







 Author Affiliations
Author Affiliations
Abstract
Background: Progressive supranuclear palsy (PSP) is a rare neurodegenerative disorder that presents with a spectrum of motor, behavioral, and cognitive features. Its clinical overlap with Parkinson’s disease and other Parkinsonian syndromes often leads to misdiagnosis. In low-resource settings, diagnostic challenges are compounded by limited access to neuroimaging, specialist care, and awareness of atypical Parkinsonian disorders.
Case presentation: We report a 69-year-old Nigerian male with a 10-month history of progressive gait disturbance, behavioral changes, and recurrent falls. Initial misdiagnoses and reliance on traditional remedies delayed appropriate care. Neurological examination revealed axial rigidity, retrocollis, and supranuclear vertical gaze palsy. Magnetic resonance imaging (MRI) demonstrated midbrain atrophy with preserved pontine volume, the characteristic “hummingbird sign,” a radiological hallmark of PSP. A concurrent left femoral head fracture, a rare musculoskeletal complication of PSP, was identified, likely secondary to repeated falls and immobility.
Conclusion: This case emphasizes the diagnostic complexity of PSP in resource-limited environments and highlights the importance of clinical vigilance, early neuroimaging, and multidisciplinary management. It also underscores the need for proactive fall-prevention strategies to reduce secondary complications. Greater awareness among clinicians and integration of imaging findings into routine practice may improve recognition and outcomes in similar settings.
Keywords
Progressive supranuclear palsy, Vertical gaze palsy, Magnetic resonance imaging, Hummingbird sign, Femoral fracture, Low-resource setting.
Introduction
PSP is a rare neurodegenerative tauopathy characterized by postural instability, vertical gaze palsy, axial rigidity, and cognitive dysfunction.[1] First described by Steele, Richardson, and Olszewski in 1963.[2] PSP remains a diagnostic challenge due to its clinical overlap with Parkinson’s disease and other atypical Parkinsonian syndromes.[1] The hallmark features, including early falls, supranuclear gaze palsy, and poor levodopa response, often emerge gradually, leading to misdiagnosis, especially in low-resource settings where access to advanced neuroimaging and subspecialty care is limited.[3]
In sub-Saharan Africa, the burden of neurodegenerative diseases is rising, yet diagnostic infrastructure remains underdeveloped.[4] This case report highlights the clinical and radiological diagnosis of PSP in a Nigerian patient, with emphasis on the role of MRI in confirming the diagnosis.[5] It also explores the musculoskeletal complications associated with PSP, including a femoral fracture secondary to repeated falls and prolonged immobility.[6]
Case Presentation
A 69-year-old male presented to our neurology unit with a 10-month history of progressive gait disturbance and recurrent falls. The initial symptoms were subtle, involving unsteadiness and difficulty initiating movement. Over time, the patient experienced three documented falls, followed by noticeable behavioral changes, including apathy, reduced social interaction, and cognitive slowing. Due to increasing rigidity and confinement to a fixed flexed posture, the family sought help from traditional bone setters, but no improvement was noted. He was later evaluated at a primary health care center, where he received conflicting diagnoses of Parkinson’s disease and stroke and was treated empirically without benefit.
Upon presentation to our center, neurological examination revealed marked axial rigidity, retrocollis, and supranuclear vertical gaze palsy. The patient was non-ambulatory and required assistance with all activities of daily living. Given the constellation of symptoms, a clinical diagnosis of PSP was made. Despite financial constraints, the patient’s family obtained a brain MRI, which revealed midbrain atrophy with preserved pontine volume, the classic “hummingbird sign” confirming the diagnosis of PSP as shown in Figure 1. Considering his history of repeated falls and prolonged immobility, a pelvic radiograph was performed, revealing a fracture of the left femoral head (Figure 2).
