arranged in glandular, cribriform, papillary, and solid patterns with marked pleomorphism. There was also evidence of high mitotic activity and vascular invasion. Immunohistochemistry was not performed due to resource limitations. However, the diagnosis of ceruminous adenocarcinoma was established based on classical histological features and tumor location. Due to its nonspecific symptoms and histological overlap with other tumors, accurate diagnosis relies heavily on thorough histopathological examination. Distant metastases of ceruminous adenocarcinoma have been reported in the lungs, liver, kidneys, cervical lymph nodes, and bones, along with intracranial extension. The presence of metastasis is associated with poor prognosis, with mortality most commonly resulting from either intracranial invasion or pulmonary metastases. This case emphasizes the importance of diligent morphological analysis in the absence of immunohistochemical facilities.
Keywords
Ceruminous adenocarcinoma, External auditory canal, Histopathology, Ear tumor, Resource-poor setting.
Introduction
The external ear canal (EAC) comprises the bony inner two-thirds and the cartilaginous outer third. The skin of the cartilaginous section has many hair follicles, sebaceous glands, and a particular kind of apocrine sweat gland called ceruminous glands; the skin covering the bony portion has few appendages. Tumors resulting from these glands are extremely uncommon and resemble those from sweat glands in other parts of the body.[1-4]
Because of their varied clinical and histological features, tumors originating from the ceruminous glands in the external ear canal can be difficult to diagnose. Tumors originating from the ceruminous glands in the external ear canal can pose a diagnostic challenge due to their diverse clinical and histological characteristics. These tumors constitute less than 0.0003% of all tumors and are often difficult to diagnose due to their nonspecific clinical presentation and histologic overlap with other neoplasms, such as metastatic adenocarcinoma or other adnexal tumors.[5] The actual incidence, terminology, behavior, and histopathological classification of these tumors are still uncertain, leading to ongoing debate regarding their management.[6] The pathology of ceruminous gland tumors is not well documented in standard pathology texts because they sit at the crossroads of dermatopathology and ear, nose, and throat (ENT) pathology.[6]
Case Presentation
Here, we present a case of a 60-year-old male presenting with a complaint of decreased hearing and ear discharge for 6 months. Otoscopy showed a polypoid mass in the external auditory canal.
Radiological imaging: Radiological findings on CT scan showed well-defined soft tissue density with foci of calcification in the right external auditory canal, with its complete obscuration and erosion of the anterior wall of the mastoid bone, providing differential diagnosis of cholesteatoma and aural polyp. Incisional biopsy was sent for further evaluation with clinical diagnosis of external auditory canal polyp.
Gross examination: The specimen consisted of multiple grey-white soft tissues collectively measuring 2.5×2 cm. On the cut section, the tissue was firm and partially necrotic. The entire specimen was processed and submitted for routine paraffin embedding.
Microscopic examination: Sections examined show tissue lined by keratinized stratified squamous epithelium. Underlying sub-epithelium shows tumor cells arranged in nests, glandular, cribriform, papillary, and solid patterns separated by dense hyalinized stroma. The glandular structures are lined by inner luminal and outer myoepithelial cells. Individual cells are exhibiting marked pleomorphism in the form of a high N: C ratio, irregular nuclear contour, vesicular to coarse chromatin, prominent nucleoli, and a moderate to abundant amount of eosinophilic granular cytoplasm. These tumor cells are seen infiltrating into the deep fibrous tissue. Frequent mitotic figures are also noted. Focal areas show tumor cells emboli in the lumen of blood vessels. There is also a dense infiltration of chronic inflammatory cells and areas of necrosis and hemorrhage. However, surface epithelial dysplasia is not identified. The overall histopathological features are consistent with ceruminous adenocarcinoma NOS.