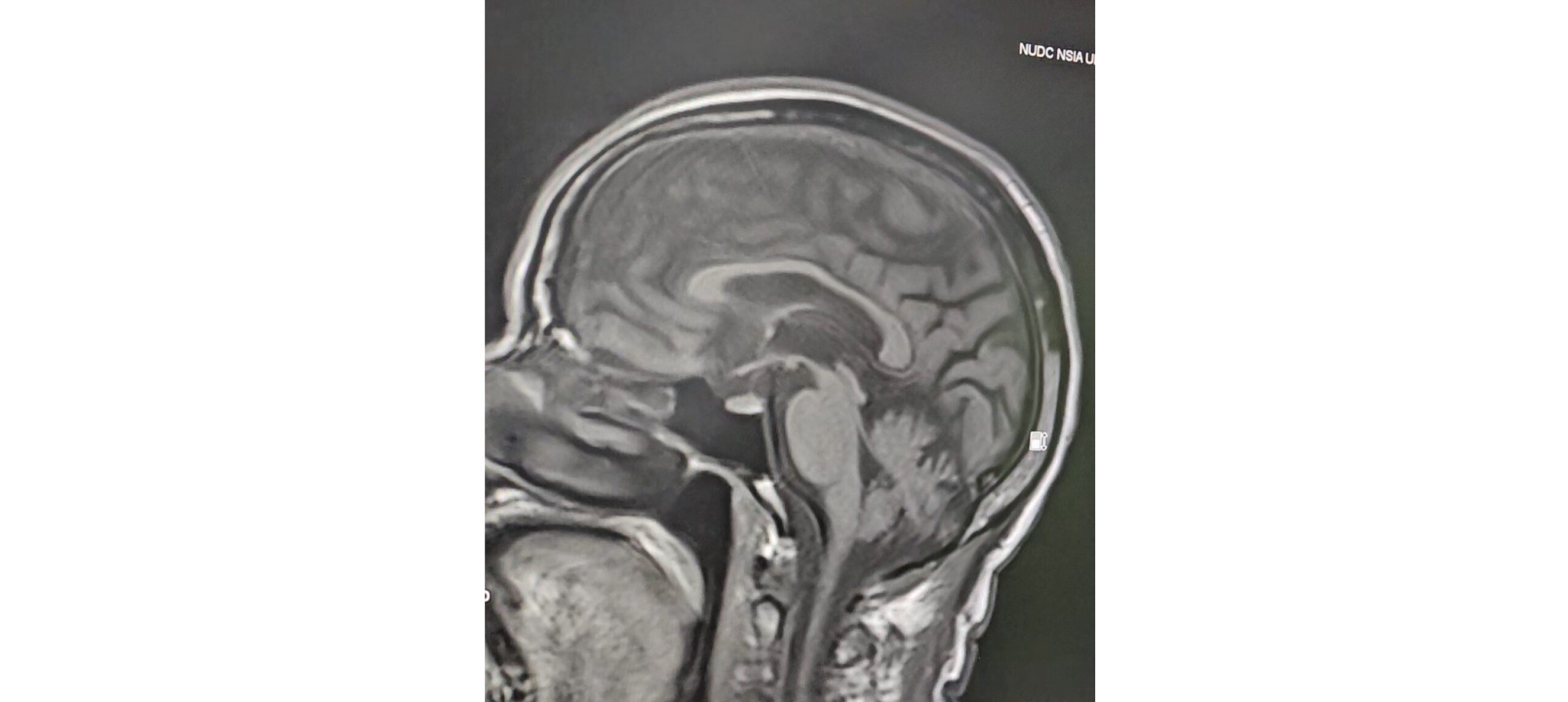
Figure 1: Midbrain atrophy demonstrating the “Hummingbird Sign” on brain MRI in PSP
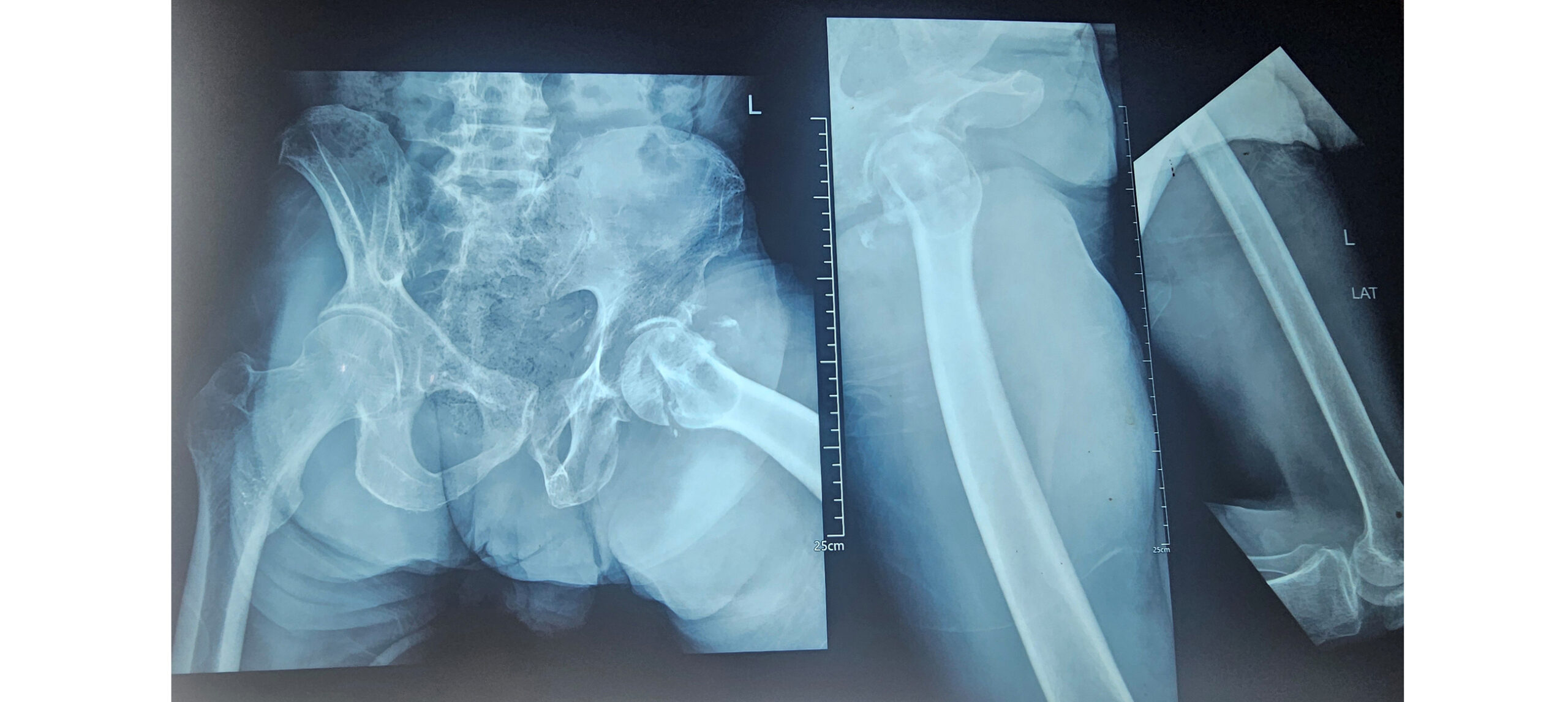
Figure 2: Pelvic and left femoral radiographs showing femoral head fracture following recurrent falls
Case Management
The patient was managed conservatively with supportive care, physiotherapy, and counseling. Orthopedic consultation was sought for a femoral fracture, and a multidisciplinary approach was initiated to optimize quality of life. Patient continued with regular physiotherapy, reporting subjective improvement in mobility and functional status while under our neurology clinic follow-up. On account of the left femoral head fracture sustained from the recurrent falls, the orthopedic team, in view of the marked axial rigidity, equally recommended continuation of physiotherapy until sufficient relief was achieved to permit surgical intervention.
Discussion
PSP is a neurodegenerative disorder that often masquerades as Parkinson’s disease, particularly in its early stages.[1] The classic presentation includes postural instability, vertical gaze palsy, axial rigidity, and cognitive decline. These features were evident in our patient. However, in low-resource settings, the diagnosis is frequently delayed due to limited access to neuroimaging, lack of awareness, and overlapping clinical features with more common conditions such as stroke and idiopathic Parkinson’s disease.[3]
Our patient’s journey reflects the diagnostic odyssey typical of PSP in underserved regions. Initial misdiagnoses and reliance on traditional healers underscore the need for improved neurological education and access to specialized care.[4] The eventual identification of vertical gaze palsy and retrocollis, both hallmark signs of PSP, guided the clinical suspicion, which was confirmed by MRI showing the “hummingbird sign,” a well-established radiological marker of midbrain atrophy.[7] Importantly, our diagnostic approach aligns with the Movement Disorder Society (MDS) clinical criteria for PSP, which emphasize early recognition of postural instability and supranuclear gaze palsy as key diagnostic anchors.[8]
The presence of a femoral head fracture adds a unique dimension to this case. While musculoskeletal complications are not primary features of PSP, they may arise secondary to frequent falls, prolonged immobility, and rigidity.[6] This highlights the importance of early mobility interventions, fall prevention strategies, and orthopedic evaluation in PSP management. In resource-limited settings, where rehabilitation services are sparse, such complications can significantly worsen morbidity and caregiver burden.[9]
This case also emphasizes the resilience of families in low-income contexts, who, despite financial hardship, pursued advanced diagnostics to secure an accurate diagnosis. Their commitment enabled a multidisciplinary approach to care, including neurology, orthopedics, and physiotherapy, a model that should be encouraged and supported through health policy and advocacy. Thus, emerging global investigations into Parkinson’s disease among African and African‑admixed populations have underscored the critical role of African neurologists in international research consortia, thereby reinforcing the imperative for robust advocacy and policy frameworks aimed at strengthening neurological care across the continent.[10]
Conclusion
This case illustrates the clinical and radiological diagnosis of PSP in a low-resource Nigerian setting, highlighting the challenges of early recognition and the consequences of delayed intervention. The co-occurrence of a femoral fracture underscores the need for comprehensive care that addresses both neurological and musculoskeletal complications. Greater awareness, improved access to neuroimaging, and multidisciplinary collaboration guided by international diagnostic criteria are essential to enhance outcomes for patients with PSP in low- and middle-income countries.