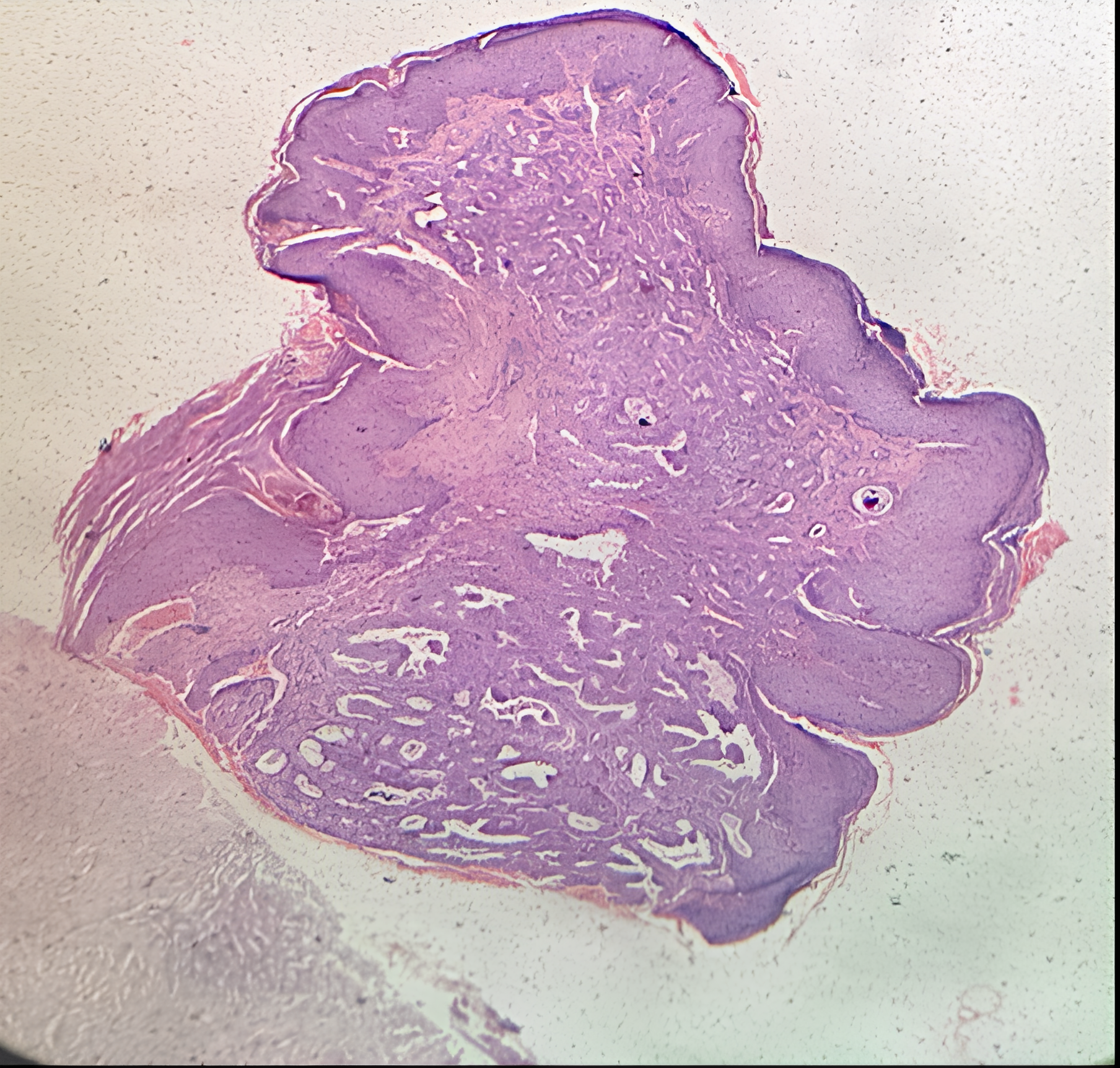
Figure 1: 40x magnification
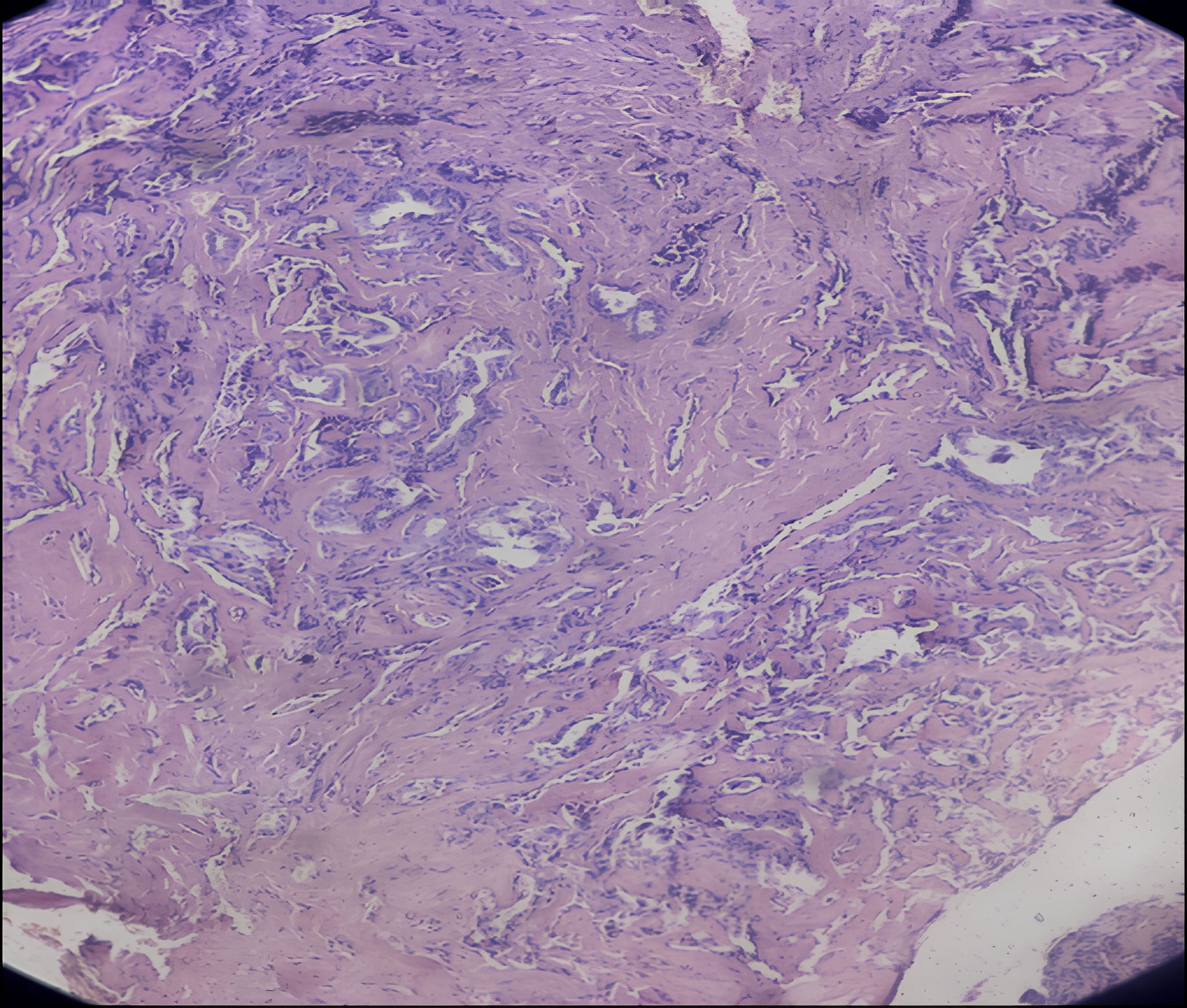
Figure 2: 100x magnification
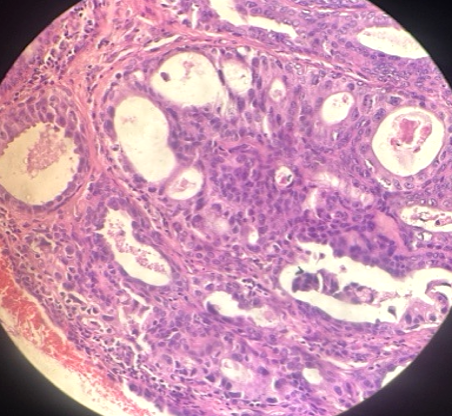
Figure 3: 400x magnification
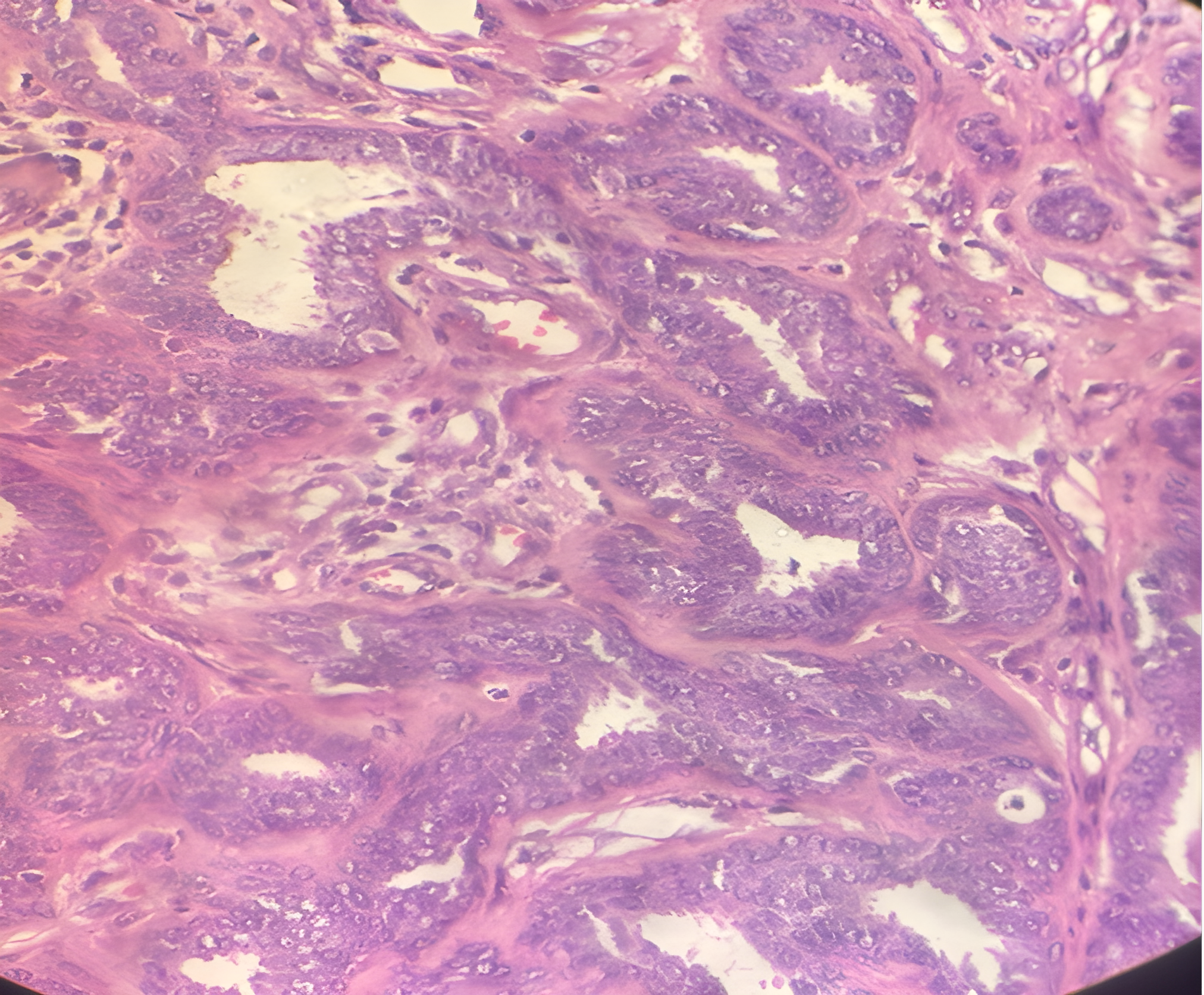
Figure 4: 400x magnification
Figures 1–4 show tumor cells arranged in nests, and in glandular, cribriform, papillary, and solid patterns, infiltrating into the deep fibrous tissue. The glandular structures are lined by inner luminal and outer myoepithelial cells. Focal areas reveal tumor cell emboli within the lumens of blood vessels.