References
- Batheja V, Fish M, Balar AB, Hogg JP, Lakhani DA, Khan M. Progressive supranuclear palsy: A case report and brief review of the literature. Radiol Case Rep. 2023;19(1):250-253. doi:10.1016/j.radcr.2023.09.012
PubMed | Crossref | Google Scholar - Steele JC, Richardson JC, Olszewski J. Progressive Supranuclear Palsy. A Heterogeneous Degeneration Involving the Brain Stem, Basal Ganglia and Cerebellum with Vertical Gaze and Pseudobulbar Palsy, Nuchal Dystonia and Dementia. Arch Neurol. 1964;10:333-359. doi:10.1001/archneur.1964.00460160003001
PubMed | Crossref | Google Scholar - Williams DR, Lees AJ. Progressive supranuclear palsy: clinicopathological concepts and diagnostic challenges. Lancet Neurol. 2009;8(3):270-279. doi:10.1016/S1474-4422(09)70042-0
PubMed | Crossref | Google Scholar - Dotchin CL, Msuya O, Walker RW. The challenge of Parkinson’s disease management in Africa. Age Ageing. 2007;36(2):122-127. doi:10.1093/ageing/afl172
PubMed | Crossref | Google Scholar - Boxer AL, Yu JT, Golbe LI, Litvan I, Lang AE, Höglinger GU. Advances in progressive supranuclear palsy: new diagnostic criteria, biomarkers, and therapeutic approaches. Lancet Neurol. 2017;16(7):552-563. doi:10.1016/S1474-4422(17)30157-6
PubMed | Crossref | Google Scholar - Yatakarla V, Deshmukh J, Patil R, Ruikar D, Limbapure A. A case report on progressive supranuclear palsy. Exclusive Real World Evidence Journal. 2022;2. doi:10.54136/ERWEJ-0201-10013
Crossref - Oba H, Yagishita A, Terada H, et al. New and reliable MRI diagnosis for progressive supranuclear palsy. Neurology. 2005;64(12):2050-2055. doi:10.1212/01.WNL.0000165960.04422.D0
PubMed | Crossref | Google Scholar - Höglinger GU, Respondek G, Stamelou M, et al. Clinical diagnosis of progressive supranuclear palsy: The movement disorder society criteria. Mov Disord. 2017;32(6):853-864. doi:10.1002/mds.26987
PubMed | Crossref | Google Scholar - Rowe JB, Holland N, Rittman T. Progressive supranuclear palsy: diagnosis and management. Pract Neurol. 2021;21(5):376-383. doi:10.1136/practneurol-2020-002794
PubMed | Crossref | Google Scholar - Rizig M, Bandres-Ciga S, Makarious MB, et al. Identification of genetic risk loci and causal insights associated with Parkinson’s disease in African and African admixed populations: a genome-wide association study. Lancet Neurol. 2023;22(11):1015-1025. doi:10.1016/S1474-4422(23)00283-1
PubMed | Crossref | Google Scholar
Acknowledgments
We acknowledge the contributions of the orthopaedic team and physiotherapy team who were actively involved in the patient’s management and follow-up.
Funding
None
Author Information
Corresponding Author:
Donald Chukwunonso Okerulu
Department of Internal Medicine
Federal Medical Centre Umuahia, Abia State, Nigeria
Email: [email protected]
Co-Authors:
Joseph Ugwunna Iheanacho, Ihunanya Happiness Mba, Perfection Chinyere Igwe, Rowland Ihezuo Nwanke
Department of Internal Medicine
Federal Medical Centre Umuahia, Abia State, Nigeria
Authors Contributions
Joseph Ugwunna Iheanacho conducted the clinical evaluation and documented the patient’s neurological findings. Donald Chukwunonso Okerulu retrieved the radiological images, performed a literature review, and drafted the manuscript. Ihunanya Happiness Mba reviewed and documented the radiological findings, ensuring accuracy of imaging details. Perfection Chinyere Igwe obtained written informed consent from the patient and his family for the publication of this case report. Rowland Nwanke critically revised the manuscript for important intellectual content. All authors meet the criteria for authorship as defined by the International Committee of Medical Journal Editors (ICMJE), contributed significantly to the work, reviewed the manuscript, and approved the final version for publication.
Informed consent
Informed consent was obtained from the patient and his family.
Conflict of Interest Statement
The authors declare that they have no conflict of interest.
Guarantor
In this case report, Donald Chukwunonso Okerulu serves as the guarantor.
DOI
Cite this Article
Iheanacho JU, Okerulu DC, Mba IH, Igwe PC, Nwanke RI. A Diagnostic Odyssey: Progressive Supranuclear Palsy Presenting with Gait Disturbance, Behavioral Changes, and Femoral Fracture in a Low-Resource Setting.
medtigo J Neurol Psychiatr. 2026;3(2):e3084323. doi:10.63096/medtigo3084323 Crossref