Case Management
After the histopathology report was issued, the patient did not return for further evaluation, and subsequent attempts at communication were unsuccessful.
Discussion
Ceruminous neoplasms of the EAC were first termed as “ceruminoma” by Haugh in 1894.[7] The term “ceruminoma” has historically been used to describe both benign and malignant neoplasms of the ceruminous glands, leading to some confusion. Wetli et al. proposed a classification in 1972, these tumors were commonly grouped under the term “Ceruminoma,” which misleadingly implies a benign adenoma of ceruminous glands, even though over half of these tumors are malignant. Further confusion arises from older literature using the term “cylindroma” for what is now known as adenoid cystic carcinoma. Wetli et al. surveyed all cases of glandular tumors of the EAC and categorized them into four types based on their histological features: adenoid cystic carcinomas, ceruminous adenocarcinomas, ceruminous adenomas, and pleomorphic adenomas.[8]
Ceruminous adenocarcinomas and adenoid cystic carcinomas are malignant glandular tumors of the EAC. Pulec proposed mucoepidermoid carcinoma as another category of malignant glandular tumor of the EAC.[9] In 1991, the World Health Organization (WHO) excluded the term “ceruminoma” from its classification. The current WHO classification now categorizes malignant tumors of the ceruminous glands into three types: adenocarcinoma (both low and high grades), adenoid cystic carcinoma, and mucoepidermoid carcinoma.[10] Pleomorphic adenoma (mixed tumor), eccrine cylindroma, syringocystadenoma papilliferum, and the rare and disputed mucoepidermoid carcinoma are similar to their counterparts in other areas of the skin.[7,8,11] Etiopathogenesis of ceruminous carcinoma has not been fully clarified, but presumptive progenitors are embryonic anlage, ectopic remnants of salivary glands, and the ceruminal gland itself.[12] There are no known risk factors for the development of these tumors till now, although otitis externa has been implicated in animal models.[13] Ceruminous adenocarcinoma primarily affects individuals in their fifth or sixth decades of life, with a mean age of 48 years. However, there is a wide range of present ages, from 26 to 71 years. Both males and females are equally affected by this condition.[14,15]
Ceruminous adenocarcinoma typically presents in adults and often has a prolonged subclinical phase, sometimes lasting for years before symptoms become evident. The most common clinical symptoms include pain, a palpable mass in the ear canal, which may be blocked, followed by conductive hearing loss, aural fullness, otorrhea, and otalgia.[14-16] Other symptoms can include discharge, bleeding from the ear, cranial nerve palsies (such as facial nerve paralysis), and sensory abnormalities (paraesthesias).[5,16] On otoscopic examination, nodules covered by normal skin may be observed, sometimes associated with discharge or bleeding.[16,17] Ceruminous adenocarcinomas can present with different surface appearances. They may be covered by intact squamous epithelium, which can make them appear benign on initial inspection. However, if there is skin ulceration or erosion, along with signs of bony erosion on imaging studies like CT or magnetic resonance imaging (MRI), these findings strongly suggest a malignant neoplasm. The presence of ulceration and bony erosion indicates aggressive behavior and potential invasion into surrounding tissues, which is characteristic of malignancy.[16,17]
To assess the extent of the lesion and rule out invasion into surrounding bone or tissues, temporal bone CT or MRI scans are recommended. These imaging techniques also help in identifying any potential spread beyond the petrous part of the temporal bone or metastasis.[18] On immunohistochemistry (IHC), these tumors stain diffusely positive for keratin cocktail, epithelial membrane antigen (EMA), CD117, p63, and CK7. IHC can be helpful in highlighting the individual components, such as the dual cell population of epithelial and myoepithelial cells in ceruminous neoplasms, but it does not assist in diagnosing ceruminous malignancies.[19] In our study, we did not perform IHC because the histological appearance of the anatomical site was characteristic, and we are in a resource-limited setting.
Distant metastases from ceruminous adenocarcinoma to the lung, liver, kidney, cervical lymph nodes, and bones have been reported. These metastases tend to maintain the primary histological identity of the original tumor.[5,16] Adenocarcinoma can present with intracranial invasion.[19,20] Metastasis indicates a poor prognosis in these types of cancer. Death is usually caused by intracranial extension of the tumor or by pulmonary metastases.[21] This case highlights the challenges in diagnosis and management of this rare entity, emphasizing the importance of comprehensive histopathological evaluation and a multidisciplinary approach to the case of the patient.
Conclusion
Ceruminous carcinomas are rare malignancies that typically present with a mass or pain in the outer ear canal of middle-aged patients. These tumors are relatively large for their anatomical site and exhibit an infiltrative pattern, moderate to severe nuclear pleomorphism, increased mitotic figures, and occasionally necrosis. They are classified into ceruminous adenocarcinoma, NOS (not otherwise specified), ceruminous adenoid cystic carcinoma, and ceruminous mucoepidermoid carcinoma. Pathologists often encounter diagnostic difficulties, especially with small samples. In resource-constrained environments, diagnosis solely on histomorphology grounds can be challenging, and hence our study highlights the pivotal role of routine microscopy and a structured morphological approach.
References
- Johnstone JM, Lennox B, Watson AJ. Five cases of hidradenoma of the external auditory meatus: So‐called ceruminoma. J Pathol Bacteriol. 1957;73(2):421-427. doi:10.1002/path.1700730212 Crossref | Google Scholar
- Cankar V, Crowley H. Tumors of ceruminous glands: A clinicopathological study of 7 cases. Cancer. 1964;17:67-75. doi:10.1002/1097-0142(196401)17:1<67::aid-cncr2820170109>3.0.co;2-a PubMed | Crossref | Google Scholar
- JUBY HB. Tumours of the ceruminous glands; so called ceruminoma. J Laryngol Otol. 1957;71(12):832-837. doi:10.1017/s0022215100052531 PubMed | Crossref | Google Scholar
- Ramadass T, Satuanarayana C. Ceruminoma of external ear. A clinico-pathological study of three cases. J Laryngol Otol. 1973;87(12):1201-1210. doi:10.1017/s0022215100078178 PubMed | Crossref | Google Scholar
- Crain N, Nelson BL, Barnes EL, Thompson LD. Ceruminous gland carcinomas: a clinicopathologic and immunophenotypic study of 17 cases. Head Neck Pathol. 2009;3(1):1-17. doi:10.1007/s12105-008-0095-9 PubMed | Crossref | Google Scholar
- Batsakis, John G. Tumors of the Head and Neck: Clinical and Pathological Considerations. 2d ed. Baltimore: Williams & Wilkins; 1979. Tumors of the Head and Neck: Clinical and Pathological Considerations
- Tzagaroulakis A, Pasxalidis J, Papadimitriou N, et al. Recurrent ceruminous adenocarcinoma of the external auditory canal. ORL J Otorhinolaryngol Relat Spec. 2003;65(5):300-302. doi:10.1159/000075230 PubMed | Crossref | Google Scholar
- Wetli CV, Pardo V, Millard M, Gerston K. Tumors of ceruminous glands. Cancer. 1972;29(5):1169-1178. doi:10.1002/1097-0142(197205)29:5<1169::aid-cncr2820290507>3.0.co;2-8 PubMed | Crossref | Google Scholar
- Pulec JL. Glandular tumors of the external auditory canal. Laryngoscope. 1977;87(10 Pt 1):1601-1612. doi:10.1288/00005537-197710000-00001 PubMed | Crossref | Google Scholar
- Yang Y, Liu H, Fang J, Li Y, Chen S. Ceruminous adenoma of the external auditory canal: 9 cases series with imaging and pathologic findings. Front Oncol. 2023;13:1041282. doi:10.3389/fonc.2023.1041282 PubMed | Crossref | Google Scholar
- Garin P, Degols JC, Delos M, Marbaix E. Benign ceruminous tumours of the external ear canal. J Otolaryngol. 1999;28(2):99-101. Benign ceruminous tumours of the external ear canal
- Thompson LD, Nelson BL, Barnes EL. Ceruminous adenomas: a clinicopathologic study of 41 cases with a review of the literature. Am J Surg Pathol. 2004;28(3):308-318. doi:10.1097/00000478-200403000-00003 PubMed | Crossref | Google Scholar
- Moisan PG, Watson GL. Ceruminous gland tumors in dogs and cats: a review of 124 cases. J Am Anim Hosp Assoc. 1996;32(5):448-452. doi:10.5326/15473317-32-5-448 PubMed | Crossref | Google Scholar
- Mills RG, Douglas-Jones T, Williams RG. ‘Ceruminoma’–a defunct diagnosis. J Laryngol Otol. 1995;109(3):180-188. ‘Ceruminoma’–a defunct diagnosis
- Jan J, Wang C, Kwan P, Wu S, Shu H. Ceruminous Adenocarcinoma With Extensive Parotid, Cervical, and Distant Metastases: Case Report and Review of Literature. Arch Otolaryngol Head Neck Surg. 2008;134(6):663–666. doi:10.1001/archotol.134.6.663 PubMed | Crossref | Google Scholar
- Soon SL, Bullock M, Prince ME. Ceruminous adenocarcinoma: a rare tumour of the external auditory canal. J Otolaryngol. 2001;30(6):373-377. Ceruminous adenocarcinoma: a rare tumour of the external auditory canal
- Shim J. Ceruminous gland adenocarcinoma of external ear canal – A case report -. Journal of pathology and translational medicine. 2007;41(1):66-68. Ceruminous Gland Adenocarcinoma of External Ear Canal: A Case Report
- Iqbal A, Newman P. Ceruminous gland neoplasia. Br J Plast Surg. 1998;51(4):317-320. doi:10.1054/bjps.1997.0075 PubMed | Crossref | Google Scholar
- McDonald M, Brophy BP, Raymond W. Intracranial invasion from a primary adenocarcinoma arising in the middle and external ear. Aust N Z J Surg. 1995;65(6):454-456. doi:10.1111/j.1445-2197.1995.tb01780.x PubMed | Crossref | Google Scholar
- Berlin L. Intracranial ceruminous adenoma. J Neurosurg. 1949;6(5):415-418. doi:10.3171/jns.1949.6.5.0415 PubMed | Crossref | Google Scholar
- Hageman ME, Becker AE. Intracranial invasion of a ceruminous gland tumor. A follow-up of 12 years. Arch Otolaryngol. 1974;100(5):395-397. doi:10.1001/archotol.1974.00780040407020 PubMed | Crossref | Google Scholar
Acknowledgments
None
Funding
None
Author Information
Corresponding Author:
Ujjwal Sangroula
Department of Pathology
National Medical College and Teaching Hospital, Birgunj, Nepal
Email: [email protected]
Co-Authors:
Guru Prasad Mainali, Ratan Shah
Department of Pathology
National Medical College and Teaching Hospital, Birgunj, Nepal
Authors Contributions
Guru Prasad Mainali reported and signed out the histopathological diagnosis of the case, proposed the idea for the case report, outlined its structure, and took a lead role in writing the manuscript. Ratan Shah drafted the manuscript, coordinated revisions, and conducted a literature review to contextualize the case. Ujjwal Sangroula was responsible for gathering and selecting histopathological images, assisting in reviewing relevant literature, contributing to the drafting and revision of the manuscript, obtaining patient consent, and submitting the manuscript while handling communication with the journal.
Informed Consent
Written informed consent was obtained from the patient for the publication of this case report and the accompanying images.
Conflict of Interest Statement
None
Guarantor
Dr. Guru Prasad Mainali, Lecturer in the Department of Pathology at National Medical College, Birgunj, Nepal, serves as the guarantor for this case report.
DOI
Cite this Article
Mainali GP, Shah R, Sangroula U. A Rare Case of Ceruminous Adenocarcinoma of External Auditory Canal. medtigo J Med. 2025;3(2):e30623231. doi:10.63096/medtigo30623231 Crossref













